")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
A Retrospective Machine Learning Analysis to Predict 3-Month Nonunion of Unstable Distal Clavicle Fracture Patients Treated with Open Reduction and Internal Fixation
Authors Ma C, Lu W, Liang L, Huang K, Zou J
Received 5 February 2025
Accepted for publication 28 April 2025
Published 5 May 2025 Volume 2025:21 Pages 633—645
DOI https://doi.org/10.2147/TCRM.S518774
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Changke Ma,1,* Wei Lu,2,3,* Limei Liang,4,* Kaizong Huang,3 Jianjun Zou3,5
1Department of Orthopaedics, Nanjing Luhe People’s Hospital, Yangzhou University, Nanjing, People’s Republic of China; 2School of Basic Medicine and Clinical Pharmacy, China Pharmaceutical University, Nanjing, People’s Republic of China; 3Department of Pharmacology, Nanjing First Hospital, Nanjing Medical University, Nanjing, People’s Republic of China; 4Department of Rehabilitation, Nanjing Luhe People’s Hospital, Yangzhou University, Nanjing, People’s Republic of China; 5Department of Pharmacy, Nanjing First Hospital, China Pharmaceutical University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kaizong Huang, Email [email protected] Jianjun Zou, Email [email protected]
Background: This retrospective study aims to predict the risk of 3-month nonunion in patients with unstable distal clavicle fractures (UDCFs) treated with open reduction and internal fixation (ORIF) using machine learning (ML) methods. ML was chosen over traditional statistical approaches because of its superior ability to capture complex nonlinear interactions and to handle imbalanced datasets.
Methods: We collected UDCFs patients at Nanjing Luhe People’s Hospital (China) between January 2015 and May 2023. The unfavorable outcome was defined as 3-month nonunion, as represented by disappeared fracture line and continuous callus. Patients meeting inclusion criteria were randomly divided into training (70%) and testing (30%) sets. Five ML models (logistic regression, random forest classifier, extreme gradient boosting, multi-layer perceptron, and category boosting) were developed. Those models were selected based on univariate analysis and refined using the Least Absolute Shrinkage and Selection Operator (LASSO). Model performance was evaluated using AUROC, AUPRC, accuracy, sensitivity, specificity, F1 score, and calibration curves.
Results: A total of 248 patients were finally included into this study, and 76 (30.6%) of them had unfavorable outcomes. While all five models showed similar trends, the CatBoost model achieved the highest performance (AUROC = 0.863, AUPRC = 0.801) with consistent identification of the risk factors mentioned above. The SHAP values identified the CCD as the significant predictor for assessing the risk of 3-month nonunion in patients with UDCFs within the Chinese demographic.
Conclusion: The refined model incorporated four readily accessible variables, wherein the CCD, HDL levels, and blood loss were associated with an elevated risk of nonunion. Conversely, the application of nerve blocks, including postoperative block, was correlated with a reduced risk. Our results suggest that ML, particularly the CatBoost model, can be integrated into clinical workflows to aid surgeons in optimizing intraoperative techniques and postoperative management to reduce nonunion rates.
Keywords: distal clavicle fracture, machine learning, prediction, nonunion
Introduction
Distal clavicle fractures constitute a prevalent type of upper limb fracture, representing 28% of all adult clavicle fractures.1 Among these, 10% to 52% are classified as displaced and unstable, attributed to the multidirectional forces exerted by the robust trapezius, latissimus dorsi, and pectoral muscles.2 Recent research indicates that the nonunion rate for unstable distal clavicle fractures (UDCFs) subjected to nonoperative treatment can reach up to 30%.3,4 Consequently, Open reduction and internal fixation (ORIF), incorporating anatomic locking plate and hook plate techniques, is widely recommended in China. Nevertheless, clinicians frequently encounter adverse outcomes, including internal fixation failure, re-fracture, 3-month nonunion (ie, delayed union) and eventual bone nonunion.5–8 Nonunion poses significant treatment challenges and incurs considerable financial burdens, with indirect costs like productivity losses being pivotal in escalating the total expenses for non-union patients. Hence, any strategy aimed at reducing healing duration, facilitating quicker return to work, and minimizing financial implications should be advocated for patients with fractures and non-unions. Predicting high-risk factors following UDCFs could yield compelling evidence to guide reasonable intraoperative and postoperative interventions, thereby abbreviating the disease course and alleviating discomfort.
Some studies reveal that various risk factors are associated with the adverse outcomes of 3-month nonunion and nonunion in fracture patients. These include physiological factors (eg, advanced age, smoking), comorbidities (eg, metabolic diseases, use of non-steroidal anti-inflammatory drugs, diabetes, nutritional deficiencies), and patient-specific factors (eg, fracture pattern and location, displacement, infection, degree of bone loss, and severity of soft tissue injury).9,10 Distal clavicle fractures, particularly unstable types, are prone to complications such as nonunion, significantly impacting patient recovery and healthcare resources. Despite advancements in surgical techniques, the nonunion rates remain high, posing a challenge for effective management. Traditional functional assessments of the shoulder joint, such as the Constant-Murley and Neer scores, predominantly evaluate recovery from a functional standpoint without providing reliable predictions for fracture healing outcomes.
Recent research has demonstrated the growing application of ML models in the medical sector.11–16 Logistic regression is a mature modeling technique in public health, boasts high computational efficiency and accurate predictions.17,18 Random forest is a robust machine learning algorithm, combines multiple-decision trees to effectively mitigate overfitting and handle both discrete and continuous data without normalization.19 Extreme gradient boosting is a classic ensemble boosting framework, excels in high training efficiency, good prediction outcomes, numerous controllable parameters, and user-friendly implementation.20 Multi-layer perceptron is a neural network model capable of capturing complex patterns and relationships in data through its layered architecture, offering high flexibility and predictive power.21 Category boosting enhances the performance of categorical data predictions by combining multiple weak learners, focusing on difficult-to-classify instances for improved accuracy.
