")
Back to Journals » Advances in Medical Education and Practice » Volume 15
Academic Health System Framework for Health Services Transformation: A Perspective View from West Java, Indonesia
Authors Agustian D , Arya IFD , Adnani QES , Wiwaha G , Bashari MH , Nurdiawan W , Bandiara R, Hasansulama W, Berbudi A , Nugraha GI , Permadi W, Anwar R, Afriandi I , Kartasasmita A , Hidayat YM , Achmad TH, Norcini J
Received 19 June 2024
Accepted for publication 2 September 2024
Published 11 October 2024 Volume 2024:15 Pages 957—969
DOI https://doi.org/10.2147/AMEP.S474314
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Balakrishnan Nair
Dwi Agustian,1 Insi Farisa Desy Arya,1 Qorinah Estiningtyas Sakilah Adnani,1 Guswan Wiwaha,1 Muhammad Hasan Bashari,2 Windi Nurdiawan,3 Ria Bandiara,4 Wijana Hasansulama,5 Afiat Berbudi,2 Gaga Irawan Nugraha,2 Wiryawan Permadi,3 Ruswana Anwar,3 Irvan Afriandi,1 Arief Kartasasmita,6 Yudi Mulyana Hidayat,3 Tri Hanggono Achmad,2 John Norcini7
1Department of Public Health, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 3Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 4Department of Internal Medicine, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 5Department of Otolaryngology, Head and Neck Surgery, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 6Department of Ophthalmology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 7Department of Psychiatry, SUNY Upstate Medical University, Philadelphia, PA, USA
Correspondence: Dwi Agustian, Department of Public Health, Faculty of Medicine, Universitas Padjadjaran, Jl. Prof. Eyckman No. 38, Bandung, West Java, 40161, Indonesia, Email [email protected]
Abstract: Although the field of medicine has made significant progress in recent decades, low and middle-income countries continue to face significant difficulties in addressing the unprecedented obstacles to improving health. Medical schools should play a critical role in driving health services reform and take on a new leadership role in strengthening the health system. This paper discusses a conceptual framework and outlines the Academic Health Systems (AHS) agenda in Indonesia. A comprehensive analysis was conducted on the existing literature and frameworks regarding AHS, applying the system thinking method, which engages stakeholders actively. The findings and interpretations from interviews, focus groups, and collaborative workshops were consolidated and a set of proposed frameworks, fundamental principles, and a route for enhancing the health system in Indonesia were put forward. Our recommendations include transformative learning, community engagement, and translational research as pillar principles of AHS program. These recommendations have the potential to be modified and implemented in other low- and middle-income countries.
Keywords: academic health system, medical education, Indonesia, health system reform, health services transformation
Introduction
Since 2007, the World Health Organization (WHO) has supported enhancing the health system by endorsing an action framework that enables countries to establish shared characteristics and specific benchmarks. A key factor to consider is that health programs or interventions were historically not designed based on a disease-centred strategy but instead adopted a comprehensive approach believed to yield broader, organised, and enduring effects. By adopting this approach, countries are anticipated to transition from focusing on individual diseases to implementing broader system-level interventions.1 However, the practical implementation of this technique has proven to be difficult because of the inherent characteristics of the system, which include dynamic complexity and numerous interactions and interdependencies among its components.2
The COVID-19 pandemic serves as an instance of an intricate issue that has lately caused a significant impact on the worldwide healthcare system. It has emphasised the necessity and immediacy for all nations to adopt a system-thinking approach to address complexity. This approach considers problems as interconnected components of a broader, ever-changing system.3 This strategy is broader than merely responding to current outcomes or events. It requires a more thorough examination of the connections, associations, interactions, and behaviours among the complete system’s components. As a result, this approach to thinking systematically has significant implications for the higher education sector, specifically medical schools worldwide. These institutions aim to consistently reshape their vision and revise their curriculum and learning methods to meet the evolving demands of the real world.4
The origins of Academic Health Centers (AHCs) can be traced back several decades, and their formal investigation has gained significant prominence in the United States. The Institute of Medicine (now the National Academy of Medicine) conducted a thorough investigation into this subject throughout the early 2000s, yielding crucial discoveries that continue to shape conversations and activities in healthcare systems globally. Their influential study, titled “Academic Health Centers: Leading Change in the 21st Century”, highlighted the pivotal role of AHCs in driving innovation, fostering collaboration between academics and healthcare service, and improving health outcomes through interdisciplinary approaches. This preliminary research laid the foundation for future advancements and discussions on AHCs, setting a benchmark for cutting-edge healthcare models on a worldwide scale.5
In 2010, Dzau et al introduced the idea that medical schools should take on a new leadership role within the academic community. They suggested that these institutions should actively participate in and guide the efforts to build the health system. They also proposed the term “academic health (science) system” (AHS) to further develop this notion.6 This concept is founded on the observation that while the field of medicine has made significant progress in recent decades, developing nations continue to face significant difficulties in addressing the unprecedented obstacles to improving health. These challenges include disparities in healthcare access, inconsistent quality of care, and escalating healthcare expenses resulting from the growing burden of preventable diseases. In order to have a meaningful effect, medical schools should not solely depend on the conventional approach of producing high-quality physicians to support the healthcare system. Instead, they should focus on promoting new priorities in research discovery that encompass the entire spectrum of care, ranging from community-based to advanced tertiary care. Additionally, medical schools should actively collaborate with various organizations, considering the intricate and often disjointed nature of regulations, business models, reimbursement systems, and incentive structures.
