")
Back to Journals » Orthopedic Research and Reviews » Volume 17
Weight-Bearing Monitoring Devices in Lower Extremity Fractures: A Scoping Review
Authors Robinson J, Wang AWT , Stockton DJ
Received 26 February 2025
Accepted for publication 15 May 2025
Published 21 June 2025 Volume 2025:17 Pages 257—267
DOI https://doi.org/10.2147/ORR.S521013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Jackson Robinson, Alice Wei Ting Wang, David J Stockton
Department of Orthopaedics, The University of British Columbia Faculty of Medicine, Vancouver, BC, Canada
Correspondence: David J Stockton, Email [email protected]
Background: Orthopaedic surgeons commonly prescribe weight-bearing parameters for their patients for a variety of reasons. Weight-bearing may be limited in order to control the healing environment, but advancing a patient’s weight-bearing status is preferably done as quickly as possible to maximize functional recovery. However, it is entirely unclear to what extent these prescriptions are followed in practice. The purpose of this scoping review is to identify and compare non-invasive devices used for the measurement of weight-bearing following lower extremity fractures.
Methods: Database searches of MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials (CENTRAL) were completed to identify relevant studies. Titles were screened for relevance, and abstracts were screened against the eligibility criteria. We identified studies that investigated the use of external force, pedal pressure, or activity monitoring devices used in adults after lower extremity fractures and excluded studies involving compartment pressure measurement.
Findings: Sixty-two studies met the inclusion criteria. About 39% of studies used an insole-type device, which could be worn in a shoe or integrated into a removable boot. Other device types included step count or activity monitors (52%), force plates (18%), pressure film (2%) and external pedobarography systems (27%).
Interpretation: We found that different monitors offered varying types of measurements and are suitable for a variety of applications. Therefore, selecting the ideal device depends on the metric of interest. Further high-quality prospective studies utilizing device monitoring are needed to validate the theory that early weight-bearing is beneficial and safe for patients with lower extremity fractures.
Keywords: trauma, fracture, lower extremity, weight-bearing, monitoring
Introduction
Orthopaedic surgeons commonly prescribe weight-bearing parameters for their patients for a variety of reasons. The AO Foundation recommends periods of non-weight-bearing or limited weight-bearing for the majority of lower extremity peri-articular fracture patterns.1 Weight-bearing may be limited in order to modulate the strain environment of a fracture as it heals, to protect soft tissues or to ensure construct safety. However, advancing a patient’s weight-bearing status is preferably done as quickly as possible in order to minimize tissue atrophy and disuse osteopenia and maximize functional recovery.2,3 These conflicting priorities are an ongoing focus in the literature.
Multiple studies have explored the relationship between load bearing and fracture recovery on a theoretical level. In an in-vitro computer modelling study by Claes et al found that while increased fracture distance was associated with reduced stability, interfragmentary motion was well tolerated at lower fracture distances.4 Using a finite element model, Bailon-Plaza and van der Muelen showed that both fracture site stimulation and increase in ambulatory moments within limits resulted in accelerated healing.5 Theoretical models support ambulation as a catalyst in early healing of a fracture.
Comparative studies support the safety of early post-operative weight-bearing in a variety of fracture types. A study by Graham showed that accelerated weight-bearing is safe and effective in surgically treated hip fracture patients at 1 and 3 year follow ups.6 Similarly, a Cochrane review by Lin et al showed that patients in early and delayed weight-bearing groups have similar activity levels and complication rates following surgical fixation of ankle fractures.7 These studies are limited in that no measure of participants’ weight-bearing behavior was utilized. This significantly limits the conclusions that can be drawn since the only discrete difference between the comparative groups is the investigators’ instructions, not necessarily the patient’s behavior. However, comparative studies using current load sensing technology have been proposed. Kalmet et al have suggested a comparison of “permissive weight bearing” and traditional non-weight-bearing outcomes in pelvic, acetabular and lower extremity peri-articular fractures, and plan to use an electronic insole to monitor weight-bearing activity.8
It remains unclear to what extent weight-bearing prescriptions are followed in practice. Multiple published studies have shown high non-compliance rates. In a study of 51 lower extremity fracture patients with non-weight-bearing instructions, Chiodo et al found that 27.5% of patients exceeded loading limits over the 3-month study duration.9 Similarly, Braun et al showed that 53% of patients were unable to comply with weight-bearing prescriptions post-operatively in multiple lower extremity fracture types.10 Dabke et al found similar results during crutch assisted weight-bearing in a lab setting.11
Given high rates of non-compliance following lower extremity fracture, accurate methods of weight-bearing monitoring are critical to ensure the integrity of future studies. The purpose of this scoping review was to identify and compare non-invasive devices used for the measurement of weight-bearing following lower extremity fractures.