In comparison to traditional regression models, ML has been validated as an effective method for prognosis prediction in modeling due to its capacity to intricately analyze complex non-linear interrelations among variables,22,23 and to enhance prediction accuracy through its superior algorithms, particularly when analyzing large datasets with numerous variables.24,25 Crucially, the widespread adoption of Electronic Patient Record systems and the extensive use of structured patient data have made sophisticated algorithmic modeling and bedside application feasible.26
Recent studies emphasize the potential of predictive modeling in enhancing the prognosis of fracture healing by identifying risk factors that are not immediately modifiable but crucial for postoperative management. Recognizing the significant variability in nonunion rates across different demographics and institutions, our study aims to develop a machine learning model that incorporates both modifiable and non-modifiable predictors. This approach seeks to enable tailored postoperative strategies to mitigate the risk of 3-month nonunion and enhance patient outcomes across diverse clinical settings. By focusing on a high-risk population within a specific medical setting, this study provides a foundation for validating our model in broader contexts, thereby addressing the pressing need for precise and adaptable predictive tools in orthopedic surgery.
Patients and Methods
Study Population
This retrospective study was performed in the Nanjing Luhe People’s Hospital, China, where electronic health records from the orthopedic unit for patients diagnosed with UDCFs were collected and analyzed, spanning from January 2015 to May 2023. Before data collection, we estimated the minimum sample size required using the 10 EPV (events per variable) rule. We expected 4 variables to enter our final and assume that in our database incidence rate of the outcome is 25% based on previous study. Therefore, we need at least (4*10)/0.25=160 patients according to the EPV rule. The primary outcome was the union of UDCFs within the first three months post-operation, as determined by clinical signs of healing and corroborated by shoulder X-rays images. The exclusion criteria were patients with incomplete clinical or pre-treatment data, those receiving conservative treatment, individuals under 18, and patients with concurrent neurovascular injuries.
Predictors and Outcomes
In this study, the candidate variables for our model included demographic factors such as age, sex, smoking status, drinking status, level of education, and labor intensity, medical histories like diabetes mellitus, hypertension, anemia, and hypoproteinemia, baseline characteristics including height, weight, diastolic and systolic blood pressures, presence of comminuted or multiple fractures, and results of blood biochemical tests, as well as surgical details such as the method of operation, types of implants (including the lateral locking plate and Hook plate), CCD, type of anesthesia, duration of surgery, volume of blood loss, length of incision, and use of osteogenic stimuli, and postoperative outcomes, including 3-month fracture union status and complications.
We sought to predict a binary outcome, either the achievement of union within 3 months or a 3-month nonunion, and evaluated the status of fracture union during the initial 3 months postoperatively by analyzing shoulder X-rays images, focusing on the disappearance of the fracture line and the formation of continuous callus as indicators of union. CCD was defined as the measure between the coracoid process and the inferior aspect of the clavicle,27 determined from shoulder X-ray images taken within 7 days after surgery. In addition, educational attainment was categorized into two levels: high, for those with college education, and low, for those without.
Data Pre-Processing
The dataset was randomly split into a training set (70% of the cases) and a testing set (30% of the cases) to ensure robust internal validation of the predictive models. Two methods were mainly used to deal with missing data in both training and test sets. Variables with a missing data rate exceeding 30% were removed outright from the dataset, and for the rest of remaining variables exhibiting missing values, multiple imputation employing predictive mean matching (PMM) was executed. The One-Hot Encoding technique was applied to transform multiple categorical variables into dummy variables. Whereas continuous variables underwent normalization by a z-score.
Model Development and Validation
In order to select the variables that would eventually develop models, we used the LASSO algorithm to process variables that demonstrated statistical significance in univariate analysis. The variables retaining nonzero coefficients following the LASSO were selected as the final variables for model development.
Five machine learning classifiers—logistic regression (LR), random forest classifier (RFC), extreme gradient boosting (XGB), multi-layer perceptron (MLP), and CatBoost—were employed. Their performance was compared using evaluation metrics such as AUROC, AUPRC, accuracy, sensitivity, specificity, F1 score, and calibration curves. The optimal parameters for each algorithm were determined by the grid search algorithm coupled with 10-fold cross-validation. The test set in our study provided data for internal validation to demonstrate the generalization of the machine learning model, ensuring the model, developed from the training data, maintained its applicability.
Model Evaluation
Due to the imbalance within our dataset, AUPRC was selected as the principal evaluation metric, which has been proven to be superior to AUROC, especially in the context of imbalanced data. In addition, accuracy, recall, precision, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and the F1 score were served as metrics to evaluate the models. A calibration curve analysis was also carried out to visually evaluate the degree of agreement between the model’s predicted and actual probabilities.
Model Interpretation
SHAP method was used to evaluate variable importance and provide an explanation for the predictions generated by ML algorithms in order to gain a better understanding of the machine learning model’s predictive process. SHAP is a useful tool that helps boost the model’s credibility and acceptability in clinical environments, which illustrates how each variable contributes to and influences the risk of 3-month nonunion.
Statistical Analysis
Baseline characteristics were compared between the control group and the 3-month nonunion cohort. The Shapiro–Wilk test was used firstly to determine whether continuous variables were normally distributed. Descriptive statistics were presented as means with standard deviations (for normally distributed variable), or medians with IQR (for non-normally distributed variable), and frequency (percentages) for categorical variables, respectively. We used the Student’s t-test or the Mann–Whitney U-test to assess the differences in continuous variables, while for categorical variables, the Chi-squared or Fisher’s exact tests were performed. The above statistical analysis conducted with the statistical package R, version 4.1.3 (R Development Core Team, Auckland, New Zealand), and p-values less than 0.05 was considered statistically significant.
