")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 20
Vitamin D and Sarcopenia in the Senior People: A Review of Mechanisms and Comprehensive Prevention and Treatment Strategies
Received 28 March 2024
Accepted for publication 31 August 2024
Published 5 September 2024 Volume 2024:20 Pages 577—595
DOI https://doi.org/10.2147/TCRM.S471191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Fan Zhang,1,2 Wenjian Li3
1Department of Endocrinology, Changzhou Third People’s Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China; 2Department of Clinical Nutrition, Changzhou Third People’s Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China; 3Department of Urology, Changzhou Third People’s Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China
Correspondence: Wenjian Li, Department of Urology, Changzhou Third People’s Hospital, Changzhou Medical Center, Nanjing Medical University, 300 Lanling North Road, Changzhou, Jiangsu, 213001, People’s Republic of China, Tel +86-519-82009011, Email [email protected]
Abstract: This article reviews the mechanisms and prevention strategies associated with vitamin D and sarcopenia in older adults. As a geriatric syndrome, sarcopenia is defined by a notable decline in skeletal muscle mass and strength, which increases the risk of adverse health outcomes such as falls and fractures. Vitamin D, an essential fat-soluble vitamin, is pivotal in skeletal muscle health. It affects muscle function through various mechanisms, including regulating calcium and phosphorus metabolism, promoting muscle protein synthesis, and modulation of muscle cell proliferation and differentiation. A deficiency in vitamin D has been identified as a significant risk factor for the development of sarcopenia in older adults. Many studies have demonstrated that low serum vitamin D levels are significantly associated with an increased risk of sarcopenia. While there is inconsistency in the findings, most studies support the importance of vitamin D in maintaining skeletal muscle health. Vitamin D influences the onset and progression of sarcopenia through various pathways, including the promotion of muscle protein synthesis, the regulation of mitochondrial function, and the modulation of immune and inflammatory responses. Regarding the prevention and treatment of sarcopenia, a combination of nutritional, exercise, and pharmacological interventions is recommended. Further research should be conducted to elucidate the molecular mechanism of vitamin D in sarcopenia, to study genes related to sarcopenia, to perform large-scale clinical trials, to investigate special populations, and to examine the combined application of vitamin D with other nutrients or drugs. A comprehensive investigation of the interconnection between vitamin D and sarcopenia will furnish a novel scientific foundation and productive strategies for preventing and treating sarcopenia. This, in turn, will enhance the senior people’s quality of life and health.
Keywords: vitamin D, sarcopenia, senior people, pathogenesis, comprehensive prevention and treatment strategies
Introduction
Sarcopenia is a geriatric syndrome characterized by a significant loss of skeletal muscle mass and a marked decline in muscle strength with age.1–3 It is triggered by persistent loss of skeletal muscle mass and a decline in muscle strength and function.2 Given the central role of skeletal muscle in the body’s locomotor system, atrophy and dysfunction of this tissue are significant indicators of aging. Such conditions can result in various health complications, including fractures and joint damage.4,5 The senior people with sarcopenia may experience instability and staggering, increasing their risk of falls and subsequent fractures.6,7 Furthermore, sarcopenia has a detrimental effect on the body’s metabolic function, potentially resulting in diabetes, cardiovascular disease, lung failure, and even endangering one’s life.1,8
The prevalence of sarcopenia is known to increase with age. Although the prevalence varies depending on the diagnostic criteria and study population,9,10 it is generally recognized that sarcopenia affects 10–20% of the senior people over the age of 60 years, and this rate may climb to over 30% by the age of 80 years.11–13 The development of sarcopenia is a multifactorial process that involves genetics, neurological decline, decreased mitochondrial function in skeletal muscle, fatty infiltration, lack of exercise, chronic diseases, and malnutrition.2,14,15 It is important to note that sarcopenia is more prevalent in patients with chronic diseases than in the general population, with rates ranging from 18% in patients with diabetes to 66% in patients diagnosed with cancer.16
Vitamin D is an essential fat-soluble vitamin for human health.17 Its physiological functions are diverse and cover many core areas, including regulating calcium and phosphorus metabolism, maintaining bone health, and regulating immune function.18–20 There are two primary forms of vitamin D: vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol).21 Vitamin D3 is primarily synthesized naturally in the skin through sunlight exposure, but it can also be obtained from food sources such as cod liver oil and egg yolks.18,21,22 After entering the body, vitamin D undergoes hydroxylation in the liver to form 25-hydroxyvitamin D (25(OH)D), the primary circulating form of the vitamin in the bloodstream. In the kidneys, (25(OH)D) is hydroxylated to form the biologically active 1.25-dihydroxyvitamin D.23,24 This active form binds to the vitamin D receptor (VDR) in target cells, regulating the expression of relevant genes and allowing for fine-tuned regulation of calcium and phosphorus metabolism, cellular differentiation, and other vital physiological processes.17–20
Vitamin D is essential for maintaining bone and muscle health. It facilitates the absorption of calcium and phosphorus in the intestines, which are necessary minerals for building bone. Additionally, it stimulates the synthesis and mineralization of bone matrix by directly acting on osteoblasts, promoting bone growth and maturation. Vitamin D regulates blood calcium and phosphorus metabolism, maintaining their balance. This is crucial for keeping bones strong and stable.19 Vitamin D inhibits the activity of osteoclasts and reduces bone resorption, thus maintaining bone density and preventing bone diseases such as osteoporosis and fractures. Additionally, it has an essential impact on muscle function. Research has unequivocally demonstrated that vitamin D receptors are widely present in muscle tissue, and vitamin D directly impacts the differentiation and metabolism of muscle cells to ensure normal muscle function.25,26 A deficiency in vitamin D unequivocally reduces muscle strength and increases the risk of falls due to fatigue.27,28 Furthermore, vitamin D plays an indirect yet crucial role in maintaining overall skeletal muscle health by regulating the immune and neuromuscular systems.26
In recent years, research on the relationship between vitamin D and sarcopenia has received increased attention due to its potential significance. Many studies have examined the relationship between vitamin D levels and sarcopenia and have reached some meaningful conclusions. Some studies have demonstrated a significant correlation between vitamin D deficiency and an elevated risk of sarcopenia. However, not all studies have yielded consistent results, and some have also failed to observe a significant association between vitamin D levels and sarcopenia. These discrepancies in findings may be attributed to many factors, including study design, sample size, selection of study participants, definition of vitamin D deficiency, and diagnostic criteria for sarcopenia. Nevertheless, most studies continue to support the crucial role of vitamin D in maintaining skeletal muscle health and suggest that vitamin D deficiency may be an independent risk factor for sarcopenia. Therefore, a comprehensive investigation of the relationship between vitamin D and sarcopenia is of significant scientific and practical importance and will positively impact the quality of life of the senior people.
Vitamin D Deficiency and the Incidence of Sarcopenia in the Senior People
Several studies have shown a strong association between vitamin D deficiency and sarcopenia in the senior people. The prevalence of vitamin D deficiency in the senior people ranges from 17.4% to 87%.29 This decrease in serum vitamin D levels is attributed to inadequate intake,30 lack of sun exposure,31 skin pigmentation,32 and absorption inhibition.33 The senior people, in particular, have lower levels of 7-dehydrocholesterol in their skin, resulting in less vitamin D production from sunlight.34 This, in turn, increases the risk of vitamin D deficiency in this population. Recent studies have shown that the skin produces about 13% less vitamin D per decade, meaning that 70-year-old subjects produce only half as much vitamin D as 20-year-old subjects.35 It is worth noting that the vitamin D status of older hospitalized patients is particularly concerning.36 As the skin’s ability to synthesize vitamin D declines and kidney function deteriorates with age, there is a corresponding decrease in the conversion of vitamin D to its active form, 1.25-dihydroxyvitamin D.37 This deficiency ultimately leads to reduced stimulation of the VDR.37 VDR expression decreases with age, reducing sensitivity to 1.25-dihydroxyvitamin D.38 Furthermore, there is an association between iron deficiency, anemia, and vitamin D deficiency.39,40 This suggests combining these nutritional deficiencies will create a greater risk for muscle health and inflammation.29,41
Multiple academic studies have confirmed a significant positive correlation between vitamin D deficiency and loss of muscle strength.42–44 Low levels of serum (25(OH)D) are strongly associated with the loss of muscle strength45–47 and impairment of physical function.48–50 Vitamin D deficiency can lead to muscle abnormalities, such as type II fibrous atrophy, infiltration of adipocytes and glycogen granules in the muscle, enlarged fibrous gaps, and increased fibrosis.51 A recent report by Yang et al52 suggests that the combination of low serum vitamin D levels and lack of exercise can further exacerbate muscular atrophy in the senior people. Bang et al53 demonstrated that older women with vitamin D deficiency had significantly lower lumbar muscle strength and a higher percentage of fat infiltration in paraspinal muscles compared to the control and vitamin D-sufficient groups. Furthermore, various studies in the senior people have indicated that lower vitamin D levels are significantly associated with reduced muscle strength and physical activity.54,55 Research has shown a significant correlation between vitamin D deficiency, decreased muscle function, and an increased risk of sarcopenia in humans.56 In the senior people, serum vitamin D levels may predict the decline in skeletal muscle function and atrophy with age, and its deficiency may significantly increase the risk of sarcopenia.57,58
The academic community has produced a range of findings regarding exploring the link between vitamin D deficiency and sarcopenia in the senior population. While the majority of studies tend to conclude that there is a strong association between the two, some studies still fail to reveal this interconnection. Table 1 summarizes a series of relevant studies to dissect the potential association between vitamin D deficiency and sarcopenia in the senior population.
