")
Back to Journals » Journal of Pain Research » Volume 18
Assessing the Causal Effect of Pulse Pressure on Migraine Risk: A Mendelian Randomization Study
Authors Xu H, Qin X, Feng Z, You S
Received 18 January 2025
Accepted for publication 31 May 2025
Published 25 June 2025 Volume 2025:18 Pages 3159—3170
DOI https://doi.org/10.2147/JPR.S512795
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Alexandre F DaSilva
Hongli Xu,1,* Xiaoyan Qin,2,* Zeguo Feng,3 Shaohua You3
1Medical Big Data Research Center, Medical Innovation Research Department of PLA General Hospital, Beijing, 100853, People’s Republic of China; 2Department of Clinical Laboratory, Shijingshan Teaching Hospital of Capital Medical University, Beijing Shijingshan Hospital, Beijing, 100049, People’s Republic of China; 3Department of Pain Medicine, The First Medical Center of Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shaohua You, Department of Pain Medicine, The First Medical Center of Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China, Email [email protected] Zeguo Feng, Department of Pain Medicine, The First Medical Center of Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China, Email [email protected]
Background: Migraine is notably prevalent among young individuals and women, who generally demonstrate favorable arterial compliance. Pulse pressure is a reliable measure of arterial compliance; nevertheless, the association between pulse pressure and migraine is not well understood.
Aim: To investigate the potential causal relationship between pulse pressure and the risk of migraine using Mendelian randomization (MR).
Methods: The pulse pressure studies mainly involved participants of European descent, while the migraine studies included individuals from various parts of the UK. The primary analysis used Inverse Variance Weighted (IVW) method, supplemented by weighted median and MR-Egger regression. Validation data came from the FinnGen study. Genes linked to pulse pressure were analyzed for Gene Ontology (GO) and KEGG enrichment using the DAVID platform.
Results: Single-nucleotide polymorphisms linked to pulse pressure were sourced from a GWAS database (810,865 individuals), while migraine data came from UK Biobank (13,971 cases, 470,627 controls). The IVW method showed an OR of 0.992 [95% confidence interval (CI), 0.987– 0.997; p = 0.002]. Both weighted median (OR 0.988; 95% CI, 0.982– 0.994; p < 0.001) and MR-Egger (OR 0.985; 95% CI, 0.972– 0.997; p = 0.016) analyses confirmed a negative causal link between pulse pressure and migraine risk. The MR-Egger intercept analysis showed minimal evidence of horizontal pleiotropy (b = 0.00013, SE = 0.00010, p = 0.209). Finnish data confirmed a causal link between migraine and pulse pressure, with the IVW method indicating a significant association (OR = 0.790, 95% CI: 0.676– 0.922; p = 0.003). KEGG enrichment analysis revealed significant pathways regulating pulse pressure, many related to cardiovascular disease and type 2 diabetes.
Conclusion: MR analysis showed that pulse pressure causally affects migraines, potentially explaining why young people and women experience more migraines, while those with type 2 diabetes have a lower risk. Further research is needed to understand this relationship.
Keywords: migraine, pulse pressure, gwas, causal association, Mendelian randomization
Graphical Abstract:

Introduction
Migraine is a recurrent neurovascular disorder.1 It affects an estimated 15% of the worldwide population.2 Migraine attacks primarily impact individuals in the young and middle-aged demographic, with a significantly higher prevalence noted among females.3 The prevalence of migraine is 2 to 3 times greater in women of childbearing age compared to men.4 The complex physiopathology of migraine adds to its burden. Several peripheral and central mechanisms are involved in migraine physiopathology, such as peripheral and central sensitization, lack of habituation, thalamo - cortical dysrhythmia, and hyperexcitability of the motor cortex.5 Migraine also presents various comorbidities. These comorbidities can significantly influence the course and management of migraine. Moreover, sex differences play a crucial role not only in the prevalence of migraine but also in the manifestation of comorbidities. Females may experience different types of comorbidities and show distinct responses to treatment compared to males.6
Pulse pressure, the difference between systolic and diastolic blood pressure, indicates arterial endothelial function, elasticity, compliance, and cardiovascular aging.7 Pulse pressure increases with age, and compared to males, females generally exhibit more pronounced changes in pulse pressure levels during middle age.8 Vascular changes in migraine patients are considered important driving factors for migraine.9 However, current research on endothelial function and compliance in migraine patients yields contradictory results. Some reports suggest that migraine patients may demonstrate stronger arterial endothelial function and better compliance, while others indicate no difference in endothelial function between migraine and non-migraine individuals.10 However, a greater body of research supports endothelial dysfunction and reduced elasticity in the arterial system of migraine patients.11–13 However, this perspective fails to account for why migraines typically manifest in early adulthood, a period characterized by generally good arterial wall elasticity and minimal compliance reduction.14,15 It also fails to elucidate why migraines are more prevalent in females during both young and middle adulthood, despite females often exhibiting superior vascular elasticity and compliance during these life stages compared to males.16–18 Regarding the above paradoxes surrounding migraine, in 2020, Al-Hassany et al contributed a review titled “Giving Researchers a Headache - Sex and Gender Differences in Migraine”, specifically discussing the paradoxes regarding sex and vascular function in migraine patients and emphasizing the importance of such research for migraine diagnosis and treatment.19 In 2024, Duan et al discovered potential protective effects of migraine against coronary artery disease and ischemic stroke.20 Al-Hassany et al emphasized the necessity of conducting more in-depth research into the mechanisms of migraine and vascular processes to address this phenomenon.19 Based on the above background, it is evident that the academic community lacks a clear understanding of the causal relationship between pulse pressure and migraine risk. This is especially the case when considering the complex interplay of gender differences, migraine comorbidities, and the paradoxes present in studies of vascular function related to migraine.
