")
Back to Journals » Nature and Science of Sleep » Volume 16
Association Between Nocturnal Hypoxemia Parameters and Coronary Microvascular Dysfunction: A Cross-Sectional Study
Authors Feng L , Zhao X , Song J, Yang S, Xiang J, Zhang M, Tu C, Song X
Received 31 August 2024
Accepted for publication 21 December 2024
Published 28 December 2024 Volume 2024:16 Pages 2279—2288
DOI https://doi.org/10.2147/NSS.S494018
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Valentina Alfonsi
Lanxin Feng,1 Xin Zhao,1 Jianqiao Song,2 Shuwen Yang,1 Jianping Xiang,3 Min Zhang,1 Chenchen Tu,1 Xiantao Song1
1Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Sun Yat Sen University, Zhongshan School of Medicine, Guangzhou, People’s Republic of China; 3ArteryFlow Technology Co., Ltd., Hangzhou, People’s Republic of China
Correspondence: Chenchen Tu, Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, People’s Republic of China, Email [email protected]
Objective: There is a connection between obstructive sleep apnea (OSA) and coronary microvascular dysfunction (CMD), but the underlying mechanisms remain unclear. This study aims to evaluate the correlation between OSA-related nocturnal hypoxemia parameters and CMD.
Methods: This is an observational, single-center study that included patients who underwent polysomnography and coronary angiography during hospitalization. The presence of CMD was determined by angio-based index of microcirculatory resistance (AccuIMR). Categorical variables were compared using chi-square test or Fisher exact test. The t-test and Mann–Whitney U-test were used to compare normally and non-normally distributed continuous variables, respectively. Univariate and multivariable logistic regression analyses were performed to evaluate the relationship between nocturnal hypoxemia parameters and CMD.
Results: A total of 133 patients were included in this study, of whom 72 (54.14%) had evidence of CMD. Patients with CMD exhibited a higher prevalence of OSA and experienced more severe nocturnal hypoxia. After adjusting for potential confounding factors, minimum oxygen saturation (minSpO2) ≤ 90% (OR 5.89; 95% CI 1.73– 19.99; P=0.004) and the percentage of time spent with oxygen saturation below 90% (T90) ≥ 5% (OR 3.13; 95% CI 1.05– 9.38; P=0.041) were independently associated with CMD. However, no significant association was observed between apnea-hypopnea index (AHI) and CMD.
Conclusion: Parameters of nocturnal hypoxemia are associated with CMD. Hypoxemia parameters may more sensitively reflect the correlation between OSA and CMD than AHI.
Keywords: obstructive sleep apnea, coronary microvascular dysfunction, nocturnal hypoxemia, cardiology, dentistry
Introduction
Coronary microvascular dysfunction (CMD), a crucial mechanism underlying myocardial ischemia, is considered one of the leading causes of ischemic heart disease (IHD).1 CMD is prevalent in patients with cardiovascular disease risk factors and is closely associated with the risk of long-term cardiovascular adverse events in these patients.2,3 Index of microcirculatory resistance (IMR) is an invasive diagnostic method for evaluating coronary microvascular function independently of epicardial vascular stenosis and has high diagnostic specificity.4 As a novel wire-free physiological assessment method for CMD, angio-based index of IMR (AccuIMR) has high consistency with wire-based IMR and shows significant diagnostic and predictive potential.5
Obstructive sleep apnea (OSA) is a global disease in which patients often experience repeated upper airway tract collapse during sleep, characterized by repeated episodes of hypoxemia and reoxygenation.6 Increasing evidence indicates that OSA is an important risk factor for cardiovascular diseases such as IHD, hypertension, and heart failure, and is associated with increased morbidity and mortality.7,8 Previous clinical studies have shown that OSA, defined by apnea-hypopnea index (AHI), was independently associated with CMD.9,10 Nocturnal hypoxia caused by OSA may be an important cause of CMD, but the pathophysiological mechanisms linking OSA and CMD are still unclear.11 The relationship between hypoxemia parameters such as oxygen desaturation index (ODI), minimal oxygen saturation (SpO2), and mean apnea duration (MAD) with CMD remains controversial.
