")
Back to Journals » Journal of Pain Research » Volume 18
A Randomized, Sham-Controlled Trial on the Efficacy and Safety of Electroacupuncture for Lumbar Disc Herniation with Radiculopathy: Rationale and Study Protocol
Authors Yang Y, Liu L, Yuan L, Liu X, Ding H, Zhou X, Cao Q
Received 17 December 2024
Accepted for publication 30 April 2025
Published 5 May 2025 Volume 2025:18 Pages 2307—2319
DOI https://doi.org/10.2147/JPR.S512711
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Yuwei Yang,1,* Liting Liu,1,* Lixia Yuan,1 Xiaoya Liu,1 Haoying Ding,2 Xu Zhou,3 Qianan Cao4
1Graduate School, Jiangxi University of Chinese Medicine, Nanchang, Jiangxi, 330004, People’s Republic of China; 2The First Department of Acupuncture and Moxibustion, The Affiliated Hospital of Jiangxi University of Chinese Medicine, Nanchang, Jiangxi, 330004, People’s Republic of China; 3Evidence-Based Medicine Research Center, Jiangxi University of Chinese Medicine, Nanchang, Jiangxi, 330004, People’s Republic of China; 4Acupuncture and Moxibustion Rehabilitation Center, The Affiliated Hospital of Jiangxi University of Chinese Medicine, Nanchang, Jiangxi, 330004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qianan Cao, Acupuncture and Moxibustion Rehabilitation Center, The Affiliated Hospital of Jiangxi University of Chinese Medicine, ba Yi Avenue No. 445, Nanchang, Jiangxi, 330004, People’s Republic of China, Tel +8618720928675, Fax +86079186210551, Email [email protected] Xu Zhou, Evidence-based Medicine Research Center, Jiangxi University of Chinese Medicine, Mei Ling Avenue No. 1688, Nanchang, Jiangxi, 330004, People’s Republic of China, Tel +8618870050733, Fax +86079187118012, Email [email protected]
Introduction: Electroacupuncture, validated in preclinical studies, is a promising alternative approach for lumbar disc herniation with radiculopathy (LDHR). This trial aims to evaluate the efficacy and safety of electroacupuncture in patients with LDHR.
Methods: This randomized, single-blind, sham-controlled trial will enroll 170 participants diagnosed with LDHR and who present Numerical Rating Scale (NRS) scores ≥ 4 for both lower back and leg pain. Participants will be allocated at a 1:1 ratio to receive either electroacupuncture or sham electroacupuncture (superficial needling at nonacupoint sites). The sample size was determined based on pilot study data and power calculations. Treatments will be administered three times weekly over 8 weeks (24 sessions total), with blinding maintained throughout. An 18-week noninterventional follow-up will be extended to address the knowledge gap regarding the durability of neuromodulatory effects of electroacupuncture. The following outcomes will be evaluated: 1) primary outcome: the proportion of responders achieving ≥ a 2-point NRS reduction in both lower back and leg pain from baseline at weeks 8 and 24; 2) secondary outcomes: changes from baseline at weeks 4, 8, 16, and 24 in the intensity of low back pain and leg pain, level of disability, severity of depression and anxiety, sleep quality, as well as the incidence of lumbar spine surgery and the proportion of use of analgesics at weeks 8 and 24; and 3) safety outcome: the incidence of adverse events. The efficacy outcomes will be analyzed based on the full analysis set with the modified intention-to-treat principle. Treatment effects will be estimated using a generalized linear mixed-effects model for repeated measures. Blinding validity will be assessed via James’s and Bang’s indices.
Conclusion: This rigorously designed randomized controlled trial will generate confirmatory evidence to support the efficacy and safety of electroacupuncture in the treatment of LDHR.
Trial Registration No.: NCT06611332 (https://clinicaltrials.gov/study/NCT06611332).
Keywords: electroacupuncture, lumbar disc herniation, radiculopathy, sham control, randomized controlled trial
Introduction
Lumbar disc herniation with radiculopathy (LDHR) is a major cause of low back pain, radicular pain in the leg, and disability, with a lifetime risk ranging from 1% to 3%.1 Among patients with low back pain, the incidence of LDHR varies from 12% to 40%.2 The pathophysiology of LDHR is closely associated with protruded nucleus pulposus tissue: as a result of lumbar disc herniation, the annulus fibrosus ruptures, and the intervertebral disc material exceeds the basal edge of the vertebral body; the protruded nucleus pulposus tissue compresses the nerve roots distributed in the intervertebral foramen, triggering an immune response that generates inflammatory substances.3 Under the dual influence of mechanical compression and inflammatory factors, nerve roots develop edema, increased vascular permeability, inflammatory reactions, and abnormal discharges, eventually resulting in lower back pain, radiating pain in the lower extremities, and nerve root symptoms (eg, pain, weakness, and numbness in the muscle layer or cortex).4 With the acceleration of the social rhythm and the increase in desk work time, the incidence of LDHR is rising annually and has emerged as the third leading cause of disability among individuals over 45 years of age.5
Currently, the treatment approaches for LDHR include surgery and conservative therapy. However, both approaches have limitations. Surgery is only applicable for a small proportion of patients with severe symptoms. Even after surgery, patients may still experience complications such as reprotrusion, numbness, and pain, and surgery-related expenses impose a considerable economic burden.6,7 Minimally invasive surgeries, represented by epidural steroid injections, have lower medical costs than open surgeries, but their efficacy is limited, and they may lead to neurological sequelae.8,9 Oral medications, including analgesics and nonsteroidal anti-inflammatory drugs, can relieve pain to a certain extent, but their efficacy is limited, with significant side effects (eg, addiction, constipation, and sedation caused by opioids; gastrointestinal adverse reactions; and cardiovascular risks caused by nonsteroidal anti-inflammatory drugs).10,11 Physical therapies, including transcutaneous neuromodulation, manual therapy, and mobilization, have demonstrated pain-relieving effects. However, transcutaneous neuromodulation and manual therapy primarily alleviate pain by modulating superficial nerves, with limited efficacy in stimulating deep acupoints or muscles.12–16 While mobilization techniques are widely used, their therapeutic outcomes remain controversial. For example, a clinical trial revealed no statistically significant difference in pain relief between real mobilization and sham mobilization in patients with chronic low back pain.17 Therefore, it is necessary to discover alternative therapeutic modalities that are cost-efficient and safe.