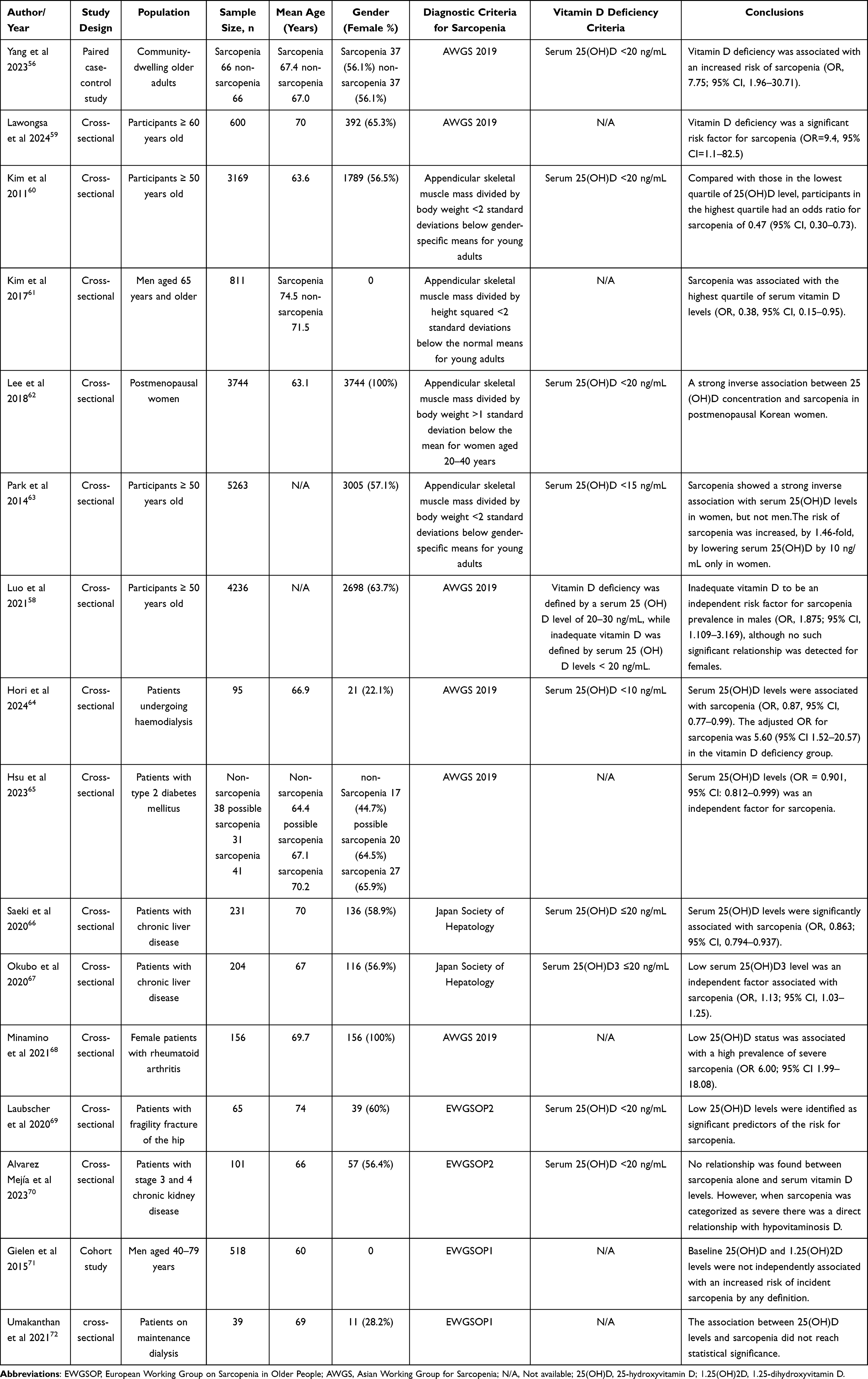 |
Table 1 Studies About Sarcopenia and Vitamin D in Senior People |
In particular, the findings of several studies indicate a positive correlation between vitamin D deficiency and sarcopenia in older adults. For example, a paired case-control study conducted by Yang et al56 demonstrated that vitamin D deficiency (serum 25(OH)D < 20 ng/mL) was significantly associated with an increased risk of sarcopenia in a community-dwelling group of older adults (OR = 7.75, 95% CI: 1.96–30.71). Similarly, two cross-sectional studies by Lawongsa et al59 and Kim et al60 corroborated the assertion that vitamin D deficiency represents a significant risk factor for sarcopenia.
The complexity of this association is further revealed by gender-specific analyses, with negative associations between 25(OH)D concentrations and sarcopenia confirmed in a study of men aged 65 years and older by Kim et al61 and in a study of postmenopausal women by Lee et al.62 However, the opposite conclusion, In contrast, the study by Park et al and Luo et al yielded different results. The study by Park et al,63 which included 5263 participants aged 50 years and older, revealed a strong negative correlation between serum 25(OH)D levels and sarcopenia in women. Still, no such association was observed in men. In contrast, a cross-sectional study by Luo et al,58 which included 4236 participants aged 50 years and older, indicated that vitamin D insufficiency (serum 25(OH)D < 20 ng/mL) was an independent risk factor for sarcopenia in men. In contrast, no significant correlation was observed in women.
Studies have similarly indicated an association between vitamin D deficiency and sarcopenia in the context of specific diseases. For example, a study by Hori et al64 in hemodialysis patients found that vitamin D deficiency (serum 25(OH)D < 10 ng/mL) was significantly associated with sarcopenia (OR = 5.60, 95% CI: 1.52–20.57). Similarly, low vitamin D levels were also found to be strongly associated with a high prevalence of sarcopenia in patients with type 2 diabetes mellitus,65 patients with chronic liver disease,66,67 female patients with rheumatoid arthritis,68 and patients with hip fragility fractures.69
It is nevertheless noteworthy that not all studies have yielded consistent results. For example, a cross-sectional study of 101 patients with stage 3 and 4 chronic kidney disease by Alvarez Mejía et al70 found no association between sarcopenia alone and serum vitamin D levels. However, a direct association was observed between vitamin D deficiency and the presence of severe sarcopenia. Furthermore, a cohort study by Gielen et al71 did not identify a notable elevation in the risk of sarcopenia with baseline vitamin D levels. Similarly, a study by Umakanthan et al72 in dialysis patients did not discern a substantial correlation between vitamin D levels and sarcopenia.
In conclusion, most available studies indicate that vitamin D deficiency is a significant risk factor for sarcopenia in older adults. However, the inconsistency of diagnostic criteria for sarcopenia and the variability in cut-off values for determining vitamin D deficiency must be considered when interpreting the results of these studies. Therefore, using uniform diagnostic criteria and judgmental thresholds in future studies will facilitate the accurate revelation of the association between vitamin D deficiency and sarcopenia.
Mechanism of Vitamin D in the Pathogenesis of Sarcopenia in the Senior People
Promoting Muscle Protein Synthesis
Vitamin D is important in promoting muscle protein synthesis. This is primarily achieved through the activation of the VDR, which binds to specific DNA sequences and regulates the expression of genes associated with protein synthesis.73–76 These genes encode enzymes and factors necessary for muscle protein synthesis, essential for muscle growth and repair.77,78 Vitamin D deficiency can decrease the rate of muscle protein synthesis, reducing muscle mass.74,79
Vitamin D helps maintain calcium ion balance in muscle cells and reinforces the signaling role of calcium ions, which is critical for protein synthesis.80 Vitamin D regulates metabolic processes within muscle cells, optimizing energy metabolic pathways to provide sufficient energy and substrates for muscle protein synthesis.81–84 It also reduces muscle cell apoptosis and enhances cell survival, thereby maintaining muscle mass and protein synthesis capacity.85–87 In sarcopenia, increased apoptosis of muscle cells is a critical pathological change. Vitamin D interacts with other nutrients and hormones to enhance its effect on promoting muscle protein synthesis.84,88,89 These regulatory networks work together to maintain muscle health and function.
Regulation of Muscle Cell Proliferation and Differentiation
Vitamin D is essential for the proliferation and differentiation of muscle cells. Research has demonstrated that vitamin D can effectively promote the proliferation and differentiation of muscle stem cells.75,78,90 These cells play a crucial role in muscle regeneration and repair processes. Without sufficient vitamin D, the proliferation and differentiation of muscle stem cells may be hindered, negatively impacting muscle regeneration.73 Vitamin D binds to the VDR and forms a heterodimer with the retinoic acid X receptor (RXR). This heterodimer then binds to vitamin D response elements (VDREs) located in the promoter regions of muscle-associated genes, directly regulating their transcriptional activity.91–93
Activation of key regulators, such as cell cycle proteins and cell cycle-dependent kinases, achieves proliferation. Vitamin D significantly promotes the proliferation of muscle satellite cells, which supply new muscle fibers in response to muscle damage or growth demands.80,84,90,94 The stimulatory effect of vitamin D increases the number and activity of satellite cells, thereby aiding muscle regeneration and repair.76,84,94 Regarding differentiation, vitamin D upregulates the expression of muscle-specific genes, such as myosin heavy chain (MyHC) and muscle creatine kinase (MCK), promoting muscle cell differentiation and maturation.95 Additionally, vitamin D significantly enhances myoblast differentiation, as demonstrated by increased expression of differentiation markers, including myogenin and troponin T type 1.84 These effects contribute to the transition of muscle cells from a proliferative state to mature muscle fibers, enhancing muscle mass and strength.88,90 Additionally, vitamin D may influence muscle contractile and diastolic processes by modulating calcium ion homeostasis within muscle cells.80,96 Vitamin D regulates the reabsorption and utilization of calcium ions, key signaling molecules for muscle contraction, within muscle cells, ensuring the regular maintenance of muscle function.73
Impact on Mitochondrial Function
The proper functioning of mitochondria is critical for muscle function and strength as they are an essential energy supply center within muscle cells. Vitamin D significantly influences mitochondrial function and metabolism through its unique regulatory mechanisms.97–99 When vitamin D binds to intracellular receptors (VDRs), it activates a series of signaling pathways that regulate mitochondrial production and function.97,98,100 Vitamin D plays a crucial role in maintaining the stability and function of mitochondrial DNA. Mitochondrial DNA encodes vital proteins within the mitochondria, and its integrity is essential for mitochondrial function. Vitamin D facilitates mitochondrial DNA synthesis and repair processes, ensuring accurate transmission of genetic information and functional execution.101
Vitamin D regulates mitochondrial energy metabolism. Mitochondria produce ATP through oxidative phosphorylation, providing essential energy for muscle cells. Studies have shown that vitamin D supplementation significantly improves mitochondrial oxidative phosphorylation in vitamin D-deficient skeletal muscle, increasing the efficiency of mitochondrial energy production.102 Vitamin D deficiency may inhibit mitochondrial energy metabolism, leading to insufficient energy supply to muscle cells and affecting normal muscle function.84,97,98,100 Vitamin D has antioxidant properties that can reduce intracellular oxidative stress, protecting mitochondria from damage.98,100,103 Oxidative stress is typically the result of an imbalance between the overproduction of reactive oxygen species (ROS) and the cell’s antioxidant mechanism. Vitamin D has an antioxidant effect that effectively reduces ROS production and helps maintain mitochondria’s structural and functional integrity.97,102,104,105 Additionally, vitamin D’s metabolic role in skeletal muscle cells may be interrelated with its effect on mitochondrial function. Vitamin D is crucial in maintaining calcium ion homeostasis, which regulates muscle energy metabolism.98,106 Optimizing calcium ion homeostasis enhances the functional state of mitochondria.