However, the relationship between OSA-related hypoxemia parameters, aside from AHI, and CMD has not been explored in previous clinical studies. In this study we investigated the relation between OSA and CMD determined by AccuIMR and further evaluated the association between nocturnal hypoxemia parameters and CMD.
Methods
Study Design
This study enrolled patients who underwent sleep study during their hospitalization at the Coronary Heart Disease Center of Beijing Anzhen Hospital from March 2023 to June 2024. The exclusion criteria were as follows: (1) failure to undergo coronary angiography during hospitalization; (2) predominantly central sleep apnea (≥50% central events and central AHI ≥10 events/h); (3) received continuous positive airway pressure (CPAP) treatment; (4) inability to calculate AccuIMR due to reasons such as poor image quality.
A total of 149 patients completed the sleep study, of whom 133 had complete sleep data and obtained AccuIMR. These 133 patients were included in the final analysis (Figure 1). This study was approved by the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University, and written informed consent was obtained from all patients.
 |
Figure 1 Flowchart of patient enrollment in the study. Abbreviations: AccuIMR, angio-based index of microcirculatory resistance; CAG, coronary angiography; CPAP, continuous positive airway pressure. |
Coronary Microvascular Assessment
AccuIMR was computed in a blinded manner by an independent laboratory using AccuIMR version 1.0 (ArteryFlow Technology, Hangzhou, Zhejiang, China). The specific calculation method for AccuIMR has been described previously.5
Briefly, two angiographic images from different angles were first selected to perform a three-dimensional reconstruction of the target vessel. The average blood flow velocity was then calculated using the TIMI frame count, and the fractional flow reserve (FFR) value was subsequently determined. The AccuIMR was then calculated using the following formula:

where Pa is the mean aortic pressure, L is the length of the target vessel, V is the average flow velocity, and AccuFFR is the calculated FFR value.
Figure 2 illustrates the calculation method of AccuIMR. As reported in previous studies, AccuIMR >25U is considered the critical value indicating significant microvascular dysfunction.12,13 Data were evaluated by three experienced operators, each of whom was blinded to the patients’ clinical characteristics.
 |
Figure 2 Schematic diagram of AccuIMR calculation. (A) The coronary angiogram. (B and C) Angiograms from 2 projections with automatically delineated lumen contour. (D) Lumen diameter and computed FFR (AccuFFRangio) pullback. (E) Computed AccuIMR value. Abbreviations: AccuIMR, angio-based index of microcirculatory resistance; FFR, fractional flow reserve. |
Sleep Study
All patients underwent overnight polysomnography during their hospitalization using the Alice PDx sleep diagnostic system (Philips Respironics, Murrysville, Pennsylvania, USA). The recorded signals included: pulse oximetry, nasal airflow, thoracoabdominal movement, electroencephalogram, electromyogram, electrocardiogram, and snoring episodes. The oximetry data were collected using the pulse oximeter with continuous monitoring, sampled at a frequency of 10 hz.
All sleep parameters and stages were collected and analyzed by experienced polysomnography technicians according to the American Academy of Sleep Medicine standards.14 Apnea was defined as ≥90% reduction in airflow lasting at least 10 seconds. Hypopnea was defined as ≥30% reduction in airflow lasting at least 10 seconds, accompanied by≥3% decrease in oxygen saturation from baseline. The AHI was defined as the total number of apnea and hypopnea events per hour of recorded sleep. OSA was diagnosed when AHI was ≥5 events/h and obstructive events accounted for more than 50% of all respiratory events. OSA was classified as mild with an AHI of 5–14 events/h, moderate with an AHI of 15–29 events/h, and severe with an AHI of ≥30 events/h.15
Nocturnal hypoxemia parameters primarily included the percentage of time spent with SpO2 below 90% (T90), while the ODI was the hourly frequency of oxygen desaturation ≥3% from baseline. Unlike the AHI, the optimal cutoff for T90 to classify the severity of OSA remains unclear. Some studies have used T90≥10% threshold to define significant nocturnal hypoxia.16,17 Huang et al identified T90≥5% as the optimal threshold for predicting poor cardiovascular outcomes in heart failure patients.18 A recent study by Wang et al introduced a classification system for hypoxic burden, categorizing patients as having light hypoxia (T90 <5%), mild hypoxia (T90 5–10%), or moderate to severe hypoxia (T90 >10%).19 Given that this study shares similarities with our study population, we adopted the T90 threshold standards from Wang et al’s research for our study. Other hypoxemia parameters included the mean and longest duration of hypopnea and apnea, as well as the mean and minimum SpO2.