The MR determines causal links between exposures and outcomes by using genetic variations that are inherited at conception and not influenced by external factors.21 Recent genome-wide association studies (GWAS) have uncovered numerous genetic loci associated with pulse pressure in individuals of European ancestry,22 which supports the primary objective of this study. In this study, we will utilize relevant data from individuals of European ancestry from the UK Biobank and FinnGen. By applying MR, we aim to validate the hypothesis proposed in this research, that is, an increase in pulse pressure reduces the risk of migraine, thus providing new insights into the pathogenesis and treatment strategies of migraine.
Methods
Study Design
MR analysis relies on three fundamental assumptions, to reduce bias in research results: 1. Relevance Assumption: The instrumental variable (IV) selected should have a strong correlation with the exposure. 2. Independence Assumption: The IVs must be free from any confounding factors in the relationship between exposure and outcome. 3. Exclusion Restriction Assumption: Exposure to IVs should be the only way the IVs affect the outcome.23 The fundamental principles underlying MR analysis for exploring the causal impact of pulse pressure on migraine are illustrated in Figure 1. To enhance the credibility of our findings, apart from utilizing the discovery dataset for research exploration, we conducted result validation using a separate validation dataset. As the genetic nature of migraine and the relationship between migraine patients and the occurrence of cardiovascular diseases are not fully understood,24 an analysis of reverse causal relationships was conducted using MR. Subsequently, we explored the underlying mechanisms behind pulse pressure and migraine by using GO and KEGG enrichment analysis. The study design is depicted in Figure 2.
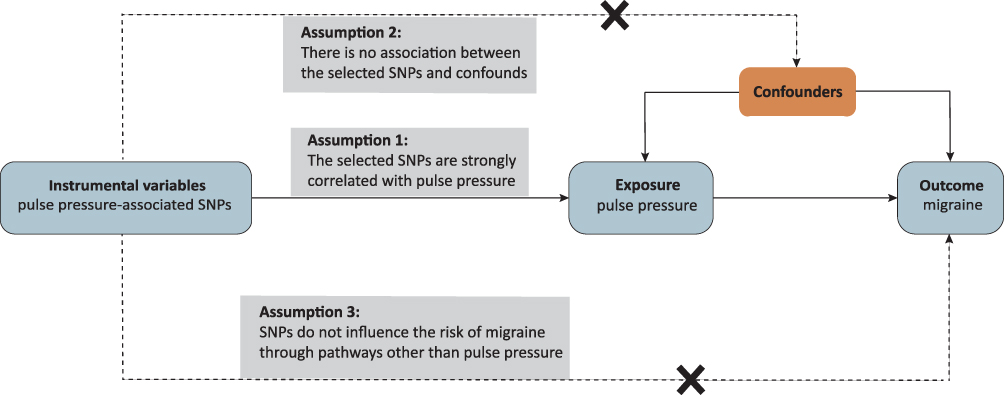 |
Figure 1 MR analysis was utilized to explore the causal impact of pulse pressure on migraine. Abbreviation: SNP, single nucleotide polymorphisms. |
 |
Figure 2 Study Design. Abbreviations: GWAS, genome-wide association studies; ID, identification; UK, United Kingdom; LD, linkage disequilibrium; MAF, minor allele frequency; GO, gene ontology; KEGG, Kyoto encyclopedia of genes and genomes; SNP, single nucleotide polymorphisms; MR, Mendelian randomization. |
Data Sources and Study Participants
The genetic correlation and two-sample MR studies were conducted from September to October 2024. We included GWAS data sources with maximum and most recent sample sizes available. These sources included information on pulse pressure participants from 810,865 European ancestry individuals from four collaborative groups (CHARGE, CHD Exome+, GoT2D:T2DGenes, ExomeBP) and the UK Biobank (UKBB). Among these 810,865 individuals, 445,360 European individuals were from the UKBB. The pulse pressure database contained a total of 240,694 single nucleotide polymorphisms (SNPs) (GWAS ID: ebi-a-GCST90000065).22 As reported by Surendran et al, pulse pressure was defined as systolic pressure minus diastolic pressure, utilizing mean values of measured values. For those known to be on antihypertensive therapy, augment their initial systolic blood pressure by 15 mmHg and their diastolic blood pressure by 10 mmHg to derive medication-adjusted pulse pressure values. The migraine datasets consist of a discovery dataset and a validation dataset. The discovery dataset is sourced from the UK Biobank (GWAS ID: ebi-a-GCST90038646), comprising 13,971 migraine cases and 470,627 controls, all from various regions of the UK, with results from association analysis of 9,587,836 SNPs. The validation dataset is derived from the FinnGen study (GWAS ID: FINN-B-MIGRAINE_TRIPTAN), including 19,676 migraine cases and 199,116 controls, along with association analysis results of 16,380,466 SNPs. This study was approved by the Ethics Committee of the First Medical Center (approval number: S2025-228-01), PLA General Hospital.
Instrumental Variable Selection
To enhance the precision and dependability of the study outcomes, a stringent SNP selection protocol was employed. Specifically, SNPs demonstrating genome-wide significant associations (p < 5×10−8) with the exposure were selected, whereas those showing high linkage disequilibrium, (r2 < 0.001, with a window size of 10,000 kb) were excluded from the analysis. The confounding factors were identified utilizing PhenoScanner (http://www.phenoscanner.medschl.cam.ac.uk/phenoscanner). The palindrome SNPs were retained based on the MAF < 0.3. MR-PRESO is capable of detecting outliers in IVW linear regression and removing them. To assess the robustness of the association between IVs and exposure, and to mitigate the potential influence of weak IVs, the F-statistic was employed. IVs exhibiting an F < 10 were excluded to reduce the effects of genetic confounding or measurement errors.25
Statistical Analysis
This study employs bidirectional two-sample MR analysis to explore the potential causal relationship between pulse pressure and migraine risk. The primary analytical method employed was the IVW approach,26 supplemented by the weighted median and Mendelian randomization-Egger (MR-Egger) regression techniques. The IVW method exhibits robust statistical power; however, it is susceptible to horizontal pleiotropy, posing challenges in fulfilling the three fundamental assumptions of MR.27 Therefore, we further employed the Weighted Median approach, under the premise that as long as at least half of the instruments utilized in the MR analysis are valid, the weighted median estimator remains applicable even with invalid instruments.28 We also employed MR-Egger, a method that remains applicable even in scenarios where all SNPs originate from invalid instruments.29 Significance was deemed to be attained when p < 0.05 was demonstrated.