Materials and Methods
Database searches of MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials (CENTRAL) were completed to identify relevant studies. Searches of MEDLINE and EMBASE databases were completed on and were inclusive to September 6th, 2023, with the CENTRAL database search completed on March 27th, 2025 and inclusive to December 31st, 2023. Our eligibility criteria included studies that used non-invasive force, plantar pressure, or activity monitoring devices in adults after lower extremity fractures. We specifically excluded studies involving compartment pressure measurement. The review protocol was developed with the assistance of a medical librarian and finalized prior to being implemented, however was not formally registered. An example of the search terms used is included in Table 1, with full database specific search terms included in Appendix 1.
 |
Table 1 MEDLINE Database Search Terms |
Titles were screened for relevance and abstracts were screened against the eligibility criteria. Title, abstract and full text screening was completed by two independent reviewers (JR, AW). An additional search of clinicaltrials.gov, the WHO International Clinical Trial Registry Platform (ICTRP), Networked Digital Library of Theses and Dissertations (NDLTD), Dissertations and Theses Global and Grey Matters was completed to identify unpublished literature. Any theses or dissertations meeting eligibility criteria were screened for relevant published sub-studies. Reference lists of all studies meeting inclusion criteria after full text review were reviewed to identify additional relevant literature. Results were documented in a pre-defined charting form. A PRISMA diagram outlining the review process is shown in Figure 1.
 |
Figure 1 PRISMA diagram. Adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. under the CC BY 4.0 license. |
Results
Device types were identified and separated into 5 groups for further analysis (Table 2). Some studies used more than one method of measurement, and devices were included in multiple categories as necessary. About 39% of studies used an insole-type device, which could be worn in a shoe or integrated into a removable boot. Other device types included step count or activity monitors (52%), force plates (18%), pressure film (2%) and external pedobarography systems (27%).
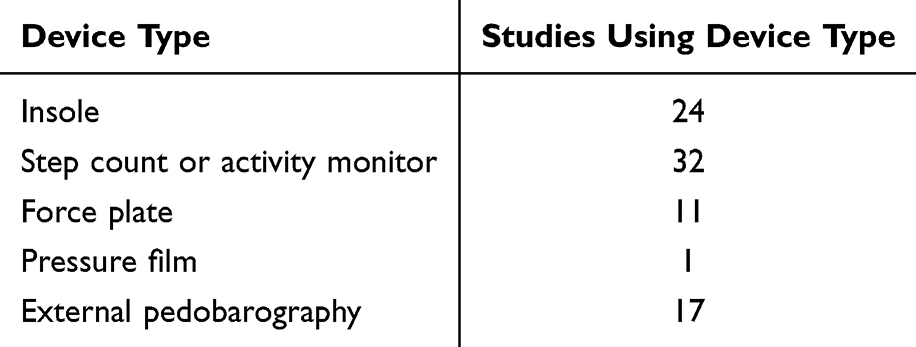 |
Table 2 Weight-Bearing Monitoring Device Sub-Categories |
Relevant metrics for each identified device were collected from available manufacturer data (Table 3). In the case that manufacturer data was not publicly available, manufacturers and study authors were contacted to request missing information. Relevant information from review studies and cited background work were used when manufacturer data were unavailable, and we were unable to contact study authors.
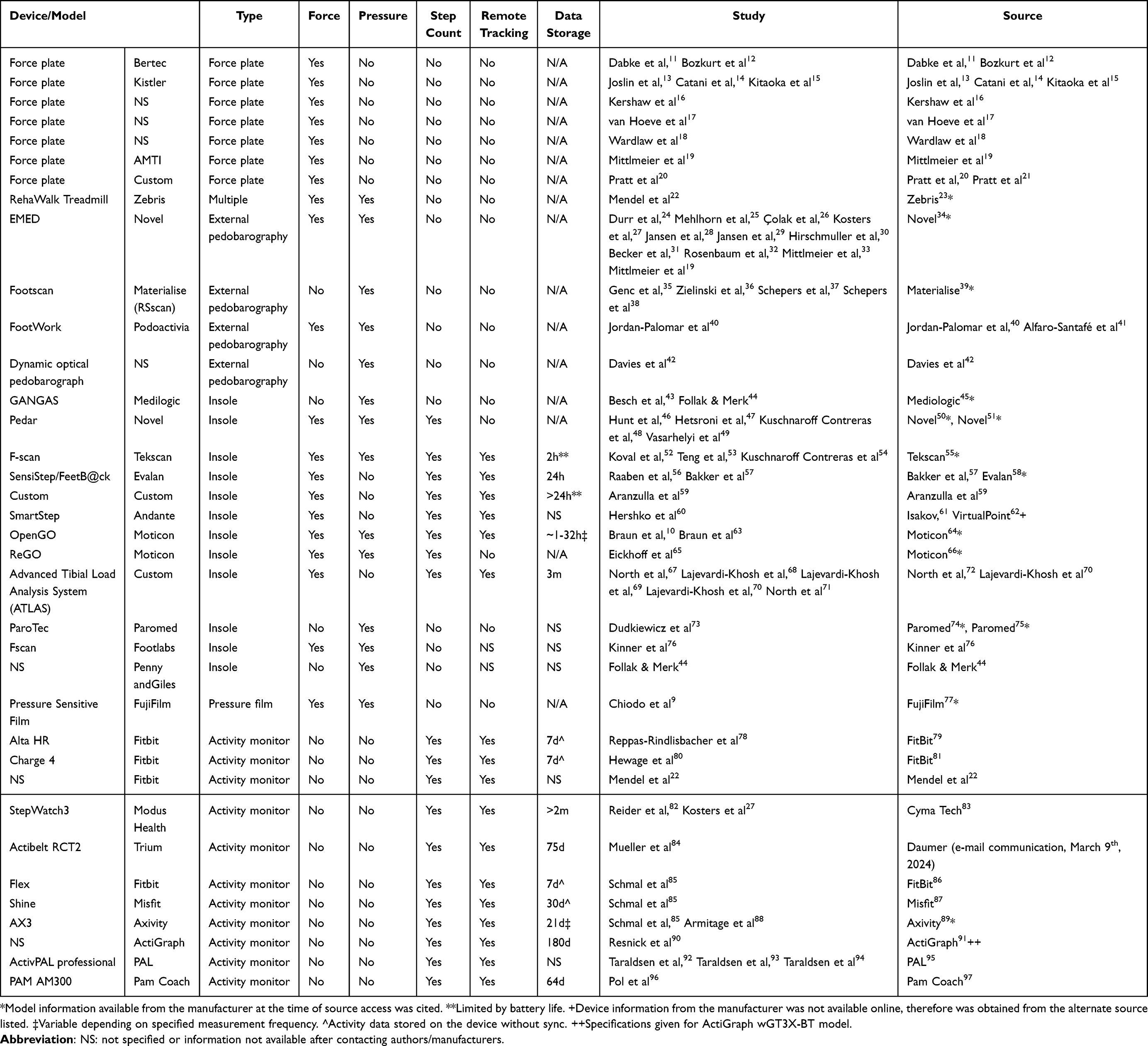 |
Table 3 Device Metrics |
About 47% of devices were found to be suitable for remote monitoring or tracking based on available information. Data storage capacity ranged from hours to multiple months. Storage capacity metrics were not included for all force plate, pressure plate and pedobarographic systems.