Acupuncture, a traditional acupoint therapy, is widely used for its analgesic efficacy. After inserting filiform needles into specific acupoints, it stimulates the body to release endogenous opioid substances and increase the expression of opioid receptors, thereby producing an analgesic effect.18 Systematic reviews have demonstrated that acupuncture is significantly superior to sham acupuncture in alleviating pain in chronic diseases.19 Animal studies have suggested that opioid substances are involved in the mediation of acupuncture analgesia and that the opioid receptor antagonist naloxone can block or reverse the effect of acupuncture analgesia.20,21 Electroacupuncture is developed based on manual acupuncture, which applies electrical stimulation of different frequencies and intensities to augment the intensity of stimulation at acupoints and enhance the effect. Animal experiments have indicated that electroacupuncture at the Huantiao (GB30) and Yanglingquan (GB34) acupoints reduces the release of 5-hydroxytryptamine and calcitonin gene-related peptides in areas of rats with sciatica and increases the content of neuropeptide Y. These substances are involved in the peripheral sensitization of pain and are associated with analgesia, improvement of microcirculation, and neuroinflammatory mechanisms.22 Electroacupuncture may achieve analgesic effects and neural repair through dual mechanisms involving peripheral and central pathways. Peripherally, electroacupuncture has been demonstrated to reduce the expression of proinflammatory mediators (eg, tumor necrosis factor α, interleukin-1β) while increasing the production of anti-inflammatory factors. It also decreases inflammatory mediator levels in the dorsal root ganglion and triggers the release of endogenous opioids and adenosine, thereby alleviating pain.23–25 Centrally, electroacupuncture mitigates central inflammatory responses, modulates neuronal excitability in the spinal dorsal horn, and regulates opioid peptides and their receptors to suppress pain transmission.26–28 A study on varying intensities of electroacupuncture stimulation at the “Zusanli” (ST36) acupoint in rats demonstrated that electroacupuncture reduces the Aδ-fiber component, C-fiber component, and after-discharge activity of wide dynamic range neurons in the spinal dorsal horn. These findings confirm the ability of electroacupuncture to inhibit short-term sensitization of wide dynamic range neurons, effectively blocking the amplification of nociceptive signals at the spinal level.29 Therapeutic efficacy varies with electroacupuncture parameters. Current evidence indicates that stimulation parameters of 2 mA current intensity and 4 hz frequency demonstrate significantly superior efficacy compared with other parameters.30–32
Owing to its potential analgesic effect, electroacupuncture has been clinically employed as a complementary and alternative therapy for treating pain-related disorders. For example, clinical trials have shown that electroacupuncture can alleviate chronic musculoskeletal pain in cancer survivors, reduce pain intensity in patients with knee osteoarthritis, and delay the need for analgesic drugs after cesarean section.33–35 However, current evidence from three randomized controlled trials (RCTs) on electroacupuncture for chronic low back pain remains inconsistent. One RCT demonstrated that electroacupuncture significantly enhanced analgesic effects compared with sham electroacupuncture,36 whereas two other RCTs failed to show such therapeutic benefits.37,38 This discrepancy may be attributed to variations in intervention types (eg, body acupuncture versus auricular acupuncture) and acupoint selection across trials, as well as methodological limitations, including lack of long-term follow-up, small sample sizes, inadequate sham acupuncture designs, and unreported handling of missing data. More importantly, these studies focused on chronic low back pain rather than specifically targeting LDHR. Therefore, we propose to conduct an RCT to assess the efficacy and safety of electroacupuncture in the treatment of pain and dysfunction in patients with lumbar disc herniation. We will focus on patients complicated with radiculopathy and establish a sham electroacupuncture control to minimize the placebo effect.
Methods and Design
Study Design
This is a single-center, randomized, single-blind, sham-controlled trial. We will recruit patients with LDHR at the Affiliated Hospital of Jiangxi University of Chinese Medicine. The trial protocol has been approved by the Ethics Committee of the Affiliated Hospital of Jiangxi University of Chinese Medicine (approval number: JZFYLL202400822103) and has been prospectively registered at clinicaltrials.gov (registration number: NCT06611332). Prior to participating in the trial, all participants will sign the informed consent form. The implementation of the trial will strictly follow the Declaration of Helsinki.39 The reporting of this trial protocol adhered to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) statement (Supplementary Table S1).40,41
Participants
Eligible patients should be diagnosed with LDHR in accordance with the criteria of the North American Spine Society’s guidelines,3 namely, local displacement of the lumbar intervertebral disc material beyond the normal margin of the intervertebral disc space confirmed by computed tomography or magnetic resonance imaging, resulting in pain, weakness or numbness distributed in the muscular or cortical layers. In addition, patients should be aged between 18 and 70 years and have a Numerical Rating Scale (NRS) score of lower back and leg pain ≥4 points that persists for at least three months. Recruitment is scheduled to start in October 2024 and is anticipated to end in October 2025.
The following patients will be excluded: those who have undergone previous spinal surgery; those who have received any physical therapy for LDHR in the past three months, such as epidural local block and acupoint stimulation treatments; those with concurrent diseases that can cause low back or leg pain, such as spinal fractures, epidural abscesses, spondylolisthesis, lumbar spinal stenosis, synovial cysts, and symptomatic foraminal stenosis caused by severe degenerative diseases; those with severe nerve injuries such as lower extremity muscle atrophy, paralysis, and cauda equina syndrome; those with previous severe mental illness, organ failure or malignant tumors; those who plan to undergo spinal surgery or other major surgeries within the next three months; those who are pregnant or lactating; and those who are expected to have poor compliance or are unwilling to sign the informed consent form.
During the trial, if a participant underwent lumbar spine surgery or experienced serious adverse reactions that made it impossible for them to continue participating in the trial, they will be determined to be unable to continue.
Randomization and Allocation Concealment
Eligible participants will be randomly assigned at a 1:1 ratio to the electroacupuncture group or the sham electroacupuncture group. An independent researcher will generate and save the random sequence via the “blockrand” package in R version 4.2.2. Block randomization will be applied, with dynamically varied block sizes automatically generated as a random combination of 4 or 6 by the “blockrand” algorithm. The random sequence will be sealed within sequentially numbered scratch cards. Neither the acupuncturists nor the patients could know the randomized grouping before scratching the coating, thereby achieving allocation concealment. During the trial, the acupuncturists will not be blinded, whereas the patients, the researchers collecting the outcome data, and the researchers analyzing the data will be blinded. For this purpose, we will implement a sham electroacupuncture intervention for patients in the control group (Figure 1).