While it is commonly acknowledged that there is no universally ideal organizational model for AHS, to make significant advancements, AHS leaders are anticipated to revamp the organizational structure and promote a cultural shift that enables both the horizontal integration of healthcare model discovery and the vertical integration of the healthcare continuum. It is universally expected that AHS leaders should support a flexible system that allows them to close gaps in knowledge translation and speed up the spread of new knowledge throughout the process of discovery and care. In the end, this strategy is anticipated to uncover efficient, cost-effective, easily implementable technology and care models.
West Java, Indonesia, faces a multitude of healthcare challenges, including both infectious diseases and non-communicable diseases (NCDs).7 The intricate nature of these challenges necessitates a comprehensive and cohesive approach to healthcare provision, research, and education, aligning with the core concepts of AHS. The healthcare infrastructure in the region has been seeing significant advancements, characterized by the establishment of cutting-edge hospitals, research centres, and educational institutions. The healthcare ecosystem in West Java has a wide range of players, including government agencies, academic institutions, healthcare providers, and community organizations.8,9 The region is experiencing an increasing number of healthcare professionals, students, and researchers who are eager to make valuable contributions to the advancement of healthcare practices and regulations. The AHS framework can optimize these developments by fostering synergies between clinical care, research projects, and educational activities. AHS serves as a focal point for nurturing talent, fostering multidisciplinary education, and facilitating continuous learning and professional development for healthcare professionals.10 This will finally enhance the calibre of healthcare and its results. Integrating these diverse stakeholders into AHS can promote collaboration, information sharing, and innovation, leading to enhanced and long-lasting transformation of healthcare.
Recognizing and esteeming the cultural complexities and communal norms in West Java are essential for delivering patient-centred healthcare and promoting health equity. AHS can have a significant impact on improving healthcare services that are inclusive, fair, and tailored to the needs of the local population.10 It can be achieved by giving importance to community involvement, patient support, and culturally sensitive healthcare techniques. The unique aspects of the situation in West Java, Indonesia, offer another justification for adopting an AHS framework to support the transformation of healthcare services. The alignment between the fundamental principles of AHS and the unique requirements, possibilities, and challenges of the region underscores the strategic and influential approach to enhancing healthcare quality and tackling public health demands.
This paper presents our proposed AHS program model, which envisions a higher education institution leadership specializing in the health science field. As one of the leading medical schools in Indonesia that mandated by the Indonesian government to formulate AHS model, we would like to set our agenda to invest in a learning healthcare system.11 In addition, to run this AHS mission, we would like to elaborate transformative education,6 community engagement,12 and translational research13 model that include new methods in the multi and interdisciplinary investigation, problem-solving, knowledge acquisition, teamwork that involve not only medicine but also other health-related professions.14,15 This study aims to provide a comprehensive discourse of AHS concept and to offer our perspective on its framework and program model. In the subsequent part, we will begin by elucidating the processes and approach entailed in idea development. Next, we will engage in a comprehensive discussion of the mission and goal, conceptual framework, pillar principles (Transformative Learning, Community Engagement, Translational Research), result pathway, and action agenda that are specifically tailored to the Indonesian context. The insights gained from this analysis may have broad applicability to other nations as well.
