")
Back to Journals » Journal of Pain Research » Volume 18
Healthcare Workers’ Pain Management-Correlated Barriers and Self-Efficacy at Teaching Hospitals in the City of Ismailia
Authors Elmansy FM , Elbqry MG , Al-Ahdal SA, Ashmieg FSO , Elgazzar SE , Nasir PO, Abdullahi NM
Received 11 January 2025
Accepted for publication 7 May 2025
Published 13 May 2025 Volume 2025:18 Pages 2417—2425
DOI https://doi.org/10.2147/JPR.S515344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Karina Gritsenko
Fatma Mohamed Elmansy,1 Mohamed Goda Elbqry,1 Saddam Ahmed Al-Ahdal,1 Fatima S O Ashmieg,1 Samia Eaid Elgazzar,1 Patience Osose Nasir,2 Nasiru Mohammed Abdullahi3
1Department of Medical and Surgical, College of Nursing, Qassim University, Buraydah City, 52571, Saudi Arabia; 2Accident and Emergency Department, King Fahad Specialist Hospital, Buraydah City, 51452, Saudi Arabia; 3Department of Psychiatric and Mental Health, and Community Health, College of Nursing, Qassim University, Buraydah, 52571, Saudi Arabia
Correspondence: Mohamed Goda Elbqry, Department of Medical and Surgical, College of Nursing, Qassim University, P.O. Box: 52571, Buraydah City, Saudi Arabia, Tel +966560403003, Email [email protected]
Aim: To determine healthcare workers’ pain management-correlated barriers and self-efficacy at teaching hospitals in the city of Ismailia, Egypt.
Methods: A descriptive study was enrolled. 117 healthcare workers (nurses and physicians) were recruited through a purposive sampling technique. An online valid closed-ended online questionnaire was used to collect data between June and December 2023 to assess demographic data, pain management-correlated barriers, and self-efficacy.
Results: The findings indicated that medical staff, patients and families, and the healthcare system each perceived distinct barriers to care, with mean scores of 4.88 (SD = 0.56), 5.65 (SD = 1.74), and 3.11 (SD = 0.36), respectively. Furthermore, healthcare workers’ self-efficacy was found to be moderate, with a mean score of 12.99 (SD = 4.02) A statistically significant difference (p ≤ 0.05) was found in healthcare workers’ self-efficacy based on their workplace and years of experience.
Conclusion: In the critical care setting, healthcare workers perceived correlated barriers as significant obstacles to successful pain management. High self-efficacy in pain management was reported among healthcare workers in the critical care unit. Effective pain management necessitates specialized training programs that incorporate diverse tools and consider patients’ cultural backgrounds. Integrating cultural competence into academic curricula and hospital training programs is vital. Healthcare organizations and policymakers should prioritize addressing the identified barriers to improve healthcare delivery and outcomes.
Study Implication: Firstly, enhancing pain management practices is crucial in improving patient care. Identifying and addressing the barriers that healthcare professionals face in pain management. Improving healthcare workers’ self-efficacy in pain management for consistent and effective care, reducing unnecessary suffering and bridge the gaps to improve overall patient outcomes.