Regulation of Immune and Inflammatory Responses
Vitamin D plays a critical role in regulating immune and inflammatory responses. Chronic inflammation exacerbates muscle cell damage and apoptosis in the pathological process of sarcopenia.107 Vitamin D intervention can significantly mitigate this process.108 As a critical immunomodulatory factor, vitamin D regulates the function and activity of a wide range of immune cells by interacting with its receptor (VDR).20,109 In the context of sarcopenia, vitamin D promotes the activity of anti-inflammatory cells, such as regulatory T cells and macrophages, while suppressing the production of inflammatory cells, such as Th17 cells and cytotoxic T cells.20,109 This helps to achieve a dynamic balance in the immune system.
Additionally, vitamin D attenuates the inflammatory response by modulating inflammatory factors released by immune cells. In sarcopenia, chronic inflammation is a significant factor contributing to muscle damage and loss of muscle mass.107 Vitamin D inhibits the production of pro-inflammatory cytokines, such as IFN-γ, IL-1, 6, 12, 18, and TNF-α, which have direct catabolic effects on muscle cells and inhibit muscle protein synthesis.110 Vitamin D effectively alleviates the inflammatory response and reduces the symptoms of sarcopenia by lowering the levels of inflammatory factors. Studies have shown that vitamin D deficiency leads to increased expression of TNFα, matrix metalloproteinase 3 (MMP3), and IL-6 in mouse muscle, further validating the critical role of vitamin D in regulating inflammatory responses.111
Other Mechanisms
In addition to the characteristics above, vitamin D may play a crucial role in the development of sarcopenia by affecting the ratio and transformation of muscle fiber types. Sarcopenia is often characterized by a decrease in fast muscle fibers and a relative increase in slow muscle fibers. Vitamin D regulates the expression of specific genes and related signaling pathways, affecting the muscle fiber type transition process and ultimately impacting muscle function and strength.112–114
Additionally, Vitamin D is involved in regulating apoptosis and autophagy processes in muscle cells. In sarcopenia, increased apoptosis and abnormal autophagy in muscle cells may lead to significant loss of muscle mass. Vitamin D regulates the expression of apoptosis—and autophagy-related genes, which helps maintain the balance between muscle cell survival and death.75,115,116
It also plays a vital role in the repair process after muscle damage. In cases of sarcopenia, the weakened ability of muscle cells to repair damage may lead to a further decline in muscle function. Vitamin D may enhance the repair and regeneration of muscle damage by promoting muscle cell proliferation, differentiation, and migration.117,118
In conclusion, vitamin D exerts its influence on muscle health through a multitude of mechanisms, including the stimulation of muscle protein synthesis, the regulation of muscle cell proliferation and differentiation, the maintenance of mitochondrial function, the modulation of immune and inflammatory responses, and a number of additional mechanisms. Collectively, these mechanisms elucidate the pivotal role of vitamin D in the maintenance of muscle health (Figure 1). However, it is essential to note that these aspects are based on current research and theoretical speculations. Further research and validation are necessary to fully understand vitamin D’s role in the pathogenesis of sarcopenia. The process involves multiple complex signaling pathways and molecular interactions, making it multi-dimensional and intricate.
 |
Figure 1 Mechanisms of vitamin D in the pathogenesis of sarcopenia in the senior people. |
Comprehensive Prevention and Treatment Strategies for Sarcopenia
Nutritional Interventions
Vitamin D is primarily obtained through sun exposure and food consumption. Good sources of vitamin D include cod liver oil, milk, and eggs.119–121 However, the body’s vitamin D production is affected by various factors, such as age, race, skin condition, environmental factors (such as sunlight intensity and latitude), and individual behaviors (such as duration of sun exposure and use of sunscreen).25,37 Due to seasonal, geographic, and dietary constraints, obtaining sufficient vitamin D from food alone is difficult. Therefore, individuals with sarcopenia should take vitamin D supplements in appropriate amounts and under the guidance of a physician or a dietitian.
Numerous studies have demonstrated the beneficial effects of vitamin D on muscle strength and function in the senior people.122–125 Additionally, combined calcium and vitamin D supplementation has been found to improve many muscle strength indicators significantly.126 Randomized controlled trials have confirmed the importance of vitamin D for skeletal muscle function and general health.127 Animal model studies have demonstrated the potential therapeutic benefits of diet and vitamin D supplementation on muscle health.87,128
Therefore, it is essential to adjust the intake of vitamin D individually. The recommended daily intake for adults is generally 400–800 international units (IU).122 However, individuals with severe vitamin D deficiency and those with sarcopenia may require higher doses.18 The senior people, in particular, should consider supplementing with at least 800–1000 IU/day of vitamin D.129 Studies have shown that vitamin D supplementation through food fortification, such as vitamin D-fortified milk, significantly improves vitamin D status.130 This suggests the potential of food sources to enhance muscle health. Double-blind, randomized controlled trials have shown that nutritional interventions targeting the senior people with sarcopenia, such as fortified foods containing 1,000 IU of vitamin D, improve their handgrip strength and stride speed.131 Therefore, proper intake of vitamin D is essential for maintaining muscle health.
In treating sarcopenia, the synergistic effect of other nutrients with vitamin D is equally significant. Protein, an essential building block for muscle growth and repair, works with vitamin D to effectively promote muscle mass.132 Ensuring adequate protein intake is necessary for senior people to maintain muscle mass and function.133,134 Whey protein is a valuable source of high-quality protein due to its ease of digestion and richness in all essential amino acids, particularly leucine, a crucial activator of muscle protein synthesis.135 According to a study by Ottestad et al,136 protein-enriched milk positively impacted the senior people aged 70 years or older with reduced physical strength or mobility, significantly improving their body composition and muscle strength.
Vitamin D and leucine have been shown to have synergistic effects in promoting protein anabolism.137–139 Therefore, combining whey protein with vitamin D supplementation may further improve gait speed in the senior people with sarcopenia.140 It is important to note that the synergistic effects of multiple nutrients, including vitamin D, with protein sources, may produce even more significant results. For instance, a 12–13 week intervention study showed that the senior people with sarcopenia experienced substantial improvements in muscle mass, lower extremity strength, and function when supplemented with vitamin D and leucine-rich whey protein, mainly when adequate protein intake.138,140,141 Furthermore, fortified dairy products have the potential to enhance skeletal muscle health as a nutrient-dense food.142 These dairy products are fortified with vitamin D and rich in protein and various micronutrients, such as vitamin B12, calcium, riboflavin, and zinc, essential for maintaining muscle health and function.143 It is worth noting that normalizing circulating vitamin D concentrations may be a critical factor in the efficacy of protein supplements.124
In nutritional interventions for sarcopenia, it is essential to focus on a balanced intake of nutrients, including calcium and phosphorus, which are crucial in maintaining bone and muscle health.28 Avoiding excessive fat and sugar intake is also necessary, as they may adversely affect muscle health. Therefore, individuals diagnosed with sarcopenia are advised to control their daily fat and sugar intake while increasing their fiber—and vitamin-rich fruits and vegetables to maintain a healthy diet.
Sports Interventions
Resistance exercise,144 low-impact aerobic exercise,145 and balance training146 are recommended for older adults. These activities have been shown to alleviate or improve the symptoms of sarcopenia and enhance overall physical functioning and quality of life in this population.
Currently, there is a lack of safe pharmacological treatments for sarcopenia. Nutritional interventions and exercise training are recognized as effective non-pharmacological therapies, but their exact effects are still under investigation.147 Exercise can effectively stimulate muscle growth and metabolic processes, while nutrition is an indispensable source of energy and raw materials for muscle maintenance and repair. It is essential to replenish energy and nutrients after exercise for optimal muscle repair and growth, particularly for older individuals.
While whey protein, leucine, and vitamin D supplements can promote muscle health without physical activity, combining them with aerobic or resistance training can significantly enhance muscle mass, strength, and functional performance.148–151 Furthermore, physical activity can enhance the effects of branched-chain amino acid (BCAA) and protein supplementation. Muscle proteolysis during exercise releases essential amino acids, promoting protein synthesis.152 Research has demonstrated that the combination of vitamin D and physical activity may have potentially positive effects on muscle function, particularly in the senior people.52 Guidelines for treating sarcopenia recommend incorporating resistance exercise (RE), optimizing protein intake, and addressing vitamin D insufficiency or deficiency.2 However, the optimal way to combine these variables remains unclear. Consuming fortified dairy products after resistance training can help improve muscle strength for the senior people.153 Meta-analyses have shown that maintaining a daily protein intake of 1.2–1.59 g/kg body weight in combination with resistance exercise training positively affects lean body mass and muscle function in the senior people.154 Additionally, studies have found that vitamin D supplementation increases physical activity levels.155
In conclusion, exercise and nutrition have a synergistic effect that effectively prevents and treats sarcopenia, improving the physical fitness and health of the senior people. However, it is essential to note that exercise and nutrition programs should be personalized according to individual differences. Seek guidance from professional health managers or doctors when necessary.