Discussion
The purpose of this scoping review was to identify and compare non-invasive devices used for monitoring lower extremity weight-bearing activity after fracture. Device suitability for monitoring applications is reviewed below for each group.
Force Plate
A force plate can be a versatile tool for weight-bearing monitoring and can be used in different capacities depending on the metric of interest. Of the devices identified, all were able to collect force data in a lab setting. Early studies by Pratt et al20 and Wardlaw et al18 measured limb loading using a force plate and oscillograph paired with an instrumented cast system and were able to calculate fracture stiffness. Kershaw et al16 and Joslin et al13 used force plate systems to demonstrate an increase in longitudinal weight-bearing activity with fracture healing, in addition to fracture stiffness measurements. Other studies used force plates paired with video analysis, goniometers and/or electromyography to assess joint and muscle forces during gait.12,14,15,17,19 None of the identified systems were found to be suitable for ambulatory use and therefore would require interval assessment and extrapolation of loading behaviour to the home environment.
External Pedobarography
These systems allow for the measurement of underfoot pressure distribution through an instrumented mat or pressure plate. For example, the Novel EMED measures underfoot pressure distribution during standing or with movement,34 with functionality demonstrated in multiple studies.19,24–33 Pedobarography devices can also be coupled with traditional gait analysis techniques, such as force, video and strength testing, to provide an additional metric to assess patient function and recovery.19,25,27,30,33,36,40 Some models of the Materialise Footscan allow researchers to synchronize gait analysis with pressure data acquisition through an integrated system.39 A unique treadmill based system is demonstrated by Mendel et al22 in a mobility study of sacral fracture patients. The Zebris RehaWalk allows for collection of pressure distribution and step count, in addition to force data, while providing visual feedback to the patient.23 As with force plate systems, these devices are generally not suitable for ambulatory use and require monitoring by an experienced research team during data collection.
Insole Monitoring
These devices allow researchers to collect force, pressure and step count data through an instrumented insole in the patient’s shoe. Based on the available information, most of the devices in this category are capable of collecting force and step count data simultaneously.50,51,55,57–59,61,62,64,66,70,72 The Novel Pedar, Tekscan F-scan and Moticon OpenGo/ReGO systems also have the additional benefit of providing pressure distribution data.50,51,55,64,66 Some devices are optimized for ambulatory monitoring. For example, the ATLAS is a multi-sensor system integrated into the sole of a CAM walking boot and is designed for continuous monitoring for up to 3 months.72 The Moticon OpenGO has been used in multiple studies of lower extremity weight-bearing post-fracture10,63 and allows for continuous monitoring on the order of days using the “SmartRecording mode” (depending on the measurement frequency setting, Figure 2).64 In contrast, the Tekscan F-scan and Evalan SensiStep have an ambulatory capability limited to less than 1 day by battery or storage capacity,55,58 making them less than ideal for home monitoring applications. In general, insole systems with the ability to collect a range of gait data, including force, pressure distribution and step count over weeks to months, are ideally suited for ambulatory monitoring applications. These devices allow a range of gait data to be collected while minimizing intervention by both the patient and research team.
 |
Figure 2 Moticon OpenGo Insole (Color). Used with permission from moticon.com. |
Step Count/Activity Monitors
All of the identified activity monitors had ambulatory monitoring capabilities that ranged in their storage capacity from 7 to 180 days depending on the device (Daumer, e-mail communication, March 9th, 2024).79,81,83,86,87,89,91,97 Popular consumer wearables produced by FitBit are capable of monitoring step count data for up to 7 days without syncing.79,81,86 Some other devices marketed towards research applications, such as the Cyma Tech StepWatch, Trium ActiBelt, ActiGraph wGT3X-BT and Pam Coach AM300, are capable of collecting activity data for multiple months (Daumer, e-mail communication, March 9th, 2024).83,91,97 While relatively simple to implement and easy to use, an inherent limitation of these devices is their inability to collect load or pressure distribution data. However, when taken as a proxy for load bearing activity step count remains a valuable source of information for patient mobility and functional status.