To assess heterogeneity across estimates derived from individual genetic variants, the Cochran’s Q test (CQT) was used.30 An IVW random effects model was utilized instead of a fixed effects model when significant heterogeneity was detected.31 MR analyses were conducted using a variety of methodologies to assess the effect of horizontal pleiotropy. Initially, the intercept value was determined using MR-Egger intercept analysis. Subsequently, the MR-PRESSO test was utilized to identify and eliminate outliers potentially influenced by horizontal genetic pleiotropy, thereby enhancing the reliability of the MR analysis. Additionally, leave-one-out (LOO) analyses were conducted to assess the individual impact or bias of each SNP on the collective estimate. The MR analyses and associated tests were carried out using the “MRPRESSO” and “TwoSampleMR” packages within the R software environment, specifically version 4.2.2. (The R Project for Statistical Computing, Vienna, Austria).
Pathway and Functional Enrichment Analyses
To explore the potential mechanisms linking pulse pressure difference and migraine, the National Center for Biotechnology Information SNP database (https://www.ncbi.nlm.nih.gov/snp) was employed to find genes associated with the SNPs included in the MR analysis. In this study, we used the DAVID web tool (https://david.ncifcrf.gov/tools.jsp) to analyze Gene Ontology (GO) functional annotation and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment. The GO terms or KEGG pathways meeting the Bonferroni correction-corrected p≤ 0.05 were considered significantly enriched.
Result
Causal Effect of Pulse Pressure on Migraine Risk from MR Analysis
We identified 190 SNPs closely associated with abnormal pulse pressure. Adhering to the SNP screening criteria outlined above, we identified a total of 187 instruments within the UK Biobank dataset. After excluding two SNPs (rs1229984,32 rs934937933) that violated the third assumption, 185 SNPs remained. Utilizing migraine discovery data from the UK Biobank, we applied MR-PRESSO to detect five outlier SNPs (rs2895811, rs4926, rs72932557, rs9373985, and rs9982601), which were subsequently removed from the analysis. As a result, these 180 SNPs were employed as IV for the MR analysis. In Supplementary Table 1, comprehensive details are provided about these SNPs.
According to CQT, there is substantial heterogeneity among the instruments, which is illustrated by the Q statistic of 300.86 (p = 3.138e-8). Consequently, we performed a MR analysis employing an IVW random effects model. Supplementary Figure 1 and Supplementary Table 2 present the forest plot illustrating the causal effect of each SNP on migraine risk, accompanied by detailed results. The IVW method showed a statistically significant causal association between pulse pressure and migraine risk, with an odds ratio (OR) of 0.992 [95% confidence interval (CI), 0.987–0.997; p = 0.00086]. The weighted median analysis produced an OR of 0.988 (95% CI, 0.982–0.994; p = 0.0002), while MR-Egger analysis indicated an OR of 0.984 (95% CI, 0.973–0.995; p = 0.005). Collectively, these results suggest a negative causal relationship between pulse pressure and migraine risk, as depicted in Figure 3 and detailed in Supplementary Table 3. Figure 4 presents the scatter plot, funnel plot, and kernel density plot derived from the MR analysis. Utilizing the primary analytical approach, namely IVW analysis, it can be inferred that each 1 mmHg increment in genetically determined pulse pressure is associated with a 0.8% reduction in migraine risk. The MR-Egger intercept analysis suggests a minimal probability of horizontal pleiotropy, as evidenced by a b intercept value of 0.00015, a standard error of 0.000091, and a p value of 0.1065. Additionally, sensitivity analyses employing the LOO method produced consistent results, thereby bolstering the reliability of our findings (Supplementary Table 4).
 |
Figure 3 Forest plot of Mendelian randomization analysis between pulse pressure and migraine risk in the UK Biobank dataset. Abbreviations: OR, odds ratio; CI, confidence intervals; MR, Mendelian randomization. |
 |
Figure 4 The Scatter Plot, Funnel Plot, and Kernel Density Plot of MR Analysis Between Genetically Predicted Pulse Pressure and Migraine Risk in the UK Biobank dataset. (A) Scatter plot for the causal effect of pulse pressure on migraine risk. (B) Funnel plot for the overall heterogeneity in the effect of pulse pressure on migraine risk. (C) The kernel density plot for each SNP in MR analysis. Abbreviations: SNP, single nucleotide polymorphisms; MR, Mendelian randomization; SE, standard error; IV, instrumental variables. |
It is important to acknowledge that there is an overlap between the pulse pressure and migraine datasets used in this study from the UK Biobank. To assess the potential impact of this overlap on our findings, we utilized an online assessment application (https://sb452.shinyapps.io/overlap/) to determine that the bias attributed to sample overlap did not exceed 0.004, and that the Type I error rate remained below 0.05. Furthermore, the minimum F-statistic for these SNPs was 29.81, with an average of 81.61, suggesting that the likelihood of bias due to weak instruments is minimal.
Reverse Mendelian Randomization Analysis
In the reverse MR analysis, employing the migraine discovery dataset from the UK Biobank, we identified four SNPs significantly associated with migraine risk. Following the exclusion of one SNP (rs9349379) due to a violation of the third assumption, three SNPs (rs11172113, rs12295710, rs6738979) remained for subsequent MR analysis. These analyses appear to be robust against weak instrument bias, as evidenced by the F-statistics (Supplementary Table 5). For a comprehensive analysis of these SNPs, please consult Supplementary Table 6. The IVW method identified a statistically significant causal association between migraine and pulse pressure, with an OR of 0.138 (95% CI: 0.038–0.499; p = 0.003). The weighted median analysis produced an OR of 0.181 (95% CI: 0.082–0.398; p = 0.00002), whereas the MR-Egger analysis indicated an OR of 0.009 (95% CI: 0.00013–0.658; p = 0.277). CQT showed significant heterogeneity among the instruments, yielding a Q statistic of 9.72 (p = 0.008). LOO sensitivity test examining the impact of migraine on pulse pressure is detailed in Supplementary Table 7, which provides comprehensive data. Furthermore, the pleiotropy assessment conducted via the MR-Egger intercept analysis demonstrated a minimal probability of pleiotropy (intercept b = 0.009; standard error = 0.007; p = 0.420).
