")
Back to Journals » Journal of Pain Research » Volume 18
A Cross-Sectional Study on Current Perioperative Pain Management and Nurses’ Pain Management Self-Efficacy in China’s Interventional Department
Authors Zhang H, Meng Y, Xu X, Li Y, Li X, Hu H, Zheng L, Hu X
Received 8 August 2024
Accepted for publication 2 March 2025
Published 14 March 2025 Volume 2025:18 Pages 1291—1303
DOI https://doi.org/10.2147/JPR.S478935
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Hao Zhang,1 Ya Meng,2 Xiaoxia Xu,3 Yanwei Li,4 Xue Li,5 Hongtao Hu,1 Lin Zheng,1 Xiaochun Hu6
1Department of Interventional Radiology, The Affiliated Cancer Hospital of Zhengzhou University (Henan Cancer Hospital), Zhengzhou, People’s Republic of China; 2Department of Nursing, Zhengzhou Health Vocational College, Zhengzhou, People’s Republic of China; 3Department of Nursing, The Affiliated Cancer Hospital of Zhengzhou University (Henan Cancer Hospital), Zhengzhou, People’s Republic of China; 4Department of Pain and Palliative Medicine, The Affiliated Cancer Hospital of Zhengzhou University (Henan Cancer Hospital), Zhengzhou, People’s Republic of China; 5Department of Radiology, Daping Hospital, Army Medical University, Chongqing, People’s Republic of China; 6Minimally Invasive Interventional Operating Room, Sun Yat-sen University Cancer Center, Guangzhou, People’s Republic of China
Correspondence: Hongtao Hu, Email [email protected]
Objective: To critically evaluate the present status of perioperative pain management among nurses in interventional departments as well as to delineate the factors influencing the self-efficacy of pain management to provide a foundation for enhancing perioperative pain management practices.
Methods: This was a descriptive cross-sectional study on 941 nurses from 24 Chinese provinces and municipalities. A questionnaire was conducted to examine the current pain management practices. Independent sample t-test and analysis of variance were used for inter-group comparison. Multiple linear regression analysis was done to analyze the influencing factors of pain management self-efficacy.
Results: About 76.5% of the nurses in the interventional departments had undergone pain management training; however, more than one-third (37.6%) had not in the past two years. Merely 4.9% of nurses expressed confidence that their knowledge in pain management was sufficient to meet the demands the clinical practice. The foremost three areas of pain management information desired by the nurses in the intervention department were pain psychology (79.6%), pharmacological pain treatment (78.1%), and non-pharmacological pain interventions (77.4%). A majority (57.6%) of the nurses failed to assess the patients’ comprehension and perspectives of analgesia, elements contributing to pain exacerbation or alleviation, and the outcomes of analgesic measures. The cumulative score for the pain self-efficacy questionnaire among nurses in the intervention department was 63.95± 21.83. Multiple linear regression analysis revealed that variables such as the acquisition of pain knowledge, the frequency of pain training in the past two years, the ratio of evaluation tools employed for assessment, the prevalent utilization of multi-dimensional evaluation instruments, and professional course studies in academia were determinants influencing pain management self-efficacy.
Conclusion: Perioperative pain management by interventional department nurses in China is unstandardized and lacks continuous education. Nursing administrators should create targeted training to boost pain assessment, prevention and treatment abilities.
Keywords: intervention, pain management, the status quo, self-efficacy
Introduction
With the development of interventional methodologies, an increasing array of diseases are now amenable to diagnosis and therapeutic intervention through these techniques. Nevertheless, part of interventional procedures are often accompanied by significant pain, both during the procedure and in the postoperative phase.1 For example, the incidence of moderate-to-severe pain following transcatheter arterial chemoembolization in patients with primary liver cancer ranges from 59.3% to 85.5%.2 Among factors contributing to extended hospitalization post-procedure, pain accounted for the highest proportion, at 31%.3–5 Similarly, pain is the most prevalent symptom associated with uterine artery embolization; approximately 90% of patients experience varying degrees of postoperative pain, with around 60% reporting moderate or more severe pain within 24 hours of procedure.6,7 Inadequate pain control can detrimentally impact not only patients’ quality of life, postoperative recovery, but also reduce compliance with subsequent intervention programs for those unable to endure the pain. Nurses, as the evaluators of patients’ pain, implementers of analgesic measures, and observers of adverse reactions have the most direct and profound understanding of the effectiveness of current pain management approaches. They are thus pivotal in optimizing pain management practices.
