")
Back to Journals » Journal of Pain Research » Volume 18
“Zhibian (BL54) to Shuidao (ST28)” Acupuncture Manipulation Combined with Analgesics in Postoperative Pain Management for Patients with Mixed Hemorrhoids: A Randomized Controlled Trial Protocol
Authors Wang T , Gao JQ , Chang M, Ma MC , Wang YT , Guo TN , Zhang YL , Gao Z , Wang HJ , Cao YX
Received 25 January 2025
Accepted for publication 11 April 2025
Published 24 April 2025 Volume 2025:18 Pages 2163—2174
DOI https://doi.org/10.2147/JPR.S519232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Te Wang,1 Jun Qiang Gao,2 Min Chang,1 Ming Chen Ma,1 Yu Tong Wang,1 Tu Ning Guo,1 Yan Lin Zhang,3 Zhen Gao,1 Hai Jun Wang,1,* Yu Xia Cao4,*
1The Second Clinical College, Shanxi University of Chinese Medicine, Jinzhong, Shanxi, People’s Republic of China; 2 7th Ward of Colorectal and Anal Surgery Department, Shanxi Provincial People’s Hospital, Taiyuan, Shanxi, People’s Republic of China; 3College of Acupuncture and Massage, Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China; 4 3rd Ward of Acupuncture Department, The Affiliated Acupuncture and Tuina Hospital of Shanxi University of Chinese Medicine, Taiyuan, Shanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hai Jun Wang, Professor, Shanxi University of Chinese Medicine, Jinzhong, Shanxi, People’s Republic of China, Email [email protected] Yu Xia Cao, Chief Physician, the Affiliated Acupuncture and Tuina Hospital of Shanxi University of Chinese Medicine, Taiyuan, Shanxi, People’s Republic of China, Email [email protected]
Purpose: Mixed hemorrhoids patients often face severe postoperative pain, typically treated with Non-steroidal anti-inflammatory drugs (NSAIDs) or opioids, which may lead to gastrointestinal and Central Nervous System (CNS) side effects. The “Zhibian (BL54) to Shuidao (ST28)” manipulation acupuncture combined with analgesics shows promise as a safe and effective alternative. Thorough randomized controlled trials (RCTs) are crucial for determining the effectiveness and safety when used in conjunction with pain relievers.
Patients and Methods: This double-blind randomized controlled trial aims to assess the effectiveness and safety of the acupuncture method connecting the “Zhibian (BL54)” and “Shuidao (ST28)” points combined with analgesics in alleviating pain following surgery for mixed hemorrhoids. A total of 104 patients who meet diagnostic criteria and undergo Milligan-Morgan open hemorrhoidectomy (MMH) will be randomized into control (n = 52) or acupuncture (n = 52) groups. The control group will receive diclofenac sodium, while the acupuncture group will additionally undergo the “Zhibian (BL54) to Shuidao (ST28)” manipulation acupuncture. The intervention will span a duration of five days, with data collection occurring both prior to and following the intervention. Primary outcomes include Visual analogue scale (VAS) scores for pain, with secondary outcomes assessing analgesic efficiency, increased pain medication use, and pain interference in daily activities. Statistical analysis will be conducted utilizing SPSS software, version 26.0.
Discussion: This forward-looking, randomized study aims to assess the effectiveness of combining acupuncture with medication in alleviating postoperative pain for individuals suffering from mixed hemorrhoids, wih the goal of establishing a safe and potent therapeutic strategy and broadening the clinical applications of this intervention.
Conclusion: This randomized study evaluates the effectiveness of combining acupuncture with medication to relieve postoperative pain in patients with mixed hemorrhoids, aiming to establish a safe and effective treatment strategy and expand its clinical use.
Keywords: mixed hemorrhoid, pain, acupuncture, Zhibian (BL54) to Shuidao (ST28), protocol
Introduction
Hemorrhoids, graded I–IV, are prevalent anorectal diseases with a 39% prevalence rate.1 They are categorized as internal, external, and mixed, with mixed being particularly common.2,3 Mixed hemorrhoids affect patients with both internal and external types. Hemorrhoids are categorized based on their location relative to the dentate line. The ones found beneath this line are referred to as external hemorrhoids, are marked by pain and swelling, whereas internal hemorrhoids, which lie above the line, typically present with prolapse and bleeding.4 The etiology of hemorrhoids remains elusive, it is hypothesized that chronic constipation and excessive straining contribute to the degeneration of anal tissues and the displacement of the anal cushions.5 For mixed hemorrhoids, surgical intervention is predominantly employed.6 Surgical procedures are highly recommended for addressing grade III (reducible) and grade IV (irreducible) hemorrhoids.7 The Milligan-Morgan hemorrhoidectomy (MMH)8 continues to be the premier surgical intervention for addressing these issues. However, MMH has limitations, including severe pain, stenosis, fissure, bleeding, and papillary hypertrophy.9–11 It can also cause complications like urinary retention and infection.8