Validation of the Causal Relationship Between Migraine and Pulse Pressure
We identified 190 SNPs closely associated with abnormal pulse pressure. Utilizing the specified SNP screening criteria, we identified 186 instruments within the Finnish dataset. Following the exclusion of two SNPs (rs9349379, rs1229984) that did not satisfy the third assumption, 184 SNPs remained. In the analysis of migraine-related data from Finland, we employed MR-PRESSO to detect and exclude two outlier SNPs (rs9373985, rs4074536). The analysis proceeded with the remaining 182 SNPs, which served as IVs in the MR analysis. Comprehensive details regarding these 182 SNPs can be found in Supplementary Table 8. A Q statistic of 272.99 (p = 1.167e−5) indicated significant heterogeneity among the IVs according to CQT. Subsequently, we performed a MR analysis utilizing the IVW random-effects model. Detailed results, including the forest plot illustrating the causal effect of each SNP on migraine risk, are presented in Supplementary Figure 2 and Supplementary Table 9. The IVW approach identified a statistically significant causal association between pulse pressure and migraine risk, with an OR of 0.790, 95% CI: 0.676–0.922; p = 0.003). The weighted median analysis produced an OR of 0.835 (95% CI: 0.686–1.020, p = 0.073), while the MR-Egger analysis indicated an OR of 0.742 (95% CI: 0.509–1.082, p = 0.123). The detailed data for these results are provided in Supplementary Table 10. The MR-Egger intercept analysis indicated a minimal probability of horizontal pleiotropy, evidenced by an intercept b value of 0.001, a standard error of 0.003, and a P-value of 0.725. Moreover, sensitivity analysis employing the “leave-one-out” method yielded consistent outcomes, thereby reinforcing the robustness of our findings (refer to Supplementary Table 11). Additionally, the minimum F-statistic for these SNPs was 29.81, with an average of 81.17, suggesting that the influence of weak instruments on our results is likely negligible.
In the reverse MR analysis conducted using the migraine discovery dataset from Finland, we identified three SNPs—rs10187654, rs11172113, and rs9349379—that exhibited significant associations with migraine risk. Upon excluding the SNP rs9349379 due to its violation of the third assumption, two SNPs, rs11172113 and rs10187654, remained for subsequent MR analysis. The F-statistics for these SNPs were 64.80 and 33.01, respectively. For a comprehensive overview of the analysis results pertaining to these SNPs, please refer to Supplementary Table 12. Utilizing only two IVs, our fixed-effect IVW analysis demonstrated a significant causal association between migraine and pulse pressure (OR: 0.920, 95% CI:0.898–0.943; p =2.34 e-11).
Gene-Set Enrichment Analyses
A total of 160 candidate genes were identified from the 182 SNPs included in the MR analysis, as reported on the NCBI SNP database. These genes are located on various chromosomes throughout the genome. Through the online platform https://www.bioinformatics.com.cn/, GO enrichment analysis and KEGG analysis were performed on the 160 identified genes. GO enrichment analysis categorizes these genes into molecular function, cellular component, and biological process, aiming to further understand their associated functionalities. The results indicate that in terms of cellular components, the genes are primarily enriched in GO: Golgi apparatus, Z disc, microvillus, extracellular matrix, lateral plasma membrane, stress fiber. Regarding molecular functions, these genes are mainly associated with actin binding, protein binding, actin filament binding. In terms of biological processes, the genes are primarily related to regulation of fatty acid metabolic process, cardiac muscle contraction, embryonic skeletal system morphogenesis, sarcomere organization, positive regulation of transcription, DNA-templated, positive regulation of nuclear-transcribed mRNA poly (A) tail shortening, methylation (Refer to Supplementary Figure 3 and Supplementary Tables 13–15 for details). The KEGG analysis aims to elucidate the signaling pathways involved within these genes. The KEGG enrichment pathway analysis reveals significant enrichment of these genes in pathways such as hypertrophic cardiomyopathy, aldosterone synthesis and secretion, cGMP-PKG signaling pathway, insulin resistance, dilated cardiomyopathy, alcoholic liver disease, adrenergic signaling in cardiomyocytes, cardiac muscle contraction, type 2 diabetes mellitus (Refer to Figure 5 and Supplementary Table 16 for details).
 |
Figure 5 The Sankey and Bubble plot illustrating KEGG analysis. The Sankey diagram only displays the KEGG analysis results with a significance level of P < 0.05. Abbreviation: KEGG, Kyoto Encyclopedia of Genes and Genomes. |
Discussion
In our study, MR analysis was used to investigate the causal relationship between pulse pressure levels and migraine risk. The MR analysis unveiled a noteworthy finding: there is a negative causal relationship between pulse pressure and migraine risk, with each 1 mmHg increase in pulse pressure associated with a 0.8% reduction in migraine risk. The tests for horizontal pleiotropy and sensitivity analyses further substantiated the reliability of our findings. The consistency between the MR analysis results from the Finnish and UK databases underscored the robustness of our study outcomes. Additionally, the results of GO enrichment analysis and KEGG pathway analysis highlighted the involvement of the identified genes in cardiovascular diseases and type 2 diabetes-related pathways. These findings contribute to our understanding of the potential mechanisms underlying the relationship between cardiovascular anomalies, insulin resistance, and the incidence of migraines.