Pain management refers to the process of controlling or alleviating pain through medical services and other means, mainly including pain assessment, pain intervention, and effectiveness evaluation.8 This cross-sectional study represents the first nationwide survey directed specifically at the nursing staff within interventional departments. The intention is to scrutinize the existing status and determinants of pain management by nurses in these specialized areas, identify any weak links in the current process of pain management, and subsequently offer insights for ameliorating pain management in patients undergoing interventional procedures. Ultimately, these findings may contribute to the collaborative promotion of a “painless intervention” paradigm, reflecting a more holistic and patient-centered approach to interventional care.
Literature Review
Minimally invasive therapy has revolutionized modern medicine. But at the same time, interventional treatments may induce varying degrees of pain during and after procedures.9 Undertreatment of pain could lead to some serious consequences, including increased risk of persistent postoperative pain, impaired rehabilitation, increased length of stay and/or hospital readmission. On the other hand, overtreatment of pain also leaded to adverse events related to excessive analgesic use, such as oversedation.10 Conversely, adequate pain management can help accelerate patient recovery and improve quality of life.11,12
In recent years, more and more innovative explorations have being made in the realm of perioperative pain management. The traditional focus on postoperative analgesia has evolved towards preventive analgesia and comprehensive perioperative pain management strategies.13–15
Nurses have close contact with patients in clinical work. They play a very important role in perioperative pain management, such as conducting pain assessment, providing pain relief measures, evaluating pain relief effects, and conducting pain health education.16 The clinical practice guideline from the American pain society emphasized once again the importance of establishing a nurse led pain management model for pain control.17
Materials and Methods
Study Design and Participants
Utilizing a convenience sampling approach and leveraging the platform of the nursing working group within the Radiology Branch of the Chinese Medical Association, a comprehensive survey was conducted targeting the operating room and ward nurses from interventional departments in the country. A total of 966 nurses from 24 provinces and municipalities directly under the Central Government completed the questionnaire. Upon inspection, those invalid questionnaires marked by regular answers and responses under one minute were discarded, resulting in 941 valid questionnaires, equating to an effective recovery rate of 97.41%. Inclusion Criteria: (1) Nurses actively engaged in interventional wards and interventional operating rooms; (2) Individuals possessing a valid nurse’s practice certificate. Exclusion Criteria: Nurses with less than 3 months of experience in the interventional department. All respondents were duly informed and consented to participate in this study on a voluntary basis.
Instruments
A self-designed demographic information form was used, which encompassed information on the nurses’ province, age, gender, department, years of practice, educational background, professional title, pain knowledge training (six items), and implementation of pain management in practice (15 items).
Pain Management Self-Efficacy Questionnaire
This questionnaire was originally devised by Macindo et al and translated by Li et al, which including 3 dimensions and 21 items.18,19 Items 1–14 pertain to the comprehensive management of pain, focusing on the nurses’ role in the treatment, management, and documentation of pain; items 15–18 are dedicated to the pain assessment dimension; and items 19–21 are supplementary explanations related to pain. The instrument employs a Likert-6 scoring scheme ranging from “Completely Uncertain” = 0 points to “Completely Certain” = 5 points, with a total score range of 0–105 points. A higher score is indicative of a higher level of self-efficacy in pain management among nurses. The reliability and validity of the questionnaire were robust, with a Cronbach’s α coefficient of 0.901, and the coefficients for each dimension range from 0.869 to 0.924. The validity of the questionnaire and its various items were above 0.85.
Data Collection
During October 1–31, 2022, data were collected via the professional survey platform Wenjuanxing (www.wjx.cn). The survey was developed by creating a customized questionnaire featuring multiple-choice items, 5-point Likert scales, and open-ended questions. Conditional logic jumps and mandatory response settings were implemented to enhance data validity, followed by a systematic preview to ensure technical functionality. The finalized survey was distributed as a QR code through the Nursing Working Committee’s WeChat group affiliated with the Radiology Branch of the Chinese Medical Association, targeting certified interventional radiology nurses representing provincial-level medical institutions across China. Upon closure, response data were automatically aggregated by the platform and exported in Excel (XLSX) format for subsequent analysis.