Pressure Sensitive Film
Chiodo et al9 placed a pressure sensitive film in the casts of lower extremity fracture patients to assess compliance with non-weight-bearing restrictions. The Fujifilm material allows for assessment of pressure distribution via the proprietary software once removed.77 While simple to implement, this approach has multiple limitations. A pressure threshold must be set to differentiate compliance versus non-compliance. As well, data is lost when a previously measured value is exceeded, therefore, information on the frequency of load bearing events cannot be assessed over time. While a reasonable approach for assessing if a patient has been 100% compliant with non-weight-bearing restrictions, this material is not ideal for following the loading behaviours of patients with partial weight-bearing restrictions over time.
Study Limitations
While this scoping review identified a variety of non-invasive devices used to monitor activity or load bearing in patients with lower extremity fractures, there are some limitations to the study. Our database search included a focused search through MEDLINE, EMBASE and CENTRAL. An expanded search of other databases specializing in medical and biomechanical literature may identify additional studies and devices that are not captured in this study. As well, many studies included limited or incomplete information on the monitoring device used, and in some cases did not report manufacturer information. However, we attempted to provide a comprehensive overview by obtaining missing data from published device documentation, manufacturer specifications, user and product manuals when available, and contacting manufacturers with information requests as necessary.
We also note that the included studies are heterogeneous in their choice of device and fracture types studied, resulting in varying endpoints of interest. Nevertheless, we chose to focus on the capabilities of each device to demonstrate possible indications for use in future research (ie measurement type, ability to facilitate remote tracking, and data storage capacity). Thus, this scoping review may serve as a guide for future studies to focus on specific device indications, related complications and the effect on treatment outcomes.
Conclusions
In this scoping review, a variety of approaches and devices used for weight-bearing and activity monitoring for patients with lower extremity fractures were found in the literature. We found that different monitors offered varying types of measurements and are suitable for a variety of applications. Therefore, selecting the ideal device depends on the metric of interest. If detailed gait analysis is necessary, devices such as the Zebris RehaWalk, Novel Pedar/EMED and Tekscan F-scan provide many sensing elements to collect pressure distribution data with a high degree of resolution.23,34,50,51,55 Increased resolution does come at the cost of higher data and storage requirements. With reduced number of sensors, the ATLAS and Moticon OpenGO devices require less data storage, which improves ambulatory monitoring capacity.64,72 Some activity monitors also have the benefit of reduced storage requirements given simplified data metrics83,91 but rely on the assumption that step count correlates with the degree of lower extremity loading. Pressure sensitive films may be suitable for monitoring of non-weight-bearing compliance but are limited in providing time course data.9
As fracture care continues to evolve, we expect external weight-bearing monitoring devices to play a key role in data collection and monitoring patient compliance. With reduced costs and increasing system resolution over time, the accessibility of these devices should improve. Once the ideal parameters for weight-bearing following lower extremity fracture are elucidated, there may be a role for such devices to provide real-time feedback to the patient on their compliance. In the interim, the systems currently available on the market provide an array of options for researchers to choose from in monitoring loading post-lower extremity fracture. Further high-quality prospective studies utilizing device monitoring are needed to validate the theory that early weight-bearing is beneficial and safe for patients with lower extremity fractures.2,3,7
Ethics Approval and Informed Consent
Not required as based on previously published data and does not include novel data on humans (individuals, samples or data) or animals.
Consent for Publication
The authors confirm that the details of any images, videos, recordings, etc. can be published, and that the person(s) providing consent have been shown the article contents to be published. We will provide copies of signed consent forms to the journal editorial office if requested.
Acknowledgments
We would like to thank Kristina McDavid and Aubrey Geyer (UBC Library) for their assistance in developing our search strategy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the University of British Columbia Department of Orthopaedics Summer Student Research Grant. We did not use funds from any other grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors have no financial or non-financial competing interests to report, including but not limited to employment with the study sponsor, stock holdings or options, patents, royalties, personal fees, holding a board position, or any political, religious, or academic interest relevant to the published content.