Pulse pressure serves as an indicator of arterial endothelial function, elasticity, and compliance.17,34,35 Therefore, we can interpret this result as lower arterial compliance possibly being associated with a reduced risk of migraine. This interpretation is supported by consistent evidence in the literature. The highest incidence of migraine occurs in the 10–14 age group, with a subsequent decrease in risk as individuals age.14 Evidence suggests that optimal arterial elasticity is observed in healthy adolescents aged 11 to 17 years,15 with a corresponding decline in arterial compliance as age increases. A nationwide survey in the United States regarding migraine incidence indicates a significant decrease in migraine prevalence among individuals aged 60 and above in each state.36 This discovery is consistent with the overall decrease in vascular compliance seen in elderly individuals,37 offering additional evidence for the inverse correlation between vascular compliance and the occurrence of migraines. Women are 2–3 times more likely than men to suffer from migraines, according to reports.16 This finding may correlate with the commonly observed higher vascular compliance in adult females compared to males,17,18 thereby offering additional support for our findings from a gender perspective. In youth and middle age, men consistently display higher systolic and diastolic blood pressure than women. However, after the age of 55, women’s blood pressure significantly increases.18 This developmental pattern of pulse pressure difference between genders with age highly coincides with the trend in migraine prevalence between genders.38–42 Our study results may provide insights into the paradoxes and contradictions regarding age and sex in migraine risk, as discussed in the articles “Cerebrovascular reactivity in subjects with migraine: Age paradox?”43 and “Giving Researchers a Headache - Sex and Gender Differences in Migraine”.19 In a 2024 MR study, it was found that migraine has a potential protective effect against coronary artery disease and ischemic stroke. In the reverse MR analysis, coronary atherosclerosis and myocardial infarction were found to have a potential protective effect against migraine. The reciprocal protective relationship in this study is mutually supportive of the findings of our current research.20 Evidently, the cardiovascular and cerebrovascular risks among migraine patients may vary due to individual differences, including genetic factors, lifestyle, and comorbidities. Future research needs to further take these individual differences into account to more accurately assess and predict the cardiovascular and cerebrovascular risks of migraine patients.44
The most commonly used animal model for migraine involves the systemic administration of nitroglycerin,45 which can induce migraine-like symptoms in both migraine patients and healthy individuals.46 Nitroglycerin, as a nitric oxide donor, is a potent vasodilator compound that significantly increases vascular compliance, thus affecting pulse pressure.47 The most revolutionary drugs in migraine treatment are the triptans, which exert a vasoconstrictive effect on dilated cerebral and meningeal vessels by stimulating 5-HT1B receptors.46 It is hypothesized that triptans achieve acute migraine treatment by increasing tension in intracranial vessels and reducing intracranial vascular compliance to normalize the pulse pressure. Recent developments in migraine drug research have been largely driven by in-depth studies on the calcitonin gene-related peptide (CGRP) pathway. Studies have shown that intravenous administration of CGRP increases the frequency of migraine-like symptom attacks,48 further emphasizing the importance of CGRP. In recent years, CGRP inhibitors have been approved for the treatment of episodic and chronic migraines.49 CGRP, a neuropeptide located in the peripheral and central nervous systems, participates in pain regulation in the trigeminal vascular system and possesses potent vasodilatory effects.49 CGRP inhibitors block cranial vascular dilation, reduce intracranial vascular compliance, and normalize the pulse pressure difference of intracranial vessels to achieve the goal of treating migraines. Multiple clinical studies have shown that propranolol is more effective than placebo in preventing migraines, and it can significantly reduce the frequency of migraine attacks.50 A meta - analysis51 investigated various medications for migraine prevention, including β - blockers. The results indicated that β - blockers such as propranolol have moderate - certainty evidence in reducing the number of monthly migraine days.52 The possible mechanism by which β - blockers prevent migraine attacks is that by blocking the β - receptors of the sympathetic nervous system, they reduce the contraction and dilation of blood vessels, thereby decreasing the likelihood of migraine attacks. For example, propranolol can regulate vascular tone and reduce excessive vascular responses, thus preventing the onset of migraines.53 The representative drugs mentioned above related to migraines, namely nitroglycerin, triptans, CGRP inhibitors, and β - blockers, all have the potential to influence the pathogenesis of migraines by affecting arterial vascular compliance. Our research findings rationalize the efficacy of the above - mentioned drugs in preventing migraine attacks or alleviating migraine symptoms by reducing vascular pulse pressure.
GO enrichment analysis and KEGG analysis have provided additional insights into the biological mechanisms underlying the observed causal association between pulse pressure and the risk of migraine. The analysis results may elucidate the potential involvement of these pathways in the pathophysiology of pulse pressure abnormalities and migraine. Specifically, these pathways encompass heart processes, contractile actin filament bundles, actin filament binding, striated muscle cell development, and myofibril assembly, among others. Our findings contribute to our understanding of the causal relationship between migraines and cardiovascular system abnormalities. Patients with migraine with aura appear to face a higher risk of cardiovascular and cerebrovascular diseases. For instance, a study discovered that patients with migraine with aura exhibited increased arterial stiffness, which could be a crucial mediating factor for cardiovascular and cerebrovascular diseases.54 Another study also indicated that there is a causal relationship between migraine with aura and coronary heart disease as well as ischemic stroke.20 The subtypes of migraine, the multiple biological pathways mentioned above, and the possible involvement of cerebral autoregulation and the trigeminal vascular system may all influence the risk of migraine onset. This is mutually corroborated with the pleiotropy of SNPs in this study. Therefore, further research is needed to explore their interaction mechanisms. Furthermore, it is intriguing to note that we also found the insulin resistance pathway may play a role in the pathophysiology of pulse pressure and migraine. This may help elucidate some of the questions raised in Gelfand et al’s commentary article “Potential Benefits of Migraine—What Is It Good For?”,55 such as the reduced risk of migraine in women with type 2 diabetes.56 Based on the results of our study, we speculate that this may be because insulin resistance leads to type 2 diabetes, which can cause and exacerbate arterial hardening,57 leading to increased pulse pressure and thus reducing the risk of migraine. As indicated in the commentary, migraine patients are more likely to have a healthier cardiovascular system.