Postoperative pain is common after hemorrhoidectomy, affecting 75% of patients, with 80% experiencing moderate-to-severe pain.12 This pain can delay wound healing and affect daily activities.13,14 Pain-induced stress triggers cortisol overproduction, which suppresses immune function by reducing proinflammatory cytokines and critical repair enzymes while simultaneously elevating cardiovascular stress markers.15 This neuroendocrine-immune dysregulation disrupts the coordinated cellular interactions required for early wound healing phases.16 Even patients may continue to experience pain for a long time after surgery. Cheetham et al reported in their study that in the postoperative monitoring of 16 individuals who had SH (Stapled Hemorrhoidectomy) surgery, five reported ongoing pain and a constant feeling of urgency over 15 months, and two were incapacitated for work due to intense pain.17
In clinical settings, postoperative pain management for mixed hemorrhoids primarily relies on opioids, NSAIDs, and central analgesics.18,19 Diclofenac, a common NSAID, is effective for postoperative pain relief following hemorrhoidectomy. A study found Diclofenac to be more effective than placebo in controlling pain within 24 hours post-surgery when used as a rectal suppository.20 However, these medications require frequent administration for pain relief and carry risks of gastrointestinal and CNS adverse effects like nausea, vomiting, and bleeding,21–23 with a 37% incidence rate.24
There is a significant clinical need for a safe, non-pharmacological therapy to effectively alleviate postoperative discomfort in patients with mixed hemorrhoids, improving their quality of life. This aligns with pain management goals, which aim to reduce pain duration, minimize medication side effects, and lower treatment costs. Acupuncture, a time-honored practice in Traditional Chinese Medicine (TCM), is recognized for its safety. Unlike many Western medical treatments, it does not cause adverse reactions such as nausea or vomiting, and drug dependency risks. A review shows acupuncture has a 0.55 serious adverse events rate per 10,000 patients, making it a low-risk intervention.25 Additionally, acupuncture is easy to administer and cost-effective. However, research on acupuncture for postoperative pain from mixed hemorrhoids is limited. It has shortcomings, such as complex procedures, multiple acupoint selection, and long treatment times. Thus, this study used the “Zhibian (BL54) to Shuidao (ST28)” manipulation acupuncture, using one needle for two acupoints. A 150mm needle facilitated sensation movement along the needle, accurately targeting areas and increasing stimulation.26,27 This technique offers precise acupoint selection, ease of operation, and no adverse effects.28 It alleviates pain, increases tolerance, and prevents NSAID-related adverse effects. Combining acupuncture with medication leverages their respective strengths for improved therapy. Clinically, acupuncture and drug therapy integration is highly effective. Li et al’s research showed electroacupuncture (EA) with milnacipran enhanced pain relief in a rat model.29
This study evaluates the effectiveness and safety of combining “Zhibian (BL54) to Shuidao (ST28)” manipulation acupuncture with analgesics for postoperative pain management in mixed hemorrhoids patients. The primary objective is to assess analgesic efficacy using VAS pain scores measured twice daily from postoperative day 1 to day 5, which are expected to show significant reductions at key time points. Secondary objectives include evaluating analgesic efficiency through pain episode frequency; determining the need for additional analgesics, reflecting NSAID-sparing effects; and assessing the impact of pain on daily activities using the BPI-SF.
Materials and Methods
Study Design and Setting
This prospective, multicenter, double-blind randomized controlled trial will adhere to the Consolidated Standards of Reporting Trials (CONSORT) and the updated guidelines for reporting acupuncture interventions in clinical trials. A total of 104 patients who meet diagnostic criteria30 and undergo MMH will be randomized into control (n = 52) or acupuncture (n = 52) groups. The control group will receive diclofenac sodium, while the acupuncture group will additionally undergo the “Zhibian (BL54) to Shuidao (ST28)” manipulation acupuncture. The research encompasses a 5-day intervention period and a subsequent 1-month follow-up phase. The study has received ethical clearance from the Ethics Review Board of the affiliated Acupuncture and Tuina hospital of Shanxi University of Chinese Medicine (clinical trial no.004, 2024) and will adhere to the principles outlined in the Declaration of Helsinki. All participants will provide written informed consent. The trial is listed with the China Clinical Trial Registration Center, bearing the registration number ChiCTR2400081302. The schedule (Figure 1) will be used to show the enrollment, interventions, and assessment, and the flowchart (Figure 2) will be used to illustrate the trial’s progression.
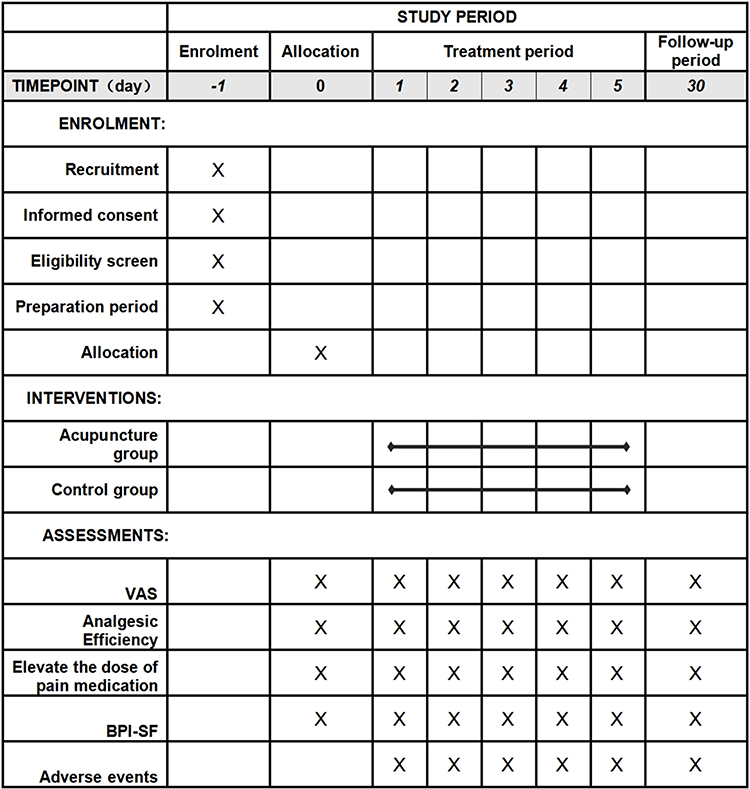 |
Figure 1 The SPIRIT schedule of enrollment, interventions and assessment. |
 |
Figure 2 Flowchart. Depicting the process throughout the trial. |
Recruitment
The study will recruit participants who meet the specified inclusion and exclusion criteria and are admitted to the Acupuncture and Moxibustion Massage Hospital of Shanxi University of Traditional Chinese Medicine and the People’s Hospital of Shanxi Province between June 2024 and June 2025. Recruitment will be carried out by posting posters in the outpatient department. Intervention and follow-up will be conducted in relevant departments within the hospital.