The questionnaire was divided into two main sections: the first encompassed the instructions, delineating the research objectives, significance, and guidance for completion, while the second encapsulated the content of the questionnaire itself. Every question required a response, and through meticulous customization of the attributes of each question, along with a stringent provision allowing only a single completion per account. The potential occurrence of invalid or redundant questionnaires (such as those featuring omissions or erroneous entries) was substantially minimized.
The platform’s automated data aggregation features were utilized exclusively for dataset retrieval. Following data acquisition, Dr. Ya Meng (co-author) conducted statistical analyses using SPSS Statistics (version 25.0; IBM Corp.), employing dual verification protocols to ensure data integrity during software importation. Both descriptive and inferential statistical approaches were systematically applied to examine the compiled dataset.
Statistical Analysis
Data retrieved from the “Wenjuanxing” platform were imported into the SPSS 25.0 software for comprehensive statistical analysis. Descriptive statistics for the general data of nurses were expressed using frequency and percentage, while measurement data conforming to a normal distribution were articulated as mean ± standard deviation. Comparative analyses were undertaken through independent sample t-tests and analysis of variance (ANOVA) between groups. The influential determinants of pain management self-efficacy among nurses in the interventional department were explored through multiple linear regression techniques. A p-value of less than 0.05 was designated as the threshold for statistical significance.
Results
General Information of Nurses
The study participants predominantly consisted of women (93.1%), with ages ranging from 21 to 59 years and a mean age of (37.14±7.79) years. The respondents were chiefly engaged in comprehensive interventional disciplines (58.8%) and tumor interventional specialties (21.1%). The distribution across nursing units comprised the interventional operating room (59.5%) and the interventional ward (40.5%), as detailed in Table 1.
 |
Table 1 General Information of Nurses in Interventional Department (n=941) |
Pain Training and Pain Management in Work
Insights into the subjects’ knowledge of pain, their selection of tools to gauge pain intensity, the impediments faced by medical staff in the intervention of perioperative pain management, and the department’s mode of pain management are depicted in Table 2.
 |
Table 2 Pain Training and Pain Management of Nurses in Interventional Department (n=941) |
The Score of Pain Management Self-Efficacy of Nurses in Interventional Department
The average score for each item of the pain management self-efficacy questionnaire for nurses in the interventional department was (3.05±1.04). The mean score of the pain assessment dimension was the highest (3.22±1.09), whereas the comprehensive management dimension yielded the lowest average score (2.98±1.06), as presented in Table 3.
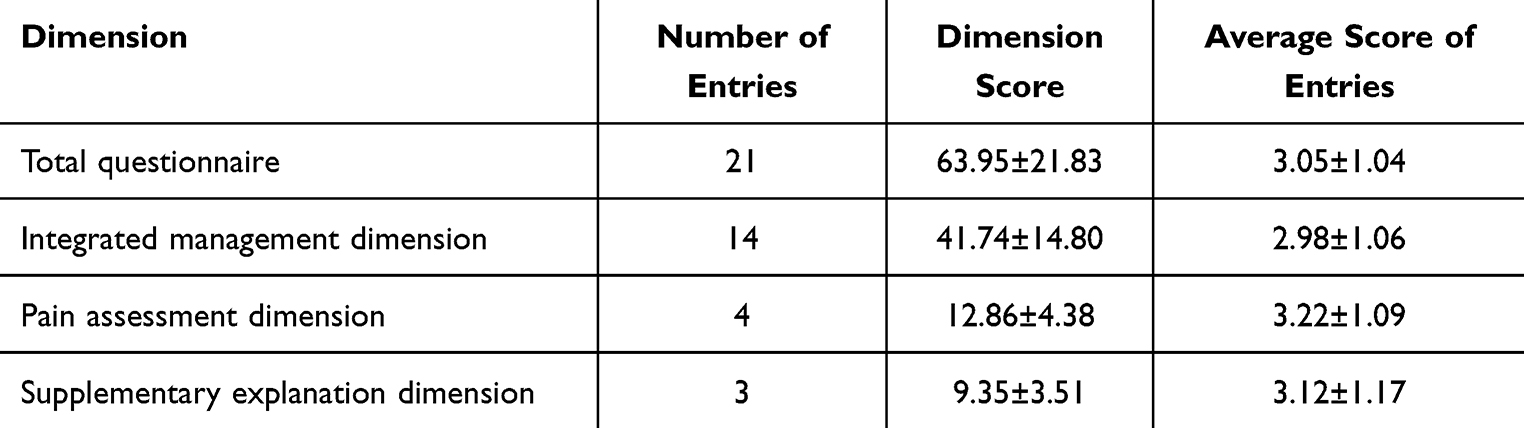 |
Table 3 Scores of Pain Management Self-Efficacy of Nurses in Intervention Department (n=941) |
Comparison of Pain Management Self-Efficacy Scores of Nurses in Interventional Departments with Different Characteristics
A comparative analysis was conducted based on factors such as the receipt of pain knowledge training, the employment of preventive analgesia, the study of specialized pain courses during education, pain-related training within the last two years, the proportion of interventional surgeries performed under local anesthesia in the department, the percentage of patients assessed using specific tools, and the self-efficacy scores for pain management among nurses across various interventional departments. The observed differences were statistically significant (P<0.05), as indicated in Table 4.