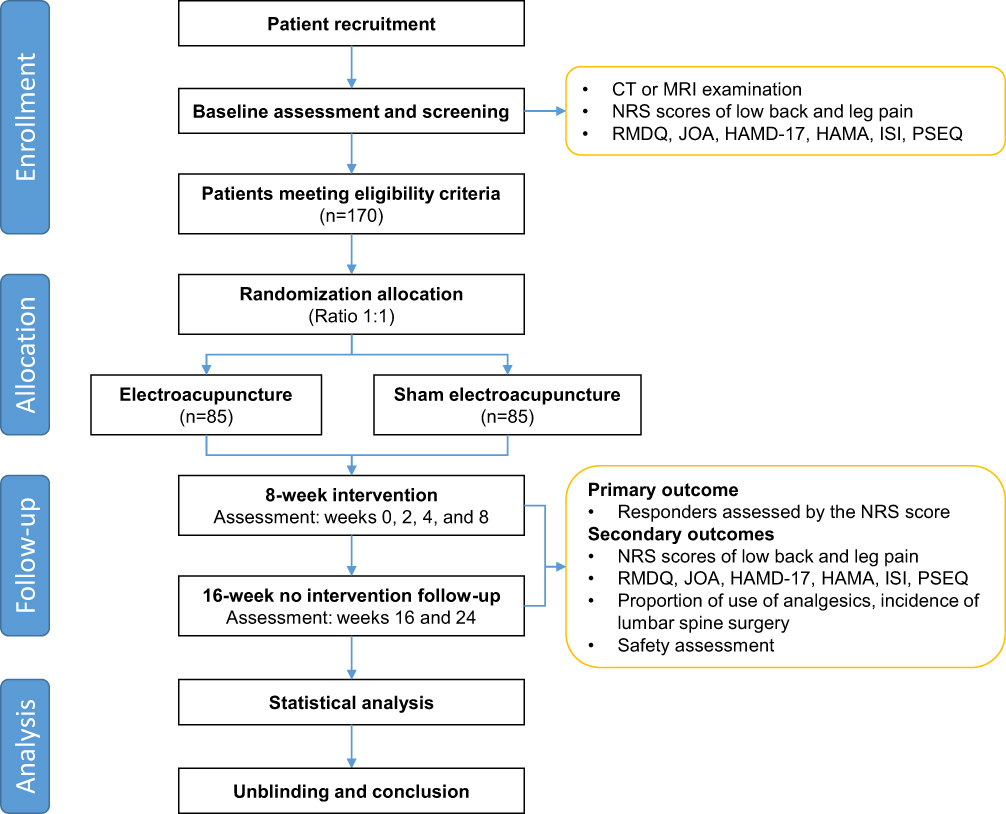 |
Figure 1 Flowchart of the trial procedure. This is a randomized, single-blind, sham-controlled trial. Block randomization and patient single-blinding will be implemented. Patients in the electroacupuncture group will receive treatment at the bilateral BL23 and BL25 acupoints using a continuous wave at 4.0 hz frequency and 2 mA current intensity. The sham electroacupuncture group will undergo shallow insertion (2–3 mm depth) at nonacupoint locations with a weak current stimulation of 0.1–0.2 mA. The total follow-up period spans 24 weeks, including an 8-week intervention phase and a 16-week intervention-free follow-up phase. Abbreviations: NRS, Numerical Rating Scale; RMDQ, Roland‒Morris Disability Questionnaire; JOA, Japanese Orthopedic Association Scale; HAMD-17, Hamilton Depression Rating Scale; HAMA, Hamilton Anxiety Rating Scale; ISI, Insomnia Severity Index; PSEQ, Pain self-efficacy Questionnaire. |
Interventions
The intervention will be administered by two qualified acupuncturists who possess at least five years of experience in electroacupuncture. The acupuncturists will receive training in standardized interventions before the trial. During the trial, disposable acupuncture needles manufactured by Suzhou Medical Supplies Factory Co., Ltd. and an SDZ-II electroacupuncture apparatus will be used.
In the electroacupuncture group, we will select the acupoints that frequently show a force-sensitive state in patients with LDHR for acupuncture. The latest acupuncture research has demonstrated that acupoints in a force-sensitive state are more sensitive to the stimulation of mechanical force and are thus more likely to achieve the “deqi” sensation, which is expected to result in better therapeutic effects. For LDHR, the acupoints with a high frequency of force-sensitive states include Shenshu (BL23), Dachangshu (BL25), Huantiao (GB30), Yinlian (LR11), Ququan (LR8), Mingmen (GV4), Yaoyangguan (GV3), Weizhong (BL40), Zhibian (BL54), Chengshan (BL57), and Kunlun (BL60). The former eight will be selected as the main acupoints, and the latter three will be the accessory acupoints. Patients will be positioned in a prone posture, and following skin disinfection, disposable Hwato filiform needles will be inserted into the designated acupoints. The insertion depth ranges from 30 to 50 mm, with the needle gauge and angle adjusted according to the anatomical location and individual somatic variations. The detailed acupoint locations and needling parameters for the electroacupuncture group are provided in Supplementary Figure S1 and Supplementary Table S2. The acupuncturist will perform small and equal lifting-thrusting-rotating manipulations at all acupoints once every 10 minutes for 30 seconds to induce “de qi” sensations, such as comfortable pain, numbness, swelling, and heaviness. The needles will be retained for 30 minutes. On this basis, electroacupuncture therapy will be implemented: the positive and negative electrodes of the electroacupuncture apparatus will be connected to the needle handles of the bilateral BL23 and bilateral BL25, respectively, with a continuous wave, a frequency of 4.0 hz, and a current intensity of 2 mA. The current stimulation will also last for 30 minutes per session.
In the control group, patients will receive sham electroacupuncture at sham acupoints. After the correct acupoints are excluded, those positioned 2 cm horizontally lateral to these correct acupoints will be designated sham acupoints for the control group. The detailed acupoint locations and needling parameters for the control group are presented in Supplementary Figure S2 and Supplementary Table S3. To make stimulation comparable between the two groups, the number of filiform needles used in the control group will be identical to that used in the electroacupuncture group. The acupuncturist will insert the needles into the skin at a shallow depth of 2 to 3 mm perpendicularly to the skin at the sham acupoints and then disturb the needles only slightly without lifting-thrusting-rotating manipulation. Simultaneously, the needle handles at the sham acupoints of bilateral BL23 and BL25 will be connected to the electroacupuncture apparatus, with a weak current of 0.1 to 0.2 mA. The needle and current stimulation will also be administered for 30 minutes. Although this sham protocol may produce minimal physiological stimulation, its therapeutic impact on outcome evaluation is considered negligible compared to the placebo effect addressed by the sham design.42,43 During the trial, the treatment time and place of each participant will be staggered to prevent any communication between patients in different groups.
Participants in both groups will receive the interventions starting from the day of randomization, with a treatment frequency of one session every other day for 8 consecutive weeks. All participants will receive two extended visits without interventions at weeks 8 and 16 after the end of the interventions. The total length of follow-up will be 24 weeks.
During the trial, participants will be required not to take oral analgesics. However, if the pain is severe and intolerable, patients are allowed to take emergency oral analgesics to alleviate the pain. All the subjects will be prohibited from receiving other acupoint stimulation therapies. The treatment for other comorbidities is not restricted; for example, those with hypertension can take antihypertensive drugs. Any violations of these requirements will be recorded truthfully but will not affect the subsequent treatment and follow-up processes of the trial.
Outcomes
Primary Outcome
The primary outcome is the proportion of responders at weeks 8 and 24. A responder is defined as having at least a 2-point reduction in the NRS score for both low back pain and leg pain compared with baseline, which is the minimal clinically important difference (MCID) of this scale.44,45 The response assessment at week 8 will be conducted immediately after the completion of treatment.
Secondary Outcomes
We will evaluate changes from baseline in the following secondary efficacy outcomes at weeks 2, 4, 8, 16, and 24:
1) Intensity of low back pain as measured by the NRS score.
2) Intensity of leg pain as measured by the NRS score.
3) Level of disability as measured by the Roland‒Morris Disability Questionnaire;46 this scale consists of 24 items, with a score ranging from 0 to 24 points; a higher score indicates more severe functional disability, and the MCID is 5 points.47
4) Performance status as measured by the Japanese Orthopedic Association (JOA) Scale;48 this scale assesses three domains of performance status: symptoms, walking ability, and activities of daily living, with scores ranging from 0 to 29 points; a higher score indicates better lumbar spine functional status, and the MCID has not been established.