Keywords: barriers, healthcare workers, pain management, self-efficacy
Introduction
Pain is a complex and multifaceted experience that affects an individual’s quality of life. Pain is a common symptom that most patients suffer from in various medical conditions, which makes its evaluation and management one of the most crucial elements of healthcare.1 According to the World Health Organization (WHO), most of the patients with serious illnesses like cancer, or chronic pain conditions, are experiencing pain.2 Ineffective pain management for critically ill patients at intensive care units (ICUs) is a serious public health concern that can result in extended mechanical ventilation, diminished physical functioning, and emotional well-being. Healthcare workers are responsible for diagnosing, assessing, and delivering appropriate pain treatment to patients admitted in ICUs, as well as identifying the challenges they confront, which is critical for designing effective pain treatment programs. Pain management is an important and effective component of healthcare.1 It is addressing a common problem that affects both individuals and societies. Epidemiological studies show that pain influences around 20% of adults globally, with prevalence rates between 8% and 55% across various countries. In the United States, an estimated 50 million adults experienced chronic pain in 2016, leading to substantial healthcare costs and lost productivity.3
Economically, the burden of pain is profound; in the US, the total annual cost of pain, including healthcare expenses and lost productivity, ranges from $560 to $635 billion, surpassing the costs associated with heart disease or cancer.2 Effective pain management not only alleviates individual suffering but also reduces these economic burdens by improving quality of life and enhancing functional abilities, thereby decreasing healthcare utilization and increasing productivity. However, there are many barriers that hinder the health workers in assessing and pain management that the patient suffers from. There are various sources of these barriers, the most important of which may arise from within the health system itself, as well as the convictions and beliefs of the health worker, in addition to external factors that may relate to patients.4 Among the barriers that may prevent effective pain management are the lack of continuity in ongoing related education and the inefficiency of the courses provided to health care professionals, if any leading to insufficient treatment options and misconceptions about opioid use and addiction. Interdisciplinary communication challenges and fragmented care hinder collaboration among providers, resulting in inconsistent patient messaging.2
Institutional policies may restrict access to pain relief resources, especially for vulnerable populations. On the part of the patient, misunderstandings and cultural factors can deter individuals from seeking help. These complex issues highlight the need for comprehensive strategies to improve pain management practices, enhancing patients’ outcomes and ensuring effective pain relief.5 Self-efficacy refers to an individual’s sense of control over novel or inconvenient situations or challenges by anticipating their own competent behavior. Individuals with higher self-efficacy are more inclined to select ambitious goals, exert additional effort to achieve them, and feel more competent than those with lower self-efficacy. Self-efficacy beliefs, therefore, have a significant impact on people’s feelings, thoughts, and actions. As a result, the construct of self-efficacy has become an essential part of research on health and health behaviors.6 Bandura’s self-efficacy theory plays a crucial role in health workers’ pain management decisions, influencing their confidence in addressing patient pain. Barriers such as insufficient training and lack of resources prevent the self-efficacy of medical care providers, exacerbating pain challenges. Recent studies show that improving knowledge and attitudes can significantly improve nurses’ self-efficacy in managing postoperative pain.7 In addition, patients’ self-efficacy is positively correlated with satisfaction in care, underlining the need for teaching hospitals to foster an environment of power. Empowering health workers through specific programs can improve pain control and self-efficacy, which leads to better patient care.8
Healthcare workers play a crucial role in pain management. They often face barriers in this regard, which makes pain management ineffective. On the other hand, these challenges reduce their self-efficacy, which reduces self-confidence regarding pain management. Continuing education and providing appropriate resources and a supportive environment to healthcare professionals will inevitably help them overcome these barriers and provide better pain management solutions to their patients.9 Ultimately, concerning pain management in the prementioned settings, especially around critical care, there is a scarcity of studies that have assessed healthcare workers’ pain management-correlated barriers and self-efficacy at teaching hospitals. So, the research question was what are healthcare workers’ pain management-correlated barriers and self-efficacy at teaching hospitals?
Materials and Methods
Study Design and Participants
This study employed a descriptive study to determine healthcare workers’ pain management-correlated barriers at a teaching hospital in Ismailia city, Egypt. It was conducted from June to December 2023 (Figure 1) in the critical care unit, oncology unit, cardiac care unit, and emergency unit of the hospital. The estimated sample size was calculated based on Fisher’s formula among 162 healthcare workers, but overall, 117 questionnaires were returned due to different exclusion criteria, which was mostly busy time. The Fisher equation is expressed through the following formula: (1 + i) = (1 + r) (1 + π). Where: i – the nominal interest rate, r – the real interest rate, and π – the inflation rate. Participants were recruited using a purposive sampling technique, with the following inclusion criteria: individuals who willingly consented to participate, had a minimum of six months of experience, and represented both genders. Participants who planned for vacation, refused or were busy were excluded from the study (Table 1).