References
1. Buckley RE, Moran CG, Apivatthakakul T. AO Principles of Fracture Management. AO Foundation; 2017.
2. Kubiak EN, Beebe MJ, North K, Hitchcock R, Potter MQ. Early weight bearing after lower extremity fractures in adults. J Am Acad Orthop Surg. 2013;21(12):727–739. doi:10.5435/JAAOS-21-12-727
3. Dong W, Lisitano LSJ, Marchand LS, Reider LM, Haller JM. Weight-bearing guidelines for common geriatric upper and lower extremity fractures. Curr Osteoporos Rep. 2023;21:698–709. doi:10.1007/s11914-023-00834-2
4. Claes LE, Heigele CA, Neidlinger-Wilke C. Effects of mechanical factors on the fracture healing process. Clin Orthop Relat Res. 1998;355:S132. doi:10.1097/00003086-199810001-00015
5. Bailón-Plaza A, van der Meulen MCH. Beneficial effects of moderate, early loading and adverse effects of delayed or excessive loading on bone healing. J Biomech. 2003;36(8):1069–1077. doi:10.1016/S0021-9290(03)00117-9
6. Graham J. Early or delayed weight-bearing after internal fixation of transcervical fracture of the femur. A clinical trial. J Bone Joint Surg Br. 1968;50(3):562–569. doi:10.1302/0301-620X.50B3.562
7. Lin CWC, Donkers NAJ, Refshauge KM, Beckenkamp PR, Khera K, Moseley AM. Rehabilitation for ankle fractures in adults. Cochrane Database Syst Rev. 2012;11:CD005595. doi:10.1002/14651858.CD005595.pub3
8. Kalmet PHS, Meys G, Horn YY V, et al. Permissive weight bearing in trauma patients with fracture of the lower extremities: prospective multicenter comparative cohort study. BMC Surg. 2018;18(1):8. doi:10.1186/s12893-018-0341-3
9. Chiodo CP, Macaulay AA, Palms DA, Smith JT, Bluman EM. Patient compliance with postoperative lower-extremity non-weight-bearing restrictions. J Bone Joint Surg Am. 2016;98(18):1563–1567. doi:10.2106/JBJS.15.01054
10. Braun B, Veith N, Rollmann M, et al. Weight-bearing recommendations after operative fracture treatment-fact or fiction? Gait results with and feasibility of a dynamic, continuous pedobarography insole. Int Orthop. 2017;41(8):1507–1512. doi:10.1007/s00264-017-3481-7
11. Dabke HV, Gupta SK, Holt CA, O’Callaghan P, Dent CM. How accurate is partial weightbearing? Clin Orthop Relat Res. 2004;421(421):282. doi:10.1097/01.blo.0000127116.13377.65
12. Bozkurt M, Kentel BB, Yavuzer G, Öçgüder A, Heycan C, Tonuk E. Functional evaluation of intraarticular severely comminuted fractures of the calcaneus with gait analysis. J Foot Ankle Surg. 2004;43(6):374–379. doi:10.1053/j.jfas.2004.09.006
13. Joslin CC, Eastaugh-Waring SJ, Hardy JRW, Cunningham JL. Weight bearing after tibial fracture as a guide to healing. Clin Biomech. 2008;23(3):329–333. doi:10.1016/j.clinbiomech.2007.09.013
14. Catani F, Benedetti MG, Simoncini L, Leardini A, Giannini S. Analysis of function after intra-articular fracture of the os calcis. Foot Ankle Int. 1999;20(7):417–421. doi:10.1177/107110079902000704
15. Kitaoka HB, Schaap EJ, Chao EY, An KN. Displaced intra-articular fractures of the calcaneus treated non-operatively. Clinical results and analysis of motion and ground-reaction and temporal forces. J Bone Joint Surg Am. 1994;76(10):1531–1540. doi:10.2106/00004623-199410000-00013
16. Kershaw CJ, Cunningham JL, Kenwright J. Tibial External Fixation, Weight Bearing, and Fracture Movement. Clin Orthopaedics Related Res. 1993;293. doi:10.1097/00003086-199308000-00005
17. van Hoeve S, de Vos J, JPAM V, Willems P, Meijer K, Poeze M. Gait analysis and functional outcome after calcaneal fracture. J Bone Joint Surg Am. 2015;97(22):1879–1888. doi:10.2106/JBJS.N.01279
18. Wardlaw D, McLauchlan J, Pratt D, Bowker P. A biomechanical study of cast-brace treatment of femoral shaft fractures. J Bone Joint Surg Br. 1981;63-B(1):7–11. doi:10.1302/0301-620X.63B1.7204477
19. Mittlmeier T, Morlock MM, Kollmitzer J, Zwick EB, Lob GC. Efficiency of gait measurement after complex foot trauma. Foot Ankle Surg. 1996;2(4):197–208. doi:10.1016/S1268-7731(96)80002-6
20. Pratt D, Bowker P, Wardlaw D, McLauchlan J. Biomechanical study of the function of the femoral fracture brace during stance. Med Biol Eng Comput. 1980;18(5):667–673. doi:10.1007/BF02443144
21. Pratt DJ, Bowker P, Wardlaw D, McLauchlan J. Load measurement in orthopaedics using strain gauges. J Biomed Eng. 1979;1(4):287–296. doi:10.1016/0141-5425(79)90168-7
22. Mendel T, Schenk P, Ullrich BW, et al. Mid-term outcome of bilateral fragility fractures of the sacrum after bisegmental transsacral stabilization versus spinopelvic fixation. Bone Joint J. 2021;103-B(3):462–468. doi:10.1302/0301-620X.103B3.BJJ-2020-1454.R1
23. The zebris FDM-T System for stance and gait analysis. 2012. Available from: https://www.zebris.de/fileadmin/Editoren/zebris-PDF/zebris-Prospekte-EN/FDM-T_Prospekt_en_120901_72dpi.pdf.