5) The severity of depression as measured by the Hamilton Depression Rating Scale (HAMD-17);49 this scale consists of 17 items, with a total score of 0 to 54 points; a higher score indicates more severe depression, and the MICD score is 2 points.50
6) Severity of anxiety as measured by the Hamilton Anxiety Rating Scale (HAMA);51 this scale consists of 14 items, with a total score of 0 to 56 points; a higher score indicates more severe anxiety, and the MCID is 3.91 points.52
7) Sleep quality as measured by the Insomnia Severity Index (ISI);53 this scale has 7 items, with a total score of 0 to 28 points; a higher score indicates more severe insomnia, and the MCID is 2.4 points.54
8) Pain self-efficacy as measured by the Pain Self-Efficacy Questionnaire (PSEQ);55 this scale has 10 items, with a score range of 0 to 60; a higher score indicates stronger self-efficacy, and the MCID is 6.48 points.56
9) The proportion of emergency use of analgesics (at weeks 8 and 24).
10) The incidence of any lumbar spine surgery (at weeks 8 and 24).
Safety Outcomes
The safety outcomes include the incidences of any adverse events (AEs), treatment-related AEs, and serious adverse events (SAEs). AEs include those reported by patients and determined by clinicians, without association with the natural progression of LDHR. “Treatment-related” refers to any AE determined by clinicians to be caused by electroacupuncture or sham electroacupuncture treatment. The anticipated treatment-related AEs include pain, bleeding or subcutaneous hematoma at the acupuncture site, broken needles, infections, and syncope. SAEs are defined as those that lead to hospitalization or prolongation of hospital stay, disability, a threat to life, or death. In the event of an SAE, the intervention to the patient will be terminated, rescue measures will be taken, and an immediate report will be made to the ethics committee.
Blinding Evaluation
At the end of the 8-week intervention, we will assess the success rate of blinding using the James Blinding Index (JBI) and Bang Blinding Index (BBI).57,58 The JBI evaluates overall blinding, with an index range of 0 (indicating completely successful guesses) to 1 (indicating completely failed guesses). A higher value represents more successful blinding. A JBI of 0.5 indicates that half of the guesses are correct and that half are incorrect, signifying ideal blinding.59 The BBI evaluates the blinding of each group, with a range of −1 to 1, where a positive value represents failed blinding (ie, more subjects guessed the grouping correctly), a negative value represents successful blinding (ie, more subjects guessed the grouping incorrectly), and 0 implies an ideal blinding outcome.60 Blinding is considered successful when the upper limit of the 95% CI for JBI is >0.5 and the BBI index is <0.3.58,61
Visit Schedule
During the intervention period, patients will receive four visits at baseline and at the end of weeks 2, 4, and 8. During the extended follow-up period, they will receive two visits at the end of weeks 16 and 24. The time window for the first three visits is ±3 days, whereas for the last two visits, it is ±5 days. If a patient fails to receive a visit within the stipulated time window, data for this visit will no longer be collected and will be regarded as missing. At the baseline follow-up, we will collect data on demographic characteristics (age, sex, ethnicity, marital status, education level, occupation, and body mass index) and baseline disease status (location of lumbar disc herniation, duration of LDHR, and baseline scores of each outcome). At each follow-up visit, we will assess the primary and secondary outcomes and collect data on the use of analgesics, new lumbar surgeries, and AEs. The detailed visit schedule is shown in Figure 2.
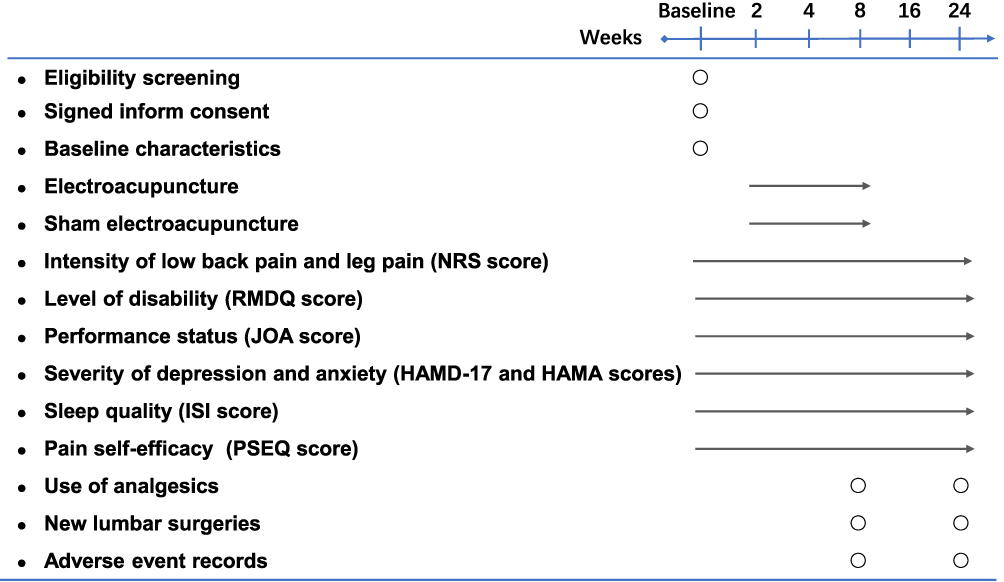 |
Figure 2 Schedule of study visits. Abbreviations: NRS, Numerical Rating Scale; RMDQ, Roland‒Morris Disability Questionnaire; JOA, Japanese Orthopedic Association Scale; HAMD-17, Hamilton Depression Rating Scale; HAMA, Hamilton Anxiety Rating Scale; ISI, Insomnia Severity Index; PSEQ, Pain self-efficacy Questionnaire. |
Data Collection and Management
Before the initiation of the trial, researchers, including acupuncturists, outcome assessors, and data analysts, will undergo training adhering to the standard operating procedure. Data collection will be predicated on a pretested case report form (CRF). A data and safety monitoring board composed of acupuncture experts, orthopedic experts, ethics experts, and statisticians will be established to monitor data quality and safety. The baseline and follow-up data of each participant will be evaluated by the same researcher to guarantee data consistency. Paper-based CRF files will be stored in a locked filing cabinet and managed by an independent researcher. Once the data collection is accomplished, two independent researchers will independently and repeatedly input the data into the electronic data collection form created in Microsoft Access (Microsoft Corporation, USA). A third researcher will subsequently verify the results of the two data entries and corrected inconsistencies by referring to the original CRF. The electronic dataset will be anonymized and doubly backed up in a dedicated computer.
Recruitment and Compliance Assurance
We will recruit participants via official websites, posters, and recommendations from clinicians. The participants will be informed of the entire trial protocol, especially the intervention and follow-up they will undergo during the trial. Only after providing their informed consent can participants engage in this trial. To facilitate recruitment and patient compliance, patients in the electroacupuncture group will receive free 8-week electroacupuncture treatment, whereas those in the control group will receive the same free treatment as the trial group upon the completion of the trial. In addition, patients will undergo a comprehensive assessment of their disease condition at each visit, which also contributes to enhancing the enthusiasm of patients to participate in the study.