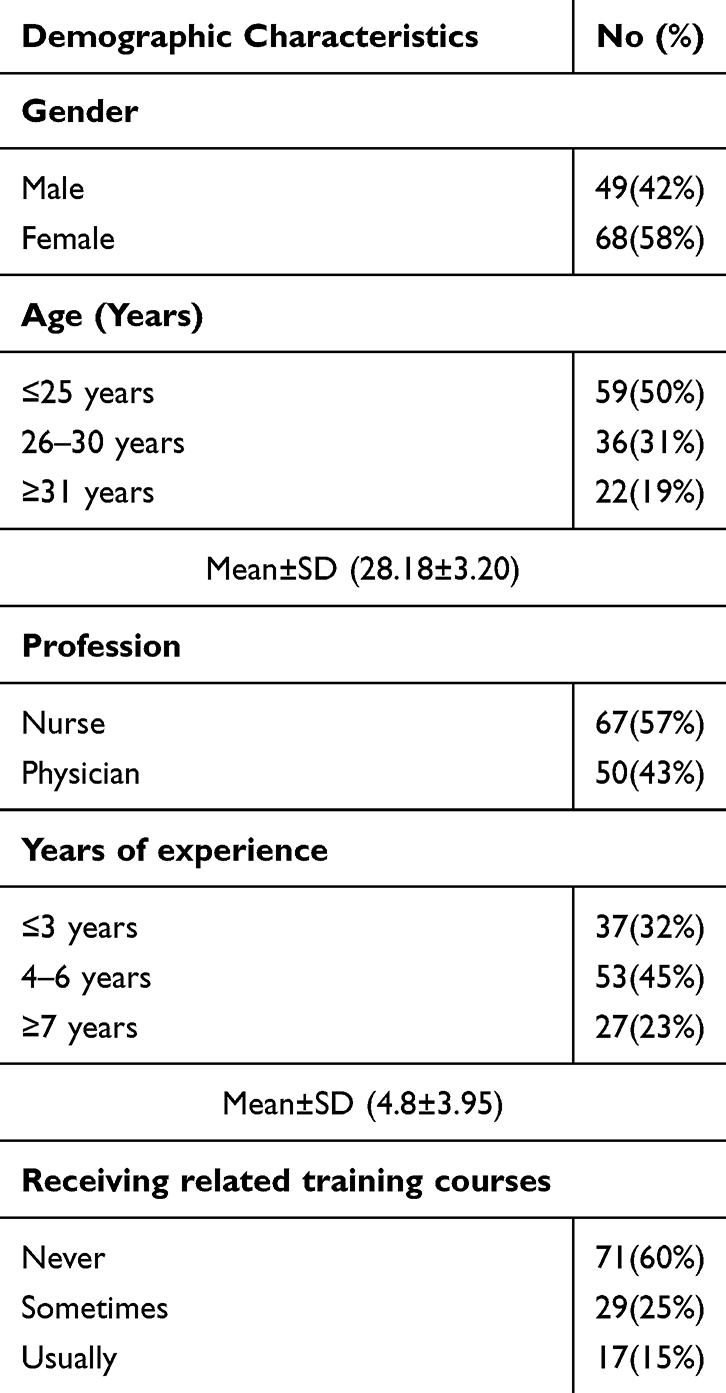 |
Table 1 The Studied Healthcare Workers’ Demographic Characteristics. (n = 117) |
 |
Figure 1 The studied healthcare workers’ working place. (n=117). |
Data Collection Tools
A valid and reliable self-administrated online survey in the form of multiple-choices and tru of false questions to facilitate data collection and time consuming. It consisted of three sections: (1) information about the demographic healthcare characteristics, such as age, gender, profession, working place, and years of experience. (2) The National Institutes of Health barriers to pain management tool adapted to determine pain management-related barriers among critically ill patients.1 The tool underwent pilot testing and was reviewed by a panel of pain management experts comprising nine healthcare workers. The tool demonstrated high reliability, with a Cronbach’s alpha coefficient exceeding 0.70. It consisted of two sections: one assessing medical staff, patient, and family-related barriers (9 items), and another evaluating healthcare system-related barriers (5 items). Statistically, the tool utilized a 4-point Likert scale, where: scale 1 specified “never’, 2 specified “sometimes’, 3 specified “often”, and 4 specified “always”. For analysis purposes, the scale was dichotomized, where: scales 1 and 2 were categorized as “no barrier”, while scales 3 and 4 were categorized as “presence of a barrier”. (3) General Self-Efficacy Scale (GSES): This scale is a viable and reliable measure for assessing the general sense of perceived self-efficacy, with the goal of predicting coping with daily challenges as well as the capacity to adjust after encountering a variety of stressful daily situations.10 The scale consists of ten items, with response grades ranging from 1 (not at all true) to 4 (exactly true) on a four-point Likert scale. The overall score runs from 10 to 40, with higher values indicating greater self-efficacy and scores below 30 indicating low self-efficacy.