Drug Interventions
Various vitamin D preparations exist, such as calcitriol, alfacalcidol, calcifediol, and eldecalcitol. These medications are typically administered orally, and a combination of individual patient and physician recommendations should determine their exact dosage and use. Vitamin D preparations should be taken regularly over a long period to achieve a stable therapeutic effect. Studies have shown that supplementation with calcitriol156 or eldecalcitol157 can effectively reduce the risk and number of falls in the senior people. Calcifediol is a suitable treatment option for patients with all types of vitamin D deficiency, particularly those with obesity, liver disease, and malabsorption.158 Eldecalcitol, a novel vitamin D analog, has a stronger affinity for vitamin D-binding protein (DBP) and a weaker affinity for the VDR than alfacalcidol. According to a study by Saito et al,159 eldecalcitol positively improved quadriceps and back extensor muscle strength.
However, caution should be exercised regarding the potential side effects of vitamin D supplementation. Despite its numerous benefits, excessive vitamin D intake can also have adverse consequences.160 The most frequent side effect is hypercalcemia, an abnormally high level of calcium in the blood, which can cause digestive symptoms such as nausea, vomiting, and diarrhea and may even result in serious health issues such as kidney stones and heart arrhythmia.161 When supplementing with vitamin D, strictly following your doctor’s or dietitian’s advice is crucial. The dose, frequency, and duration of supplementation should be precisely determined based on factors such as serum (25(OH)D) concentration, patient type, therapeutic conditions, and comorbidities such as obesity and malabsorption syndromes. This will help avoid the risk of overdosage.
Significant progress has been made in the pharmacologic treatment of sarcopenia, in addition to vitamin D preparations. New drugs such as muscle growth factor, anti-sarcopenia protein, and irisin have attracted much attention recently.162–165 These drugs act directly on muscle cells, effectively promoting muscle growth and repair, opening up a new path for sarcopenia treatment. Meanwhile, hormonal drugs and immunosuppressants play a crucial role in treating sarcopenia by regulating the immune system function and reducing the inflammatory response, significantly improving muscle condition.166–168 Studies have also shown that overactivity of the renin-angiotensin system has adverse effects on the neuromusculoskeletal and cardiovascular systems. The combination of angiotensin-converting enzyme inhibitors and vitamin D has positively impacted physical and cognitive function, making it an effective strategy for treating sarcopenia in the senior people.169 However, the use of these drugs requires strict management of indications and contraindications to avoid potential risks.
In conclusion, a combined prevention and treatment strategy involving vitamin D, in isolation or in combination with exercise and medication, is of significant importance in the management of sarcopenia. This approach can effectively enhance the muscle status and quality of life of patients with sarcopenia (Table 2).
 |
Table 2 Effectiveness of Vitamin D Alone and in Combination with Other Interventions |
Outlook for Future Research Directions
Molecular Mechanisms of Vitamin D in Sarcopenia
Future research should investigate the specific molecular mechanisms of vitamin D in sarcopenia, including its effects on muscle cell growth, differentiation, function, and protein synthesis and degradation. Elucidating these mechanisms will enhance our understanding of the therapeutic potential of vitamin D in sarcopenia.
Study of Genes Associated with Vitamin D and Sarcopenia
Genes play an essential role in the pathogenesis and treatment of sarcopenia. Future studies can further explore the interactions between vitamin D and sarcopenia-related genes, such as the relationship between vitamin D receptor gene polymorphisms and sarcopenia. This will help to reveal the genetic basis of sarcopenia and provide a theoretical basis for the development of targeted therapies.
Large-Scale Clinical Trials
In addition to the need for further verification of the therapeutic effects of vitamin D supplementation in sarcopenia due to the small sample sizes of previous studies, it is also essential to consider the potential benefits of vitamin D in other conditions related to muscle health. Given the possible role of vitamin D in muscle health, it is crucial to conduct future large-scale, multicenter clinical trials to assess vitamin D’s efficacy and safety in treating sarcopenia.
Research on Special Populations
The existing research on vitamin D and sarcopenia has predominantly concentrated on the general population, overlooking the specific needs and responses of special populations such as the senior people, chronically ill, and bedridden individuals. These unique populations may have distinct physical conditions that could influence their requirements for vitamin D. Consequently; future research must prioritize investigating vitamin D’s effects on these particular populations to develop more tailored treatment options that address their specific circumstances.
Combination of Vitamin D with Other Nutrients or Drugs
Vitamin D may have synergistic effects with other nutrients or drugs in the treatment of sarcopenia. Future studies could explore the impact of combining vitamin D with nutrients such as proteins, calcium, and antioxidants and the interactions between vitamin D and drugs such as hormones and immunosuppressants. Healthcare professionals can develop more effective and personalized treatment approaches for sarcopenia and related conditions by understanding how vitamin D interacts with various nutrients and drugs.
Prospects and Challenges for Clinical Applications
The clinical application of vitamin D to treat sarcopenia is promising despite challenges. Determining the appropriate dosage of vitamin D supplementation and avoiding side effects associated with excessive intake are important considerations. Additionally, the duration of supplementation is an essential aspect to consider in the clinical application of vitamin D for sarcopenia. Furthermore, it is essential for future research to explore the potential synergistic effects of vitamin D supplementation with other interventions, such as exercise or specific dietary modifications. Future studies will undoubtedly advance the clinical application of vitamin D in the treatment of sarcopenia by addressing practical issues and providing specific solutions and recommendations.
In summary, many unanswered questions regarding the relationship between vitamin D and sarcopenia still require further exploration. By conducting in-depth research on its molecular mechanism, gene action, large-scale clinical trials, and studies on special populations, we can establish a more robust scientific basis for treating sarcopenia. Focusing on the prospects and challenges of clinical applications will help translate research results into practical treatment programs, improving the quality of life for patients with sarcopenia.
Conclusion
In conclusion, there is a robust correlation between vitamin D and sarcopenia in older adults, with existing studies providing varying degrees of support for this association. Vitamin D, a crucial fat-soluble vitamin, plays a pivotal role in calcium and phosphorus metabolism and the maintenance of bone health. Additionally, it is instrumental in muscle growth and functional maintenance. A comprehensive analysis of existing studies revealed that vitamin D deficiency represents a significant risk factor for sarcopenia in older adults. The majority of studies have demonstrated a significant correlation between low vitamin D levels and the prevalence of sarcopenia. Vitamin D supplementation has also been shown to enhance muscle strength and function. Despite differences in sample selection, diagnostic criteria, and definition of vitamin D deficiency across studies, the overall trend suggests a potential role for vitamin D in the prevention and management of sarcopenia. Additionally, vitamin D affects muscle health through various mechanisms, including promoting muscle protein synthesis, regulating muscle cell proliferation and differentiation, maintaining mitochondrial function, and modulation of immune and inflammatory responses. These mechanisms collectively elucidate vitamin D’s crucial role in maintaining muscle health.
A comprehensive approach to preventing and treating sarcopenia should encompass nutritional interventions, exercise, and pharmacological agents. Senior people need to consume a reasonable amount of vitamin D, which plays a significant role in nutritional intervention. It is also imperative to underscore the necessity of appropriate exercise and pharmacological treatment programs for senior people. These strategies have been demonstrated to improve muscle status and enhance quality of life in patients with sarcopenia. Further research is required to elucidate the precise mechanism of action of vitamin D in sarcopenia. Additionally, large-scale, multicenter clinical trials are necessary to confirm the efficacy and safety of vitamin D supplementation in treating sarcopenia. Furthermore, it is essential to consider the vitamin D requirements and intervention effects in specific populations, such as patients with chronic diseases and bedridden individuals, to develop more personalized and precise treatment plans.
In conclusion, the relationship between vitamin D and sarcopenia is of significant scientific and practical importance. Further research in this area and the development of comprehensive prevention and treatment strategies can devise new ideas and methods for preventing and treating sarcopenia, thus improving seniors’ overall health and quality of life.
Acknowledgments
The authors wish to thank all hands and minds involved in this review.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Key Talents Project of Changzhou Third People’s Hospital.
Disclosure
The authors declare no conflicts of interest in this study.