Inclusion Criteria
Qualified individuals who satisfy the designated prerequisites will be included in the research:
- Those diagnosed with mixed hemorrhoids30 and have undergone MMH treatment;
- Aged 18 to 65 years, both male and female;
- The surgical anesthesia method is combined spinal-epidural anesthesia;
- The surgical procedure used is external stripping and internal ligation for mixed hemorrhoids, with the same person performing both the surgery and dressing changes;
- Regular diet, normal sleep, and previously healthy;
- Participants will be voluntarily enrolled in this study, having signed the informed consent form and demonstrated good compliance. They must also express a willingness to cooperate with both observation and treatment protocols.
Exclusion Criteria
Individuals will be ineligible for the study if they:
- Receiving treatments that could influence the study’s outcome measures;
- Having other rectal or anal conditions, such as perianal abscess, anal fistula, or anal fissure;
- Suffering from severe cardiac, hepatic, pulmonary, renal, or psychiatric disorders;
- Being pregnant or lactating;
- Diagnosed with infectious diseases, including hepatitis B or tuberculosis;
- Presenting with local skin infections or dermatological conditions unsuitable for acupuncture;
- Having a known allergy to diclofenac sodium dual-release enteric-coated capsules;
- Participants are currently taking part in other clinical trials.
Randomization and Allocation Concealment
A statistician, unaware of the patient details, will utilize SPSS 26.0 to create a random number list, guaranteeing that 104 patients are evenly and randomly assigned to either the acupuncture or control group. To ensure allocation concealment, sequentially numbered, opaque, sealed envelopes will be used.
Blinding
We will apply a double-blind (patient-assessor-blinded) method. Patients will be informed that they will receive one of several legitimate treatments, which will help maintain blinding to the specific group allocation, and will be instructed not to discuss their treatment details with the outcome assessors. The acupuncturist and prescribing physician will be aware of the treatment allocations due to the need to administer and supervise the treatment accurately. To prevent bias, those involved will not participate in the outcome assessment. Initial clinical outcomes will be evaluated by a third researcher who is blinded to group assignments. Subsequently, an independent statistician, also blinded to group allocation, will analyze the data to ensure impartial statistical evaluation. To minimize bias, we will document and analyze any protocol deviations that might affect blinding. Regular meetings will be held to review the blinding procedures and ensure strict adherence.
Interventions
The two cohorts underwent standardized postoperative proctological care protocols. Throughout the therapeutic phase, participants were instructed to adhere to a low light dietary regimen, incorporate moderate exercise routines, and practice regular perianal hygiene. Postoperative pharmacological interventions were systematically implemented based on clinical evaluations, including antibiotic prophylaxis (Cefradine Capsules) for infection risk mitigation, stool softeners (Shouhui Tongbian) to optimize bowel function, and analgesic medications (Diclofenac Sodium and Codeine Phosphate Tablets) administered as required. Notably, therapeutic regimens remained uniformly standardized across all participant cohorts in this experimental design.
Acupuncture Treatment Group
Based on the “Zhibian(BL54) to Shuidao(ST28)” manipulation of acupuncture, combined with the treatment of the control group. Sterile disposable acupuncture needles (Hwato brand): 150mm in length and 0.40mm in diameter (Suzhou Medical Device Production License, issued under Registration Certificate No. 20162200970; the manufacturer is Suzhou Medical Appliance Factory Co., Ltd).
Patients will be positioned prone during acupuncture sessions. The practitioner will initially locate the specific acupuncture points designated for stimulation. The skin is first sanitized using a 75% isopropyl alcohol wipe. A long, slender needle, 150mm long and 0.40 mm in diameter (Figure 3), is then inserted at the Zhibian acupuncture point (BL54), with its tip directed towards the Shuidao point (ST28). The needle is inserted diagonally at a point that is two-fifths of the distance from the top and three-fifths from the bottom along the line connecting the posterior superior iliac spine to the inner edge of the greater trochanter (Figure 4). The needle is placed at a 20° angle relative to the patient’s sagittal plane and parallel to the horizontal plane. The depth of insertion will be between 4 and 6 cun, and the Deqi sensation, often experienced in the pubic area or lower abdomen, will be elicited. After achieving Deqi, the needle will be rotated for 1 minute, followed by retention at the acupuncture point for 30 minutes, with interval needle manipulation. Acupuncture will begin postoperatively each morning after dressing changes, once daily, until discharge, for a total of 5 sessions. To maintain consistency, all the acupuncture methods used will determine through standardized technical training, covering acupoint localization, needle insertion techniques (including depth and angle), and needle manipulation techniques. The detailed operation procedures will also be specified in the Investigator’s Manual.
 |
Figure 3 The long needle. Length: 6 cun/150 mm, diameter: 0.40 mm. |
 |
Figure 4 “Zhibian(BL54) to Shuidao(ST28)” acupuncture manipulation, the specific acupuncture points for the penetration technique, ranging from Zhibian (BL54) to Shuidao (ST28). |
Control Group
The patients will be given diclofenac double-release enteric-coated capsules, 75 mg.
(Temmler Ireland Ltd., Killorglin, Co. Kerry, Ireland; Approval number: Imported Drug Registration Certificate No. 20170098). The medication will be administered once every morning following the postoperative dressing change, continuing for a total of 5 days.
Outcomes
Primary Outcome
The Visual Analogue Scale (VAS), which is used to evaluate the postoperative pain on the postoperative day 1 to day 5 (0–10 point, which ranges from 0 (no pain) to 10 (severe pain), higher score means severe pain). Evaluations are conducted two times a day, at 8 a.m. and 8 p.m. from the first to the fifth day post-surgery, allowing detailed understanding of pain trends and the immediate effect of treatment.