This MR study possesses several strengths. Firstly, to our knowledge, this study is the first to investigate the relationship between pulse pressure and the risk of migraine. Secondly, the MR study design is based on three main assumptions, and different methodologies were employed to validate these assumptions. Thirdly, we utilized the largest-scale GWAS of pulse pressure and migraine to date. Fourthly, GWAS from European ancestry populations mitigated the impact of population stratification.
Certainly, our study has several limitations. Firstly, our MR analysis was exclusively based on European ancestry, thus necessitating validation of our study conclusions in other populations. Secondly, we will carefully interpret the results of the reverse causality analysis. These results need to be further validated with a larger sample size and the support of more instrumental variables. Thirdly, although it has been demonstrated that genetically elevated pulse pressure can reduce the risk of migraines, and GO enrichment and KEGG pathway analyses have been conducted, these biological mechanisms are still in the speculative stage and require further experimental validation. Fourthly, genetically elevated pulse pressure may not necessarily reflect intracranial arterial pressure, which might have a more direct causal relationship with migraine, necessitating further investigation. Fifthly, while our MR study may provide compelling evidence for the causal relationship between pulse pressure and migraine risk, it does not address the impact of pulse pressure on the severity of migraine in diagnosed patients. Sixthly, despite the numerous advantages of MR studies, they also have inherent limitations, including pleiotropy, low statistical power, bias due to sample overlap and population stratification (ie, confounding by ancestry). To detect and correct for pleiotropy, we employed a robust MR-Egger intercept method in our MR study. To enhance statistical power, we utilized the largest-scale GWAS of pulse pressure and migraine to date. To mitigate population stratification, both the pulse pressure GWAS and migraine GWAS were sourced from European ancestry populations. Despite our efforts to minimize shortcomings, some limitations may persist. Therefore, our findings warrant replication in randomized controlled trials.
Conclusions
Our MR analysis provides evidence of a causal relationship between genetically elevated pulse pressure and a reduced risk of migraine. This offers a reasonable explanation for the relatively high prevalence of migraine among young people and women, and also provides a speculative explanation for the lower risk of migraine in patients with diabetes. Further research is needed to elucidate the underlying mechanisms behind this relationship. Further research is needed to elucidate the underlying mechanisms behind this relationship. Additionally, the results of this study may provide a reference for the development of new migraine treatments. Drugs that appropriately increase pulse pressure without damaging the arterial system may play a role in the treatment of migraines.
Data Sharing Statement
No datasets were generated or analyzed during the current study.
Acknowledgments
We would like to express our gratitude to the other staff members of the First Medical Center of the PLA General Hospital.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no competing interests.
References
1. Mulder IA, Li M, de Vries T, et al. Anti-migraine calcitonin gene-related peptide receptor antagonists worsen cerebral ischemic outcome in mice. Ann Neurol. 2020;88(4):771–784. doi:10.1002/ana.25831
2. Eigenbrodt AK, Ashina H, Khan S, et al. Diagnosis and management of migraine in ten steps. Nat Rev Neurol. 2021;17(8):501–514. doi:10.1038/s41582-021-00509-5
3. Tao X, Yan Z, Meng J, et al. The efficacy and safety of atogepant for the prophylactic treatment of migraine: evidence from randomized controlled trials. J Headache Pain. 2022;23(1):19. doi:10.1186/s10194-022-01391-2
4. Vetvik KG, MacGregor EA, Lundqvist C, et al. Symptoms of premenstrual syndrome in female migraineurs with and without menstrual migraine. J Headache Pain. 2018;19(1):97. doi:10.1186/s10194-018-0931-6
5. Deodato M, Granato A, Martini M, et al. Neurophysiological and clinical outcomes in episodic migraine without aura: a cross-sectional study. J Clin Neurophysiol. 2024;41(4):388–395. doi:10.1097/WNP.0000000000001055
6. Russo A, Coppola G, Pierelli F, et al. Pain perception and migraine. Front Neurol. 2018;9:576. doi:10.3389/fneur.2018.00576
7. Podrug M, Šunjić B, Bekavac A, et al. The effects of experimental, meteorological, and physiological factors on short-term repeated pulse wave velocity measurements, and measurement difficulties: a randomized crossover study with two devices. Front Cardiovasc Med. 2022;9:993971. doi:10.3389/fcvm.2022.993971
8. Winston GJ, Palmas W, Lima J, et al. Pulse pressure and subclinical cardiovascular disease in the multi-ethnic study of atherosclerosis. Am J Hypertens. 2013;26(5):636–642. doi:10.1093/ajh/hps092
9. Andreou AP, Edvinsson L. Mechanisms of migraine as a chronic evolutive condition. J Headache Pain. 2019;20(1):117. doi:10.1186/s10194-019-1066-0
10. Steppan J, Barodka V, Berkowitz DE, et al. Vascular stiffness and increased pulse pressure in the aging cardiovascular system. Cardiol Res Pract. 2011;2011:263585. doi:10.4061/2011/263585
11. Cortese K, Tagliatti E, Gagliani MC, et al. Ultrastructural imaging reveals vascular remodeling in migraine patients. Histochem Cell Biol. 2022;157(4):459–465. doi:10.1007/s00418-021-02066-w
12. Giniatullin R, Khazipov R, van den Maagdenberg A, et al. Editorial: common and distinct mechanisms of migraine and stroke. Front Cell Neurosci. 2023;17:1171836. doi:10.3389/fncel.2023.1171836
13. Saddik SE, Dawood SN, Rabih AM, et al. Risk of stroke in migrainous women, a hidden association: a systematic review. Cureus. 2022;14(7):e27103. doi:10.7759/cureus.27103
14. Fan L, Wu Y, Wei J, et al. Global, regional, and national time trends in incidence for migraine, from 1990 to 2019: an age-period-cohort analysis for the GBD 2019. J Headache Pain. 2023;24(1):79. doi:10.1186/s10194-023-01619-9
15. Pahkala K, Laitinen TT, Heinonen OJ, et al. Association of fitness with vascular intima-media thickness and elasticity in adolescence. Pediatrics. 2013;132(1):e77–84. doi:10.1542/peds.2013-0041
16. Linde K, Rossnagel K. WITHDRAWN: propranolol for migraine prophylaxis. Cochrane Database Syst Rev. 2017;2(2):Cd003225. doi:10.1002/14651858.CD003225.pub3
17. Chung JW, Lee YS, Kim JH, et al. Reference values for the augmentation index and pulse pressure in apparently healthy Korean subjects. Korean Circ J. 2010;40(4):165–171. doi:10.4070/kcj.2010.40.4.165
18. Avolio AP, Kuznetsova T, Heyndrickx GR, et al. Arterial flow, pulse pressure and pulse wave velocity in men and women at various ages. Adv Exp Med Biol. 2018;1065:153–168.