24. Durr C, Apinun J, Mittlmeier T, Rammelt S. Foot function after surgically treated intraarticular calcaneal fractures: correlation of clinical and pedobarographic results of 65 patients followed for 8 years. J Orthop Trauma. 2018;32(12):593–600. doi:10.1097/BOT.0000000000001325
25. Mehlhorn A, Walther M, Yilmaz T, et al. Dynamic plantar pressure distribution, strength capacity and postural control after Lisfranc fracture-dislocation. Gait Posture. 2017;52:332–337. doi:10.1016/j.gaitpost.2016.11.043
26. Çolak TK, Çolak İ, Timurtaş E, Bulut G, Polat M. Pedobarographic and radiological analysis after treating a talus neck fracture. J Foot Ankle Surg. 2016;55(6):1216–1222. doi:10.1053/j.jfas.2016.07.017
27. Kosters C, Bockholt S, Muller C, et al. Comparing the outcomes between Chopart, Lisfranc and multiple metatarsal shaft fractures. Arch Orthop Trauma Surg. 2014;134(10):1397–1404. doi:10.1007/s00402-014-2059-8
28. Jansen H, Fenwick A, Doht S, Frey S, Meffert R. Clinical outcome and changes in gait pattern after pilon fractures. Int Orthop. 2013;37(1):51–58. doi:10.1007/s00264-012-1716-1
29. Jansen H, Frey SP, Ziegler C, Meffert RH, Doht S. Results of dynamic pedobarography following surgically treated intra-articular calcaneal fractures. Arch Orthop Trauma Surg. 2013;133(2):259–265. doi:10.1007/s00402-012-1655-8
30. Hirschmuller A, Konstantinidis L, Baur H, et al. Do changes in dynamic plantar pressure distribution, strength capacity and postural control after intra-articular calcaneal fracture correlate with clinical and radiological outcome? Injury. 2011;42(10):1135–1143. doi:10.1016/j.injury.2010.09.040
31. Becker H, Rosenbaum D, Kriese T, Gerngross H, Claes L. Gait asymmetry following successful surgical treatment of ankle fractures in young adults. Clin Orthop Relat Res. 1995;311:262–269.
32. Rosenbaum D, Lubke B, Bauer G, Claes L. Long-term effects of hindfoot fractures evaluated by means of plantar pressure analyses. Clin Biomech. 1995;10(7):345–351.
33. Mittlmeier T, Morlock MM, Hertlein H, et al. Analysis of morphology and gait function after intraarticular calcaneal fracture. J Orthop Trauma. 1993;7(4):303–310. doi:10.1097/00005131-199308000-00002
34. Pressure distribution measurement under the foot- Pedography. novel.de. 2024. Available from: https://novel.de/products/emed/.
35. Genc Y, Gultekin A, Duymus T, Mutlu S, Mutlu H, Komur B. Pedobarography in the assessment of postoperative calcaneal fracture pressure with gait. J Foot Ankle Surg. 2016;55(1):99–105. doi:10.1053/j.jfas.2015.07.018
36. Zielinski SM, Keijsers NL, Praet SFE, et al. Functional outcome after successful internal fixation versus salvage arthroplasty of patients with a femoral neck fracture. J Orthop Trauma. 2014;28(12):e273–80. doi:10.1097/BOT.0000000000000123
37. Schepers T, Kieboom B, Van Diggele P, Patka P, Van Lieshout E. Pedobarographic analysis and quality of life after Lisfranc fracture dislocation. Foot Ankle Int. 2010;31(10):857–864. doi:10.3113/FAI.2010.0857
38. Schepers T, Van Der Stoep A, Van Der Avert H, Van Lieshout E, Patka P. Plantar pressure analysis after percutaneous repair of displaced intra-articular calcaneal fractures. Foot Ankle Int. 2008;29(2):128–135. doi:10.3113/FAI.2008.0128
39. Materialise Motion. Available from: https://www.materialise.com/en/healthcare/phits-suite/pressure-plates-3d-scanners#pressure-plates.
40. Jordan-Palomar E, Javierre E, Rey-Vasalo J, Alfaro-Santafe V, Gomez-Benito M. An evaluation of surgical functional reconstruction of the foot using kinetic and kinematic systems: a case report. J Foot Ankle Surg. 2017;56(1):208–216. doi:10.1053/j.jfas.2016.01.038
41. Alfaro-Santafé JV, Gómez-Bernal A, Almenar-Arasanz AJ, Alfaro-Santafé J. Reliability and repeatability of the footwork plantar pressure plate system. J Am Podiatr Med Assoc. 2021;111(6). doi:10.7547/18-057
42. Davies M, Betts R, Scott I. Optical plantar pressure analysis following internal fixation for displaced intra-articular os calcis fractures. Foot Ankle Int. 2003;24(11):851–856. doi:10.1177/107110070302401108
43. Besch L, Radke B, Mueller M, et al. Dynamic and functional gait analysis of severely displaced intra-articular calcaneus fractures treated with a hinged external fixator or internal stabilization. J Foot Ankle Surg. 2008;47(1):19–25. doi:10.1053/j.jfas.2007.10.013
44. Follak N, Merk H. The benefit of gait analysis in functional diagnostics in the rehabilitation of patients after operative treatment of calcaneal fractures. Foot Ankle Surg. 2003;9(4):209–214. doi:10.1016/S1268-7731(03)00092-4