Data Collection Process
Following informed consent, participants acknowledged understanding the study’s objectives. The data collection tool was validated, and subsequent to obtaining hospital approval, the data collection procedure was initiated. The lead author distributed the online questionnaires to participants who gave their informed consent as a mandatory condition term to continue the survey and agreed to participate in the study within 3–5 minutes. A simplified Arabic and English closed-ended questionnaire were shared among the healthcare workers, and the authors provided a detailed explanation of the project’s goal and its effects on the community and hospital. Completed questionnaires were returned to Microsoft Forms.
Statistical Analysis
The data was statistically analyzed using IBM’s statistical package for social studies (SPSS) version 25, which was established in Chicago, Illinois, USA. Categorical variables were shown as quantities and percentages. The numerical variables were provided as mean ± SD. The Kruskal–Wallis’s test was fit to the variables, if the p-value is <0.05 at the 95% confidence of interval, this variable is statistically significant.
Results
The Studied Healthcare Workers’ Demographic Characteristics
This table exhibits more than half (58%) of the participants were female, and half their age ≤ 25 years. Moreover, less than two-quarters (57%) were nurses and most (45%) had 4–6 years of experience, less than or equal to 22 years, followed by more than three-quarters (85.3%) being female. More than half (70%) never received related training courses. (Table 1)
The Studied Healthcare Workers’ Pain Management-Correlated Barriers
Healthcare workers perception of pain management-correlated barriers by gender: the female group scored the highest mean (SD) of 4.01 (1.90); 4.01 (1.05); and 3.30 (0.76) compared to the male group, who scored the lowest mean (SD) of 4.01 (1.90); 3.09 (1.03); and 3.01 (0.90), respectively. Kruskal–Wallis’s test exhibits not a statistically significant difference between healthcare workers’ perceived barriers by gender (p-value ≤0.05). Concerning healthcare workers’ perceived barriers by profession, the physician group stated the highest mean (SD) than nurses. There was not a statistically significant difference between healthcare workers’ perceived barriers by age, profession, and experience (p-value ≤0.05). Nurses who usually received related training courses had the highest mean (SD) compared to those who did not receive the training courses. There was not a statistically significant difference between healthcare workers’ perceived barriers to receiving related training courses. (Table 2)
 |
Table 2 The Studied Healthcare Workers’ Pain Management Correlated Barriers and Self-Efficacy Mean, Standard Deviation and Kruskal-Walli’s Test Through Their Demographic Characteristics. (n = 117) |
About healthcare workers perception of pain management self-efficacy by gender, the male group counted the highest mean (SD) of 12.46 (3.02), compared to the male group, who scored the lowest mean (SD) of 12.03 (3.20). A Kruskal–Wallis’s test displays a statistically significant difference between healthcare workers’ self-efficacy by gender (p-value ≤0.05). Regarding healthcare workers’ self-efficacy by working place, the critical care unit group declared the highest mean (SD) of 15.06 (1.88) compared to other working places mean (SD). There was a statistically significant difference between healthcare workers’ self-efficacy by working places (p-value ≤0.05). While their self-efficacy by years of experience in the ≥7-year group confirmed the highest mean (SD) of 4.99 (1.01) than other years of experience mean (SD). There was a statistically significant difference between healthcare workers’ self-efficacy by years of experience (p-value ≤0.05). (Table 2)
The Studied Healthcare Workers’ Working Place
It shows that about more than one-quarter (27%; 26%; 25%) of the participants worked at the critical care unit, oncology unit, and emergency unit consecutively, while less than one-quarter (22%) worked in the cardiac care unit. (Figure 1)
Discussion