 |
Table 4 Single Factor Analysis of Pain Management Self-Efficacy Questionnaire of Nurses in Intervention Department |
Multivariate Analysis of Influencing Factors of Pain Management Self-Efficacy of Nurses in Interventional Department
A multivariate linear regression analysis was executed, taking the pain management self-efficacy score of the nurses in the interventional department as the dependent variable. Independent variables encompassed gender (male=0, female=1), age, professional title (nurse=1, primary nurse=2, supervisor nurse=3, deputy chief nurse and above=4), receipt of pain knowledge education (yes=0, no=1), professional course studies in school (no=1, one or more chapter courses=2, independent elective courses=3, independent compulsory courses=4). The results elucidated that factors such as the acquisition of pain knowledge, the quantity of pain thematic training undertaken in the past two years, the proportion of assessment tools employed, the frequent utilization of multi-dimensional assessment tools, and the instruction in professional courses in school significantly influenced the self-efficacy of pain management among nurses in the interventional department (R2=0.222, F=18.801, P<0.001), as elucidated in Table 5.
 |
Table 5 Multiple Linear Regression Analysis of Influencing Factors of Pain Management Self-Efficacy of Nurses in Interventional Department |
Discussion
Insufficient Pain Continuing Education for Nurses in Interventional Departments
The findings of this study highlight a significant gap in the continuing education of nurses regarding pain management in interventional departments. Despite 76.5% of nurses having received some form of pain management training, more than one-third (37.6%) had not participated in any pain-related training in the past two years. This lack of ongoing education is concerning, as only 4.9% of nurses felt confident that their knowledge was sufficient to meet the demands of clinical practice. Pain, often referred to as the “fifth vital sign”, should be a core component of annual nursing training programs. Incorporating pain case rounds into clinical practice could enhance nurses’ clinical thinking and decision-making skills in pain management.
The top three areas of pain management knowledge that nurses expressed a desire to learn more about were pain psychology (79.6%), pharmacological pain treatment (78.1%), and non-pharmacological pain interventions (77.4%). These findings align with the self-efficacy scores, which suggest that nurses’ understanding of pain management is still lacking. Therefore, future training programs should focus on these areas, employing diverse teaching methods such as flipped classrooms, case-based learning, and scenario simulations to improve both theoretical knowledge and practical skills.
Poor Clinical Pain Management Practices
Effective pain management begins with prompt and accurate pain assessment, which can significantly reduce postoperative complications related to pain.20 However, this study revealed that 57.9% of nurses did not use multidimensional pain assessment tools, focusing primarily on the location and intensity of pain while neglecting other critical aspects such as the nature and duration of pain. This finding is consistent with previous research by Chen et al, which suggested that nurses often prioritize the immediate relief of pain over a comprehensive assessment.21 This may be due to the high workload and time constraints faced by nurses, which limit their ability to conduct thorough pain assessments.21
To address this issue, nursing administrators should integrate pain management into existing clinical workflows, reducing the additional burden on nurses and ensuring that pain management does not become a superficial task. Additionally, as patients increasingly demand a more comfortable and pain-free experience during interventional procedures, nurses must expand their assessments to include the adverse effects of pain on patients and the efficacy of analgesic interventions. This will enable them to adopt alternative strategies for patients who do not respond well to initial treatments.