Secondary Outcomes
- Analgesic Efficiency: Patients are required to record the frequency of pain episodes daily for the first 5 days post-operation. Each episode’s onset and duration should be documented. A reduction of more than 30% in the frequency of pain episodes is considered clinically significant.
- Elevate the dose of pain medication: The number of additional doses of other analgesic medications (excluding Diclofenac Sodium Dual Release SR Capsules) will be recorded to evaluate potential reductions in medication use within the acupuncture group. A comprehensive patient assessment will be conducted at 8 a.m. each day to review the previous day’s situation.
- The Brief Pain Inventory-Short Form (BPI-SF): BPI-SF will be utilized to evaluate the extent to which pain interferes with seven specific aspects of daily activities. A comprehensive patient assessment will be conducted at 8 a.m. each day for the previous day.
Safety Evaluation and Adverse Events
The Case Report Form (CRF) will systematically document adverse events related to patient safety during the study. These adverse events (AEs) will be categorized into two main types: treatment-related and non-treatment-related. Treatment-related AEs will further include adverse reactions associated with pain medication—such as nausea, vomiting, and gastrointestinal bleeding—as well as those linked to acupuncture, including local hematomas, dizziness, local infections, broken needles, and post-treatment discomfort. If the patient experiences any related adverse reactions, treatment can be immediately discontinued. Each entry in the CRF must include detailed information on the timing, cause, clinical presentation, and indications of the adverse event. Additionally, it should document the emergency management measures implemented and any notable abnormal laboratory results. Additionally, all incidents will be assessed for their relationship to the intervention and their severity.
Data Collection and Management
A digital repository will be created using the information from the case report forms (CRFs). Data entry personnel will be responsible for promptly and precisely entering all pertinent information as detailed in the CRFs. Access to the CRFs will be restricted to outcome assessors, who will perform double data entry to ensure data integrity and accuracy. In addition, a Data Monitoring Committee will be constituted for this trial. The committee will oversee the safety, efficacy, and quality assurance of the study while maintaining strict data confidentiality. Any changes to the research plan will be carried out under the supervision of the monitoring committee.
Sample Size
The objective of this research is to evaluate the contrast in therapeutic effectiveness between the group receiving acupuncture and the control group. Based on an earlier pilot study, the acupuncture group reported a VAS score of 3.76 ± 1.62, while the control group had a VAS score of 4.73 ± 1.68, with a type I error (α) of 0.05 and a type II error (β) of 0.2, and a 1:1 ratio of sample sizes for the acupuncture treatment and control groups, the sample size calculation formula is as follows:
In the formula,  represents the required sample size per group,
represents the required sample size per group,  is the pooled standard deviation,
is the pooled standard deviation,  and
and  are the standard normal distribution quantiles corresponding to the significance level α and the power 1−β, respectively, and
are the standard normal distribution quantiles corresponding to the significance level α and the power 1−β, respectively, and  and
and  are the means of the two groups. The required sample size is 46 for both the acupuncture and control groups. Accounting for a 10% dropout rate, each group needs at least 52 participants.
are the means of the two groups. The required sample size is 46 for both the acupuncture and control groups. Accounting for a 10% dropout rate, each group needs at least 52 participants.
Statistical Analysis
Data analysis will be conducted with the aid of SPSS, version 26.0 (IBM, Armonk, NY, USA). Continuous data that follow a normal distribution will be summarized using the mean and standard deviation, while non-normally distributed continuous data will be reported as the median along with the interquartile range. Frequencies and proportions will be used to represent categorical data. The Kolmogorov–Smirnov test will be utilized to evaluate normality and variance homogeneity. The decision to use either parametric or non-parametric statistical techniques will be based on the results of the normality tests. For data that is normally distributed, a paired t-test will be employed to compare pre- and post-treatment values within the same group, while a Wilcoxon signed-rank test will be used for data that does not follow a normal distribution. To compare different groups, an independent samples t-test will be applied if the data is normally distributed, and a Wilcoxon rank-sum test will be used otherwise. All statistical analyses will employ two-tailed tests, with a P-value of 0.05 or less considered statistically significant.
Discussion
Postoperative pain is also the most common symptom following hemorrhoidectomy.13,14 However, the mechanism of pain following hemorrhoidectomy is Correspondence to Mehrdad Sayadinia. Mixed hemorrhoids postoperative pain is currently considered to be caused by multiple factors: (1) The increased pain sensitivity is a consequence of both peripheral and central sensitization, including the spread of spinal nerve activity beneath the dentate line; (2) local tissue damage and inflammatory responses release inflammatory mediators after surgery such as prostaglandins, interleukins, histamines, etc.; (3) Postoperative activities such as defecation and dressing changes can stimulate the wound surface, leading to continuous spasms of the sphincter muscles; (4) poor and delayed wound healing; (5) type of postoperative anesthesia and surgical method.31–36
NSAIDs have excellent analgesic effects and can even reduce the dosage of opioid drugs by 18.3% in acute pain.37 Their analgesic principle is to inhibit cyclooxygenase and reduce the synthesis of prostaglandins, thereby alleviating pain, fever, and inflammation.