Results
Baseline Characteristics
We analyzed the data of 248 patients treated for UDCFs from January 2015 to May 2023. In general, the overall median age was 55 years, interquartile ranges (IQR): 47–63 years, and with males constituting 60.1% of the cohort. 3-month nonunion was observed in 76 patients (30.6%, median age: 55 years, number of male patients: 52), finally 6 cases had bone nonunion after extended follow-up time, and underwent secondary surgery. Whereas 172 patients exhibited primary healing post-procedure (69.4%, median age: 54.5 years, number of male patients: 97). After data split, 173 patients were allocated to the training set and 75 to the test set. The detailed baseline information of the training set is shown in Table 1 and the training set and the testing set were similar in baseline characteristics.
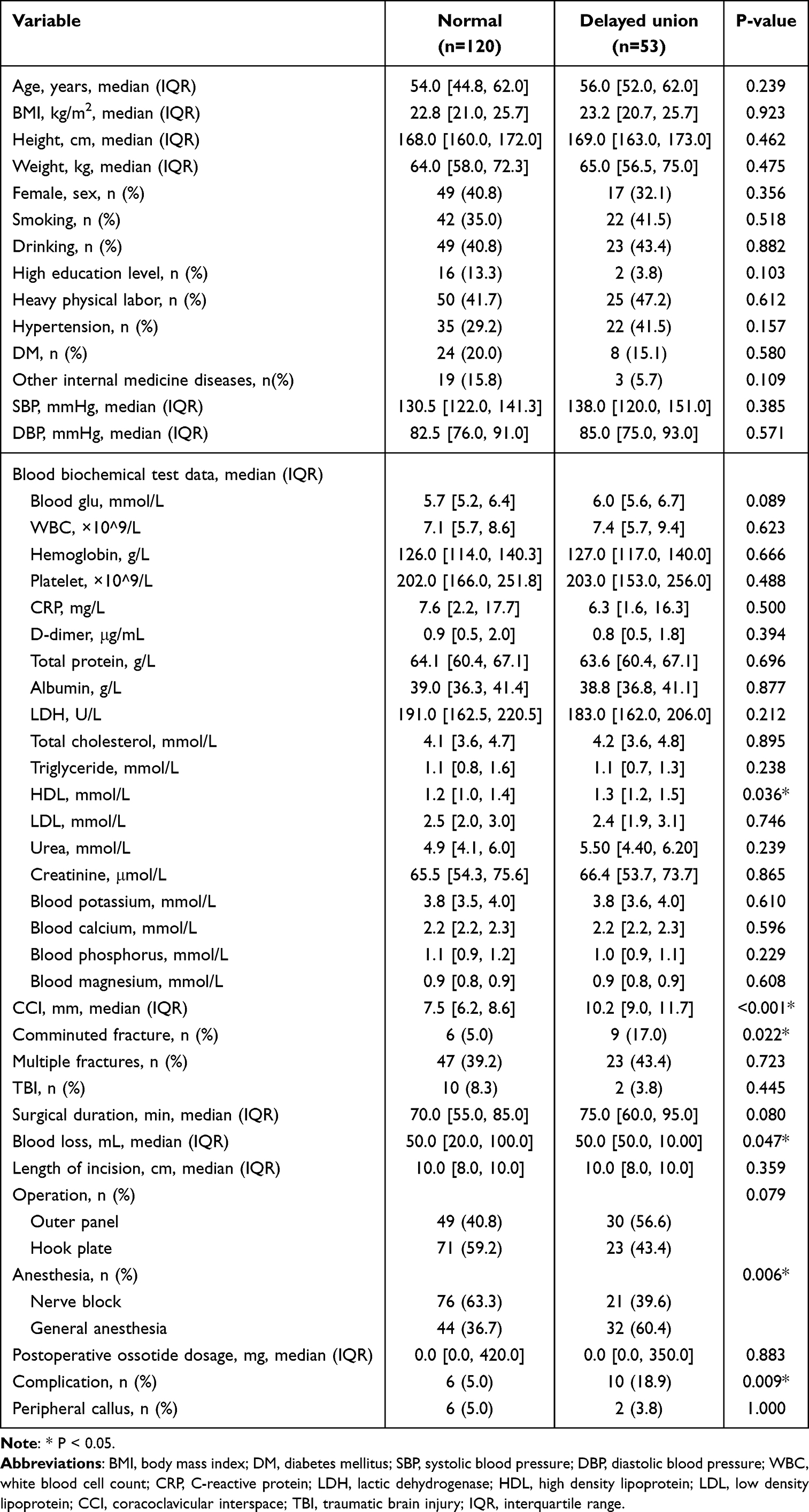 |
Table 1 Baseline Characteristics of Patients in Normal and Delayed Union Groups in the Training Set |
Feature Selection
Seven of the 47 variables we gathered that may be connected to 3-month nonunion were statistically significant after univariate analysis. Furthermore, after exclusion of variables with zero coefficients through the Least Absolute Shrinkage and Selection Operator(LASSO) process, we ultimately used four variables for model construction: Coracoclavicular distance(CCD), anesthesia method, High-density lipoprotein(HDL), and blood loss. The detailed coefficients of these non-zero coefficient variables are detailed in Supplementary Table 1.
Model Performance
All machine learning models that have been constructed have demonstrated similar performance, with no significant differences in AUROCs, as determined by the DeLong test (Supplementary Table 2). Among the five predictive models, the Category Boosting (CatBoost) model attained the greatest AUROC (0.863, 95% CI: 0.762–0.964) and Area Under the Precision-Recall Curve (AUPRC 0.801, 95% CI: 0.592–0.918), the highest accuracy (74.7%), F1 score (0.689), and PPV (55.3%) in the test set. AUROCs and AUPRCs for both the training and test sets are depicted in Figure 1. In addition, the calibration curve, presented in Figure 2, demonstrates a good alignment between the predictions of the CatBoost model and the actual outcomes. Evaluation metrics for all models are compiled in Table 2.