Idea Development Process
In December 2022, a group consisting of academic members from several departments within the Faculty of Medicine, Universitas Padjadjaran, was formed to create the vision, goal, and framework model for the Academic Health System program. The roster of the committee, together with their respective areas of competence, can be obtained from Table 1.
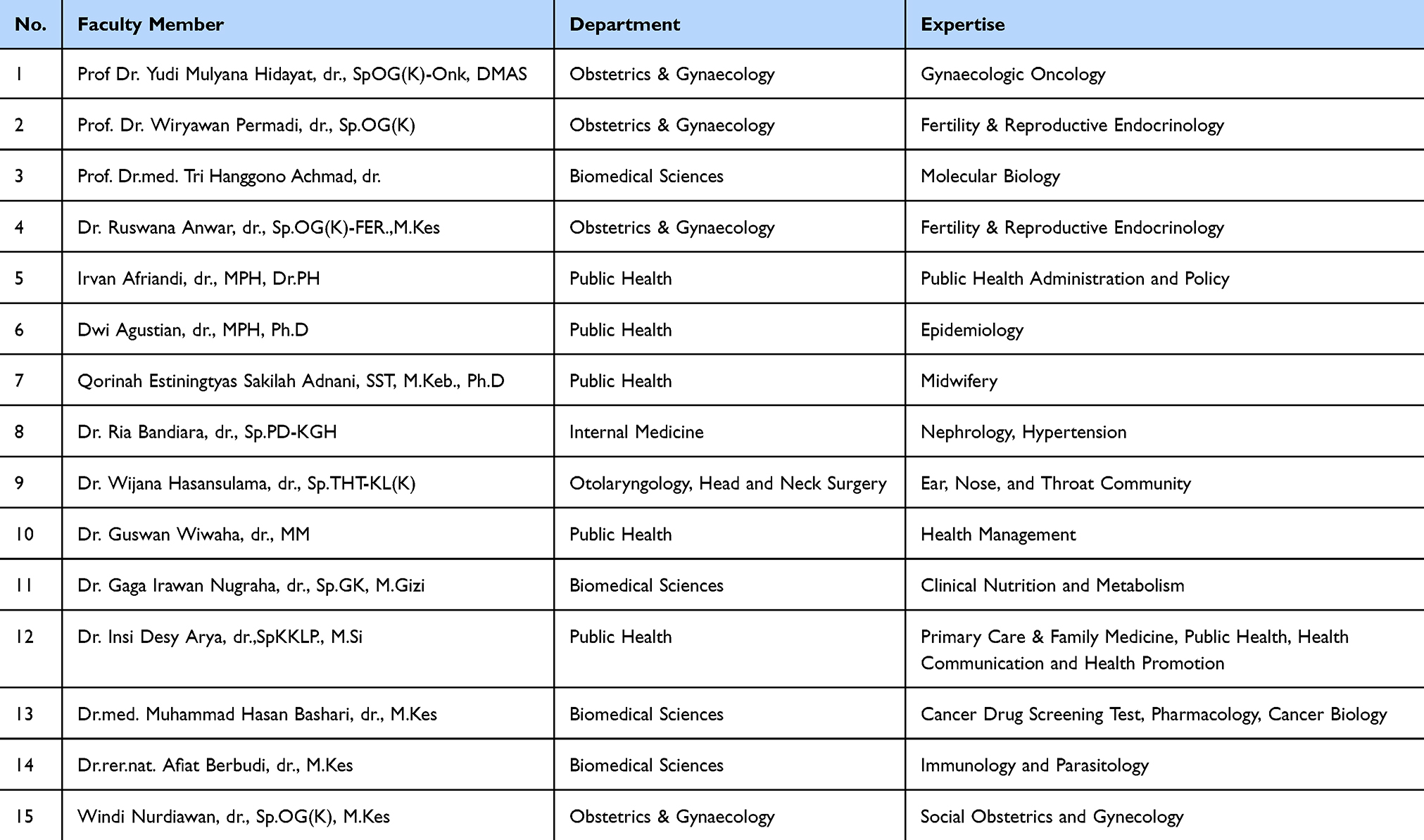 |
Table 1 Faculty of Medicine AHS Committee Member |
In order to complete the work, the committee carried out a literature review with dual objectives. The primary objectives are to establish the theoretical framework of AHS and conduct comprehensive evaluations of local and national health and higher education systems. The latter will offer contextual analysis and enhance the framework’s pertinence to the implementation in Indonesia. Our work did not follow the traditional approach of a systematic review, which normally involves a comprehensive and systematic examination. Instead, it presented an academic perspective that included a concept note and program model on AHS. These were developed based on our collective interpretation of a convenience selection of literature.