Acupuncture, a TCM therapy, has significant analgesic effects, but its pain relief mechanism is still unclear. Currently, the main perspectives are as follows: Acupuncture alleviates pain by suppressing the conduction of nociceptive signals within the central nervous system and stimulating the release of endogenous pain-relieving compounds.38 This approach activates the opioid receptor network in the spinal dorsal horn, resulting in the secretion of inherent opioids like endorphins, norepinephrine, and serotonin.39–42 Opioid peptides, including β-endorphins, enkephalins, and dynorphins, have been found to produce pain-relieving effects by interacting with the central nervous system. Additionally, their analgesic action is closely associated with the suppression of cholecystokinin (CCK) octapeptide, 5-hydroxytryptamine (5-HT), and N-methyl-D-aspartic acid (NMDA) receptors.39,43 Acupuncture stimulates specific acupoints, activating peripheral nerve receptors, particularly A-β and C fibers. These fiber types are the primary ones associated with acupuncture-induced analgesia.44,45 Activation of these nerve fibers impedes the conduction of nociceptive signals, thereby significantly reducing the sensation of pain. This process is integral to the analgesic efficacy attributed to acupuncture. Furthermore, acupuncture modulates the immune response, thereby mitigating inflammation. This treatment method has demonstrated the ability to decrease the concentrations of pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), thereby alleviating pain caused by inflammatory responses.29
In addition, Research in animal models has shown that acupuncture possesses both systemic regulatory and specific therapeutic impacts. It can facilitate tissue healing, ameliorating pathological conditions, regulating immune reactions, affecting hormonal functions, balancing the cytokine network, mitigating urinary system issues, bolstering local blood flow, and optimizing energy metabolism.46 Recent research indicates that acupuncture can mitigate the pain response and enhance pain tolerance.47 A study has indicated that acupuncture is more efficacious in treating post-hemorrhoidectomy pain than painkillers.48 Current evidence suggests that the integration of electroacupuncture with the technique of acupoint catgut embedding is highly effective in alleviating the postoperative discomfort associated with hemorrhoids and in reducing the need for pain-relief medications.49 Numerous studies have indicated that conventional body acupuncture holds significant promise in alleviating pain and minimizing the negative side effects associated with both intravenous and oral pain medications. A meta-analysis encompassing fifteen RCTs juxtaposing acupuncture against sham controls indicated that patients in the acupuncture cohort exhibited decreased postoperative opioid usage and reduced pain levels for up to 72 hours post-surgery, surpassing the outcomes of the control group. Moreover, this cohort of patients showed a lower incidence of adverse effects associated with opioids, such as nausea, drowsiness, and difficulty urinating.50 Even if it cannot fully replace analgesics, its use in combination with painkillers can decrease the quantity and dosage of painkillers that patients need to take, thereby reducing the occurrence of adverse reactions.
However, the aforementioned numerous protocols involve multiple acupuncture points and complex procedures, making it difficult for patients to accept. Additionally, the limited number of participants hinders a comprehensive assessment of the effectiveness and safety of these procedures. The acupuncture technique involving the “Zhibian (BL54) to Shuidao (ST28)” manipulation acupuncture, which involves needling from the Zhibian point (BL54) to the Shuidao point (ST28), offers the benefits of requiring a limited number of acupoints, being straightforward to perform, and yielding substantial outcomes.
The “Zhibian (BL54) to Shuidao (ST28)” manipulation acupuncture was developed by Professor Laixi Ji’s team at Shanxi University of Chinese Medicine. Building on previous practitioners’ experiences, the team systematically explored key elements such as the anatomical localization of Zhibian (BL54) acupoint, operational norms, conduction mechanisms of needling sensation, indications, principles of action, and safety assessments.27 Initially applied to male prostate-related diseases with favorable clinical efficacy,51–53 the technique’s scope has expanded to include stress urinary incontinence, postoperative voiding dysfunction, male sexual dysfunction, and dysmenorrhea.28,54,55 In clinical trials, our team treated 17 patients with postoperative voiding dysfunction using this technique. Patients experienced warmth, fullness, and relaxation in the pelvic cavity, sometimes extending to the external genitalia, indicating stimulation of the pelvic plexus and pudendal nerve. This facilitated coordination between the autonomic and somatic motor systems, improving voiding function.56,57 Experimental studies on oxytocin-induced dysmenorrhea in rats revealed that the technique enhances central serotonin 5-HT synthesis and utilization, promotes inhibitory neurotransmitter release, and exerts central analgesic effects.58 Further research suggests that its efficacy may be linked to inhibiting the Nucleotide-binding Oligomerization Domain-containing protein 1/Receptor Interacting Serine/Threonine-protein Kinase 2/Nuclear Factor kappa-light-chain-enhancer of activated B cells (NOD1/RIP2/NF-κB) signaling pathway, reducing uterine inflammation.59
The Zhibian (BL54) and Shuidao (ST28) acupoints were documented as early as in the Classic of Acupuncture and Moxibustion (Zhenjiu Jiayi Jing) and the Great Compendium of Acupuncture and Moxibustion (Zhenjiu Dacheng). In modern Chinese Acupuncture and Moxibustion textbooks, the precise locations and therapeutic indications of these acupoints are described in detail. Zhibian (BL54), is located in the sacral region at the level of the fourth sacral posterior foramen, 3 cun lateral to the posterior median sacral crest. It is used for lumbosacral pain, urinary retention, constipation, and hemorrhoids. Shuidao (ST28), is 3 cun below the umbilicus and 2 cun lateral to the midline, primarily treating fluid metabolism disorders. In a study, catgut embedding at Changqiang (DU1) and bilateral Zhibian (BL54) acupoints demonstrated good analgesic effects and safety for postoperative pain management after mixed hemorrhoidectomy.60 Another study found that adzuki bean application at the Shuidao (ST28) acupoint effectively prevented postoperative urinary retention following hemorrhoidectomy.61
This technique requires the needle to be inserted at a specific intersection point, where the upper 40% and lower 60% meet along the line from the posterior superior iliac spine to the greater trochanter of the femur. The needle is angled at 20° relative to the sagittal plane and must penetrate more than 5 cun deep. Patients frequently describe sensations that extend to the lower abdomen, genital area, or perineum, experiencing a sense of fullness, warmth, and relief in the pelvic region. This highlights the accuracy and profound therapeutic effect of the method.62 Clinical observations highlight the dense vascular and neural anatomy along the acupuncture pathway, suggesting stimulation of the pelvic plexus and pudendal nerves.62 These nerves, branching in the pudendal canal, innervate key pelvic structures, including the anal and genital regions.63 External hemorrhoid pain, transmitted via somatic nerves, contrasts with the visceral nerve innervation of internal hemorrhoids, which lack pain sensitivity.63 Needle sensations can reach the urethra or anus, indicating potential modulation of sympathetic and parasympathetic functions.64 This stimulation enhances hormonal responses, blood circulation, and tissue repair, reducing congestion and edema to achieve analgesic effects.26
This study aims to evaluate the effectiveness and safety of integrating the “Zhibian (BL54) to Shuidao (ST28)” acupuncture manipulation with analgesics for postoperative pain management in mixed hemorrhoids patients. Through randomized controlled trials, we assess the analgesic efficacy using the VAS, the analgesic efficiency and potential for elevated doses of pain medication. Additionally, we will evaluate the impact of pain on daily activities using the BPI-SF.