 |
Table 2 The Performance of the Models in Training and Test Set |
 |
Figure 1 Receiver operating characteristic (ROC) curve and precision-recall curve (PRC) of the five models for predicting the risk of 3-month nonunion. (a) The ROC curve of the training set. (b) The ROC curve of the testing set. (c) The PRC of the training set. (d) The PRC of the testing set. Abbreviations: LR, logistic regression; RFC, random forests classifier; XGB, eXtreme gradient boosting; MLP, multi-layer perceptron; CatBoost, category boosting. |
 |
Figure 2 Calibration curve of the five models. Abbreviations: LR, logistic regression; RFC, random forests classifier; XGB, eXtreme gradient boosting; MLP, multi-layer perceptron; CatBoost, category boosting. |
Model Interpretation
We offer Figure 3 as the global interpretation to the prediction behavior of the CatBoost model using SHapley Additive exPlanations(SHAP). Our model identified CCD as the main driving factor based on the mean absolute SHAP value as Figure 3a shows. Figure 3b summarizes the direction of effects for each variable. Feature values are indicated by a spectrum with blue representing the lowest value and red color indicates higher risk of 3-month nonunion while blue color shows lower risk. As a result, the variables included in the CatBoost are all risk factors except for the anesthesia method of nerve block.
 |
Figure 3 Shapley additive explanations (SHAP) plots of the selected variables in the CatBoost model. (a) The mean absolute SHAP value ranks the relative importance of the variables in the model. (b) The direction of effects for each variable in the model. Abbreviations: CCD, coracoclavicular distance; HDL, high density lipoprotein. |
From our result, this study is the first to employ ML techniques for predicting 3-month nonunion in UDCF patients treated with ORIF within a Chinese cohort, providing novel insights into both risk stratification and potential avenues for clinical intervention.
Discussion
Despite the clinical efficacy of diverse surgical approaches in managing UDCFs, the issue of postoperative nonunion persists, influenced by numerous factors pre-, intra-, and post-operatively. Accurately predicting the risk of nonunion following ORIF remains an unresolved challenge. Developing a prediction model for the risk of 3-month nonunion among UDCFs patients aids in identifying risk factors and facilitates early intervention to reduce incidence.
A significant advantage of our model is its outstanding performance. This study employed five distinct machine learning methodologies to develop a predictive model for the risk of 3-month nonunion in Chinese patients with UDCFs undergoing ORIF, based on four critical variables: CCD, anesthesia method (nerve block), HDL, and blood loss. Among these models, the CatBoost model emerged as the most effective, achieving an AUPRC of 0.801, a critical measure for assessing the predictive accuracy of models trained on imbalanced datasets. In addition, other evaluation metrics such as sensitivity and F1 score also achieve better performance. Subsequently, risk stratification was executed using the optimal threshold defined by the CatBoost model, enabling the high-risk group identified by the model to benefit from preventive interventions targeting CCD, HDL and blood loss. The results showed that CCD, HDL levels, and blood loss were associated with an elevated risk of 3-month nonunion. Conversely, the application of nerve blocks, including postoperative block, was correlated with a reduced risk.
Risk Factors Affecting Fracture Union
It is well known that many factors can affect bone union. Qvist et al 28 conducted a retrospective analysis of 150 clavicle fracture cases, assessing eight factors: age, sex, smoking status, comminuted fractures, fracture shortening exceeding 2 cm, Disabilities of the Arm, Shoulder and Hand (DASH) scores, Visual Analogue Scale (VAS) scores, and the VAS ratio (four-week VAS score/two-week VAS score). Their findings revealed that: (1) a rise in the absolute pain score 4 weeks post-fracture correlated with a heightened risk of nonunion at 6 months; (2) patients with a VAS ratio above 0.6 faced an 18-fold increased relative risk of nonunion compared to those with a VAS ratio below 0.6. Nicholson et al 29 conducted a prospective follow-up of 200 patients with clavicle fractures, assessing them 6 weeks post-fracture to predict the likelihood of nonunion after 6 months. The AUROC of the final established model was 0.873. This study gathered data on 7 patient-related factors, 3 fracture characteristics, 5 outcomes from physical examinations, and 3 results from subjective functional evaluations. Analysis via a conditional stepwise regression model indicated that a QuickDASH score ≥ 40, absence of callus formation in X-ray images, and fracture displacement observed during physical examinations were predictors of nonunion. Takahashi et al 30 used ML to predicted osteoporotic vertebral fracture nonunion, the ML architecture utilized in this study included a logistic regression model, decision tree, extreme XGBoost, and random forest RF, and found that MRI findings, anterior height ratio, kyphotic angle, posterior wall injury, fracture level, and smoking habit ranked as important features in the ML algorithms. Leister et al 31 used XGBoost algorithm to identify treatment-related risk factors, found that the odds of odontoid fracture nonunion increased significantly with age. Similar to the aforementioned studies, our research serves as a risk alert for 3-month nonunion; however, we discovered that preoperative HDL levels, intraoperative blood loss, and postoperative CCD were linked to the risk of nonunion, diverge from those of previous research, likely due to its foundation on distinct risk factors. These predictors are readily ascertainable via laboratory tests, imaging examination and surgical documentation, and the developed model based on these risk factors has relatively good prediction performance (AUROC of the Catboost is 0.863 and the AUPRC is 0.801). This significantly aids clinicians in making tailored and accurate treatment decisions for high-risk individuals, thereby mitigating the risk of 3-month nonunion and offering broad applicability in clinical settings.
Predicted Factors
Our results indicate that an increased CCD is associated with a higher risk of 3-month nonunion. It is widely recognized that conservative treatment of UDCFs carries a higher risk of nonunion and may result in shoulder instability.32–34 The coracoclavicular ligament is pivotal in stabilizing the acromioclavicular joint, consisting of the trapezoid and conoid ligaments. These components are instrumental in preventing forward and backward displacement, as well as upward rotation of the clavicle. Notably, the trapezoid ligament exhibits a significantly enhanced capacity to restrict backward displacement compared to the conoid ligament.35,36 An increase in the CCD is predominantly attributed to injuries of the coracoclavicular ligament, which leads to stress concentration at the distal fracture end, thereby diminishing stability. Fleming et al 37 highlighted that combined coracoclavicular ligament repair more effectively restores the CCD and stabilizes the acromioclavicular joint. Surgical strategies to restore the CCD typically encompass ORIF for anatomical realignment, Coracoclavicular Screw Fixation in cases where ligaments are intact, Ligament Reconstruction with grafts to replicate shoulder biomechanics, Hook Plate Fixation for provisional stability, and minimally invasive Arthroscopic Techniques utilizing various devices for less invasive interventions.38 Therefore, radiological images reveal significantly increased CCD in the preoperative or intraoperative, which suggest that it is necessary to reevaluate the stability and surgical strategy.