Ineffective Pain Management Strategies
The study found that 54.3% of departments only initiated analgesic interventions after patients reported pain, indicating that pain management strategies in many interventional departments are reactive rather than proactive. This approach is not aligned with current best practices, which emphasize preventive analgesia and multimodal pain management strategies. Ineffective pain management can negatively impact patients’ quality of life, postoperative recovery, and overall satisfaction with care. It may also lead to resistance to subsequent interventional treatments, ultimately affecting the efficacy of the therapy.13
To improve pain management, a comprehensive and systematic approach is needed, involving collaboration among anesthesiologists, interventional physicians, and nurses. Multimodal analgesia, which combines different analgesic drugs and techniques, should be employed to achieve seamless, continuous, and effective pain management. This approach can help minimize adverse reactions and improve patient comfort and satisfaction.22
Patient-Related Barriers to Pain Management
The study identified several patient-related barriers to effective pain management, including misconceptions about pain (eg, fear of addiction to analgesics), difficulty in accurately reporting pain, poor compliance with pain management protocols, and adverse drug reactions such as dizziness, nausea, and constipation. These barriers highlight the need for nurses to educate patients about pain concepts, self-assessment techniques, and the safety of analgesic medications. Creative and diverse educational approaches, such as lectures, discussions, manuals, videos, and social media, can help correct misconceptions, encourage accurate pain reporting, and alleviate patients’ fears.23,24
Non-Pharmacological Pain Management Strategies
Non-pharmacological pain management strategies, such as psychological support (96.9%) and distraction techniques (70.4%), were commonly used by nurses in the interventional department. These findings are consistent with previous research by Wang et al.22 Tailored psychological nursing care should be rendered to meet individual patient needs, soothing apprehensions and bolstering confidence in treatment. Concurrently, therapeutic modalities such as acupoint massage and/or music therapy may be judiciously selected.19
Factors Influencing Pain Management Self-Efficacy
Self-efficacy, defined as an individual’s belief in their ability to perform specific tasks, plays a crucial role in pain management.18 This study found that several factors significantly influenced nurses’ self-efficacy in pain management, including the acquisition of pain knowledge, the frequency of pain-related training, the use of multidimensional assessment tools, and exposure to professional pain management courses during academic training.
The study revealed that only 44.0% of nurses had the opportunity to learn about pain management during their academic studies, with a mere 1.3% having access to it as an independent compulsory course. This lack of formal education in pain management has resulted in a deficiency in both knowledge and skills among nurses. Therefore, nursing curricula in Chinese colleges and universities should be revised to include more comprehensive and in-depth pain management content.18
Existing studies articulate that systematic and continuous professional pain education can enhance nurses’ knowledge and skills in pain management, rectify misconceptions, amend attitudes towards pain management, and subsequently refine both pain management behaviors and nursing practices.25 However, only 6.3% of nurses in this study had participated in more than two pain-related training sessions in the past two years, indicating a lack of systematic and structured pain education. This suggests a paucity in the interventional pain training received by these nurses, with the lack of systematic structure and coherence leading to inadequate depth and precision in pain management knowledge.26 Therefore, nursing staff must pursue continuous learning to refresh their knowledge and insights into pain assessment and management. Simultaneously, fostering communication and collaboration among professional groups should be encouraged to enhance pain management.27
The meticulous and comprehensive assessment of pain stands as the cornerstone for efficacious pain management and bears significant implications for the design and modification of intervention programs and nursing strategies.28,29 Findings from this study indicate that the absence of quantified pain assessment tools precludes the establishment of a foundation for the implementation of intervention measures, culminating in suboptimal clinical pain management. This underscores the need for future training of nurses in interventional departments to place greater emphasis on the principles and methodologies of pain assessment.
The Importance of Multidimensional Pain Assessment
The use of multidimensional pain assessment tools was identified as a key factor influencing nurses’ self-efficacy in pain management. These tools provide a holistic evaluation of pain, including its intensity, nature, location, and impact on patients’ physical and psychological well-being. However, 57.9% of nurses in this study did not use these tools, which may have contributed to suboptimal pain management practices. Future training programs should emphasize the principles and methodologies of pain assessment, encouraging nurses to adopt a more comprehensive approach to pain management.28
Conclusion
In conclusion, the current state of pain management in interventional departments in China is characterized by a lack of standardized practices, insufficient continuing education, and inadequate pain assessment and intervention strategies. Nurses’ self-efficacy in pain management is influenced by several factors, including their access to pain knowledge, the frequency of pain-related training, and the use of multidimensional assessment tools.