Sample Size Calculation
The sample size calculation was informed by preliminary data from our nonrandomized pilot trial, which reported response rates of 76.7% (electroacupuncture) and 50.0% (control) (the results have not yet been published). To ensure robustness, we conservatively hypothesize that the proportion of responders is 75% in the electroacupuncture group and 55% in the control group. With the allowed type I error probability set at 5% and the type II error probability at 20%, the sample size calculation formula of superiority design yielded a sample size of at least 68 patients in each group. Considering a 20% attrition rate, we increased the sample size in each group to 85 cases, with a total sample size of 170 cases.
Statistical Analysis
The statistical analysis of the efficacy outcomes will be based on the full analysis set established by the modified intention-to-treat principle, which includes all patients who received one randomization intervention and had at least one outcome measurement of low back and leg pain. Regarding the primary outcome, only when a statistically significant between-group difference is obtained at week 8 will the results at week 24 be evaluated as the primary outcome. Sensitivity analysis for efficacy outcomes will be conducted based on the per-protocol set, which is the population without major protocol violations, including completing at least 80% of the intervention sessions, being visited within the study visit window, having the last visit, and not receiving emergency analgesics, other acupoint stimulation therapies, or lumbar surgeries during the trial. Missing values will be imputed via multiple imputation based on the regression model. Safety outcomes will be based on the safety set, where patients who receive one dose of intervention will be included in the corresponding group.
The baseline characteristics and outcome data of the patients will be described using means and standard deviations (for continuous variables with a normal distribution), medians and interquartile ranges (for continuous variables with a skewed distribution), or frequencies and percentages (for categorical or ordinal variables). The generalized linear mixed-effects model for repeated measures will be used to estimate the treatment effects, where the link function for binary outcomes is logit and that for continuous outcomes is identity. The main effect will be the treatment group; the fixed-effect covariates will include age, disease duration, baseline NRS score of low back pain, history of analgesics, time, and treatment × time interaction; and the random-effect covariates will be patient ID and acupuncturist. The effect sizes of binary and continuous outcomes will be measured by odds ratios and mean differences along with their 95% confidence intervals, respectively. All the statistical analyses will be performed in SAS 9.4 (SAS Institute Inc). As a hierarchical test is conducted for the primary outcome, no multiplicity correction is implemented, with the significance threshold for all the statistical analyses being α = 0.05. For efficacy outcomes, we will conduct subgroup analyses to explore heterogeneity in electroacupuncture (EA) effects across populations: sex (male vs female), age (<60 years vs ≥60 years), and pain duration (<6 months vs ≥6 months). Statistical differences between subgroups will be tested by including subgroup × treatment interactions in the mixed-effects models.
Discussion
This research is designed as a single-blind, randomized, sham-controlled trial. Electroacupuncture has well-established basic research evidence supporting its mechanisms. It achieves analgesic effects through multiple pathways, including stimulating the endogenous opioid system to release β-endorphin, enkephalin, and dynorphin; modulating pro-inflammatory and anti-inflammatory cytokine levels via neuroimmune interactions; and increasing brain-derived neurotrophic factor levels to promote synaptic regeneration and cortical functional reorganization.62–64 The completion of this trial will provide detailed and precise evidence regarding the efficacy and safety of electroacupuncture in the treatment of LDHR in humans. The advantages of this trial are manifested in the following aspects.
One advantage of this trial lies in the selection of important outcomes for patients. Specifically, the proportion of responders defined by a reduction of at least 2 points in the NRS score is used as the primary outcome. The NRS scale has good validity and repeatability and is widely used in studies of chronic low back pain because of its robust psychometric information.65 The NRS has been demonstrated to have fewer missing or incomplete data than the Visual Analogue Scale, potentially because the NRS is more straightforward in understanding and expressing the intensity of chronic pain, thereby reducing the response time.44 The receiver operating characteristic curve indicates that a cutoff of 2 points has the best ability to differentiate responders from nonresponders.66 Clinical trials have also confirmed that for patients with low back pain, a reduction of at least 2 points in the total NRS score can be used as the threshold for predicting low back pain relief.67 Therefore, the selection of this threshold to calculate the proportion of responders in our primary outcomes is conducive to accurately reflecting the treatment effect. In addition, LDHR may affect functional status, sleep, psychological condition, and quality of life. Therefore, we employed multiple scales (ie, the RMDQ, JOA, HAMD-17, HAMA, ISI, and PSEQ) to comprehensively evaluate the efficacy of electroacupuncture for various symptom dimensions of LDHR. Furthermore, some studies suggest that electroacupuncture may only have short-term efficacy that is not sustainable.37,38 Therefore, in addition to the 8-week intervention period, we will conduct a 16-week nonintervention follow-up (weeks 9 to 24) to observe the sustained effects after the end of the electroacupuncture intervention.
Another advantage is the reasonable control design and the implementation of blinding for participants. Selecting an appropriate sham control in acupuncture trials is crucial for ensuring the success of blinding.68 A placebo is, in principle, required to be ineffective; however, there is currently no flawless placebo control for acupuncture. Some previous studies have shown that all sham acupuncture methods are noninert and elicit a certain placebo effect (nonspecific effect),69 which may be related to the activation of the spinal pain inhibitory system and diffuse noxious inhibitory control.26,70 Although the analgesic effect of sham acupuncture may be weak, it diminishes the difference from that of real acupuncture.71 In acupuncture studies, insertion at acupoints has the greatest placebo effect, followed by insertion at nonacupoints, no insertion at nonacupoints, and no insertion at acupoints.71 Considering that Chinese people are generally acquainted with electroacupuncture, we chose the placebo design of superficial insertion at nonacupoints and nonmeridians with a weak current to give patients the sensation of insertion into the skin and electrocution, striving to achieve the minimum placebo effect while ensuring the success of blinding. To evaluate the blinding effect, we will assess the overall blinding and within-group blinding through the JBI and BBI at the end of week 8, and the results of the two indices can also be regarded as sensitivity analyses for each other.
If our trial validates that electroacupuncture is an effective and safe approach for treating LDHR, it could change clinical practice. First, electroacupuncture may emerge as an important option for patients with LDHR, thereby reducing reliance on invasive surgeries and pharmacological interventions while improving quality of life. Compared with exercise therapy, transcutaneous electrical nerve stimulation, and manual therapy, electroacupuncture can also be anticipated to demonstrate superior immediate analgesic effects and long-term adherence.12–15,17 Second, the results of this trial will also provide clinicians with evidence for decision-making through subgroup analyses. We predefined three subgroup analyses stratified by sex, age, and pain duration, with hypotheses about effect directions. With respect to sex, we anticipate that female patients will achieve better outcomes than male patients, since estrogen enhances μ-opioid receptor signaling, which may improve the analgesic response.18 With respect to age, we hypothesize that younger patients respond better than older patients, as younger individuals typically exhibit milder intervertebral disc degeneration, where nerve root edema is the primary pathology. The anti-inflammatory effects of electroacupuncture may alleviate nerve root compression in these patients, leading to better outcomes. In contrast, older patients have a reduced capacity for neural adaptive remodeling, leading to poorer recovery.72 For pain duration, we hypothesize that patients with symptoms lasting <6 months will benefit more from electroacupuncture, as early-stage inflammation is more responsive to the immunomodulatory effects of electroacupuncture.73 Thus, subgroup findings could guide personalized clinical interventions—such as more intensive electroacupuncture for short-duration cases, adjunctive neurorestorative therapies for elderly patients, and menstrual cycle-based (ie, estrogen fluctuation-guided) frequency adjustments—to optimize efficacy.