19. Al-Hassany L, Haas J, Piccininni M, et al. Giving researchers a headache - sex and gender differences in migraine. Front Neurol. 2020;11:549038. doi:10.3389/fneur.2020.549038
20. Duan X, Du X, Zheng G, et al. Causality between migraine and cardiovascular disease: a bidirectional Mendelian randomization study. J Headache Pain. 2024;25(1):130. doi:10.1186/s10194-024-01836-w
21. Holmes MV, Ala-Korpela M, Smith GD. Mendelian randomization in cardiometabolic disease: challenges in evaluating causality. Nat Rev Cardiol. 2017;14(10):577–590. doi:10.1038/nrcardio.2017.78
22. Surendran P, Feofanova EV, Lahrouchi N, et al. Discovery of rare variants associated with blood pressure regulation through meta-analysis of 1.3 million individuals. Nat Genet. 2020;52(12):1314–1332. doi:10.1038/s41588-020-00713-x
23. Taylor M, Rode L, Bjørngaard J, et al. Is smoking heaviness causally associated with alcohol use? A Mendelian randomization study in four European cohorts. Int J Epidemiol. 2018;47(4):1098–1105. doi:10.1093/ije/dyy027
24. Rist PM, Buring JE, Cook NR, et al. Contribution of Migraine to Cardiovascular Disease Risk Prediction. J Am Coll Cardiol. 2023;81(23):2246–2254. doi:10.1016/j.jacc.2023.03.429
25. Burgess S, Thompson SG. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. 2011;40(3):755–764. doi:10.1093/ije/dyr036
26. Brumpton B, Sanderson E, Heilbron K, et al. Avoiding dynastic, assortative mating, and population stratification biases in Mendelian randomization through within-family analyses. Nat Commun. 2020;11(1):3519. doi:10.1038/s41467-020-17117-4
27. Gormley M, Dudding T, Sanderson E, et al. A multivariable Mendelian randomization analysis investigating smoking and alcohol consumption in oral and oropharyngeal cancer. Nat Commun. 2020;11(1):6071. doi:10.1038/s41467-020-19822-6
28. Mutie PM, Pomares-Millan H, Atabaki-Pasdar N, et al. An investigation of causal relationships between prediabetes and vascular complications. Nat Commun. 2020;11(1):4592. doi:10.1038/s41467-020-18386-9
29. Yang Q, Borges MC, Sanderson E, et al. Associations between insomnia and pregnancy and perinatal outcomes: evidence from mendelian randomization and multivariable regression analyses. PLoS Med. 2022;19(9):e1004090. doi:10.1371/journal.pmed.1004090
30. Bovijn J, Krebs K, Chen CY, et al. Evaluating the cardiovascular safety of sclerostin inhibition using evidence from meta-analysis of clinical trials and human genetics. Sci Transl Med. 2020;12(549). doi:10.1126/scitranslmed.aay6570
31. Censin JC, Nowak C, Cooper N, et al. Childhood adiposity and risk of type 1 diabetes: a Mendelian randomization study. PLoS Med. 2017;14(8):e1002362. doi:10.1371/journal.pmed.1002362
32. Jennings MV, Martínez-Magaña JJ, Courchesne-Krak NS, et al. A phenome-wide association and Mendelian randomisation study of alcohol use variants in a diverse cohort comprising over 3 million individuals. EBioMedicine. 2024;103:105086. doi:10.1016/j.ebiom.2024.105086
33. Kiando SR, Tucker NR, Castro-Vega LJ, et al. PHACTR1 is a genetic susceptibility locus for fibromuscular dysplasia supporting its complex genetic pattern of inheritance. PLoS Genet. 2016;12(10):e1006367. doi:10.1371/journal.pgen.1006367
34. Li Y, Lim C, Schär M, et al. Three-dimensional assessment of brain arterial compliance: technical development, comparison with aortic pulse wave velocity, and age effect. Magn Reson Med. 2021;86(4):1917–1928. doi:10.1002/mrm.28835
35. Cecelja M, Keehn L, Ye L, et al. Genetic aetiology of blood pressure relates to aortic stiffness with bi-directional causality: evidence from heritability, blood pressure polymorphisms, and Mendelian randomization. Eur Heart J. 2020;41(35):3314–3322. doi:10.1093/eurheartj/ehaa238
36. Echiverri K, Jicha GA, Smith JH. Age-related changes in headache days across the cognitive spectrum. Pain Med. 2018;19(7):1478–1484. doi:10.1093/pm/pnx193
37. Lim MA, Townsend RR. Arterial compliance in the elderly: its effect on blood pressure measurement and cardiovascular outcomes. Clin Geriatr Med. 2009;25(2):191–205. doi:10.1016/j.cger.2009.01.001
38. Lebedeva ER. Sex and age differences in migraine treatment and management strategies. Int Rev Neurobiol. 2022;164:309–347.