References
1. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393(10191):2636–2646. doi:10.1016/S0140-6736(19)31138-9
2. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
3. Larsson L, Degens H, Li M, et al. Sarcopenia: aging-related loss of muscle mass and function. Physiol Rev. 2019;99(1):427–511. doi:10.1152/physrev.00061.2017
4. Cruz-Jentoft AJ, Landi F, Topinková E, Michel JP. Understanding sarcopenia as a geriatric syndrome. Curr Opin Clin Nutr Metab Care. 2010;13(1):1–7. doi:10.1097/MCO.0b013e328333c1c1
5. Landi F, Calvani R, Cesari M, et al. Sarcopenia as the biological substrate of physical frailty. Clin Geriatr Med. 2015;31(3):367–374. doi:10.1016/j.cger.2015.04.005
6. Sobestiansky S, Michaelsson K, Cederholm T. Sarcopenia prevalence and associations with mortality and hospitalisation by various sarcopenia definitions in 85-89 year old community-dwelling men: a report from the ULSAM study. BMC Geriatr. 2019;19(1):318. doi:10.1186/s12877-019-1338-1
7. Yeung SSY, Reijnierse EM, Pham VK, et al. Sarcopenia and its association with falls and fractures in older adults: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2019;10(3):485–500. doi:10.1002/jcsm.12411
8. Xu J, Wan CS, Ktoris K, Reijnierse EM, Maier AB. Sarcopenia Is associated with mortality in adults: a systematic review and meta-analysis. Gerontology. 2022;68(4):361–376. doi:10.1159/000517099
9. Reiss J, Iglseder B, Alzner R, et al. Consequences of applying the new EWGSOP2 guideline instead of the former EWGSOP guideline for sarcopenia case finding in older patients. Age Ageing. 2019;48(5):719–724. doi:10.1093/ageing/afz035
10. Locquet M, Beaudart C, Petermans J, Reginster JY, Bruyère O. EWGSOP2 Versus EWGSOP1: impact on the prevalence of sarcopenia and its major health consequences. J Am Med Dir Assoc. 2019;20(3):384–385. doi:10.1016/j.jamda.2018.11.027
11. von Haehling S, Morley JE, Anker SD. An overview of sarcopenia: facts and numbers on prevalence and clinical impact. J Cachexia Sarcopenia Muscle. 2010;1(2):129–133. doi:10.1007/s13539-010-0014-2
12. Wojzischke J, van Wijngaarden J, van den Berg C, et al. Nutritional status and functionality in geriatric rehabilitation patients: a systematic review and meta-analysis. Eur Geriatr Med. 2020;11(2):195–207. doi:10.1007/s41999-020-00294-2
13. Ligthart-Melis GC, Luiking YC, Kakourou A, Cederholm T, Maier AB, de van der Schueren MAE. Frailty, sarcopenia, and malnutrition frequently (Co-)occur in hospitalized older adults: a systematic review and meta-analysis. J Am Med Dir Assoc. 2020;21(9):1216–1228. doi:10.1016/j.jamda.2020.03.006
14. Walston JD. Sarcopenia in older adults. Curr Opin Rheumatol. 2012;24(6):623–627. doi:10.1097/BOR.0b013e328358d59b
15. Robinson SM, Reginster JY, Rizzoli R, et al. Does nutrition play a role in the prevention and management of sarcopenia? Clin Nutr. 2018;37(4):1121–1132. doi:10.1016/j.clnu.2017.08.016
16. Yuan S, Larsson SC. Epidemiology of sarcopenia: prevalence, risk factors, and consequences. Metabolism. 2023;144:155533. doi:10.1016/j.metabol.2023.155533
17. Gil Á, Plaza-Diaz J, Mesa MD. Vitamin D: classic and novel actions. Ann Nutr Metab. 2018;72(2):87–95. doi:10.1159/000486536
18. Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266–281. doi:10.1056/NEJMra070553
19. Bouillon R, Marcocci C, Carmeliet G, et al. Skeletal and extraskeletal actions of vitamin d: current evidence and outstanding questions. Endocr Rev. 2019;40(4):1109–1151. doi:10.1210/er.2018-00126
20. Charoenngam N, Holick MF. Immunologic effects of vitamin D on human health and disease. Nutrients. 2020;12(7):2097. doi:10.3390/nu12072097
21. Tripkovic L, Lambert H, Hart K, et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: a systematic review and meta-analysis. Am J Clin Nutr. 2012;95(6):1357–1364. doi:10.3945/ajcn.111.031070
22. Zhang RH, He DH, Zhou B, et al. Analysis of vitamin D status in men highly exposed to sunlight. Biomed Environ Sci. 2015;28(12):913–916. doi:10.3967/bes2015.125
23. Ponchon G, Kennan AL, DeLuca HF. “Activation” of vitamin D by the liver. J Clin Invest. 1969;48(11):2032–2037. doi:10.1172/JCI106168
24. Nykjaer A, Dragun D, Walther D, et al. An endocytic pathway essential for renal uptake and activation of the steroid 25-(OH) vitamin D3. Cell. 1999;96(4):507–515. doi:10.1016/S0092-8674(00)80655-8
25. Girgis CM, Clifton-Bligh RJ, Hamrick MW, Holick MF, Gunton JE. The roles of vitamin D in skeletal muscle: form, function, and metabolism. Endocr Rev. 2013;34(1):33–83. doi:10.1210/er.2012-1012
26. Dzik KP, Kaczor JJ. Mechanisms of vitamin D on skeletal muscle function: oxidative stress, energy metabolism and anabolic state. Eur J Appl Physiol. 2019;119(4):825–839. doi:10.1007/s00421-019-04104-x
27. Shimizu Y, Kim H, Yoshida H, Shimada H, Suzuki T. Serum 25-hydroxyvitamin D level and risk of falls in Japanese community-dwelling elderly women: a 1-year follow-up study. Osteoporos Int. 2015;26(8):2185–2192. doi:10.1007/s00198-015-3130-1
28. Giustina A, Bouillon R, Dawson-Hughes B, et al. Vitamin D in the older population: a consensus statement. Endocrine. 2023;79(1):31–44. doi:10.1007/s12020-022-03208-3
29. Boettger SF, Angersbach B, Klimek CN, et al. Prevalence and predictors of vitamin D-deficiency in frail older hospitalized patients. BMC Geriatr. 2018;18(1):219. doi:10.1186/s12877-018-0919-8
30. Verlaan S, Aspray TJ, Bauer JM, et al. Nutritional status, body composition, and quality of life in community-dwelling sarcopenic and non-sarcopenic older adults: a case-control study. Clin Nutr. 2017;36(1):267–274. doi:10.1016/j.clnu.2015.11.013
31. Alagöl F, Shihadeh Y, Boztepe H, et al. Sunlight exposure and vitamin D deficiency in Turkish women. J Endocrinol Invest. 2000;23(3):173–177. doi:10.1007/BF03343702
32. Loomis WF. Skin-pigment regulation of vitamin-D biosynthesis in man. Science. 1967;157(3788):501–506. doi:10.1126/science.157.3788.501
33. Zakharova I, Klimov L, Kuryaninova V, et al. Vitamin D insufficiency in overweight and obese children and adolescents. Front Endocrinol. 2019;10:103. doi:10.3389/fendo.2019.00103
34. MacLaughlin J, Holick MF. Aging decreases the capacity of human skin to produce vitamin D3. J Clin Invest. 1985;76(4):1536–1538. doi:10.1172/JCI112134
35. Lips P, Bilezikian JP, Bouillon RVD. Giveth to Those Who Needeth. JBMR Plus. 2020;4(1):e10232. doi:10.1002/jbm4.10232
36. Cashman KD. Vitamin D deficiency: defining, prevalence, causes, and strategies of addressing. Calcif Tissue Int. 2020;106(1):14–29. doi:10.1007/s00223-019-00559-4
37. Bischoff-Ferrari HA, Borchers M, Gudat F, Dürmüller U, Stähelin HB, Dick W. Vitamin D receptor expression in human muscle tissue decreases with age. J Bone Miner Res. 2004;19(2):265–269. doi:10.1359/jbmr.2004.19.2.265
38. Si Y, Kazamel M, Kwon Y, et al. The vitamin D activator CYP27B1 is upregulated in muscle fibers in denervating disease and can track progression in amyotrophic lateral sclerosis. J Steroid Biochem Mol Biol. 2020;200:105650. doi:10.1016/j.jsbmb.2020.105650
39. Malczewska-Lenczowska J, Sitkowski D, Surała O, Orysiak J, Szczepańska B, Witek K. The association between iron and vitamin D status in female elite athletes. Nutrients. 2018;10(2):167. doi:10.3390/nu10020167
40. Atkinson MA, Melamed ML, Kumar J, et al. Vitamin D, race, and risk for anemia in children. J Pediatr. 2014;164(1):153–158.e151. doi:10.1016/j.jpeds.2013.08.060
41. Perlstein TS, Pande R, Berliner N, Vanasse GJ. Prevalence of 25-hydroxyvitamin D deficiency in subgroups of elderly persons with anemia: association with anemia of inflammation. Blood. 2011;117(10):2800–2806. doi:10.1182/blood-2010-09-309708
42. Houston DK, Cesari M, Ferrucci L, et al. Association between vitamin D status and physical performance: the InCHIANTI study. J Gerontol a Biol Sci Med Sci. 2007;62(4):440–446. doi:10.1093/gerona/62.4.440
43. Janssen HC, Emmelot-Vonk MH, Verhaar HJ, van der Schouw YT. Vitamin D and muscle function: is there a threshold in the relation? J Am Med Dir Assoc. 2013;14(8):627.e613–628. doi:10.1016/j.jamda.2013.05.012
44. Mizuno T, Hosoyama T, Tomida M, et al. Influence of vitamin D on sarcopenia pathophysiology: a longitudinal study in humans and basic research in knockout mice. J Cachexia Sarcopenia Muscle. 2022;13(6):2961–2973. doi:10.1002/jcsm.13102
45. Orces CH. Prevalence of clinically relevant muscle weakness and its association with vitamin D status among older adults in Ecuador. Aging Clin Exp Res. 2017;29(5):943–949. doi:10.1007/s40520-016-0678-3
46. Wang J, Wang X, Gu Y, et al. Vitamin D is related to handgrip strength in adult men aged 50 years and over: a population study from the TCLSIH cohort study. Clin Endocrinol. 2019;90(5):753–765. doi:10.1111/cen.13952
47. Mendoza-Garcés L, Velázquez-Alva MC, Cabrer-Rosales MF, Arrieta-Cruz I, Gutiérrez-Juárez R, Irigoyen-Camacho ME. Vitamin D deficiency is associated with handgrip strength, nutritional status and T2DM in community-dwelling older Mexican women: a cross-sectional study. Nutrients. 2021;13(3). doi:10.3390/nu13030736
48. Iolascon G, de Sire A, Calafiore D, Moretti A, Gimigliano R, Gimigliano F. Hypovitaminosis D is associated with a reduction in upper and lower limb muscle strength and physical performance in post-menopausal women: a retrospective study. Aging Clin Exp Res. 2015;27(1):S23–30. doi:10.1007/s40520-015-0405-5
49. Levinger P, Begg R, Sanders KM, et al. The effect of vitamin D status on pain, lower limb strength and knee function during balance recovery in people with knee osteoarthritis: an exploratory study. Arch Osteoporos. 2017;12(1):83. doi:10.1007/s11657-017-0378-4
50. Aspell N, Laird E, Healy M, Lawlor B, O’Sullivan M. Vitamin D deficiency is associated with impaired muscle strength and physical performance in community-dwelling older adults: findings from the English longitudinal study of ageing. Clin Interv Aging. 2019;14:1751–1761. doi:10.2147/CIA.S222143
51. Ceglia L. Vitamin D and its role in skeletal muscle. Curr Opin Clin Nutr Metab Care. 2009;12(6):628–633. doi:10.1097/MCO.0b013e328331c707
52. Yang A, Lv Q, Chen F, et al. The effect of vitamin D on sarcopenia depends on the level of physical activity in older adults. J Cachexia Sarcopenia Muscle. 2020;11(3):678–689. doi:10.1002/jcsm.12545
53. Bang WS, Lee DH, Kim KT, et al. Relationships between vitamin D and paraspinal muscle: human data and experimental rat model analysis. Spine J. 2018;18(6):1053–1061. doi:10.1016/j.spinee.2018.01.007