We began our work by performing a thorough review of academic health systems, healthcare reform, and relevant case studies or experiences from similar situations around the world. Throughout this stage, we acquired a profound comprehension of the theoretical principles, highly efficient methodologies, and obstacles linked to the execution of academic health system frameworks. In order to develop and assess our suggested AHS intervention model, we utilized the system thinking 10-step framework developed by De Savigny & Adam. This framework consists of four steps for Intervention Design, which include (1) Convening Stakeholders, (2) Collectively Brainstorming, (3) Conceptualizing Effects, and (4) Adapting and Re-designing. Additionally, the framework includes six steps for Evaluation Design. The process includes the following steps: (5) Identify the indicator; (6) Select the methods; (7) Choose the design; (8) Create the plan; (9) Establish the budget; and (10) Secure the funding.2 A crucial element of our first work was the active participation of stakeholders, key persons and organizations in West Java’s healthcare ecosystem, including academic institutions, healthcare providers, government agencies, and community organizations. We collected diverse perspectives, interpretations, and goals about the restructuring of healthcare services and the potential impact of AHS model through interviews, focus groups, and collaborative workshops.
Utilizing data gathered from literature research and stakeholder engagements, we conducted a comprehensive investigation into the various factors that impact healthcare services in West Java, Indonesia. This analysis encompassed a range of factors, such as demographic trends, profiles of illness burden, healthcare infrastructure, policy frameworks, cultural considerations, and socioeconomic determinants of health. We also conducted a benchmarking analysis of key performance indicators, governance structures, funding mechanisms, educational strategies, research priorities, and clinical integration strategies that are applicable to our specific situation in West Java, using global best practices and successful models of academic health systems. The benchmarking experiment provided valuable criteria for evaluating the feasibility and effectiveness of proposed initiatives in the local context. We then created an iterative framework by actively involving stakeholders in the process. By engaging in collaboration, we collectively endeavored to build and enhance the Academic Health System Framework. This framework was tailored to meet the specific requirements, difficulties, and opportunities encountered in West Java, Indonesia. This iterative process employed feedback loops, validation exercises, and consensus-building techniques to ensure the relevance, feasibility, and stakeholder support of the framework.
Once the framework was developed, we actively sought validation and input from a diverse group of experts, policymakers, and healthcare practitioners, both within our local community and on a global scale. The validation technique enhanced the identification of any shortcomings, enhanced the execution methods, and fortified the framework’s ability to withstand and adapt to different healthcare settings. In the end, we organized our approach, discoveries, and suggestions into a comprehensive academic report structure. This ensures that our work is easily understood, can be reproduced, and enables the wider dissemination of knowledge. Furthermore, it enhances the probability that individuals who have a vested interest in promoting the transformation of health services through an academic health system framework, such as stakeholders, legislators, and healthcare executives, will take into account and possibly implement our suggestions. Our paper was exempt from ethical approval as it did not involve human subjects. Instead, it relied on publicly available data from published studies and meeting notes from stakeholder and committee meetings.
Mission and Vision
The purpose of our Academic Health System program is to develop local health systems that provide exceptional care across the entire life cycle, aiming to improve the population’s health status and promote social justice. The objective is to establish interconnected healthcare systems within certain geographic regions, as depicted in Figure 1, that seamlessly interact with healthcare professionals and other health-related higher education programs within a timeframe of 2 years. Figure 1 illustrates the population and geographical aspects, depicting the spatial dimension on earth where the health system is situated and where our program will be executed.
 |
Figure 1 Population and Geographical Dimension of AHS in the Local Health System. |
Conceptual Framework
In order to accomplish the above goals and objectives, the conceptual framework comprises multiple diagrams that depict different aspects of the academic health system were constructed. These diagrams are created in the following manner: The two dimensions are the health system dimension and the excellent health service delivery dimension. Figure 2 illustrates the health system dimension, which consists of various components known as health system building blocks. These blocks include Health Care Delivery, Human Capital, Information and Communication Technology (specifically Health Information Systems), Drugs, Vaccines & Medical Technology, Economy (specifically Health Financing), and Power & Governance.