This study assessed healthcare workers’ pain management-correlated barriers and self-efficacy at teaching hospitals in Egypt. A closer examination of the data (Table 2) revealed that, female healthcare workers reported higher mean scores for barriers related to medical staff (4.01 ± 1.90), patient and family (4.01 ± 1.05), and health system (3.30 ± 0.76) compared to male healthcare workers, who reported lower mean scores for these barriers (3.09 ± 1.03, 3.01 ± 0.90, respectively). This corroborates with findings from Recent studies with underlining significant gender perceptions surrounding pain management barriers among health workers. For example, a study highlights how social stigma affects access to medical care for marginalized people, revealing gender disparities in pain recognition.11 Another study Emphasize that conflict configuration exacerbates the challenges facing health workers related to gender biases in medical decision-making.12 Furthermore, the issue of structural violence against women in certain countries, which exemplifies the systemic obstacles that hinder effective pain management for this demographic.13 Collectively, these findings suggest the need for specific interventions to address specific gender pain management within health systems.
Regarding healthcare workers’ perceived barriers to pain management varied by profession, physicians (Table 2) reporting higher mean scores for barriers related to medical staff (4.55 ± 1.89), patient and family (4.36 ± 1.86), and health system (2.99 ± 0.41) compared to nurses, who reported lower mean scores for these barriers (4.01 ± 1.63, 3.99 ± 1.09, and 2.93 ± 0.98, respectively). Nurses who usually received related training courses had the highest mean score compared to those who did not receive the training courses. These differences in barriers perceived in pain management among the health professions, between doctors and nurses, highlight critical information on the challenges encountered in clinical areas. A study indicated that nurses have declared substantial barriers to effective pain management, especially in intensive care environments, emphasizing inadequate training and organizational support.3 Conversely, doctors have often cited time constraints and structural problems as the main obstacles to the implementation of pain management strategies.14 In addition, non-pharmacological approaches have been underused due to perceived limitations of efficiency, reflecting a shared concern between the two groups concerning complete pain management.15 Understanding these differences is crucial to fighting pain management gaps in health care.
This study’s findings further suggested that gender differences in healthcare workers’ self-efficacy for pain management can significantly impact patient care. Notably, male healthcare workers reported higher self-efficacy levels in pain management, scoring a mean of 12.46, compared to female healthcare workers, who scored 12.03 (p-value ≤0.05). This finding aligns with previous research indicating that women may experience greater disability due to lower self-efficacy.16 Furthermore, gender differences in self-efficacy can affect social support, coping strategies, and medical care practices,17 highlighting the need for tailored approaches to address these disparities.18
The study also found a significant relationship between healthcare workers’ self-efficacy in pain management and their workplace (Table 2). Specifically, healthcare workers in critical care units reported higher self-efficacy levels in pain management, with a mean score of 15.06, compared to those in other units (p-value ≤0.05). The connection between healthcare professionals’ self-efficacy in pain management and their work environment has garnered increasing attention, particularly in intensive care units. Healthcare professionals in these high-stress environments often face unique challenges that can impact their confidence in pain management. Previous research has shown that educational interventions targeting palliative care can significantly improve intensive care nurses perceived self-efficacy in pain management.19 Additionally, studies have identified work environment as a significant barrier to effective pain management, highlighting the need to address knowledge and attitude gaps among nurses in intensive care units.20 Furthermore, In the validation of this study, a recent scale that measures self -efficacy for the management of delirium patients in intensive care indicates that self -efficacy is crucial for quality patients care.21 Collectively, these findings emphasize the importance of enhancing support systems in intensive care environments to foster improvement in self-efficacy and pain management strategies.