45. Manual: medilogic pressure measurement. 2018.
46. Hunt K, Goeb Y, Bartolomei J. Dynamic loading assessment at the fifth metatarsal in elite athletes with a history of Jones fracture. Clin J Sport Med. 2021;31(6):E321–E326. doi:10.1097/JSM.0000000000000830
47. Hetsroni I, Ben-Sira D, Nyska M, Ayalon M. Plantar pressure anomalies after open reduction with internal fixation of high-grade calcaneal fractures. Foot Ankle Int. 2014;35(7):712–718. doi:10.1177/1071100714531226
48. Kuschnaroff Contreras ME, Kroth LM, Kotani KL, et al. Intra articular calcaneal fractures: a clinical and biomechanical analysis. Rev Bras Ortop Engl Ed. 2009;44(6):496–503. doi:10.1016/S2255-4971(15)30147-6
49. Vasarhelyi A, Baumert T, Fritsch C, Hopfenmuller W, Gradl G, Mittlmeier T. Partial weight bearing after surgery for fractures of the lower extremity--is it achievable? Gait Posture. 2006;23(1):99–105. doi:10.1016/j.gaitpost.2004.12.005
50. Running Analysis with Novel Pedar System; 2023. Available from: https://www.youtube.com/watch?v=1bdQDAS7ug0.
51. Footwear pressure distribution measurement- pedar. novel.de. Available from: https://novel.de/products/pedar/.
52. Koval KJ, Sala DA, Kummer FJ, Zuckerman JD. Postoperative weight-bearing after a fracture of the femoral neck or an intertrochanteric fracture. J Bone Joint Surg Am. 1998;80(3):352–356. doi:10.2106/00004623-199803000-00007
53. Teng AL, Pinzur MS, Lomasney L, Mahoney L, Havey R. Functional outcome following anatomic restoration of tarsal-metatarsal fracture dislocation. Foot Ankle Int. 2002;23(10):922–926. doi:10.1177/107110070202301006
54. Kuschnaroff Contreras ME, de Souza Muniz AM, de Souza J B, et al. Biomechanical evaluation of intra articular calcaneal fracture and clinical radiographic correlation. Acta Ortop Bras. 2004;12(2):105–112. doi:10.1590/s1413-78522004000200006
55. F-Scan GO. In-shoe foot function & gait analysis system. 2023. Available from: https://www.tekscan.com/sites/default/files/2023-06/230526_FScanGO_SystemFlyer_FINALpdf.
56. Raaben M, Holtslag HR, Leenen LPH, Augustine R, Blokhuis TJ. Real-time visual biofeedback during weight bearing improves therapy compliance in patients following lower extremity fractures. Gait Posture. 2018;59:206–210. doi:10.1016/j.gaitpost.2017.10.022
57. Bakker A, Blokhuis TJ, MDME M, Hermens HJ, Holtslag HR. Dynamic weight loading in older people with Hip fracture. J rehab med. 2014;46(7):708. doi:10.2340/16501977-1793
58. SensiStep. EVALAN. 2022. Available from: https://evalan.com/cases/sensistep/.
59. Aranzulla PJ, Muckle DS, Cunningham JL. A portable monitoring system for measuring weight-bearing during tibial fracture healing. Med Eng Phys. 1998;20(7):543–548. doi:10.1016/S1350-4533(98)00061-7
60. Hershko E, Tauber C, Carmeli E. Biofeedback versus physiotherapy in patients with partial weight-bearing. Ame J Orthopedics. 2008;37(5):E92.
61. Isakov E. Gait rehabilitation: a new biofeedback device for monitoring and enhancing weight-bearing over the affected lower limb. Eura Medicophys. 2007;43(1):21–26.
62. SmartStep from Andante, Video Produced by Virtual Point; 2009. Available from: https://www.youtube.com/watch?v=EfoE7GPwWR8.
63. Braun BJ, Bushuven E, Hell R, et al. A novel tool for continuous fracture aftercare – clinical feasibility and first results of a new telemetric gait analysis insole. Injury. 2016;47(2):490–494. doi:10.1016/j.injury.2015.11.004
64. OpenGo by Moticon: sensor Insole Specification. 2023. https://moticon.com/wp-content/uploads/2021/09/OpenGo-Sensor-Insole-Specification-A4-RGB-EN-03.03.pdf.
65. Eickhoff AM, Cintean R, Fiedler C, Gebhard F, Schütze K, Richter PH. Analysis of partial weight bearing after surgical treatment in patients with injuries of the lower extremity. Arch Orthop Trauma Surg. 2022;142(1):77–81. doi:10.1007/s00402-020-03588-z
66. ReGo Sensor Insoles - sensing foot dynamics for training & rehab. Moticon. Available from: https://moticon.com/rego/sensor-insoles.
67. North K, Simpson GM, Stuart AR, et al. Early postoperative step count and walking time have greater impact on lower limb fracture outcomes than load-bearing metrics. Injury. 2023;54(7):110756. doi:10.1016/j.injury.2023.04.043
68. Lajevardi-Khosh A, Stuart A, Ackerman M, et al. Characterization of compliance to weight-bearing protocols and patient weight-bearing behavior during the recovery period in lower extremity fractures: a pilot study. Curr Orthop Pract. 2019;30(4):395–402. doi:10.1097/BCO.0000000000000773
69. Lajevardi-Khosh A, Bamberg S, Rothberg D, Kubiak E, Petelenz T, Hitchcock R. Center of pressure in a walking boot shifts posteriorly in patients following lower leg fracture. Gait Posture. 2019;70:218–221. doi:10.1016/j.gaitpost.2019.03.010
70. Lajevardi-Khosh A, Tresco B, Stuart A, et al. Development of a step counting algorithm using the ambulatory tibia load analysis system for tibia fracture patients. J Rehabil Assist Technol Eng. 2018;5:2055668318804974. doi:10.1177/2055668318804974
71. North K, Kubiak EN, Rothberg D, et al. Longitudinal monitoring of patient limb loading throughout ankle fracture rehabilitation using an insole load monitoring system: a case series. Curr Orthop Pract. 2017;28(2):223–230. doi:10.1097/BCO.0000000000000469
72. North K, Kubiak EN, Hitchcock RW, Petelenz TJ. Load monitoring system for partial weight bearing therapy for rehabilitation of lower extremity fractures. In:
73. Dudkiewicz I, Levi R, Blankstein A, Chechick A, Salai M. Dynamic footprints: adjuvant method for postoperative assessment of patients after calcaneal fractures. Isr Med Assoc J. 2002;4(5):349–352.