 |
Figure 2 Health System Dimension. Adapted from De Savigny D, Adam T. Systems Thinking for Health Systems Strengthening [Electronic Book]; 2009. WHO is not responsible for the content or accurracy of this adaptation.2 |
The excellent health service delivery dimension encompasses the excellent features of health care delivery that AHS aims to accomplish, as depicted in Figure 3.
 |
Figure 3 Excellent Health Service Delivery Dimension. |
To further explore the supply and demand aspect of health care, we also consider community-oriented health service, as shown in Figure 4, together with all the definitions of key essential words.
 |
Figure 4 Landscape of Community-oriented Health Service Delivery. Data from these studies.16–18 |
The primary approach of our AHS model is to effectively integrate academic agenda and activities with the local health system, either through structural or functional means. We recognized that this would be a challenging endeavour, given the large number of stakeholders (as indicated in Table 2) that need to be involved, as well as the numerous complications arising from intricate health problems and a highly fragmented local health system. However, we would want to emphasize the significance of three essential attributes, specifically transformative learning (TL),19 community engagement (CE),12 and translational research (TR),13 as pillar principles for our AHS program model implementation to achieve desirable impact amid those complexities and fragmentation.
 |
Table 2 Stakeholders List |
Pillar Principle 1: Transformative Learning
In adult learning, TL has emerged as a very compelling theory for educators, which provides a theoretical lens to view students’ learning and to lead students to become agents of change. This agent of change character is expected to be achieved by TL because it induces the process of introspection through critical reflection that leads to new ways of thinking, or illumination, which is enabled by liberating learning environments or those conducive to developing autonomous thinking and self-empowerment for reinterpreting experiences. TL is triggered by specific events, real-world problems, or conditions as the notion of a “disorienting dilemma”, which is often best facilitated through immersion in a different context, like a new place outside of the classroom. Therefore, TL can be seen as a “pedagogy of place” and “pedagogy of uncertainty”, which acknowledges the role of locale and context or place in learning that prepares the graduates for uncertainty due to new challenges or problems. The disorienting dilemma and pedagogy of place are commonly facilitated by active engagement with communities that appeared to be different to what the students knew, including visiting homes of disadvantaged or marginalised patients or families, giving community services in rural or underserved communities, providing care for end-stage live patients, or travelling abroad. In addition, TL also emphasises empathic listening, rational and reflective discourse, and an awareness of the assumptions of others, which are parts of high-level communication skills. Given these features of TL, the students are expected to develop new interpretations of how things are, including conditions within the realm of health care, with a heightened awareness of others, regardless of culture and socioeconomic standing, and of different opinions and perspectives, from the progress towards considering multiple viewpoints or multiplicity. This awareness is also expected to enhance humility, integrity, patient-centredness, empathy, and caring. In addition to having a strong cognitive dimension, the TL impact should manifest in behavioural change and even shape students to become agents of change, which in Mezirow’s theory is considered an important feature to address issues of social accountability and social justice.19 The transformed student worldview is expected to allow them to examine social injustice and health inequity and be eager to act with creativity and innovation.
Pillar Principle 2: Community Engagement
In order to achieve population health impact through our AHS approach, CE is undeniably one of the fundamental concepts necessary for the program’s success. In this context, we establish the definitions of community terminology from two distinct viewpoints. The first component is the community, which encompasses individuals impacted by the health concerns being targeted and who will ultimately benefit from the AHS program. Furthermore, we adopt a comprehensive definition of community, encompassing various stakeholders such as scholars, public health experts, politicians, non-governmental and philanthropic organizations, faith-based institutions, and local communities. Therefore, we acknowledge that each group possesses its own set of norms and culture, and that any group has the potential to assume a leadership role in engagement endeavours. The objectives of our community involvement efforts are to enhance communication, foster trust, and agreement, identify additional supporters and resources, and enhance the long-term viability of collaborations and the effectiveness of our programs. CE is based on principles of equity, impartiality, empowerment, active involvement, and autonomy. From a systemic standpoint, a community can be likened to a living body comprised of diverse cells, tissues, and organ systems, each performing distinct duties and activities, all operating within defined limits to fulfil their own requirements. In order for the community to successfully identify and address health issues, each component must efficiently fulfil its designated function while maintaining strong interconnections with the entire organism. Thus, considering the viewpoint of the health system, fostering collaboration and CE emerges as a rational strategy for enhancing population health.