Second, our findings indicate that anesthesia impacts bone nonunion three months post-surgery, with nerve blocks, including postoperative nerve block, potentially serving as a protective factor against nonunion outcomes. A variety of anesthesia can be employed in clavicular surgeries,39–42 however an increasing body of literature advocates for the use of nerve blocks. Nerve blocks alleviate pain by inhibiting nerve cells from transmitting electrical signals that the brain interprets as pain. This effect is accomplished through anesthetics that obstruct the nerve receptors tasked with detecting damage or injury. Additionally, nerve blocks diminish inflammation, which aids in nerve recovery and further lessens pain.1,39 Certain studies have suggested that mitigating absolute pain may be advantageous for the union outcome following unstable distal clavicle fractures.43 A separate retrospective cohort study revealed that employing regional anesthesia in ORIF for clavicle fractures correlated with a higher rate of same-day discharge.44 Ryan et al 45 discovered that the combined use of brachial plexus regional anesthesia with a modified superficial cervical plexus block constitutes a dependable and effective approach, potentially offering advantages in terms of anesthesia initiation and overall case duration. Our retrospective analysis suggesting that opting for nerve block anesthesia, including postoperative nerve block, could diminish the risk of 3-month nonunion.
Third, HDL have a significant impact on the pathology and management of conditions such as atherosclerosis, morbid obesity, nonalcoholic fatty liver disease, type 2 diabetes, and various central nervous system disorders.46 Researchers have uncovered a novel function of HDL in the development of degenerative and metabolic bone diseases through experimental mouse studies.47,48 The findings indicate that reduced and dysfunctional HDL levels may contribute to a higher incidence of these diseases by influencing the molecular mechanisms involved in bone synthesis and degradation. Studies have reported that elevated HDL-C levels are linked to osteoporosis 49 and an increased risk of fractures.50,51 The relationship between high HDL-C levels, low bone mineral density, and osteoporosis,52 along with a genome-wide association study linking high HDL-C to low bone mineral density,53 may offer a pathophysiological explanation. A case-control study by Quan et al 54 identified osteoporosis as an independent risk factor for bone nonunion. Furthermore, another study presented high-quality evidence of a negative correlation between HDL-C levels and bone mineral density.55 Integrating these findings with our research suggests that an increased HDL-C levels may be associated with a heightened risk of nonunion. However, this view conflicts with other opinions that assert no association between HDL-C levels and osteoporosis.56 Thus, whether high HDL levels exacerbate the risk of 3-month nonunion requires further investigation.
Fourth, our research identified a correlation between intraoperative blood loss and the risk of 3-month nonunion. Research has demonstrated that formation of callus beyond the fracture site predominantly relies on the vascular supply to the periosteum and adjacent soft tissues. Furthermore, factors like trauma, excessive displacement at the fracture site, comminuted fractures, and both open and closed soft tissue injuries can impair the local blood supply. Surgical interventions can further influence the vascular supply to the fracture site, necessitating procedures like extended wound exposure, periosteal stripping, and varying levels of damage to surrounding soft tissues. Following a fracture, the blood supply to the affected end is compromised, and full restoration of vascular supply to this area may take over 6 months. 57 Insufficient blood supply prevents callus formation and increases the risk of nonunion. To mitigate the risk of postoperative nonunion, a multifaceted approach is essential for managing intraoperative hemorrhage: (1) Minimizing surgical trauma and employing minimally invasive techniques are crucial for preserving the peripheral blood supply, especially the protection of periosteum; 38 (2) The application of advanced hemostatic methods, including electrocoagulation and topical hemostatic agents, is recommended; 58 (3) It is imperative to secure stable fracture fixation to minimize displacement at the fracture site; (4) Postoperative care should encompass optimal nutrition and the initiation of controlled activities to enhance circulation; (5) The administration of anti-fibrinolytic agents, for instance, triamcinolone, is advocated to curtail bleeding.59 Employing these comprehensive strategies is beneficial for sustaining an adequate blood supply at the fracture site, thereby diminishing the likelihood of 3-month nonunion.
Practical Implications of Predictive Modeling
Our results suggest that while some predictors like HDL and intraoperative blood loss are not directly modifiable during surgery, their identification is vital for postoperative management. For instance, elevated preoperative HDL and significant intraoperative blood loss are indicators for intensive monitoring and intervention. These might include nutritional adjustments, optimization of physical therapy regimens, and stricter hematological surveillance to promote healing and mitigate the risk of nonunion. Moreover, CCD can be directly modified during the operation. Understanding the role of CCD in nonunion provides actionable insights for preoperative planning. When the CCD is significantly increased by analyzing radiological images, it suggests a potential reevaluation of surgical techniques to ensure optimal alignment and stability.
Enhancing External Validity
Acknowledging the high 3-month nonunion rate observed in our study, finally 6 cases had bone nonunion after extended follow-up and underwent secondary surgery. We are undertaking collaborative studies to validate these findings across multiple centers with varied 3-month nonunion incidences. This initiative will help determine whether the identified predictors hold universally or if their influence is context-specific. Such validation is crucial for enhancing the robustness and applicability of our predictive model in global clinical settings.
Limitations
This study is subject to certain limitations that warrant consideration in subsequent research. Firstly, the predictive model did not include functional outcomes, as another important indicator of delayed nonunion, besides radiological signs of nonunion. Secondly, similar to numerous retrospective analyses, our model’s efficacy requires prospective validation. Thirdly, prediction model was not developed based on 6 patients with final bone nonunion. Fourthly, the dataset for this research was sourced from single medical institution, which may not provide as comprehensive a perspective as a multicenter study would. Although external validation data were utilized, these originated from the same institution too, lacking validation cohorts from diverse regions and nations. Subsequently, additional datasets and prospective multicenter clinical trials are essential to confirm the reliability of our findings and model.