39. Pichler G, Martinez F, Vicente A, et al. Pulse pressure amplification and its determinants. Blood Press. 2016;25(1):21–27. doi:10.3109/08037051.2015.1090713
40. Sudershan A, Pushap AC, Younis M, et al. Neuroepidemiology study of headache in the region of Jammu of north Indian population: a cross-sectional study. Front Neurol. 2022;13:1030940. doi:10.3389/fneur.2022.1030940
41. Fila M, Pawłowska E, Blasiak J. Mitochondria in migraine pathophysiology - does epigenetics play a role? Arch Med Sci. 2019;15(4):944–956. doi:10.5114/aoms.2019.86061
42. Das SK, Sanyal K, Basu A. Study of urban community survey in India: growing trend of high prevalence of hypertension in a developing country. Int J Med Sci. 2005;2(2):70–78. doi:10.7150/ijms.2.70
43. Ornello R, Tiseo C, Pistoia F, et al. Cerebrovascular reactivity in subjects with migraine: age paradox? J Neurol Sci. 2019;398:202–203. doi:10.1016/j.jns.2019.01.040
44. Yang Q, Sun Q, Loke AY, et al. Cohort profile: migraine exposures and cardiovascular health in Hong Kong Chinese women (MECH-HK). BMJ Open. 2024;14(7):e084228. doi:10.1136/bmjopen-2024-084228
45. Demartini C, Greco R, Zanaboni AM, et al. Nitroglycerin as a comparative experimental model of migraine pain: from animal to human and back. Prog Neurobiol. 2019;177:15–32. doi:10.1016/j.pneurobio.2019.02.002
46. Akerman S, Karsan N, Bose P, et al. Nitroglycerine triggers triptan-responsive cranial allodynia and trigeminal neuronal hypersensitivity. Brain. 2019;142(1):103–119. doi:10.1093/brain/awy313
47. Liu T, Zhang M, Mukosera GT, et al. L-NAME releases nitric oxide and potentiates subsequent nitroglycerin-mediated vasodilation. Redox Biol. 2019;26:101238. doi:10.1016/j.redox.2019.101238
48. Edvinsson L. Calcitonin gene-related peptide (CGRP) is a key molecule released in acute migraine attacks-Successful translation of basic science to clinical practice. J Intern Med. 2022;292(4):575–586. doi:10.1111/joim.13506
49. Breen ID, Brumfiel CM, Patel MH, et al. Evaluation of the safety of calcitonin gene-related peptide antagonists for migraine treatment among adults with Raynaud phenomenon. JAMA Network Open. 2021;4(4):e217934. doi:10.1001/jamanetworkopen.2021.7934
50. Keerthana D, Mishra D, Chauhan MK, et al. Effect of propranolol prophylaxis on headache frequency in children with migraine without aura: a randomized, double-blind, Placebo-Controlled Trial. Indian J Pediatr. 2023;90(9):880–885. doi:10.1007/s12098-022-04279-w
51. Adeeb Sheet D, Bibani RH, Kheder AH. Comparison of the effect of propranolol combination with cinnarizine and propranolol in the prevention of acute migraine attacks. Cell Mol Biol. 2022;68(11):37–42. doi:10.14715/cmb/2022.68.11.7
52. Versijpt J, Deligianni C, Hussain M, et al. European Headache Federation (EHF) critical re-appraisal and meta-analysis of oral drugs in migraine prevention - part 4: propranolol. J Headache Pain. 2024;25(1):119. doi:10.1186/s10194-024-01826-y
53. Kalkman DN, Couturier EGM, El Bouziani A, et al. Migraine and cardiovascular disease: what cardiologists should know. Eur Heart J. 2023;44(30):2815–2828. doi:10.1093/eurheartj/ehad363
54. Can Y, Uçaroğlu can N, Akçay Ç, et al. Increased cardio-ankle vascular index values in migraine patients with aura. Angiology;2024. 33197241228043. doi:10.1177/00033197241228043
55. Gelfand AA, Loder E. Potential benefits of migraine-what is it good for? JAMA Neurol. 2019;76(3):250–251. doi:10.1001/jamaneurol.2018.3442
56. Fagherazzi G, El Fatouhi D, Fournier A, et al. Associations between migraine and type 2 diabetes in women: findings from the E3N cohort study. JAMA Neurol. 2019;76(3):257–263. doi:10.1001/jamaneurol.2018.3960
57. Jha P, Dolan LM, Khoury PR, et al. Low serum Vitamin D levels are associated with increased arterial stiffness in youth with type 2 diabetes. Diabetes Care. 2015;38(8):1551–1557. doi:10.2337/dc15-0111
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Identification of Novel Genetic Variants Associated with Insomnia and Migraine Comorbidity
An YC, Tsai CL, Liang CS, Lin YK, Lin GY, Tsai CK, Liu Y, Chen SJ, Tsai SH, Hung KS, Yang FC
Nature and Science of Sleep 2022, 14:1075-1087
Published Date: 7 June 2022
Associations Between Mean Platelet Volume and Risk of Deep Vein Thrombosis: A Mendelian Randomization Study and a Retrospective Study
Li J, Liang Y
International Journal of General Medicine 2023, 16:515-524
Published Date: 8 February 2023
IFN-γ, SCF, MIP1b and IL-16 Were Associated with Risk of Diabetic Nephropathy: A Mendelian Randomization Study
An L, Ren X, Pan Y, Gao W, Ren L, Wang J, Wang Y
Diabetes, Metabolic Syndrome and Obesity 2024, 17:851-856
Published Date: 22 February 2024
Association of Lactate with Risk of Cardiovascular Diseases: A Two-Sample Mendelian Randomization Study
Chang X, Zheng W, Zhao Y, Niku W, Deng B, Liu P, Wang Y
Vascular Health and Risk Management 2024, 20:541-551
Published Date: 6 December 2024
Mendelian Randomization Analysis Supports a Causal Relationship Between Circulating Inflammatory Proteins and Basal Cell Carcinoma
Fu ZD, Wang Y, Yan HL, Wu JH
Clinical, Cosmetic and Investigational Dermatology 2025, 18:767-779
Published Date: 31 March 2025