Pillar Principle 3: Translational Research
In our model, one of the program pillars is translational research. The TR approach is patient and population-oriented research that integrates multidisciplinary efforts to connect the scientific evidence generation flow, from basic science research to pre-clinical research to clinical research and ultimately to implementation and health services research.13 Since all this research aims to prevent, diagnose, or treat disease, integrating the findings into practice would be challenging and should be undertaken carefully. Recognising the inadequacy in the way each practitioner tries to read and extrapolate journal articles for individual clinical decision-making, most medical societies or health professional organisations put effort into synthesising information from those journal articles, mainly from clinical trials, and formulate it into practice guidelines, which considered as a mixture of proven methods and opinion-based advice. Unfortunately, albeit most of the clinical trials are conducted in developed countries. Hence, the study populations may not represent the patients seen in real-world practice in developing countries such as Indonesia, and it would be problematic to generalise those trial findings to our local patient populations. In our AHS model, we put our effort into establishing and nurturing a network of care that connects practitioners to integrated health systems, including a collective effort to use electronic health records that generate computerised databases to capture information at the point of care. As mentioned, integrated and networked care will be established for populations in well-defined geographical areas. Population-based electronic disease registries will be established in these areas to capture continuous information about the quality of care. Further, given those registries, clinical trials will be conducted within these populations with appropriate size and relevant study cohorts, leading to the timely production of definitive-revised clinical practice guidelines. All that being said, this network will use the combination of electronic health records and disease registries aimed at capturing data about the entire course of the patient’s encounter with the healthcare systems as a fundamental infrastructure of future trials of diagnostics strategies and therapies to produce a refined and continuous learning process with the patient and relevant stakeholders’ engagement, or what so-called “learning health system” by the Institute of Medicine.11 With this TR model approach, we can bridge the gap between medical and scientific discoveries and innovations and their application in healthcare practice and public health policy to improve population health.
Outcome Pathway
The AHS committee also constructed a three years-outcome oriented program with three defined outcomes as follows: (1) Improvement of Health Care Quality and Equity; (2) Improvement of Higher Education Innovation Utilization, Evidence-Based Health Care, and Public Health Policy; and (3) Improvement of Health Literacy and Community Engagement. To achieve these ultimate outcomes, the committee also defined eight intermediate outcomes (yellow-coloured box) as represented by the logical framework and system thinking dimension visualised in Figure 5 below.
 |
Figure 5 Logical Framework and System Thinking Dimension. |
Action Agenda
We have decided to begin our leadership by first collaborating with 39 private clinics and one independent physician practice in 9 specific areas (7 Districts and 2 Cities) in Jawa Barat (West Java) Province, Indonesia, as shown in Figure 6. We will then expand this collaboration by involving local health offices, community health centres, and hospitals that are located near the catchment area of these clinics.
 |
Figure 6 Geographical Distribution of AHS Clinics Network & Implementation Areas in West Java, Indonesia. |
The primary objective of the initial implementation is to merge our research and education agenda and activities with the primary care service provided by private clinics and independent physician practice. These clinics and practice have agreed to collaborate with our institution to enhance their current service delivery and fortify the local health systems. The integration at our School revolves around the design and implementation of the medical education, research, and community services program. It originated from The Program Studi Profesi Dokter (The General Physician Study Program) in the first phase and is centred on addressing real-world problems and settings at the clinics and their population. In order to achieve this goal, specifically in relation to the medical education component, a curriculum revision initiative was undertaken, using the Kern 6-step approach to Curriculum Development in Medical Education20,21 by the Curriculum Committee comprised of faculty members assigned by The Dean. This renewed curriculum is designed to infuse the transformative learning principle into our medical education teaching practices.19
Each of the 40 primary care level facilities that agree to collaborate and join the inaugural AHS primary care network will recruit, train, and assign one newly graduated physician as a dedicated field-preceptor-practicing doctor for the program. Within these 40 local learning health system sites, a total of 212 medical students have been registered and will remain on a site for a duration of around 4–5 months and then switched to the other sites for the total period of study of 2 years. During this time, they will acquire essential skills and knowledge necessary for their future medical practice by addressing real-life challenges encountered at the individual, family, community, and local health system levels. The 40 designated AHS field doctors will act as the field preceptors for these medical students, with a preceptor to student ratio of 1:5/6. Prior to that employment, the field doctors of AHS underwent training through a series of pertinent short courses and workshops, which had a total of 1854 participant-hours. Meanwhile, we also conducted clinical research practice reform by supporting more translational research to direct the discovery and innovation toward the population health pipeline and the health care continuum in the specific context of those 40 learning health system sites. In a broader term, our AHS model is designed to improve the connection of future higher education institution activity with the community needs and to bring more population health impact to society.22