Statistical Analysis
All statistical analyses were performed using R version 4.3.3 (R Foundation for Statistical Computing, Vienna, Austria). Sample size calculations were based on the formula appropriate for case-control observational studies. Previous research indicates that the prevalence of OSA in coronary artery disease patients is approximately 50%, while it is as high as 80% in CMD patients.10,20 Setting the two-sided significance level (Alpha) at 0.05 and the power (Beta) at 0.1, the estimated minimum sample size required for both the case and control groups was calculated to be 52 participants each. Considering a 10% dropout rate, we determined that at least 58 participants per group were necessary.
Categorical variables were described as frequency (percentage) and compared using chi-square test or Fisher exact test. Continuous variables were presented as mean±standard deviation (SD) or median with interquartile range (IQR), depending on whether the data were normally distributed. The data distribution was assessed using the Shapiro–Wilk test and Quantile-Quantile (QQ) plots. The t-test was used to compare normally distributed continuous variables, while the Mann–Whitney U-test was used for non-normally distributed continuous variables. Univariate and multivariable logistic regression analyses were used to identify independent risk factors for CMD. Logistic regression results were described as odds ratios (OR) with 95% confidence intervals (CI). A two-sided p-value <0.05 was considered statistically significant.
Results
Overall, 138 patients who completed both polysomnography and coronary angiography were included in the study. A total of 133 patients were included in the final analysis after excluding the patients for whom the microcirculatory resistance index could not be calculated. A cut-off of AccuIMR>25 was considered indicative of significant microvascular dysfunction and was used to divide the patients into two groups. Among them, 72 patients (54.14%) had at least one coronary vessel with an AccuIMR value greater than 25 and were therefore defined as having CMD. As shown in Table 1, the baseline clinical characteristics of patients with and without CMD were similar. However, a higher proportion of patients with CMD were diagnosed with OSA (63.93% vs 95.83%, P<0.001).
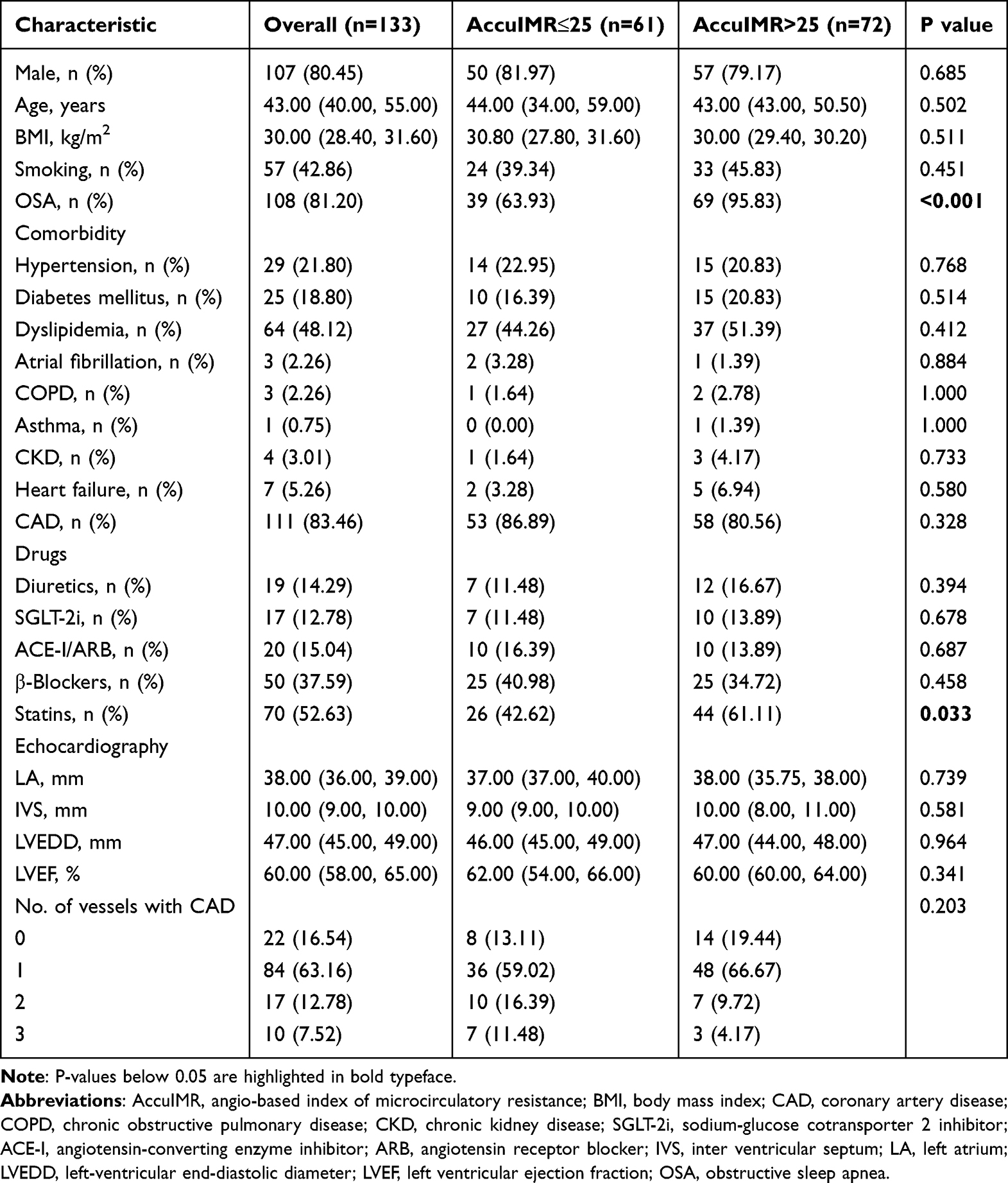 |
Table 1 Clinical Characteristics of Patients with and without Coronary Microvascular Dysfunction Defined by AccuIMR |