Conclusion
In summary, our retrospective analysis demonstrates that ML-particularly the CatBoost model-can effectively predict 3-month nonunion in patients with unstable distal clavicle fractures treated with ORIF. Key predictors identified (CCD, HDL levels, and intraoperative blood loss) offer actionable insights that can inform intraoperative adjustments and postoperative management. Integrating these predictive models into clinical practice could potentially reduce nonunion rates and improve patient outcomes by enabling more personalized treatment strategies.
Data Sharing Statement
The raw data can be obtained upon request from the Department of Orthopedics, Nanjing Luhe People’s Hospital. All data used in this study were contributed by Changke Ma.
Ethical Approval
Ethical approval for this study was obtained from the Nanjing Luhe People’s Hospital, Nanjing, China (Number LHLL2022024). Because of the retrospective study, the requirement for informed consent was waived. The research content conforms to the requirements of the Declaration of Helsinki.
Acknowledgments
This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-4280633/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (Grant Number 82173899), Nanjing Medical Science and Technical Development Foundation (Grant Number YKK23237), Jiangsu Pharmaceutical Association (Grant Number H202108, A2021024, Q202202, JY202207, A202309, Z04JKM2023E040), Open project of International Joint Laboratory of Recombinant Drug Protein Expression System in Henan Province (No.KFKTYB202208).
Disclosure
The authors have no potential conflicts of interest to disclose for this work.
References
1. Panagopoulos A, Tatani I, Kattou C, et al. Clinical and radiological outcomes of closed-loop, double button, coracoclavicular fixation for extralateral (Neer Type IIC) fractures of the distal clavicle. Cureus. 2022;14(5):e25228. doi:10.7759/cureus.25228
2. Xiong J, Chen J-H, Dang Y, et al. Treatment of unstable distal clavicle fractures (Neer type II): a comparison of three internal fixation methods. J Int Med Res. 2018;46(11):4678–4683. doi:10.1177/0300060518788245
3. Singh A, Schultzel M, Fleming JF, et al. Complications after surgical treatment of distal clavicle fractures. Orthop Traumatol Surg Res. 2019;105(5):853–859. doi:10.1016/j.otsr.2019.03.012
4. Uittenbogaard SJ, van Es LJ, den Haan C, et al. Outcomes, union rate, and complications after operative and nonoperative treatments of Neer type II distal clavicle fractures: a systematic review and meta-analysis of 2284 patients. Am J Sports Med. 2023;51(2):534–544. doi:10.1177/03635465211053336
5. Li D, Qiao R, Yang N, et al. Clinical analysis of the acromial height-measuring device combined with new-type clavicular hook plate and standard clavicular hook plate in the treatment of Neer type II distal clavicle fractures. J Orthop Surg Res. 2022;17(1):448. doi:10.1186/s13018-022-03338-4
6. Chen MJ, DeBaun MR, Salazar BP, et al. Hook versus locking plate fixation for Neer type-II and type-V distal clavicle fractures: a retrospective cohort study. Eur J Orthop Surg Traumatol. 2020;30(6):1027–1031. doi:10.1007/s00590-020-02658-7
7. Stegeman SA, Nacak H, Huvenaars KH, et al. Surgical treatment of Neer type-II fractures of the distal clavicle: a meta-analysis. Acta Orthop. 2013;84(2):184–190. doi:10.3109/17453674.2013.786637
8. Lopiz Y, Checa P, García-Fernández C, et al. Complications with the clavicle hook plate after fixation of Neer type II clavicle fractures. Int Orthop. 2019;43(7):1701–1708. doi:10.1007/s00264-018-4108-3
9. Hak DJ, Fitzpatrick D, Bishop JA, et al. Delayed union and nonunions: epidemiology, clinical issues, and financial aspects. Injury. 2014;45:S3–7. doi:10.1016/j.injury.2014.04.002
10. Zhu Y, Hu J, Zhan T, et al. Refracture after plate removal of midshaft clavicle fractures after bone union—incidence, risk factors, management and outcomes. BMC Musculoskelet Disord. 2023;24(1):308. doi:10.1186/s12891-023-06391-0
11. Kamal H, Lopez V, Sheth S. Machine learning in acute ischemic stroke neuroimaging. Front Neurol. 2018;9:945. doi:10.3389/fneur.2018.00945
12. Xiong W, Chen T, Li J, et al. Interpretable machine learning model to predict rupture of small intracranial aneurysms and facilitate clinical decision. Neurol Sci. 2022;43(11):6371–6379. doi:10.1007/s10072-022-06351-x
13. Hu Y, Yang T, Zhang J, et al. Dynamic prediction of mechanical thrombectomy outcome for acute ischemic stroke patients using machine learning. Brain Sci. 2022;12(7):938. doi:10.3390/brainsci12070938
14. Desautels T, Das R, Calvert J, et al. Prediction of early unplanned intensive care unit readmission in a UK tertiary care hospital: a cross-sectional machine learning approach. BMJ Open. 2017;7(9):e017199. doi:10.1136/bmjopen-2017-017199
15. Lin X, Zheng X, Zhang J, et al. Machine learning to predict futile recanalization of large vessel occlusion before and after endovascular thrombectomy. Front Neurol. 2024;15:1499029. doi:10.3389/fneur.2024.1499029
16. Quesada JA, Lopez‐Pineda A, Gil‐Guillén VF, et al. Machine learning to predict cardiovascular risk. Int J Clin Pract. 2019;73(10):e13389. doi:10.1111/ijcp.13389