For integrating education, research, and service delivery in the field, we chose to adopt a learning health system approach23,24 and put our effort into creating the learning ecosystem laboratory at the nine areas and inviting all relevant stakeholders with the principle of CE.12 The major responsibility of the 40 field doctors is to oversee the implementation of the AHS program, with a specific focus on fostering a culture of continuous learning and expertise in the primary care setting and its surrounding environment. Faculty members with experience in relevant fields are assigned and organized into 12 Academic Clubs. This is done to speed up the learning process and ensure that our research and community service activities are in line with our AHS program framework, roadmap, and pathway. The program input, procedure, and expected outputs were depicted in a coherent framework and system thinking diagram (Figure 5) that visually represents the pathway by which our AHS model will impact the enhancement of the population’s health. In order to evaluate the overall effect of the program on the health of the population, we will measure the quality of life of the patients who are part of the primary care network, which is the main beneficiary of our AHS program. This measurement will be done at the beginning and end of the two-year program.
Strength and Limitations
Our paper is based on perspective regarding AHS by the Committee. To the best of our knowledge, this work is the inaugural published model of AHS for Indonesia. The foundation of our academic discussion and reputation surrounding the AHS concept, model, and program is rooted in the unwavering dedication of our institutional leader to spearhead the initiative, to fully include and prioritize the AHS principles inside our institutional mission and program. Nevertheless, we acknowledge the difficulties that arise from the intricate and diverse nature of health issues, the healthcare system, and its underlying factors. We recognize the need to ensure the long-term viability of our AHS model and program in order to effectively improve population health and well-being. This entails securing adequate funding, policy backing, and active engagement from the community. The viability of the AHS program is dubious. An effective strategy to address this problem is for our institution to serve as a model for the implementation of the AHS model in West Java and the Southern portion of Sumatera. This can be achieved by forming a consortium of medical schools in these areas to collaborate on the implementation of AHS. Another method, as previously indicated, is to cultivate the fundamental principles of a Learning Health System as envisaged by Menear et al.23 To enhance adaptability, we will develop the AHS program to facilitate iterative, swift adaptation and gradual evolution to fulfill the requirements of present and future stakeholders. Another instance of core principles is open innovation, wherein the AHS program will utilize knowledge from many internal and external sources and encourage collaborative methods for innovation and the exchange of ideas across organizational boundaries. The basic values of a learning health system establish the framework for the collaboration and coordination of different components within the health system, with the ultimate objective of enhancing value for individuals as a collective strategic aim.
Conclusion
The concept of the AHS aims to empower medical schools and health professional education institutions to actively enhance the strength of the healthcare system. This involves addressing various aspects such as governance, medicine and health technologies, human resources, financing, information, and service delivery to improve population health and well-being. To effectively enhance population health and well-being, it is crucial to ensure the provision of high-quality care and focus on improving the delivery of health services from both the supply side (availability, acceptability, accessibility, affordability, accommodation) and the demand side (ability to perceive, seek, reach, pay, and engage). We advocate for the implementation of these frameworks in specific geographical regions where local learning health system sites are formed and fostered based on three fundamental principles: transformative learning, community participation, and translational research. To implement the conceptual frameworks and pillar principles of AHS, it is necessary to create an outcome pathway using a system thinking method. This pathway should include the initiation of faculty development in the early phase. These difficult endeavours can be accomplished if our school administrators are enthusiastic about offering political support, financial dedication, and academic guidance to promote a fundamental change and improvement in health professional education.
Acknowledgments
The authors wish to express gratitude to the Directorate General of Higher Education, Research, and Technology, Ministry of Education, Culture, Research, and Technology, Republic of Indonesia, and the Directorate of Provision of Health Workforce, Directorate General of Health Workforce, Ministry of Health Republic of Indonesia for their leadership and support in implementing the government decree of AHS.
Disclosure
The authors report no competing interests in this work.