This RCT may also suffer from several limitations. First, although we have standardized the electroacupuncture protocol and will provide unified training for practitioners, variations in practitioners’ expertise are unavoidable. These differences may affect the accuracy of acupoint localization, the proficiency of needling techniques, the consistency of needle insertion depth, and patients’ perception of deqi sensation, potentially introducing bias. Second, the sustained therapeutic effects after electroacupuncture cessation hold significant clinical value for LDHR; however, our 16-week untreated extended follow-up period may be insufficient to capture all long-term outcomes. Financial constraints currently prevent longer-term monitoring. Third, although we designed sham procedures with superficial needling at nonacupoint sites for the control group, minimal therapeutic effects from shallow penetration may still occur, leading to bias. However, this bias is negative (conservative). Should electroacupuncture still demonstrate efficacy compared with the sham electroacupuncture group under these conditions, the results would be more robust. Fourth, this RCT did not explore dose‒response relationships in electroacupuncture for LDHR. Should this trial confirm the efficacy of electroacupuncture for LDHR, the next step could involve dose-response studies, such as testing different combinations of current intensity and frequency, to determine the optimal electroacupuncture protocol for LDHR. Finally, as this is a single-center study conducted in China, the generalizability of the findings may be limited. After obtaining our results, further validation through multicenter studies—particularly international multicenter trials—may be necessary.
Conclusion
This RCT will provide confirmatory evidence for the efficacy and safety of electroacupuncture in treating LDHR. Should the study results demonstrate significant therapeutic effects with favorable safety profiles, electroacupuncture could serve as a minimally invasive alternative to certain medications and surgical interventions, thereby emerging as a novel clinical option for LDHR management. The evidence generated from this RCT may facilitate the integration of electroacupuncture into multimodal pain management strategies and inform updates to clinical practice guidelines for LDHR. Building upon the findings of this RCT, future research directions could prioritize extended follow-up studies to assess the sustainability of electroacupuncture effects and dose‒response relationship studies to identify optimal electroacupuncture regimens.
Trial Status
Protocol: version 1.0, 24 September 2024.
Date opened to recruitment: 15 October 2024.
Recruitment closure: 15 October 2025.
Data Sharing Statement
The datasets collected during the current study are available from the corresponding author on reasonable request.
Ethics Statements
The study protocol has been approved by the Ethics Committee of the Affiliated Hospital of Jiangxi University of Chinese Medicine (No. JZFYLL202400822103). Written informed consent will be obtained from all participants.
Acknowledgments
Yuwei Yang and Liting Liu are co-first authors of this study. The authors thank all those involved in the study, including practitioners, assessors and participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is supported by the National Natural Science Foundation of China [grant number 82460993], the Natural Science Foundation of Jiangxi Province [20242BAB20440], the Degree and Postgraduate Education Reform Project of Jiangxi Province [grant number JXYJG-2023-146], the Young Elite Scientists Sponsorship Program by the China Association of Chinese Medicine [grant number 2023-QNRC2-B29], the Ganpo Talents Support Program: University Leadership Talent Cultivation Project [grant number QN2023045], 2025 Central Government Transfer Payment Local Project—Traditional Chinese Medicine Treatment for Dominant Disease Categories (Clinical Evidence-Based Capacity Enhancement), and the Jiangxi University of Chinese Medicine Science and Technology Innovation Team Development Program [grant number CXTD-22012]. All funders had no role in the design of the study protocol and will have no role in the collection, analysis, or interpretation of the data or in the writing of the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Pojskic M, Bisson E, Oertel J, Takami T, Zygourakis C, Costa F. Lumbar disc herniation: epidemiology, clinical and radiologic diagnosis WFNS spine committee recommendations. World Neurosurg X. 2024;22:100279. doi:10.1016/j.wnsx.2024.100279
2. Yildirim P, Gultekin A. The effect of a stretch and strength-based yoga exercise program on patients with neuropathic pain due to lumbar disc herniation. Spine. 2022;47(10):711–719. doi:10.1097/BRS.0000000000004316
3. Kreiner DS, Hwang SW, Easa JE, et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J. 2014;14(1):180–191. doi:10.1016/j.spinee.2013.08.003
4. Deyo RA, Mirza SK. CLINICAL PRACTICE. herniated lumbar intervertebral disk. N Engl J Med. 2016;374(18):1763–1772. doi:10.1056/NEJMcp1512658
5. Gatchel RJ, Polatin PB, Mayer TG. The dominant role of psychosocial risk factors in the development of chronic low back pain disability. Spine. 1995;20(24):2702–2709. doi:10.1097/00007632-199512150-00011
6. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the spine patient outcomes research trial (SPORT): a randomized trial. JAMA. 2006;296(20):2441–2450. doi:10.1001/jama.296.20.2441
7. Rogerson A, Aidlen J, Jenis LG. Persistent radiculopathy after surgical treatment for lumbar disc herniation: causes and treatment options. Int Orthop. 2019;43(4):969–973. doi:10.1007/s00264-018-4246-7
8. Chou R, Hashimoto R, Friedly J, et al. Epidural corticosteroid injections for radiculopathy and spinal stenosis: a systematic review and meta-analysis. Ann Intern Med. 2015;163(5):373–381. doi:10.7326/M15-0934
9. Chang A, Ng AT. Complications associated with lumbar transforaminal epidural steroid injections. Curr Pain Headache Rep. 2020;24(11):67. doi:10.1007/s11916-020-00900-9
10. Chou R, Huffman LH, American Pain Society, American College of Physicians. Medications for acute and chronic low back pain: a review of the evidence for an American pain society/American college of physicians clinical practice guideline. Ann Intern Med. 2007;147(7):505–514. doi:10.7326/0003-4819-147-7-200710020-00008
11. Enthoven WT, Roelofs PD, Deyo RA, van Tulder MW, Koes BW. Non-steroidal anti-inflammatory drugs for chronic low back pain. Cochrane Database Syst Rev. 2016;2(2):Cd012087. doi:10.1002/14651858.CD012087
12. Benítez-Martínez JC, García-Haba B, Fernández-Carnero S, et al. Effectiveness of transcutaneous neuromodulation on abductor muscles electrical activity in subjects with chronic low back pain: a randomized, controlled, crossover clinical trial. J Pain Res. 2023;16:2553–2566. doi:10.2147/JPR.S409028
13. Chen X, Wang Z, Liang Y. Effectiveness of non-surgical treatment of lumbar disc herniation: a systematic review. Chin J Evid-Based Med. 2012;12(07):861–866.