54. Scott D, Blizzard L, Fell J, Ding C, Winzenberg T, Jones G. A prospective study of the associations between 25-hydroxy-vitamin D, sarcopenia progression and physical activity in older adults. Clin Endocrinol. 2010;73(5):581–587. doi:10.1111/j.1365-2265.2010.03858.x
55. Houston DK, Tooze JA, Hausman DB, et al. Change in 25-hydroxyvitamin D and physical performance in older adults. J Gerontol a Biol Sci Med Sci. 2011;66(4):430–436. doi:10.1093/gerona/glq235
56. Yang C, Dai Y, Li Z, Peng Y, Zhang L, Jia H. Relationship of Serum 25-hydroxyvitamin d levels with sarcopenia and body composition in community-dwelling older adults: a paired case-control study. J Am Med Dir Assoc. 2023;24(8):1213–1219. doi:10.1016/j.jamda.2023.06.004
57. Conzade R, Grill E, Bischoff-Ferrari HA, et al. Vitamin D in relation to incident sarcopenia and changes in muscle parameters among older adults: the KORA-Age study. Calcif Tissue Int. 2019;105(2):173–182. doi:10.1007/s00223-019-00558-5
58. Luo S, Chen X, Hou L, et al. The relationship between sarcopenia and vitamin D levels in adults of different ethnicities: findings from the west China health and aging trend study. J Nutr Health Aging. 2021;25(7):909–913. doi:10.1007/s12603-021-1645-z
59. Lawongsa K, Tepakorn J. Sarcopenia prevalence and risk factors among older adults in Bangkok, Thailand: a cross-sectional study. Cureus. 2024;16(6):e63483. doi:10.7759/cureus.63483
60. Kim MK, Baek KH, Song KH, et al. Vitamin D deficiency is associated with sarcopenia in older Koreans, regardless of obesity: the Fourth Korea national health and nutrition examination surveys (KNHANES IV) 2009. J Clin Endocrinol Metab. 2011;96(10):3250–3256. doi:10.1210/jc.2011-1602
61. Kim SH, Kwon HS, Hwang HJ. White blood cell counts, insulin resistance, vitamin D levels and sarcopenia in Korean elderly men. Scand J Clin Lab Invest. 2017;77(3):228–233. doi:10.1080/00365513.2017.1293286
62. Lee JH, Kim S, Kim MK, et al. Relationships between 25(OH)D concentration, sarcopenia and HOMA-IR in postmenopausal Korean women. Climacteric. 2018;21(1):40–46. doi:10.1080/13697137.2017.1395410
63. Park S, Ham JO, Lee BK. A positive association of vitamin D deficiency and sarcopenia in 50 year old women, but not men. Clin Nutr. 2014;33(5):900–905. doi:10.1016/j.clnu.2013.09.016
64. Hori M, Takahashi H, Kondo C, et al. Association between Serum 25-Hydroxyvitamin D Levels and Sarcopenia in Patients Undergoing Chronic Haemodialysis. Am J Nephrol. 2024;55(3):399–405. doi:10.1159/000536582
65. Hsu YT, Lin JY, Lin CJ, Lee YJ, Chang WH. Association of possible sarcopenia or sarcopenia with body composition, nutritional intakes, serum vitamin D levels, and physical activity among patients with type 2 diabetes mellitus in Taiwan. Nutrients. 2023;15(18). doi:10.3390/nu15183892
66. Saeki C, Kanai T, Nakano M, et al. Low serum 25-hydroxyvitamin D levels are related to frailty and sarcopenia in patients with chronic liver disease. Nutrients. 2020;12(12):3810. doi:10.3390/nu12123810
67. Okubo T, Atsukawa M, Tsubota A, et al. Relationship between serum vitamin D level and sarcopenia in chronic liver disease. Hepatol Res. 2020;50(5):588–597. doi:10.1111/hepr.13485
68. Minamino H, Katsushima M, Torii M, et al. Serum vitamin D status inversely associates with a prevalence of severe sarcopenia among female patients with rheumatoid arthritis. Sci Rep. 2021;11(1):20485. doi:10.1038/s41598-021-99894-6
69. Laubscher CV, Burger MC, Conradie MM, Conradie M, Jordaan JD. Prevalence of sarcopenia in older south African patients following surgery for fragility fractures of the Hip. Geriatr Orthop Surg Rehabil. 2020;11:2151459320971560. doi:10.1177/2151459320971560
70. Alvarez Mejía M, Marulanda Mejía F, González Correa CH, Restrepo Valencia CA, Gómez Tobón P, Chacón JA. Relationship between hypovitaminosis D and sarcopenia in patients with stage 3 and 4 chronic kidney disease in Colombian patients. Clin Nutr ESPEN. 2023;57:519–526. doi:10.1016/j.clnesp.2023.06.022
71. Gielen E, O’Neill TW, Pye SR, et al. Endocrine determinants of incident sarcopenia in middle-aged and elderly European men. J Cachexia Sarcopenia Muscle. 2015;6(3):242–252. doi:10.1002/jcsm.12030
72. Umakanthan M, Li JW, Sud K, et al. Prevalence and factors associated with sarcopenia in patients on maintenance dialysis in Australia-A single centre, cross-sectional study. Nutrients. 2021;13(9):3284. doi:10.3390/nu13093284
73. Girgis CM, Cha KM, So B, et al. Mice with myocyte deletion of vitamin D receptor have sarcopenia and impaired muscle function. J Cachexia Sarcopenia Muscle. 2019;10(6):1228–1240. doi:10.1002/jcsm.12460
74. Gogulothu R, Nagar D, Gopalakrishnan S, Garlapati VR, Kallamadi PR, Ismail A. Disrupted expression of genes essential for skeletal muscle fibre integrity and energy metabolism in Vitamin D deficient rats. J Steroid Biochem Mol Biol. 2020;197:105525. doi:10.1016/j.jsbmb.2019.105525
75. Srikuea R, Hirunsai M, Charoenphandhu N. Regulation of vitamin D system in skeletal muscle and resident myogenic stem cell during development, maturation, and ageing. Sci Rep. 2020;10(1):8239. doi:10.1038/s41598-020-65067-0
76. Bass JJ, Nakhuda A, Deane CS, et al. Overexpression of the vitamin D receptor (VDR) induces skeletal muscle hypertrophy. Mol Metab. 2020;42:101059. doi:10.1016/j.molmet.2020.101059
77. Okuno H, Kishimoto KN, Hatori M, Itoi E. 1α,25-dihydroxyvitamin D₃ enhances fast-myosin heavy chain expression in differentiated C2C12 myoblasts. Cell Biol Int. 2012;36(5):441–447. doi:10.1042/CBI20100782
78. Hosoyama T, Iida H, Kawai-Takaishi M, Watanabe K. Vitamin D inhibits myogenic cell fusion and expression of fusogenic genes. Nutrients. 2020;12(8):2192. doi:10.3390/nu12082192
79. Chanet A, Salles J, Guillet C, et al. Vitamin D supplementation restores the blunted muscle protein synthesis response in deficient old rats through an impact on ectopic fat deposition. J Nutr Biochem. 2017;46:30–38. doi:10.1016/j.jnutbio.2017.02.024
80. Ceglia L, Harris SS. Vitamin D and its role in skeletal muscle. Calcif Tissue Int. 2013;92(2):151–162. doi:10.1007/s00223-012-9645-y
81. Zeitz U, Weber K, Soegiarto DW, Wolf E, Balling R, Erben RG. Impaired insulin secretory capacity in mice lacking a functional vitamin D receptor. FASEB j. 2003;17(3):509–511. doi:10.1096/fj.02-0424fje
82. Narvaez CJ, Matthews D, Broun E, Chan M, Welsh J. Lean phenotype and resistance to diet-induced obesity in vitamin D receptor knockout mice correlates with induction of uncoupling protein-1 in white adipose tissue. Endocrinology. 2009;150(2):651–661. doi:10.1210/en.2008-1118
83. Benetti E, Mastrocola R, Chiazza F, et al. Effects of vitamin D on insulin resistance and myosteatosis in diet-induced obese mice. PLoS One. 2018;13(1):e0189707. doi:10.1371/journal.pone.0189707
84. Romeu Montenegro K, Carlessi R, Cruzat V, Newsholme P. Effects of vitamin D on primary human skeletal muscle cell proliferation, differentiation, protein synthesis and bioenergetics. J Steroid Biochem Mol Biol. 2019;193:105423. doi:10.1016/j.jsbmb.2019.105423
85. Bhat M, Ismail A. Vitamin D treatment protects against and reverses oxidative stress induced muscle proteolysis. J Steroid Biochem Mol Biol. 2015;152:171–179. doi:10.1016/j.jsbmb.2015.05.012
86. Hirose Y, Onishi T, Miura S, Hatazawa Y, Kamei Y. Vitamin D attenuates FOXO1-target atrophy gene expression in C2C12 muscle cells. J Nutr Sci Vitaminol. 2018;64(3):229–232. doi:10.3177/jnsv.64.229
87. Cheung WW, Hao S, Wang Z, et al. Vitamin D repletion ameliorates adipose tissue browning and muscle wasting in infantile nephropathic cystinosis-associated cachexia. J Cachexia Sarcopenia Muscle. 2020;11(1):120–134. doi:10.1002/jcsm.12497
88. Garcia LA, King KK, Ferrini MG, Norris KC, Artaza JN. 1,25(OH)2vitamin D3 stimulates myogenic differentiation by inhibiting cell proliferation and modulating the expression of promyogenic growth factors and myostatin in C2C12 skeletal muscle cells. Endocrinology. 2011;152(8):2976–2986. doi:10.1210/en.2011-0159
89. Haegens A, Schols AM, van Essen AL, van Loon LJ, Langen RC. Leucine induces myofibrillar protein accretion in cultured skeletal muscle through mTOR dependent and -independent control of myosin heavy chain mRNA levels. Mol Nutr Food Res. 2012;56(5):741–752. doi:10.1002/mnfr.201100695
90. Olsson K, Saini A, Strömberg A, et al. Evidence for Vitamin D receptor expression and direct effects of 1α,25(OH)2D3 in human skeletal muscle precursor cells. Endocrinology. 2016;157(1):98–111. doi:10.1210/en.2015-1685
91. Umesono K, Murakami KK, Thompson CC, Evans RM. Direct repeats as selective response elements for the thyroid hormone, retinoic acid, and vitamin D3 receptors. Cell. 1991;65(7):1255–1266. doi:10.1016/0092-8674(91)90020-Y
92. Carlberg C, Bendik I, Wyss A, et al. Two nuclear signalling pathways for vitamin D. Nature. 1993;361(6413):657–660. doi:10.1038/361657a0
93. Carlberg C, Campbell MJ. Vitamin D receptor signaling mechanisms: integrated actions of a well-defined transcription factor. Steroids. 2013;78(2):127–136. doi:10.1016/j.steroids.2012.10.019
94. Braga M, Simmons Z, Norris KC, Ferrini MG, Artaza JN. Vitamin D induces myogenic differentiation in skeletal muscle derived stem cells. Endocr Connect. 2017;6(3):139–150. doi:10.1530/EC-17-0008
95. Talib NF, Zhu Z, Kim KS. Vitamin D3 Exerts Beneficial Effects on C2C12 myotubes through activation of the vitamin D Receptor (VDR)/Sirtuins (SIRT)1/3 Axis. Nutrients. 2023;15(22):4714. doi:10.3390/nu15224714
96. Girgis CM, Cha KM, Houweling PJ, et al. Vitamin D receptor ablation and vitamin D deficiency result in reduced grip strength, altered muscle fibers, and increased myostatin in mice. Calcif Tissue Int. 2015;97(6):602–610. doi:10.1007/s00223-015-0054-x
97. Ryan ZC, Craig TA, Folmes CD, et al. 1α,25-Dihydroxyvitamin D3 regulates mitochondrial oxygen consumption and dynamics in human skeletal muscle cells. J Biol Chem. 2016;291(3):1514–1528. doi:10.1074/jbc.M115.684399
98. Ashcroft SP, Bass JJ, Kazi AA, Atherton PJ, Philp A. The vitamin D receptor regulates mitochondrial function in C2C12 myoblasts. Am J Physiol Cell Physiol. 2020;318(3):C536–c541. doi:10.1152/ajpcell.00568.2019
99. Salles J, Chanet A, Guillet C, et al. Vitamin D status modulates mitochondrial oxidative capacities in skeletal muscle: role in sarcopenia. Commun Biol. 2022;5(1):1288.