Table 2 summarizes the main characteristics of polysomnography among patients with different microcirculatory resistance. According to the findings, patients with CMD had a higher maximum heart rate and a lower minimum heart rate. There were significant differences in the central apnea index and mixed apnea index between the two groups. However, there were no significant differences in total sleep time, AHI, obstructive apnea index, hypopnea index and mean heart rate (P>0.05). Patients with CMD experienced more severe nocturnal hypoxia. Specifically, these patients had lower meanSpO2 (95.00% vs 93.00%, P<0.001) and minSpO2 (87.00% vs 83.00%, P=0.007), and a greater percentage of T90 (0.4% vs 9.3%, P<0.001). As illustrated in Figure 3, the proportion of patients with CMD whose minSpO2≤90% or T90≥5% is significantly higher than that of patients without CMD. There were no significant differences in ODI, mean apnea duration (MAD), longest apnea duration (LAD), mean hypopnea duration (MHD), and longest hypopnea duration (LHD) between the two groups.
 |
Table 2 Comparison of Polysomnographic Characteristics Between Groups Defined by AccuIMR |
 |
Figure 3 Comparison of the severity of hypoxemia between patients in different AccuIMR levels. The proportions of patients with (A) minSpO2≤90% (B) minSpO2≤80% (C) T90≥5% (D) T90≥10%. Abbreviations: AccuIMR, angio-based index of microcirculatory resistance; minSpO2, minimal oxygen saturation; T90, the percentage of time spent with SpO2 below 90%. |
Figure 4 presents the binary logistic regression results for CMD. Univariate analysis showed that meanSpO2, minSpO2≤90%, T90≥5%, and MaxHR may be associated with CMD. After adjusting for factors with significant differences in the univariate analysis, multivariable analysis revealed that minSpO2≤90% (OR 5.89; 95% CI 1.73–19.99; P=0.004) and T90≥5% (OR 3.13; 95% CI 1.05–9.38; P=0.041) were independently associated with CMD.
 |
Figure 4 Univariate and multivariable logistic analysis for coronary microvascular dysfunction defined by AccuIMR. Abbreviations: AccuIMR, angio-based index of microcirculatory resistance; AHI, apnea-hypopnea index; CI, confidence interval; OR, odds ratio; meanSpO2, mean oxygen saturation; minSpO2, minimal oxygen saturation; T90, the percentage of time spent with SpO2 below 90%; MaxHR, maximal heart rate; MinHR, minimum heart rate. |
In the sensitivity analysis, we incrementally incorporated patients’ clinical characteristics as potential confounding variables into the regression model to better assess the association of minSpO2 and T90 with CMD. As shown in Table 3, in the fully adjusted Model 3, minSpO2≤90% and T90≥5% remain independently associated with CMD.