Conclusion
This randomized study evaluates the effectiveness of combining acupuncture with medication to relieve postoperative pain in patients with mixed hemorrhoids, aiming to establish a safe and effective treatment strategy and expand its clinical use.
Abbreviations
BL54: “Zhibian”, is an acupoint located on the Bladder Meridian of Foot-Taiyang; ST28: “Shuidao”, is an acupoint located on the Stomach Meridian of Foot-Yangming; TCM, Traditional Chinese Medicine; VAS, Visual analogue scale; MMH, Milligan-Morgan open hemorrhoidectomy; SH, Stapled Hemorrhoidectomy; NSAID, Non-steroidal anti-inflammatory drug; RCT, randomized controlled trial; CRFs, Conditional Random Fields; CNS, Central Nervous System; CCK, Cholecystokinin; NMDA, N-methlD-aspartic acid; 5-HT, 5-hydroxytryptamine; NOD1/RIP2/NF-κB, Nucleotide-binding Oligomerization Domain-containing protein 1/Receptor Interacting Serine/Threonine-protein Kinase 2/Nuclear Factor kappa-light-chain-enhancer of activated B cells.
Data Sharing Statement
No datasets were generated or analysed during the current study. All relevant data from this study will be made available upon study completion.
Ethics Approval and Informed Consent
The research has obtained ethical clearance from the Institutional Review Boards and Ethics Committees of the affiliated Acupuncture and Tuina Hospital of Shanxi University of Chinese Medicine (approval code: 2024-004). It has been registered in the Chinese Clinical Trial Registry under the identifier ChiCTR2400081302 and will adhere to the principles outlined in the Declaration of Helsinki. All participants will provide written informed consent following comprehensive explanation of the study objectives, procedures, and potential risks, designed to safeguard their rights and interests. Confidentiality of personal information and secure data storage will be strictly maintained throughout the research process.
Acknowledgments
The authors would like to thank all the participants. At present, the trial is actively enrolling participants, with the research expected to conclude by June 2025.
Funding
The authors received no specific funding for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Riss S, Weiser FA, Schwameis K, et al. The prevalence of hemorrhoids in adults. Int J Colorectal Dis. 2012;27(2):215–220. doi:10.1007/s00384-011-1316-3
2. Sun Z, Migaly J. Review of hemorrhoid disease: presentation and management. Clin Colon Rectal Surg. 2016;29(1):22–29. doi:10.1055/s-0035-1568144
3. Lorenzo-Rivero S. Hemorrhoids: diagnosis and current management. Am Surg. 2009;75(8):635–642. doi:10.1177/000313480907500801
4. Sandler RS, Peery AF. Rethinking what we know about hemorrhoids. Clin Gastroenterol Hepatol. 2019;17(1):8–15. doi:10.1016/j.cgh.2018.03.020
5. Talley NJ, Lasch KL, Baum CL. A gap in our understanding: chronic constipation and its comorbid conditions. Clin Gastroenterol Hepatol. 2009;7(1):9–19. doi:10.1016/j.cgh.2008.07.005
6. Xia J, Liu F, Li Z. Clinical study on the treatment of mixed hemorrhoids by external stripping and internal injection of anal pad retraction and fixation. Chin J Gastrointest Surg. 2018;21(12):1443–1445.
7. Rivadeneira DE, Steele SR, Ternent C, et al. Practice parameters for the management of hemorrhoids (revised 2010). Dis Colon Rectum. 2011;54(9):1059–1064. doi:10.1097/DCR.0b013e318225513d
8. Sneider EB, Maykel JA. Diagnosis and management of symptomatic hemorrhoids. Surg Clin North Am. 2010;90(1):17–32. doi:10.1016/j.suc.2009.10.005
9. Ala S, Alvandipour M, Saeedi M, et al. Effects of Topical Atorvastatin (2 %) on posthemorrhoidectomy pain and wound healing: a randomized double-blind placebo-controlled clinical trial. World J Surg. 2017;41(2):596–602. doi:10.1007/s00268-016-3749-x
10. Kirchhoff P, Clavien PA, Hahnloser D. Complications in colorectal surgery: risk factors and preventive strategies. Patient Saf Surg. 2010;4(1):5. doi:10.1186/1754-9493-4-5
11. Ravo B, Amato A, Bianco V, et al. Complications after stapled hemorrhoidectomy: can they be prevented? Tech Coloproctol. 2002;6(2):83–88. doi:10.1007/s101510200018