To improve perioperative pain management, it is essential to establish a standardized interventional pain management system, develop clear guidelines, and promote collaboration among anesthesiologists, interventional physicians, and nurses. Preventive analgesia, multimodal analgesia, and individualized pain management strategies should be integrated into clinical practice to achieve optimal therapeutic outcomes. Additionally, nursing education and training programs should be enhanced to ensure that nurses are equipped with the knowledge and skills necessary to provide effective pain management.
By addressing these issues, healthcare providers can work towards achieving a “painless intervention” paradigm, improving patient comfort, satisfaction, and overall outcomes in interventional procedures.
Ethics Statement
The Institutional Ethics Committee of Henan Cancer Hospital approved this study (21-KY-0123), and it was conducted by the Declaration of Helsinki. All procedures were carried out in conformity with pertinent rules and regulations in ethical declarations. All participants provided informed consent.
Acknowledgments
The authors appreciate all participants for their participation of the study. The authors also thank the nursing working group platform of the Radiology Branch of the Chinese Medical Association for the investigation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study received full research funding from Henan Province Medical Science and Technology Research Project (LHGJ20210217), and the Medical Education Research Project of Henan Province (WJLX2024036), and the General Project of Henan Provincial Education Science Planning for 2024 (2024YB0564).
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Cashman JN, Ng L. The management of peri- and postprocedural pain in interventional radiology: a narrative review. Pain Manag. 2017;7(6):523–535. doi:10.2217/pmt-2017-0024
2. Guan Y, Tian Y, Fan YW. Pain management in patients with hepatocellular carcinoma after transcatheter arterial chemoembolisation: a retrospective study. World J Gastrointest Surg. 2023;15(3):374–386. doi:10.4240/wjgs.v15.i3.374
3. Luo J, Shao GL, Zheng JP, et al. The occurrence pattern and influencing factors of abdominal pain after hepatic artery chemoembolization for primary liver cancer. J Intervent Radiol. 2017;26:613–617.
4. Chen S, Ji R, Shi X, et al. Retrospective analysis of efficacy, safety, and prognostic factors in a cohort of Chinese hepatocellular carcinoma patients treated with drug-eluting bead transarterial chemoembolization. Braz J Med Biol Res. 2019;52(12):e8467. doi:10.1590/1414-431X20198467
5. Guo Y, Jia SM. Research progress on pain status and influencing factors after hepatic artery chemoembolization in liver cancer patients. J Nurs Cont Educ. 2020;35(4):326–329.
6. Pisanie JLD, Commander CW, Burke CT. Management of postprocedural uterine artery embolization pain. Semin Intervent Radiol. 2021;38(5):588–594. doi:10.1055/s-0041-1739161
7. Saibudeen A, Makris GC, Elzein A, et al. Pain management protocols during uterine fibroid embolisation: a systematic review of the evidence. Cardiovasc Intervent Radiol. 2019;42(12):1663–1677. doi:10.1007/s00270-019-02327-1
8. Swift A. The importance of assessing pain in adults. Nurs Times. 2015;111(41):12–17.
9. Sun J, Zhou G, Xie X, et al. Efficacy and safety of drug-eluting beads transarterial chemoembolization by CalliSpheres® in 275 hepatocellular carcinoma patients: results from the Chinese CalliSpheres® Transarterial Chemoembolization in Liver Cancer (CTILC) study. Oncol Res. 2020;28(1):75–94. doi:10.3727/096504019X15662966719585
10. Argoff CE. Recent management advances in acute postoperative pain. Pain Pract. 2014;14(5):477–487. doi:10.1111/papr.12108
11. Polanco-García M, García-Lopez J, Fàbregas N, Meissner W, Puig MM; PAIN-OUT-Spain Consortium. Postoperative pain management in Spanish hospitals: a cohort study using the PAIN-OUT registry. J Pain. 2017;18(10):1237–1252. doi:10.1016/j.jpain.2017.05.006
12. Scarborough BM, Smith CB. Optimal pain management for patients with cancer in the modern era. CA Cancer J Clin. 2018;68(3):182–196. doi:10.3322/caac.21453
13. Auvin S, Bissler JJ, Cottin V, et al. A step-wise approach for establishing a multidisciplinary team for the management of tuberous sclerosis complex: a Delphi consensus report. Orphanet J Rare Dis. 2019;14(1):91. doi:10.1186/s13023-019-1072-y
14. Wang YQ, Liu YP, Wang YL, et al. Construction and practice of pain management standard process for patients with hepatic artery chemoembolization. Chin J Nurs. 2020;55:558–563.