100. Schnell DM, Walton RG, Vekaria HJ, et al. Vitamin D produces a perilipin 2-dependent increase in mitochondrial function in C2C12 myotubes. J Nutr Biochem. 2019;65:83–92. doi:10.1016/j.jnutbio.2018.11.002
101. Latham CM, Brightwell CR, Keeble AR, et al. Vitamin D promotes skeletal muscle regeneration and mitochondrial health. Front Physiol. 2021;12:660498. doi:10.3389/fphys.2021.660498
102. Sinha A, Hollingsworth KG, Ball S, Cheetham T. Improving the vitamin D status of vitamin D deficient adults is associated with improved mitochondrial oxidative function in skeletal muscle. J Clin Endocrinol Metab. 2013;98(3):E509–513. doi:10.1210/jc.2012-3592
103. Ashcroft SP, Fletcher G, Philp AM, et al. Diet-induced vitamin D deficiency reduces skeletal muscle mitochondrial respiration. J Endocrinol. 2021;249(2):113–124. doi:10.1530/JOE-20-0233
104. Dzik K, Skrobot W, Flis DJ, et al. Vitamin D supplementation attenuates oxidative stress in paraspinal skeletal muscles in patients with low back pain. Eur J Appl Physiol. 2018;118(1):143–151. doi:10.1007/s00421-017-3755-1
105. Coen PM, Musci RV, Hinkley JM, Miller BF. Mitochondria as a target for mitigating sarcopenia. Front Physiol. 2018;9:1883. doi:10.3389/fphys.2018.01883
106. Ricca C, Aillon A, Bergandi L, Alotto D, Castagnoli C, Silvagno F. Vitamin D receptor is necessary for mitochondrial function and cell health. Int J Mol Sci. 2018;19(6):1672. doi:10.3390/ijms19061672
107. Jimenez-Gutierrez GE, Martínez-Gómez LE, Martínez-Armenta C, Pineda C, Martínez-Nava GA, Lopez-Reyes A. Molecular mechanisms of inflammation in sarcopenia: diagnosis and therapeutic update. Cells. 2022;11(15):2359. doi:10.3390/cells11152359
108. Calton EK, Keane KN, Newsholme P, Soares MJ. The impact of vitamin D levels on inflammatory status: a systematic review of immune cell studies. PLoS One. 2015;10(11):e0141770. doi:10.1371/journal.pone.0141770
109. Carlberg C, Velleuer E. Vitamin D and Aging: central Role of Immunocompetence. Nutrients. 2024;16(3):398. doi:10.3390/nu16030398
110. Bhol NK, Bhanjadeo MM, Singh AK, et al. The interplay between cytokines, inflammation, and antioxidants: mechanistic insights and therapeutic potentials of various antioxidants and anti-cytokine compounds. Biomed Pharmacother. 2024;178:117177. doi:10.1016/j.biopha.2024.117177
111. Yu S, Ren B, Chen H, Goltzman D, Yan J, Miao D. 1,25-Dihydroxyvitamin D deficiency induces sarcopenia by inducing skeletal muscle cell senescence. Am J Transl Res. 2021;13(11):12638–12649.
112. Koundourakis NE, Avgoustinaki PD, Malliaraki N, Margioris AN. Muscular effects of vitamin D in young athletes and non-athletes and in the elderly. Hormones. 2016;15(4):471–488. doi:10.14310/horm.2002.1705
113. Tanganelli F, Meinke P, Hofmeister F, et al. Type-2 muscle fiber atrophy is associated with sarcopenia in elderly men with Hip fracture. Exp Gerontol. 2021;144:111171. doi:10.1016/j.exger.2020.111171
114. Reis NG, Assis AP, Lautherbach N, et al. Maternal vitamin D deficiency affects the morphology and function of glycolytic muscle in adult offspring rats. J Cachexia Sarcopenia Muscle. 2022;13(4):2175–2187. doi:10.1002/jcsm.12986
115. Bass JJ, Kazi AA, Deane CS, et al. The mechanisms of skeletal muscle atrophy in response to transient knockdown of the vitamin D receptor in vivo. J Physiol. 2021;599(3):963–979. doi:10.1113/JP280652
116. Stratos I, Li Z, Herlyn P, et al. Vitamin D increases cellular turnover and functionally restores the skeletal muscle after crush injury in rats. Am J Pathol. 2013;182(3):895–904. doi:10.1016/j.ajpath.2012.11.006
117. Owens DJ, Sharples AP, Polydorou I, et al. A systems-based investigation into vitamin D and skeletal muscle repair, regeneration, and hypertrophy. Am J Physiol Endocrinol Metab. 2015;309(12):E1019–1031. doi:10.1152/ajpendo.00375.2015
118. Barker T, Henriksen VT, Martins TB, et al. Higher serum 25-hydroxyvitamin D concentrations associate with a faster recovery of skeletal muscle strength after muscular injury. Nutrients. 2013;5(4):1253–1275. doi:10.3390/nu5041253
119. Schmid A, Walther B. Natural vitamin D content in animal products. Adv Nutr. 2013;4(4):453–462. doi:10.3945/an.113.003780
120. Crowe FL, Steur M, Allen NE, Appleby PN, Travis RC, Key TJ. Plasma concentrations of 25-hydroxyvitamin D in meat eaters, fish eaters, vegetarians and vegans: results from the EPIC-Oxford study. Public Health Nutr. 2011;14(2):340–346. doi:10.1017/S1368980010002454
121. Dunlop E, James AP, Cunningham J, et al. Vitamin D composition of Australian foods. Food Chem. 2021;358:129836. doi:10.1016/j.foodchem.2021.129836
122. Pfeifer M, Begerow B, Minne HW, Suppan K, Fahrleitner-Pammer A, Dobnig H. Effects of a long-term vitamin D and calcium supplementation on falls and parameters of muscle function in community-dwelling older individuals. Osteoporos Int. 2009;20(2):315–322. doi:10.1007/s00198-008-0662-7
123. Iolascon G, Moretti A, de Sire A, Calafiore D, Gimigliano F. Effectiveness of calcifediol in improving muscle function in post-menopausal women: a prospective cohort study. Adv Ther. 2017;34(3):744–752. doi:10.1007/s12325-017-0492-0
124. Verlaan S, Maier AB, Bauer JM, et al. Sufficient levels of 25-hydroxyvitamin D and protein intake required to increase muscle mass in sarcopenic older adults - The PROVIDE study. Clin Nutr. 2018;37(2):551–557. doi:10.1016/j.clnu.2017.01.005
125. El Hajj C, Fares S, Chardigny JM, Boirie Y, Walrand S. Vitamin D supplementation and muscle strength in pre-sarcopenic elderly Lebanese people: a randomized controlled trial. Arch Osteoporos. 2018;14(1):4. doi:10.1007/s11657-018-0553-2
126. Muir SW, Montero-Odasso M. Effect of vitamin D supplementation on muscle strength, gait and balance in older adults: a systematic review and meta-analysis. J Am Geriatr Soc. 2011;59(12):2291–2300. doi:10.1111/j.1532-5415.2011.03733.x
127. Chiang CM, Ismaeel A, Griffis RB, Weems S. Effects of Vitamin D supplementation on muscle strength in athletes: a systematic review. J Strength Cond Res. 2017;31(2):566–574. doi:10.1519/JSC.0000000000001518
128. Cheung WW, Ding W, Hoffman HM, et al. Vitamin D ameliorates adipose browning in chronic kidney disease cachexia. Sci Rep. 2020;10(1):14175. doi:10.1038/s41598-020-70190-z
129. Bordelon P, Ghetu MV, Langan RC. Recognition and management of vitamin D deficiency. Am Fam Physician. 2009;80(8):841–846.