17. Zhang Z, Mo L, Huang C, et al. Binary logistic regression modeling with TensorFlow™. Ann Transl Med. 2019;7(20):591. doi:10.21037/atm.2019.09.125
18. Wang Q, Yu S, Qi X, et al. Overview of logistic regression model analysis and application. Zhonghua Yu Fang Yi Xue Za Zhi. 2019;53(9):955–960. doi:10.3760/cma.j.issn.0253-9624.2019.09.018
19. Pellagatti M, Masci C, Ieva F, et al. Generalized mixed‐effects random forest: a flexible approach to predict university student dropout. Stat Anal Data Min. 2021;14(3):241–257. doi:10.1002/sam.11505
20. Yuan K-C, Tsai L-W, Lee K-H, et al. The development an artificial intelligence algorithm for early sepsis diagnosis in the intensive care unit. Int J Med Inform. 2020;141:104176. doi:10.1016/j.ijmedinf.2020.104176
21. Chelladurai A, NarayanDL, Divakarachari PB, et al. fMRI-based Alzheimer’s disease detection using the SAS method with multi-layer perceptron network. Brain Sci. 2023;13(6):893. doi:10.3390/brainsci13060893
22. Deo RC. Machine learning in medicine. Circulation. 2015;132(20):1920–1930. doi:10.1161/CIRCULATIONAHA.115.001593
23. Lin S, Zou Y, Hu J, et al. Development and assessment of machine learning models for predicting recurrence risk after endovascular treatment in patients with intracranial aneurysms. Neurosurg Rev. 2022;45(2):1521–1531. doi:10.1007/s10143-021-01665-4
24. Goldstein BA, Navar AM, Carter RE. Moving beyond regression techniques in cardiovascular risk prediction: applying machine learning to address analytic challenges. Eur Heart J. 2017;38(23):1805–1814. doi:10.1093/eurheartj/ehw302
25. Goto T, Jo T, Matsui H, et al. Machine learning-based prediction models for 30-day readmission after hospitalization for chronic obstructive pulmonary disease. COPD. 2019;16(5–6):338–343. doi:10.1080/15412555.2019.1688278
26. Li X, Wu M, Sun C, et al. Using machine learning to predict stroke‐associated pneumonia in Chinese acute ischaemic stroke patients. Eur J Neurol. 2020;27(12):2676. doi:10.1111/ene.14495
27. Gstettner C, Tauber M, Hitzl W, et al. Rockwood type III acromioclavicular dislocation: surgical versus conservative treatment. J Shoulder Elbow Surg. 2008;17(2):220–225. doi:10.1016/j.jse.2007.07.017
28. Qvist AH, Væsel MT, Jensen CM, et al. Minimal pain decrease between 2 and 4 weeks after nonoperative management of a displaced midshaft clavicle fracture is associated with a high risk of symptomatic nonunion. Clin Orthop Relat Res. 2021;479(1):129–138. doi:10.1097/CORR.0000000000001411
29. Nicholson JA, Clement ND, Clelland AD, et al. Displaced midshaft clavicle fracture union can be accurately predicted with a delayed assessment at 6 weeks following injury: a prospective cohort study. J Bone Joint Surg Am. 2020;102(7):557–566. doi:10.2106/JBJS.19.00955
30. Takahashi S, Terai H, Hoshino M, et al. Machine-learning-based approach for nonunion prediction following osteoporotic vertebral fractures. Eur Spine J. 2023;32(11):3788–3796. doi:10.1007/s00586-022-07431-4
31. Leister I, Haider T, Vogel M, et al. A predictive model to identify treatment-related risk factors for odontoid fracture nonunion using machine learning. Spine. 2023;48(3):164–171. doi:10.1097/BRS.0000000000004510
32. Lian J, ChanFJ, Levy BJ. Classification of distal clavicle fractures and indications for conservative treatment. Clin Sports Med. 2023;42(4):685–693. doi:10.1016/j.csm.2023.05.007
33. Oh JH, Kim SH, Lee JH, et al. Treatment of distal clavicle fracture: a systematic review of treatment modalities in 425 fractures. Arch Orthop Trauma Surg. 2011;131(4):525–533. doi:10.1007/s00402-010-1196-y
34. Robinson CM, Cairns DA. Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am. 2004;86(4):778–782. doi:10.2106/00004623-200404000-00016
35. Lee S, Bedi A. Shoulder acromioclavicular joint reconstruction options and outcomes. Curr Rev Musculoskelet Med. 2016;9(4):368–377. doi:10.1007/s12178-016-9361-8
36. Li Q, Hsueh PL, Chen YF. Coracoclavicular ligament reconstruction: a systematic review and a biomechanical study of a triple endobutton technique. Medicine. 2014;93(28):e193. doi:10.1097/MD.0000000000000193
37. Fleming MA, Dachs R, Maqungo S, et al. Angular stable fixation of displaced distal-third clavicle fractures with superior precontoured locking plates. J Shoulder Elbow Surg. 2015;24(5):700–704. doi:10.1016/j.jse.2014.09.024
38. Panagopoulos A, Solou K, Tatani I, et al. What is the optimal surgical treatment for Neer type IIB (IIC) distal clavicle fractures? A systematic review and meta-analysis. J Orthop Surg Res. 2022;17(1):215. doi:10.1186/s13018-022-03108-2
39. Balaban O, Dülgeroğlu TC, Aydın T. Ultrasound-guided combined interscalene-cervical plexus block for surgical anesthesia in clavicular fractures: a retrospective observational study. Anesthesiol Res Pract. 2018;2018:7842128. doi:10.1155/2018/7842128
40. Vandepitte C, Latmore M, O’Murchu E, et al. Combined interscalene-superficial cervical plexus blocks for surgical repair of a clavicular fracture in a 15-week pregnant woman. Int J Obstet Anesth. 2014;23(2):194–195. doi:10.1016/j.ijoa.2013.10.004
41. Fugelli CG, Westlye ET, Ersdal H, et al. Combined interscalene brachial plexus and superficial cervical plexus nerve block for midshaft clavicle surgery: a case series. AANA J. 2019;87(5):374–378.