References
1. Adam T, de Savigny D. Systems thinking for strengthening health systems in LMICs: need for a paradigm shift. Health Policy Plan. 2012;27(suppl_4):iv1–iv3. doi:10.1093/heapol/czs084
2. De Savigny D, Adam T. Systems Thinking for Health Systems Strengthening [Electronic Book]. 2009.
3. Balqis-Ali NZ, Fun WH, Ismail M, Ng RJ, Jaaffar FSA, Low LL. Addressing gaps for health systems strengthening: a public perspective on health systems’ response towards COVID-19. Int J Environ Res Public Health. 2021;18(17):9047. doi:10.3390/ijerph18179047
4. Swanson RC, Cattaneo A, Bradley E, et al. Rethinking health systems strengthening: key systems thinking tools and strategies for transformational change. Health Policy Plan. 2012;27:iv54–iv61. doi:10.1093/heapol/czs090
5. Kohn LT. Academic Health Centers: Leading Change in the 21st Century. 2004.
6. Dzau VJ, Ackerly DC, Sutton-Wallace P, et al. The role of academic health science systems in the transformation of medicine. Lancet. 2010;375. doi:10.1016/S0140-6736(09)61082-5
7. Mboi N, Syailendrawati R, Ostroff SM, et al. The state of health in Indonesia’s provinces, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Glob Health. 2022;10(11):e1632–e1645. doi:10.1016/S2214-109X(22)00371-0
8. Gani A, Ali PB, Solikha DA, Fuady A, Sari ER. Review Dan Reformulasi Sistem Kesehatan Nasional Indonesia. Jakarta, Indonesia: Direktorat Kesehatan dan Gizi Masyarakat, Kedeputian Pembangunan Manusia, Masyarakat dan Kebudayaan, Kementerian PPN/Bappenas; 2023:6235623038.
9. Mahendradata Y, Trisnantoro L, Listyadewi S, et al. The republic of Indonesia health system review. Health Syst Transit. 2017;7(1):9789290225164.
10. Syukriani YF. Academic health system in West Java in strengthening primary health care. J Midwifery. 2021;5(1):71–80. doi:10.25077/jom.5.1.71-80.2020
11. McGinnis JM, Stuckhardt L, Saunders R, Smith M. Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. 2013.
12. CTSA. Principles of Community Engagement [Electronic Resource] / Clinical and Translational Science Awards Consortium, Community Engagement Key Function Committee, Task Force on the Principles of Community Engagement; 2011.
13. Robertson D, Williams GH. Clinical and Translational Science: Principles of Human Research. Academic Press; 2009.
14. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376(9756):1923–1958. doi:10.1016/S0140-6736(10)61854-5
15. Hamdy H. Medical college of the future: from informative to transformative. Med Teach. 2018;40(10):986–989. doi:10.1080/0142159X.2018.1498628
16. Levesque J, Harris M F and Russell G. (2013). Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity HealthInternational Journal for Equity in Health, 12(1), 18 10.1186/1475-9276-12-18
17. Penchansky R and Thomas J William. (1981). The Concept of Access. Medical Care, 19(2), 127–140. 10.1097/00005650-198102000-00001
18. Haggerty J, Levesque J, Harris M, Scott C, Dahrouge S, Lewis V, Dionne E, Stocks N and Russell G. (2020). Does healthcare inequity reflect variations in peoples’ abilities to access healthcare? Results from a multi-jurisdictional interventional study in two high-income countries. Int J Equity Health, 19(1), 10.1186/s12939-020-01281-6
19. Van Schalkwyk SC, Hafler J, Brewer TF, et al. Transformative learning as pedagogy for the health professions: a scoping review. Medical Educ. 2019;53(6):547–558. doi:10.1111/medu.13804
20. Singh MK, Gullett HL, Thomas PA. Using Kern’s 6-step approach to integrate health systems science curricula into medical education. Acad Med. 2021;96(9):1282–1290. doi:10.1097/ACM.0000000000004141
21. Thomas PA, Kern DE, Hughes MT, Chen BY. Curriculum Development for Medical Education: A Six-Step Approach. 2015.
22. Fung D. A Connected Curriculum for Higher Education. 2017.
23. Menear M, Blanchette M-A, Demers-Payette O, Roy D. A framework for value-creating learning health systems. Health Res Policy Syst. 2019;17(1):79. doi:10.1186/s12961-019-0477-3
24. Sheikh K, Abimbola S. Learning health systems: pathways to progress. Alliance Health Policy Syst Res Sci. 2021.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.