This study underscores the significant relationship between healthcare workers’ experience and their self-efficacy in pain management, highlighting its implications for clinical practice (Table 2). Notably, healthcare workers with seven or more years of experience reported higher levels of self-efficacy in pain management, with a mean score of 4.99, compared to less experienced workers (p-value ≤0.05). The experience of healthcare workers influences their self-efficacy in pain management, as supported by different studies. Research has shown that training in pain management enhances healthcare professionals’ knowledge, attitude, and self-efficacy, emphasizing the importance of education in clinical settings.22 Additionally, studies have demonstrated that targeted interventions, such as implementing pain management, can improve patient outcomes and healthcare professionals’ self-efficacy.23 Furthermore, innovative tele-education interventions in chronic pain management have shown to improve skills between basic doctors in underserved clinical areas.24 These results highlight the need for continuous education and support to strengthen self-efficacy between healthcare professionals, which eventually improves patient care.25 The study limitations are included; questionnaires could induce bias in their interactions, the current results are restricted to the specific units and subjects; they cannot generalize it.
Implication of the finding: The study’s results highlight significant perceived barriers to effective healthcare delivery among medical staff, patients, families, and the healthcare system. Here are the implications of these findings:
Barriers to Healthcare Delivery: The study identified total correlated barriers across medical staff, patients, families, and the healthcare system, with varying levels of severity. This suggests that addressing these barriers is crucial to improving healthcare outcomes.
Healthcare system barriers: The relatively low mean score (3.11 ± 0.36) for healthcare system barriers indicates that systemic issues, such as resource allocation, policies, and infrastructure, may hinder effective healthcare delivery.
Healthcare Workers’ Self-Efficacy: The overall mean score (12.99 ± 4.02) for healthcare workers’ self-efficacy indicates a moderate level of confidence in their abilities to provide effective care. Variation by working place and experience: The statistically significant difference in self-efficacy levels among healthcare workers based on their working place and years of experience suggests that these factors can influence confidence and competence.
Implications for Healthcare Practice and Policy: Addressing perceived barriers: Healthcare organizations and policymakers should prioritize addressing the identified barriers to improve healthcare delivery and outcomes. Enhancing healthcare worker self-efficacy: Investing in training programs, mentorship, and supportive work environments can help boost healthcare workers’ self-efficacy and confidence. Tailoring interventions to the working place and experience: Healthcare organizations should consider the specific needs and challenges of healthcare workers based on their working place and years of experience when designing interventions to enhance self-efficacy and address perceived barriers. Promoting a patient-centered approach: Encouraging patient-centered care and involving patients and families in decision-making processes can help alleviate perceived barriers and improve healthcare outcomes. By addressing these implications, healthcare organizations and policymakers can work towards creating a more effective, efficient, and patient-centered healthcare system.
Conclusions
This study assessed the healthcare workers perceived pain management-correlated barriers in the teaching hospitals. Healthcare workers perceived correlated barriers as significant obstacles to successful pain management in the prementioned settings. Healthcare workers’ self-efficacy was stated highly among the participants at the critical care unit. Critically related training courses on pain assessment and management utilizing various tools are necessary for successful outcomes. Moreover, successful pain management requires incorporating individuals’ cultural origins into assessments. Highlight the significance of incorporating this issue into college curricula and hospital service training programs. Closely, healthcare practitioners should identify pain management limitations in their clinical settings as early as possible and devise solutions to achieve early optimal pain management such as differences in pain expression, communication barriers and religion concept of pain.