14. Sillevis R, Cuenca-Zaldívar JN, Fernández-Carnero S, García-Haba B, Sánchez Romero EA, Selva-Sarzo F. Neuromodulation of the autonomic nervous system in chronic low back pain: a randomized, controlled, crossover clinical trial. Biomedicines. 2023;11(6):1551. doi:10.3390/biomedicines11061551
15. Molina-Payá FJ, Sánchez Romero EA, Fernández-Carnero S, Noguera-Iturbe Y, Selva-Sarzo F. Effect of transcutaneous neuromodulation on normalization of dermal body temperature and pain in a tender scar in the presence of low back pain: an update and case report. SAGE Open Med Case Rep. 2024;12:2050313x241249058. doi:10.1177/2050313X241249058
16. Huang F, Xiao Z, Zhan X, et al. Tuina combined with Adjuvant therapy for lumbar disc herniation: a network meta-analysis. Complement Ther Clin Pract. 2022;49:101627. doi:10.1016/j.ctcp.2022.101627
17. Martínez Pozas O, Cuenca-Zaldívar JN, González-Alvarez ME, et al. Effectiveness of mobilization with movement on conditioned pain modulation, mechanical hyperalgesia, and pain intensity in adults with chronic low back pain: a randomized controlled trial. Musculoskelet Sci Pract. 2025;75:103220. doi:10.1016/j.msksp.2024.103220
18. Kelly RB, Willis J. Acupuncture for pain. Am Fam Physician. 2019;100(2):89–96.
19. Vickers AJ, Vertosick EA, Lewith G, et al. Acupuncture for chronic pain: update of an individual patient data meta-analysis. J Pain. 2018;19(5):455–474. doi:10.1016/j.jpain.2017.11.005
20. Han JS. Acupuncture analgesia: areas of consensus and controversy. Pain. 2011;152(3 Suppl):S41–s48. doi:10.1016/j.pain.2010.10.012
21. Mayer DJ. Acupuncture: an evidence-based review of the clinical literature. Annu Rev Med. 2000;51:49–63. doi:10.1146/annurev.med.51.1.49
22. Chen H, Xu D, Chen S, Yang J, Wang Y. Effects of different body surface stimulation on 5-HT, CGRP and NPY inHuantiao and Yanglingquan acupoints of CCl rats. Chin J Tradit Chin Med Pharm. 2022;37(11):6471–6477.
23. Su TF, Zhao YQ, Zhang LH, et al. Electroacupuncture reduces the expression of proinflammatory cytokines in inflamed skin tissues through activation of cannabinoid CB2 receptors. Eur J Pain. 2012;16(5):624–635. doi:10.1002/j.1532-2149.2011.00055.x
24. Liu Y, Du J, Fang J, et al. Electroacupuncture inhibits the interaction between peripheral TRPV1 and P2X3 in rats with different pathological pain. Physiol Res. 2021;70(4):635–647. doi:10.33549/physiolres.934649
25. Liao HY, Hsieh CL, Huang CP, Lin YW. Electroacupuncture attenuates CFA-induced inflammatory pain by suppressing Nav1.8 through S100B, TRPV1, opioid, and adenosine pathways in mice. Sci Rep. 2017;7:42531. doi:10.1038/srep42531
26. Chen T, Zhang WW, Chu YX, Wang YQ. Acupuncture for pain management: molecular mechanisms of action. Am J Chin Med. 2020;48(4):793–811. doi:10.1142/S0192415X20500408
27. Liao HY, Hsieh CL, Huang CP, Lin YW. Electroacupuncture attenuates induction of inflammatory pain by regulating opioid and adenosine pathways in mice. Sci Rep. 2017;7(1):15679. doi:10.1038/s41598-017-16031-y
28. Duan-Mu CL, Zhang XN, Shi H, et al. Electroacupuncture-induced muscular inflammatory pain relief was associated with activation of low-threshold mechanoreceptor neurons and inhibition of wide dynamic range neurons in spinal dorsal horn. Front Neurosci. 2021;15:687173. doi:10.3389/fnins.2021.687173
29. Yu Q, Yuan M, Sun X, et al. Electroacupuncture at different intensities inhibits nociceptive discharges of wide dynamic range neurons in spinal dorsal horn of rats. Acupunct Res. 2024;49(05):448–455.
30. Han Z, Jiang YH, Wan Y, Wang Y, Chang JK, Han JS. Endomorphin-1 mediates 2 hz but not 100 hz electroacupuncture analgesia in the rat. Neurosci Lett. 1999;274(2):75–78. doi:10.1016/S0304-3940(99)00670-9
31. Lu Q, Wang F, Zhang T, Kuai L, Chen H. Effects of electroacupuncture with different current intensities on Bendorphin levels in peripheral blood in rats with tibial cancer pain. Chin J Tradit Chin Med Pharm. 2015;30(09):3329–3332.
32. Meng Q, Wang X. To compare the effect of treating lumber disc protrusion(LDP) with different waveform and frequency of electroacupuncture. Chin J Clin Rehabil. 2002;2002(16):2370–2375.
33. Mao JJ, Liou KT, Baser RE, et al. Effectiveness of electroacupuncture or auricular acupuncture vs usual care for chronic musculoskeletal pain among cancer survivors: the peace randomized clinical trial. JAMA Oncol. 2021;7(5):720–727. doi:10.1001/jamaoncol.2021.0310
34. Lv ZT, Shen LL, Zhu B, et al. Effects of intensity of electroacupuncture on chronic pain in patients with knee osteoarthritis: a randomized controlled trial. Arthritis Res Ther. 2019;21(1):120. doi:10.1186/s13075-019-1899-6
35. Wu HC, Liu YC, Ou KL, et al. Effects of acupuncture on post-cesarean section pain. Chin Med J. 2009;122(15):1743–1748.
36. Sator-Katzenschlager SM, Scharbert G, Kozek-Langenecker SA, et al. The short- and long-term benefit in chronic low back pain through adjuvant electrical versus manual auricular acupuncture. Anesthesia Analgesia;2004. 1359–1364. doi:10.1213/01.ANE.0000107941.16173.F7
37. Torres SF, de Macedo ACB, Sakai RY, Bressan GCS, Dos Santos MBR, Marques AP. Effect of different frequencies of electroacupuncture on chronic low back pain in older adults: a triple-blind, placebo-controlled, randomized clinical trial. Pain Physician. 2023;26(2):161–173. doi:10.36076/ppj.2023.26.161
38. Kong JT, Puetz C, Tian L, et al. Effect of electroacupuncture vs sham treatment on change in pain severity among adults with chronic low back pain: a randomized clinical trial. JAMA Netw Open. 2020;3(10):e2022787. doi:10.1001/jamanetworkopen.2020.22787
39. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
40. Butcher NJ, Monsour A, Mew EJ, et al. Guidelines for reporting outcomes in trial reports: the CONSORT-outcomes 2022 extension. JAMA. 2022;328(22):2252–2264. doi:10.1001/jama.2022.21022
41. Chan AW, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586. doi:10.1136/bmj.e7586
42. MacPherson H, Vertosick E, Lewith G, et al. Influence of control group on effect size in trials of acupuncture for chronic pain: a secondary analysis of an individual patient data meta-analysis. PLoS One. 2014;9(4):e93739. doi:10.1371/journal.pone.0093739
43. White AR, Filshie J, Cummings TM. Clinical trials of acupuncture: consensus recommendations for optimal treatment, sham controls and blinding. Complement Ther Med. 2001;9(4):237–245. doi:10.1054/ctim.2001.0489
44. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19. doi:10.1016/j.pain.2004.09.012
45. Ostelo RW, Deyo RA, Stratford P, et al. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine. 2008;33(1):90–94. doi:10.1097/BRS.0b013e31815e3a10
46. Stevens ML, Lin CC, Maher CG. The Roland Morris Disability Questionnaire. J Physiother. 2016;62(2):116. doi:10.1016/j.jphys.2015.10.003
47. Jordan K, Dunn KM, Lewis M, Croft P. A minimal clinically important difference was derived for the Roland-Morris Disability Questionnaire for low back pain. J Clin Epidemiol. 2006;59(1):45–52. doi:10.1016/j.jclinepi.2005.03.018
48. Yao M, Yang L, Zhu B, et al. Simplified Chinese version of the Japanese orthopaedic association back pain evaluation questionnaire: agreement, responsiveness, and minimal important change for patients with chronic low back pain. Spine. 2018;43(20):1438–1445. doi:10.1097/BRS.0000000000002692
49. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56–62. doi:10.1136/jnnp.23.1.56
50. Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018;391(10128):1357–1366. doi:10.1016/S0140-6736(17)32802-7
51. Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50–55. doi:10.1111/j.2044-8341.1959.tb00467.x
52. Xiong Z, Hu Y, Zhang J, et al. The calculation of the minimal clinically important differences of anxiety depression and quality of life scale in patients with pelvic organ prolapse. Chin J Clin Obstet Gynecol. 2022;23(04):378–381.