12. Rodríguez-Wong U, Ocharán-Hernández ME, Toscano Garibay J. Topical diltiazem for pain after closed hemorrhoidectomy. Rev Gastroenterol Mex. 2016;81(2):74–79. doi:10.1016/j.rgmx.2016.02.001
13. Joshi GP, Neugebauer EA; PROSPECT Collaboration. Evidence-based management of pain after haemorrhoidectomy surgery. Br J Surg. 2010;97(8):1155–1168. doi:10.1002/bjs.7161
14. Laughlan K, Jayne DG, Jackson D, et al. Stapled haemorrhoidopexy compared to Milligan-Morgan and Ferguson haemorrhoidectomy: a systematic review. Int J Colorectal Dis. 2009;24(3):335–344. doi:10.1007/s00384-008-0611-0
15. Ebrecht M, Hextall J, Kirtley L-G, et al. Perceived stress and cortisol levels predict speed of wound healing in healthy male adults. Psychoneuroendocrinology. 2004;29:798–809. doi:10.1016/S0306-4530(03)00144-6
16. McGuire L, Heffner K, Glaser R, et al. Pain and wound healing in surgical patients. Ann Behav Med. 2006;31(2):165–172. doi:10.1207/s15324796abm3102_8
17. Cheetham MJ, Mortensen NJ, Nystrom PO, et al. Persistent pain and faecal urgency after stapled haemorrhoidectomy. Lancet. 2000;356(9231):730–733. doi:10.1016/S0140-6736(00)02632-5
18. Shaw D, Ternent CA. Perioperative management of the ambulatory anorectal surgery patient. Clin Colon Rectal Surg. 2016;29(1):7–13. doi:10.1055/s-0035-1570023
19. Sammour T, Barazanchi AW, Hill AG; PROSPECT Group (Collaborators). Evidence-based management of pain after excisional haemorrhoidectomy surgery: a PROSPECT review update. World J Surg. 2017;41(2):603–614. doi:10.1007/s00268-016-3737-1
20. Rahimi M, Kazemeini AR, Pourtabatabaei N, et al. Comparison of topical anesthetic cream (EMLA) and diclofenac suppository for pain relief after hemorrhoidectomy: a randomized clinical trial. Surg Today. 2012;42(12):1201–1205. doi:10.1007/s00595-012-0222-9
21. Al Mamun MA, Islam K, Alam MJ, et al. Flavonoids isolated from Tridax procumbens (TPF) inhibit osteoclasts differentiation and bone resorption. Biol Res. 2015;48(1):51. doi:10.1186/s40659-015-0043-6
22. Fu H, Guo W, Zhou B, et al. Efficacy and safety of micronized purified flavonoid fractions for the treatment of postoperative hemorrhoid complications: a systematic review and meta-analysis. Phytomedicine. 2022;104:154244. doi:10.1016/j.phymed.2022.154244
23. Pei X, Song S, Li H, Lu D. Efficacy and safety of acupoint catgut embedding in treating postoperative pain of mixed hemorrhoids: a randomized controlled trial protocol. Medicine. 2021;100(19):e25948. doi:10.1097/MD.0000000000025948
24. Cao Y, Hao WW, Xie M, et al. Analysis of pain intensity and influencing factors of adverse reactions in emergency department patients with dizo-cine analgesia. Evidence-Based Care. 2019;5(8):749–751.
25. White A. A cumulative review of the range and incidence of significant adverse events associated with acupuncture. Acupuncture Med. 2004;22(3):122–133. doi:10.1136/aim.22.3.122
26. Hao CY, Zhang TS, Qi JM, et al. Acupuncture at Zhibian (BL 54) through Shuidao (ST 28) for polycystic ovary syndrome. Chin Acupuncture Moxibustion. 2015;35(5):461–464.
27. Zhang YL, Wang HJ, Cao YX, et al. Origin, development and advantageous disease spectrum of the “Zhibian (BL 54) through Shuidao (ST 28)” needling technique. Chin Acupuncture Moxibustion. 2024;44(2):200–203.
28. Wang HJ, Cao YX, Ji JQ, et al. Acupuncture of “Zhibian (BL 54) through Shuidao (ST 28)” for female stress urinary incontinence: a randomized controlled trial. Chin Acupuncture Moxibustion. 2020;40(10):1061–1064.
29. Chen T, Zhang WW, Chu YX, et al. Acupuncture for pain management: molecular mechanisms of action. Am J Chin Med. 2020;48(4):793–811. doi:10.1142/S0192415X20500408
30. van Tol RR, Kleijnen J, Watson A, et al. European Society of Coloproctology: guideline for haemorrhoidal disease. Colorectal Dis. 2020;22(6):650–662. doi:10.1111/codi.14975
31. Yang ZT, Zhang JT, Wang DX. Changes of serum levels of IL-17, IL-6 and TNF-alpha in hemorrhoids treated by internal and external treatment of traditional Chinese medicine. Chin Arch Trad Chin Medicine. 2018;36(8):1933–1935.