Data collection from different settings for generalization of the findings. Future research directions for improving pain management include Investigating cultural sensitivity training’s impact on pain management. Developing pain assessment tools for diverse populations. Examining the relationship between healthcare workers’ self-efficacy and pain management. Conducting comparative studies across different healthcare settings. Investigating interdisciplinary collaboration’s impact on pain management. Developing and evaluating pain management training programs. Pursuing these research directions can help address pain management challenges, improve patient care and develop effective strategies for better outcomes.
Institutional Review Board Statement
The faculty of Nursing, Suez Canal University Research Ethics Committee approved the study (June 2022; code No. 19). The participants were told about the research’s goal, and their responses were kept anonymous.
Data Sharing Statement
The datasets used and/or reviewed during the current investigation are available from the corresponding author upon reasonable request.
Acknowledgments
The researchers would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-2025). We would also like to thank the participants for their cooperation and support during the data collection process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shrestha S, Sapkota S, Teoh SL. et al. Comprehensive assessment of pain characteristics, quality of life, and pain management in cancer patients: a multi-center cross-sectional study. Qual Life Res. 2024;33(10):2755–2771. doi:10.1007/s11136-024-03725-w
2. World Health Organization. (2021). Assessing the development of palliative care worldwide: a set of actionable indicators.
3. Rababa M, Al-Sabbah S, Hayajneh AA. Nurses’ perceived barriers to and facilitators of pain assessment and management in critical care patients: a systematic review. J Pain Res. 2021;Volume 14:3475–3491. doi:10.2147/JPR.S332423
4. Li LW, Yi TH, Khaing NEE. Chronic pain healthcare workers’ challenges in pain management and receptiveness towards VR as an adjunct management tool: a qualitative study. BMC Digital Health. 2024;2(1):26. doi:10.1186/s44247-024-00073-0
5. Beckham J. Factors impacting multidisciplinary team communication and patient-centered communication along the cancer care continuum. 2022.
6. Warner LM, Schwarzer R. Self-efficacy and health. In: Handbook of Concepts in Health, Health Behavior and Environmental Health. Singapore: Springer Nature Singapore.; 2024:1–26.
7. Matthews RD. Examining the factors influencing self-efficacy of healthcare professionals towards end-of-life care in acute care settings Doctoral dissertation, Queensland University of Technology.
8. Youngcharoen P, Piyakhachornrot C. Online learning to improve nurses’ knowledge, attitudes, and self-efficacy about managing postoperative pain in older adults. Pain Manage Nurs. 2024;25(3):249–257. doi:10.1016/j.pmn.2024.02.007
9. Wang H, Jia J, Fan Y, et al. Impact of inpatient self-efficacy and trust in physicians on inpatient satisfaction with medical services: the mediating role of patient participation in medical decision-making. Front Psychol. 2024;15:1364319. doi:10.3389/fpsyg.2024.1364319
10. Ghahramanian A, Mirmaroofi N, Asghari-Jafarabadi M, et al. The effect of empowerment program on the pain control and self-efficacy in patients under total knee arthroplasty in Iran.