42. Banerjee S, Acharya R, Sriramka B. Ultrasound-guided inter-scalene brachial plexus block with superficial cervical plexus block compared with general anesthesia in patients undergoing clavicular surgery: a comparative analysis. Anesth Essays Res. 2019;13(1):149–154. doi:10.4103/aer.AER_185_18
43. Albi-Feldzer A, Dureau S, Ghimouz A, et al. Preoperative paravertebral block and chronic pain after breast cancer surgery: a double-blind randomized trial. Anesthesiology. 2021;135(6):1091–1103. doi:10.1097/ALN.0000000000003989
44. Beletsky A, Burton BN, Swisher MW, et al. Utilization of regional anesthesia for open reduction and internal fixation of clavicular fractures is associated with increased same-day discharge and not readmissions. Reg Anesth Pain Med. 2020;45(9):716–719. doi:10.1136/rapm-2020-101567
45. Ryan DJ, Iofin N, Furgiuele D, et al. Regional anesthesia for clavicle fracture surgery is safe and effective. J Shoulder Elbow Surg. 2021;30(7):e356–e360. doi:10.1016/j.jse.2020.10.009
46. Constantinou C, Karavia EA, Xepapadaki E, et al. Advances in high-density lipoprotein physiology: surprises, overturns, and promises. Am J Physiol Endocrinol Metab. 2016;310(1):E1–E14. doi:10.1152/ajpendo.00429.2015
47. Triantaphyllidou IE, Kalyvioti E, Karavia E, et al. Perturbations in the HDL metabolic pathway predispose to the development of osteoarthritis in mice following long-term exposure to western-type diet. Osteoarthritis Cartilage. 2013;21(2):322–330. doi:10.1016/j.joca.2012.11.003
48. Blair HC, Kalyvioti E, Papachristou NI, et al. Apolipoprotein A-1 regulates osteoblast and lipoblast precursor cells in mice. Lab Invest. 2016;96(7):763–772. doi:10.1038/labinvest.2016.51
49. Li S, Guo H, Liu Y, et al. Relationships of serum lipid profiles and bone mineral density in postmenopausal Chinese women. Clin Endocrinol. 2015;82(1):53–58. doi:10.1111/cen.12616
50. Hussain SM, Ebeling PR, Barker AL, et al. Association of plasma high-density lipoprotein cholesterol level with risk of fractures in healthy older adults. JAMA Cardiol. 2023;8(3):268–272. doi:10.1001/jamacardio.2022.5124
51. Papachristou NI, Blair HC, Kypreos KE, et al. High-density lipoprotein (HDL) metabolism and bone mass. J Endocrinol. 2017;233(2):R95–R107. doi:10.1530/JOE-16-0657
52. Lisnyansky M, Kapelushnik N, Ben-Bassat A, et al. Reduced activity of geranylgeranyl diphosphate synthase mutant is involved in bisphosphonate-induced atypical fractures. Mol Pharmacol. 2018;94(6):1391–1400. doi:10.1124/mol.118.113670
53. Chen H, Shao Z, Gao Y, et al. Are blood lipids risk factors for fracture? Integrative evidence from instrumental variable causal inference and mediation analysis using genetic data. Bone. 2020;131:115174. doi:10.1016/j.bone.2019.115174
54. Quan K, Xu Q, Zhu M, et al. Analysis of risk factors for non-union after surgery for limb fractures: a case-control study of 669 subjects. Front Surg. 2021;8:754150. doi:10.3389/fsurg.2021.754150
55. Niu P, Li H, Liu D, et al. Association between HDL-C and bone mineral density: an cross-sectional analysis. Int J Gen Med. 2021;14:8863–8872. doi:10.2147/IJGM.S334972
56. Kan B, Zhao Q, Wang L, et al. Association between lipid biomarkers and osteoporosis: a cross-sectional study. BMC Musculoskelet Disord. 2021;22(1):759. doi:10.1186/s12891-021-04643-5
57. Reed AA, Joyner CJ, Isefuku S, et al. Vascularity in a new model of atrophic nonunion. J Bone Joint Surg Br. 2003;85(4):604–610. doi:10.1302/0301-620x.85b4.12944
58. Taghinia AH. Pediatric replantation and revascularization. Hand Clin. 2019;35(2):155–178. doi:10.1016/j.hcl.2018.12.006
59. Fourman MS. CORR insights®: minimal pain decrease between 2 and 4 weeks after nonoperative management of a displaced midshaft clavicle fracture is associated with a high risk of symptomatic nonunion. Clin Orthop Relat Res. 2021;479(1):139–141. doi:10.1097/CORR.0000000000001606
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Classification and Regression Tree Predictive Model for Acute Kidney Injury in Traumatic Brain Injury Patients
Wang R, Zhang J, He M, Xu J
Therapeutics and Clinical Risk Management 2024, 20:139-149
Published Date: 22 February 2024
Machine Learning-Based Predictive Modeling of Diabetic Nephropathy in Type 2 Diabetes Using Integrated Biomarkers: A Single-Center Retrospective Study
Zhu Y, Zhang Y, Yang M, Tang N, Liu L, Wu J, Yang Y
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1987-1997
Published Date: 10 May 2024
Development and Validation of Upper Limb Lymphedema in Patients After Breast Cancer Surgery Using a Practicable Machine Learning Model: A Retrospective Cohort Study
Peng X, Lu Z
International Journal of General Medicine 2024, 17:3799-3812
Published Date: 2 September 2024
Identifying and Validating Prognostic Hyper-Inflammatory and Hypo-Inflammatory COVID-19 Clinical Phenotypes Using Machine Learning Methods
Ji X, Guo Y, Tang L, Gao C
Journal of Inflammation Research 2025, 18:3009-3024
Published Date: 27 February 2025
Machine Learning-Based Prediction Model for Multidrug-Resistant Organisms Infections: Performance Evaluation and Interpretability Analysis
Zhao W, Sun P, Li W, Shang L
Infection and Drug Resistance 2025, 18:2255-2269
Published Date: 6 May 2025