74. paroTec. Paromed Australia. 2016. Available from: https://www.paromed.com.au/our-products/foot-pressure-measurement/parotec/.
75. Paromed Technology in Action. 2017. Available from: https://www.youtube.com/watch?v=FK_8_InpDO8.
76. Kinner BJ, Best R, Falk K, Thon KP. Is there a reliable outcome measurement for displaced intra-articular calcaneal fractures? J Trauma. 2002;53(6):1094–1102. doi:10.1097/00005373-200212000-00011
77. Prescale - Pressure measurement film. Fujifilm [Canada]. Available from: https://www.fujifilm.com/ca/en/business/industrial-materials/measurement-film/prescale.
78. Reppas-Rindlisbacher C, Ahuja M, Wong E, et al. Researching the effects of sleep on step count during the postoperative period. J Am Geriatr Soc. 2021;69(10):2990–2992. doi:10.1111/jgs.17305
79. Fitbit Alta HR. 2020. Available from: https://help.fitbit.com/manuals/manual_alta_hr_en_US.pdf.
80. Hewage K, Fosker S, Leckie T, et al. The Hospital to Home study (H2H): smartwatch technology-enabled rehabilitation following Hip fracture in older adults, a feasibility non-randomised trial. Future Healthc J. 2023;10(1):14–20. doi:10.7861/fhj.2022-0101
81. fitbit charge 4. 2020. Available from: https://staticcs.fitbit.com/content/assets/help/manuals/manual_charge_4_en_US.pdf.
82. Reider L, Bai J, Scharfstein DO, Zipunnikov V. Methods for step count data: determining “valid” days and quantifying fragmentation of walking bouts. Gait Posture. 2020;81:205–212. doi:10.1016/j.gaitpost.2020.07.149
83. StepWatch3 step activity monitor. 2004.
84. Mueller A, Hoefling H, Nuritdinow T, et al. Continuous monitoring of patient mobility for 18 months using inertial sensors following traumatic knee injury: a case study. Digit Biomark. 2018;2(2):79–89. doi:10.1159/000490919
85. Schmal H, Holsgaard-Larsen A, Izadpanah K, Brønd JC, Madsen CF, Lauritsen J. Validation of activity tracking procedures in elderly patients after operative treatment of proximal femur fractures. Rehabil Res Pract. 2018;2018:3521271. doi:10.1155/2018/3521271
86. fitbit flex Wireless Activity + Sleep Wristband. Available from: https://myhelp.fitbit.com/resource/manual_flex_en_US.
87. Shine Activity Monitor: user Manual. 2012. https://m.media-amazon.com/images/I/B16EHzxTD1S.pdf.
88. Armitage LC, Chi Y, Santos M, et al. Monitoring activity of hip injury patients (MoHIP): a sub-study of the world hip trauma evaluation observational cohort study. Pilot Feasibility Stud. 2020;6:70. doi:10.1186/s40814-020-00612-2
89. AX3v2 Datasheet: 3-Axis logging movement sensor, 2023. Available from: https://axivity.com/files/resources/AX3v2_Datasheet.pdf.
90. Resnick B, Galik E, Boltz M, et al. Physical activity in the post-Hip-fracture period. J Aging Phys Act. 2011;19(4):373–387. doi:10.1123/japa.19.4.373
91. wGT3X-BT | actiGraph Wearable Devices. 2024. Availabe from: https://theactigraph.com/actigraph-wgt3x-bt.
92. Taraldsen K, Askim T, Sletvold O, et al. Evaluation of a body-worn sensor system to measure physical activity in older people with impaired function. Phys Ther. 2011;91(2):277–285. doi:10.2522/ptj.20100159
93. Taraldsen K, Sletvold O, Thingstad P, et al. Physical behavior and function early after Hip fracture surgery in patients receiving comprehensive geriatric care or orthopedic care—a randomized controlled trial. J Gerontol a Biol Sci Med Sci. 2014:69A(3):338–345. doi:10.1093/gerona/glt097.
94. Taraldsen K, Vereijken B, Thingstad P, Sletvold O, Helbostad JL. Multiple days of monitoring are needed to obtain a reliable estimate of physical activity in Hip-fracture patients. J Aging Phys Act. 2014;22(2):173–177. doi:10.1123/japa.2012-0130
95. PAL family. activPAL. 2024. Available from: https://www.palt.com/pals/.
96. Pol MC, Ter Riet G, Van Hartingsveldt M, Kröse B, Buurman BM. Effectiveness of sensor monitoring in a rehabilitation programme for older patients after Hip fracture: a three-arm stepped wedge randomised trial. Age Ageing. 2019;48(5):650–657. doi:10.1093/ageing/afz074
97. AM300 M. pamcoach. Available from: https://www.pamcoach.com/index.php?pid=3&spid=93.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.