53. Alsaadi SM, McAuley JH, Hush JM, et al. Detecting insomnia in patients with low back pain: accuracy of four self-report sleep measures. BMC Musculoskelet Disord. 2013;14:196. doi:10.1186/1471-2474-14-196
54. Johansen PM, Trujillo FA, Hagerty V, Harland T, Davis G, Pilitsis JG. Establishing minimal clinically important difference in sleep outcomes after spinal cord stimulation in patients with chronic pain disorders. Stereotact Funct Neurosurg. 2023;101(1):41–46. doi:10.1159/000527257
55. Nicholas MK. The pain self-efficacy questionnaire: taking pain into account. Eur J Pain. 2007;11(2):153–163. doi:10.1016/j.ejpain.2005.12.008
56. Suzuki H, Aono S, Inoue S, et al. Clinically significant changes in pain along the pain intensity numerical rating scale in patients with chronic low back pain. PLoS One. 2020;15(3):e0229228. doi:10.1371/journal.pone.0229228
57. Bang H. Random guess and wishful thinking are the best blinding scenarios. Contemp Clin Trials Commun. 2016;3:117–121. doi:10.1016/j.conctc.2016.05.003
58. Bang H, Ni L, Davis CE. Assessment of blinding in clinical trials. Control Clin Trials. 2004;25(2):143–156. doi:10.1016/j.cct.2003.10.016
59. James KE, Bloch DA, Lee KK, Kraemer HC, Fuller RK. An index for assessing blindness in a multi-centre clinical trial: disulfiram for alcohol cessation--a VA cooperative study. Stat Med. 1996;15(13):1421–1434. doi:10.1002/(SICI)1097-0258(19960715)15:13<1421::AID-SIM266>3.0.CO;2-H
60. Hertzberg V, Chimowitz M, Lynn M, Chester C, Asbury W, Cotsonis G. Use of dose modification schedules is effective for blinding trials of warfarin: evidence from the WASID study. Clin Trials. 2008;5(1):23–30. doi:10.1177/1740774507087781
61. Whiteside MM, Shorter ES, Margolis MS, et al. Success of masking 5% povidone-iodine treatment: the reducing adenoviral patient infected days study. Optom Vis Sci. 2021;98(5):469–475. doi:10.1097/OPX.0000000000001691
62. Fu X, Wang YQ, Wu GC. Involvement of nociceptin/orphanin FQ and its receptor in electroacupuncture-produced anti-hyperalgesia in rats with peripheral inflammation. Brain Res. 2006;1078(1):212–218. doi:10.1016/j.brainres.2006.01.026
63. Sprouse-Blum AS, Smith G, Sugai D, Parsa FD. Understanding endorphins and their importance in pain management. Hawaii Med J. 2010;69(3):70–71.
64. Cao XH, Chen SR, Li L, Pan HL. Nerve injury increases brain-derived neurotrophic factor levels to suppress BK channel activity in primary sensory neurons. J Neurochem. 2012;121(6):944–953. doi:10.1111/j.1471-4159.2012.07736.x
65. Maughan EF, Lewis JS. Outcome measures in chronic low back pain. Eur Spine J. 2010;19(9):1484–1494. doi:10.1007/s00586-010-1353-6
66. Haase I, Kladny B. Clinical relevance of changes in pain intensity in patients with specific back pain. Z Orthop Unfall. 2022;160(2):213–221. doi:10.1055/a-1304-3677
67. Childs JD, Piva SR, Fritz JM. Responsiveness of the numeric pain rating scale in patients with low back pain. Spine. 2005;30(11):1331–1334. doi:10.1097/01.brs.0000164099.92112.29
68. Cheon S, Park HJ, Chae Y, Lee H. Does different information disclosure on placebo control affect blinding and trial outcomes? A case study of participant information leaflets of randomized placebo-controlled trials of acupuncture. BMC Med Res Methodol. 2018;18(1):13. doi:10.1186/s12874-018-0474-1
69. Birch S. A review and analysis of placebo treatments, placebo effects, and placebo controls in trials of medical procedures when sham is not inert. J Altern Complement Med. 2006;12(3):303–310. doi:10.1089/acm.2006.12.303
70. Lv Q, Wu F, Gan X, et al. The involvement of descending pain inhibitory system in electroacupuncture-induced analgesia. Front Integr Neurosci. 2019;13:38. doi:10.3389/fnint.2019.00038
71. Xiong ZY, Liu XY, Ma PH, et al. Placebo response among different types of sham acupuncture for low back pain: a systematic review and meta-analysis of randomized controlled trials. Chin J Integr Med. 2023;29(10):941–950. doi:10.1007/s11655-023-3608-1
72. Zhang YH, Xu HR, Yang QH, et al. Associations between back pain incidence, and physical activity and sedentary behaviours: a prospective cohort study with data from over 365,000 participants. J Orthop Sports Phys Ther. 2024;54(7):468–476. doi:10.2519/jospt.2024.12338
73. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/ALN.0000000000000101
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Combination Treatment with Thread-Embedding Acupuncture and Electroacupuncture for Knee Osteoarthritis Patients with Postoperative Pain: A Randomized Controlled Feasibility Study
Lee YJ, Han CH, Jeon JH, Kim E, Park KH, Kim AR, Kim YI
Journal of Pain Research 2025, 18:89-103
Published Date: 8 January 2025
The Clinical Effect of Electroacupuncture Combined with Surround Needling in the Treatment of Acute Lateral Ankle Sprain Based on Musculoskeletal Ultrasound Imaging Technology: A Protocol for a Single-Centre, Randomized, Controlled Trial
Chen L, Hu Q, Gao H, Tang D
Journal of Pain Research 2025, 18:2467-2478
Published Date: 15 May 2025