15. Wick EC, Grant MC, Wu CL. Postoperative multimodal analgesia pain management with nonopioid analgesics and techniques: a review. JAMA Surg. 2017;152(7):691–697. doi:10.1001/jamasurg.2017.0898
16. Phelan SM, Hardeman RR. Health professionals’ pain management decisions are influenced by their role (nurse or physician) and by patient gender, age and ethnicity. Evid Based Nurs. 2015;18(2):58. doi:10.1136/eb-2014-101917
17. Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council [published correction appears in J Pain. 2016;17(4):508–510. Dosage error in article text]. J Pain. 2016;17(2):131–157. doi:10.1016/j.jpain.2015.12.008
18. Macindo JRB, Soriano CAF, Gonzales HRM, et al. Development and psychometric appraisal of the pain management self-efficacy questionnaire. J Adv Nurs. 2018;74:1993–2004. doi:10.1111/jan.13582
19. Li YH, Zhang GL, Weng HW. Localization of pain management self-efficacy questionnaire and its reliability and validity test. J Clin Nurs Pract. 2018;4:26–30.
20. Alghadir AH, Anwer S, Iqbal A, et al. Test–retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J Pain Res. 2018;11:851–856. doi:10.2147/JPR.S158847
21. Chen JJ, Tong YG, Li XY. The current situation and influencing factors of pain nursing practice among nurses in tertiary and first-class hospitals in China. Nurs Res. 2017;31:4193–4198.
22. Wang XY, Jia ZZ, Xu XF, et al. Expert consensus on perioperative pain management in interventional therapy of liver malignant tumors. J Intervent Radiol. 2022;31:943–948.
23. Marris D, Theophanous K, Cabezon P, et al. The impact of combining pain education strategies with physical therapy interventions for patients with chronic pain: a systematic review and meta-analysis of randomized controlled trials. Physiother Theory Pract. 2021;37(4):461–472. doi:10.1080/09593985.2019.1633714
24. Schwartz R, Urits I, Kaye AD, et al. Opioids and the predilection for violence in the pain clinic: a physician’s perspective. Pain Ther. 2019;8(2):159–161. doi:10.1007/s40122-019-00134-7
25. Achaliwie F, Wakefield AB, Mackintosh-Franklin C. Does education improve nurses’ knowledge, attitudes, skills, and practice in relation to pain management? An integrative review. Pain Manag Nurs. 2023;24(3):273–279. doi:10.1016/j.pmn.2022.12.002
26. Ahmadi S, Vojdani P, MortezaBagi HR. The study of nurses’ knowledge and attitudes regarding pain management and control in emergency departments. BMC Emerg Med. 2023;23(1):26. doi:10.1186/s12873-023-00793-y
27. Peterson A, Berggården M, Schaller AS, Larsson B. Nurses’ advocacy of clinical pain management in hospitals: a qualitative study. Pain Manag Nurs. 2019;20(2):133–139. doi:10.1016/j.pmn.2018.09.003
28. Scher C, Petti E, Meador L, et al. Multidimensional pain assessment tools for ambulatory and inpatient nursing practice. Pain Manag Nurs. 2020;21(5):416–422. doi:10.1016/j.pmn.2020.03.007
29. Deldar K, Froutan R, Sedaghat A, et al. Continuing nursing education: use of observational pain assessment tool for diagnosis and management of pain in critically ill patients following training through a social networking app versus lectures. BMC Med Educ. 2020;20(1):247. doi:10.1186/s12909-020-02159-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Healthcare Workers’ Pain Management-Correlated Barriers and Self-Efficacy at Teaching Hospitals in the City of Ismailia
Elmansy FM, Elbqry MG, Al-Ahdal SA, Ashmieg FSO, Elgazzar SE, Nasir PO, Abdullahi NM
Journal of Pain Research 2025, 18:2417-2425
Published Date: 13 May 2025