11. Voon P, Wang L, Nosova E, et al. Pain and barriers to accessing health services among people who use drugs. Pain Manage Nurs. 2021;22(2):133–140. doi:10.1016/j.pmn.2020.11.008
12. Habib RR, Halwani DA, Mikati D, Hneiny L. Sex and gender in research on healthcare workers in conflict settings: a scoping review. Int J Environ Res Public Health. 2020;17(12):4331. doi:10.3390/ijerph17124331
13. Nelson EU. Structural violence and barriers to pain management during an opioid crisis: accounts of women who use drugs in Nigeria. Health Sociol Rev. 2022;31(3):232–246. doi:10.1080/14461242.2021.1950024
14. Ng W, Slater H, Starcevich C, Wright A, Mitchell T, Beales D. Barriers and enablers influencing healthcare professionals’ adoption of a biopsychosocial approach to musculoskeletal pain: a systematic review and qualitative evidence synthesis. Pain. 2021;162(8):2154–2185. doi:10.1097/j.pain.0000000000002217
15. Zeleke S, Kassaw A, Eshetie Y. Non-pharmacological pain management practice and barriers among nurses working in Debre Tabor comprehensive specialized hospital, Ethiopia. PLoS One. 2021;16(6):e0253086. doi:10.1371/journal.pone.0253086
16. Kondo Y, Higuchi D, Miki T, Watanabe Y, Takebayashi T. Influence of pain self‐efficacy and gender on disability in postoperative cervical myelopathy. Pain Manage Nurs. 2023;24(3):335–341. doi:10.1016/j.pmn.2022.12.004
17. Samulowitz A, Hensing G, Haukenes I, Bergman S, Grimby-Ekman A. General self-efficacy and social support in men and women with pain–irregular sex patterns of cross-sectional and longitudinal associations in a general population sample. BMC Musculoskelel Disord. 2022;23(1):1026. doi:10.1186/s12891-022-05992-5
18. Kolmes SK, Boerstler KR. Is there a gender self-advocacy gap? An empiric investigation into the gender pain gap. J Bioethical Inquiry. 2020;17(3):383–393. doi:10.1007/s11673-020-09993-8
19. DeFusco C, Lewis A, Cohn T. Improving critical care nurses perceived self-efficacy in providing palliative care: a quasi-experimental study. Am J Hospice Palliative Med®. 2023;40(2):117–121. doi:10.1177/10499091221094313
20. Sweity EM, Salahat AM, Sada AA, Aswad A, Zabin LM, Zyoud SE. Knowledge, attitude, practice and perceived barriers of nurses working in intensive care unit on pain management of critically ill patients: a cross-sectional study. BMC Nurs. 2022;21(1):202. doi:10.1186/s12912-022-00990-3
21. Chang YL, Hsieh MJ, Chang YC, Yeh SL, Chen SW, Tsai YF. Self-efficacy of caring for patients in the intensive care unit with delirium: development and validation of a scale for intensive care unit nurses. Aust Crit Care. 2023;36(4):449–454. doi:10.1016/j.aucc.2022.08.006
22. Parvizy S, Tarvirdinasab S, Raznahan R, Aliakbari M. The effect of pain management training in workshop on the knowledge, attitude and self-efficacy of pediatric nurses. J Family Med Primary Care. 2020;9(6):2880–2884. doi:10.4103/jfmpc.jfmpc_92_20
23. Brunkert T, Simon M, Zúñiga F. Use of pain management champions to enhance guideline implementation by care workers in nursing homes. Worldview Evidence-Based Nurs. 2021;18(2):138–146. doi:10.1111/wvn.12499
24. Furlan AD, Zhao J, Voth J, et al. Evaluation of an innovative tele-education intervention in chronic pain management for primary care clinicians practicing in underserved areas. J Telemed Telecare. 2019;25(8):484–492. doi:10.1177/1357633X18782090
25. Kizza IB, Maritz J. Family caregivers for adult cancer patients: knowledge and self-efficacy for pain management in a resource-limited setting. Support Care Cancer. 2019;27(6):2265–2274. doi:10.1007/s00520-018-4504-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient-Centered Communication Among Pharmacy Professionals Working in Hospitals and Drug Retail Outlets in Asmara, Eritrea: Knowledge, Attitude, Self-Efficacy and Barriers
Michael E, Nurahmed A, Mihreteab H, Nurhussien M, Adem M, Goitom A, Mihreteab Siele S, Tesfamariam EH, Abdu N
Integrated Pharmacy Research and Practice 2022, 11:153-164
Published Date: 6 October 2022
A Cross-Sectional Study on Current Perioperative Pain Management and Nurses’ Pain Management Self-Efficacy in China’s Interventional Department
Zhang H, Meng Y, Xu X, Li Y, Li X, Hu H, Zheng L, Hu X
Journal of Pain Research 2025, 18:1291-1303
Published Date: 14 March 2025