32. Arabi Y, Alexander-Williams J, Keighley MR. Anal pressures in hemorrhoids and anal fissure. Am J Surg. 1977;134(5):608–610. doi:10.1016/0002-9610(77)90445-7
33. Ye F, Feng YX, Lin JJ. A ropivacaine-lidocaine combination for caudal blockade in haemorrhoidectomy. J Int Med Res. 2007;35(3):307–313. doi:10.1177/147323000703500304
34. Goldstein ET, Williamson PR, Larach SW. Subcutaneous morphine pump for postoperative hemorrhoidectomy pain management. Dis Colon Rectum. 1993;36(5):439–446. doi:10.1007/BF02050008
35. Hiltunen KM, Matikainen M. Anal manometric findings in symptomatic hemorrhoids. Dis Colon Rectum. 1985;28(11):807–809. doi:10.1007/BF02555482
36. Hetzer FH, Demartines N, Handschin AE, et al. Stapled vs excision hemorrhoidectomy: long-term results of a prospective randomized trial. Arch Surg. 2002;137(3):337–340. doi:10.1001/archsurg.137.3.337
37. Chen JY, Ko TL, Wen YR, et al. Opioid-sparing effects of ketorolac and its correlation with the recovery of postoperative bowel function in colorectal surgery patients: a prospective randomized double-blinded study. Clin J Pain. 2009;25(6):485–489. doi:10.1097/AJP.0b013e31819a506b
38. Sneddon LU. Comparative physiology of nociception and pain. Physiology. 2018;33(1):63–73. doi:10.1152/physiol.00022.2017
39. Mayor D. An exploratory review of the electroacupuncture literature: clinical applications and endorphin mechanisms. Acupuncture Med. 2013;31(4):409–415. doi:10.1136/acupmed-2013-010324
40. Chen S, Wang S, Rong P, et al. Acupuncture for visceral pain: neural substrates and potential mechanisms. Evid Based Complement Alternat Med. 2014;2014:609594. doi:10.1155/2014/609594
41. Chang FC, Tsai HY, Yu MC, et al. The central serotonergic system mediates the analgesic effect of electroacupuncture on ZUSANLI (ST36) acupoints. J Biomed Sci. 2004;11(2):179–185. doi:10.1007/BF02256561
42. Kim SK, Park JH, Bae SJ, et al. Effects of electroacupuncture on cold allodynia in a rat model of neuropathic pain: mediation by spinal adrenergic and serotonergic receptors. Exp Neurol. 2005;195(2):430–436. doi:10.1016/j.expneurol.2005.06.018
43. Erthal V, da Silva MD, Cidral-Filho FJ, et al. ST36 laser acupuncture reduces pain-related behavior in rats: involvement of the opioidergic and serotonergic systems. Lasers Med Sci. 2013;28(5):1345–1351. doi:10.1007/s10103-012-1260-7
44. Kagitani F, Uchida S, Hotta H. Afferent nerve fibers and acupuncture. Auton Neurosci. 2010;157(1–2):2–8. doi:10.1016/j.autneu.2010.03.004
45. Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
46. Wu X, Cheng K, Xu C, et al. Mechanism of acupuncture and moxibustion on chronic prostatitis/chronic pelvic pain syndrome: a narrative review of animal studies. Pain Res Manag. 2021;2021:2678242. doi:10.1155/2021/2678242
47. Zhang R, Lao L, Ren K, et al. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/ALN.0000000000000101
48. Xiao-Hua YU. Electroacupuncture for pain after hemorhoids surgery. Shanghai J Acupuncture Moxibustion. 2011;30(5):304–306.
49. Wen Y, Li J, Long Q, et al. Electroacupuncture combined with catgut implantation for postoperative pain of mixed hemorrhoids. Chin Acupuncture Moxibustion. 2017;37(3):243–246.
50. Sun Y, Gan TJ, Dubose JW, et al. Acupuncture and related techniques for postoperative pain: a systematic review of randomized controlled trials. Br J Anaesth. 2008;101(2):151–160. doi:10.1093/bja/aen146
51. Liu BG, Ji LX, Hao CY, et al. Anatomic basis of Zhibian-through-Shuidao method for treatment of chronic prostatitis. Chin Acupuncture Moxibustion. 2001;21(2):27–29.
52. Jin XF, Ji LX. Clinical research on acupuncture treatment for chronic nonbacterial prostatitis and prostatodynia. China’s Naturopathy. 2008;5:9.
53. Ji LX. Experience in the treatment of difficult diseases by technical combination of acupuncture. Chin Acupuncture Moxibustion. 2019;39(1):73–76.
54. Cao YM, Jiang HZ, Li JR, et al. Experimental study on “Zhibian (BL54) through Shuidao (ST28)” acupuncture therapy for rats with asthenospermia and oligospermia. J Shanxi Univ Chin Med. 2021;22(1):26–28,32.
55. Wang HJ, Cao YX, Ji JQ, et al. 31 cases of Acupuncture of “Zhibian (BL 54) through Shuidao (ST 28)” for primary dysmenorrhea. Chin Acupuncture Moxibustion. 2019;39(11):1245–1246.
56. Ji LX. Treatment of 17 cases of postoperative urinary retention using the acupuncture technique of “Zhibian (BL 54) through Shuidao (ST28)”. J Clin Rehabil Tissue Eng Res. 2002;12:1819.
57. Chu KB, Yang LW, He LQ. Peripheral anatomical relationships of the “Zhibian (BL 54) through Shuidao (ST 28)” acupoint and mechanism exploration in treating postoperative urinary retention. Chin J Inf Trad Chin Med. 2009;16(4):98–99.
58. Hao YF, Wen JZ, Jin XF. Study on Zhibian (BL54) through Shuidao (ST28) on 5-HT content in dysmenorrhea rats induced by oxytocin. J Shanxi Univ Chin Med. 2016;17(06):11–12+15.
59. Jin X, Zhang YL, Chang BY, et al. Analgesic effect of “Zhibian” (BL54)-toward-”Shuidao” (ST28) needling technique of acupuncture on primary dysmenorrhea based on NOD1/RIP2/NF-κB signaling pathway in the rats. Chin Acupuncture Moxibustion. 2025;45(02):209–216.
60. Shen Z, Deng Q, Yang GG, et al. Therapeutic observation of acupoint thread embedding in alleviating pain after Milligan-Morgan for Mixed Hemorrhoids. Shanghai J Acupuncture Moxibustion. 2014;33(12):1129–1131.
61. Li YJ, Meng LJ. Clinical observation on the efficacy of Adzuki Bean application at Shuidao (ST28) acupoint in preventing post-hemorrhoidectomy urinary retention. Shaanxi J Trad Chin Med. 2010;31(08):1012–1013.
62. Wang HJ, Cao YX, Jin XF, et al. Effect of an acupuncture technique of penetrating through Zhibian (BL 54) to Shuidao (ST 28) with long needle for pain relief in patients with primary dysmenorrhea: a randomized controlled trial. Pain Res Manag. 2019;7978180.
63. Madoff RD, Fleshman JW. Clinical Practice Committee. American Gastroenterological Association. American Gastroenterological Association technical review on the diagnosis and treatment of hemorrhoids. Gastroenterology. 2004;126(5):1463–1473. doi:10.1053/j.gastro.2004.03.008
64. Bendtsen TF, Parras T, Moriggl B, et al. Ultrasound-guided pudendal nerve block at the entrance of the pudendal (Alcock) canal: description of anatomy and clinical technique. Reg Anesth Pain Med. 2016;41(2):140–145. doi:10.1097/AAP.0000000000000355
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.