130. Grønborg IM, Tetens I, Andersen EW, et al. Effect of vitamin D fortified foods on bone markers and muscle strength in women of Pakistani and Danish origin living in Denmark: a randomised controlled trial. Nutr J. 2019;18(1):82. doi:10.1186/s12937-019-0504-9
131. Nasimi N, Sohrabi Z, Dabbaghmanesh MH, et al. A novel fortified dairy product and sarcopenia measures in sarcopenic older adults: a double-blind randomized controlled trial. J Am Med Dir Assoc. 2021;22(4):809–815. doi:10.1016/j.jamda.2020.08.035
132. Rizzoli R, Stevenson JC, Bauer JM, et al. The role of dietary protein and vitamin D in maintaining musculoskeletal health in postmenopausal women: a consensus statement from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Maturitas. 2014;79(1):122–132. doi:10.1016/j.maturitas.2014.07.005
133. Bauer J, Biolo G, Cederholm T, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J Am Med Dir Assoc. 2013;14(8):542–559. doi:10.1016/j.jamda.2013.05.021
134. Boirie Y. Fighting sarcopenia in older frail subjects: protein fuel for strength, exercise for mass. J Am Med Dir Assoc. 2013;14(2):140–143. doi:10.1016/j.jamda.2012.10.017
135. Gilmartin S, O’Brien N, Giblin L. Whey for sarcopenia; can whey peptides, hydrolysates or proteins play a beneficial role? Foods. 2020;9(6):750. doi:10.3390/foods9060750
136. Ottestad I, Løvstad AT, Gjevestad GO, et al. Intake of a protein-enriched milk and effects on muscle mass and strength. A 12-week randomized placebo controlled trial among community-dwelling older adults. J Nutr Health Aging. 2017;21(10):1160–1169. doi:10.1007/s12603-016-0856-1
137. Salles J, Chanet A, Giraudet C, et al. 1,25(OH)2-vitamin D3 enhances the stimulating effect of leucine and insulin on protein synthesis rate through Akt/PKB and mTOR mediated pathways in murine C2C12 skeletal myotubes. Mol Nutr Food Res. 2013;57(12):2137–2146. doi:10.1002/mnfr.201300074
138. Bauer JM, Verlaan S, Bautmans I, et al. Effects of a vitamin D and leucine-enriched whey protein nutritional supplement on measures of sarcopenia in older adults, the PROVIDE study: a randomized, double-blind, placebo-controlled trial. J Am Med Dir Assoc. 2015;16(9):740–747. doi:10.1016/j.jamda.2015.05.021
139. Rondanelli M, Cereda E, Klersy C, et al. Improving rehabilitation in sarcopenia: a randomized-controlled trial utilizing a muscle-targeted food for special medical purposes. J Cachexia Sarcopenia Muscle. 2020;11(6):1535–1547. doi:10.1002/jcsm.12532
140. Lin CC, Shih MH, Chen CD, Yeh SL. Effects of adequate dietary protein with whey protein, leucine, and vitamin D supplementation on sarcopenia in older adults: an open-label, parallel-group study. Clin Nutr. 2021;40(3):1323–1329. doi:10.1016/j.clnu.2020.08.017
141. Cramer JT, Cruz-Jentoft AJ, Landi F, et al. Impacts of high-protein oral nutritional supplements among malnourished men and women with sarcopenia: a multicenter, randomized, double-blinded, controlled trial. J Am Med Dir Assoc. 2016;17(11):1044–1055. doi:10.1016/j.jamda.2016.08.009
142. Hanach NI, McCullough F, Avery A. The impact of dairy protein intake on muscle mass, muscle strength, and physical performance in middle-aged to older adults with or without existing sarcopenia: a systematic review and meta-analysis. Adv Nutr. 2019;10(1):59–69. doi:10.1093/advances/nmy065
143. Granic A, Hurst C, Dismore L, et al. Milk for skeletal muscle health and sarcopenia in older adults: a narrative review. Clin Interv Aging. 2020;15:695–714. doi:10.2147/CIA.S245595
144. Hurst C, Robinson SM, Witham MD, et al. Resistance exercise as a treatment for sarcopenia: prescription and delivery. Age Ageing. 2022;51(2). doi:10.1093/ageing/afac003
145. Coelho-Júnior HJ, Calvani R, Picca A, Tosato M, Landi F, Marzetti E. Engagement in aerobic exercise is associated with a reduced prevalence of sarcopenia and severe sarcopenia in Italian older adults. J Pers Med. 2023;13(4):655. doi:10.3390/jpm13040655
146. Daly RM. Independent and combined effects of exercise and vitamin D on muscle morphology, function and falls in the elderly. Nutrients. 2010;2(9):1005–1017. doi:10.3390/nu2091005
147. Anton SD, Hida A, Mankowski R, et al. Nutrition and exercise in sarcopenia. Curr Protein Pept Sci. 2018;19(7):649–667. doi:10.2174/1389203717666161227144349
148. Rondanelli M, Klersy C, Terracol G, et al. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am J Clin Nutr. 2016;103(3):830–840. doi:10.3945/ajcn.115.113357
149. Kim H, Kim M, Kojima N, et al. Exercise and nutritional supplementation on community-dwelling elderly Japanese women with sarcopenic obesity: a randomized controlled trial. J Am Med Dir Assoc. 2016;17(11):1011–1019. doi:10.1016/j.jamda.2016.06.016
150. Yamada M, Kimura Y, Ishiyama D, et al. Synergistic effect of bodyweight resistance exercise and protein supplementation on skeletal muscle in sarcopenic or dynapenic older adults. Geriatr Gerontol Int. 2019;19(5):429–437. doi:10.1111/ggi.13643
151. Chang MC, Choo YJ. Effects of whey protein, leucine, and vitamin d supplementation in patients with sarcopenia: a systematic review and meta-analysis. Nutrients. 2023;15(3):521. doi:10.3390/nu15030521
152. Wolfe RR. Branched-chain amino acids and muscle protein synthesis in humans: myth or reality? J Int Soc Sports Nutr. 2017;14:30. doi:10.1186/s12970-017-0184-9
153. Huschtscha Z, Parr A, Porter J, Costa RJS. The effects of a high-protein dairy milk beverage with or without progressive resistance training on fat-free mass, skeletal muscle strength and power, and functional performance in healthy active older adults: a 12-week randomized controlled trial. Front Nutr. 2021;8:644865. doi:10.3389/fnut.2021.644865
154. Nunes EA, Colenso-Semple L, McKellar SR, et al. Systematic review and meta-analysis of protein intake to support muscle mass and function in healthy adults. J Cachexia Sarcopenia Muscle. 2022;13(2):795–810. doi:10.1002/jcsm.12922
155. Michalczyk MM, Gołaś A, Maszczyk A, Kaczka P, Zając A. Influence of Sunlight and Oral D(3) Supplementation on Serum 25(OH)D concentration and exercise performance in elite soccer players. Nutrients. 2020;12(5). doi:10.3390/nu12051311
156. Gallagher JC. The effects of calcitriol on falls and fractures and physical performance tests. J Steroid Biochem Mol Biol. 2004;89-90(1–5):497–501. doi:10.1016/j.jsbmb.2004.03.059
157. Miyakoshi N, Masutani N, Kasukawa Y, et al. Comparison of the effects of native vitamin d and eldecalcitol on muscular strength and dynamic balance in patients with postmenopausal osteoporosis. Prog Rehabil Med. 2020;5:20200026. doi:10.2490/prm.20200026
158. Jodar E, Campusano C, de Jongh RT, Holick MF. Calcifediol: a review of its pharmacological characteristics and clinical use in correcting vitamin D deficiency. Eur J Nutr. 2023;62(4):1579–1597. doi:10.1007/s00394-023-03103-1
159. Saito T, Mori Y, Irei O, Baba K, Nakajo S, Itoi E. Effect of eldecalcitol on muscle function and fall prevention in Japanese postmenopausal women: a randomized controlled trial. J Orthop Sci. 2021;26(1):173–178. doi:10.1016/j.jos.2020.02.004
160. Ross AC, Manson JE, Abrams SA, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab. 2011;96(1):53–58. doi:10.1210/jc.2010-2704
161. Pludowski P, Holick MF, Grant WB, et al. Vitamin D supplementation guidelines. J Steroid Biochem Mol Biol. 2018;175:125–135. doi:10.1016/j.jsbmb.2017.01.021
162. Vallon V, Verma S. Effects of SGLT2 Inhibitors on Kidney and Cardiovascular Function. Annu Rev Physiol. 2021;83:503–528. doi:10.1146/annurev-physiol-031620-095920
163. Cowie MR, Fisher M. SGLT2 inhibitors: mechanisms of cardiovascular benefit beyond glycaemic control. Nat Rev Cardiol. 2020;17(12):761–772. doi:10.1038/s41569-020-0406-8
164. Zhang H, Wu X, Liang J, Kirberger M, Chen N. Irisin, an exercise-induced bioactive peptide beneficial for health promotion during aging process. Ageing Res Rev. 2022;80:101680. doi:10.1016/j.arr.2022.101680
165. Rolland Y, Dray C, Vellas B, Barreto PS. Current and investigational medications for the treatment of sarcopenia. Metabolism. 2023;149:155597. doi:10.1016/j.metabol.2023.155597
166. Sakuma K, Yamaguchi A. Sarcopenia and age-related endocrine function. Int J Endocrinol. 2012;2012:127362. doi:10.1155/2012/127362
167. Meriggioli MN, Roubenoff R. Prospect for pharmacological therapies to treat skeletal muscle dysfunction. Calcif Tissue Int. 2015;96(3):234–242. doi:10.1007/s00223-014-9926-8
168. Graber E, Reiter EO, Rogol AD. Human growth and growth hormone: from antiquity to the recominant age to the future. Front Endocrinol. 2021;12:709936. doi:10.3389/fendo.2021.709936
169. Ekiz T, Kara M, Ata AM, et al. Rewinding sarcopenia: a narrative review on the renin-angiotensin system. Aging Clin Exp Res. 2021;33(9):2379–2392. doi:10.1007/s40520-020-01761-3
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
TT3, a More Practical Indicator for Evaluating the Relationship Between Sarcopenia and Thyroid Hormone in the Euthyroid Elderly Compared with FT3

Chen J, Wei L, Zhu X, Xu W, Zou Y, Qi X, Fang J, Wang X, Shi X, Sheng Y, Ding G, Ouyang X, Duan Y
Clinical Interventions in Aging 2023, 18:1285-1293
Published Date: 4 August 2023