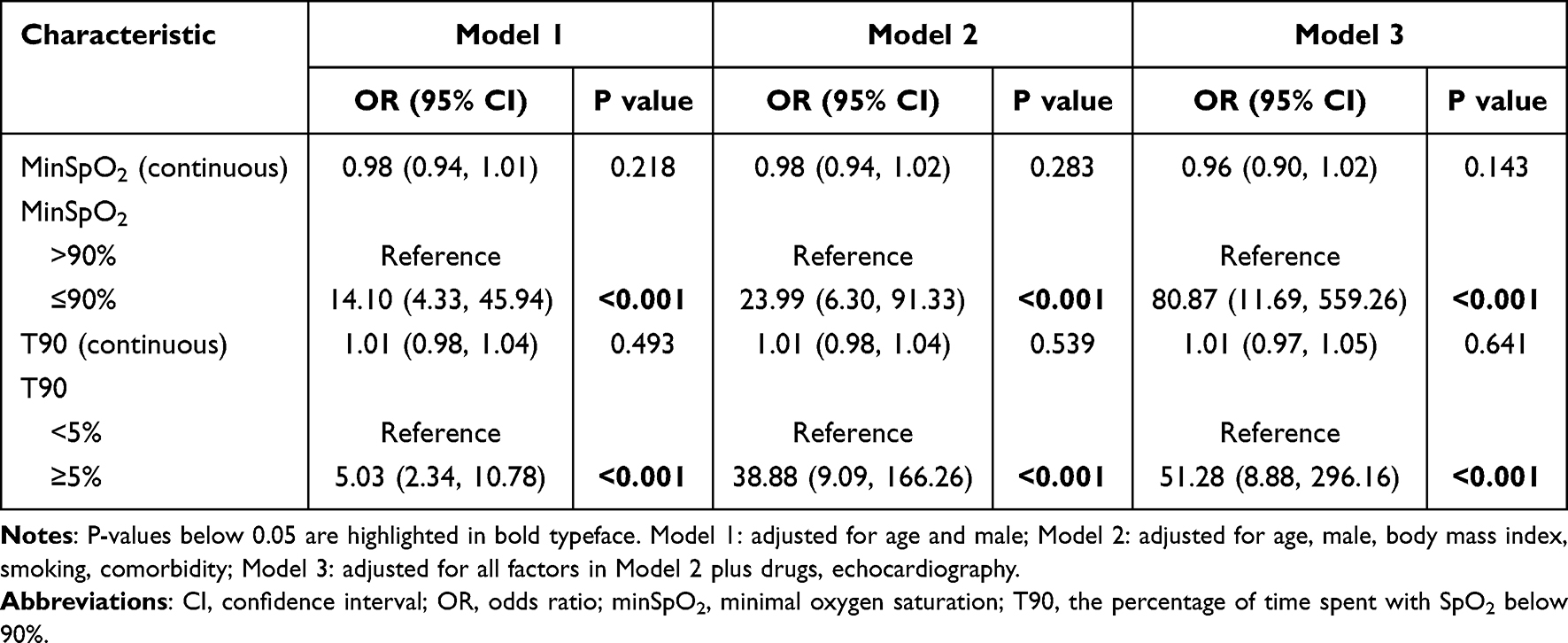 |
Table 3 Association of Nocturnal Hypoxia Parameters with Coronary Microvascular Dysfunction |
Discussion
This study found a significantly higher prevalence of OSA in patients with CMD, who also experienced a greater nocturnal hypoxic burden. The nocturnal hypoxemia parameters may more accurately reflect the relationship between OSA and CMD than AHI, highlighting the clinical importance of broadening OSA assessment beyond AHI alone in patients with cardiovascular disease. These findings challenge the traditional reliance on AHI as the sole parameter for evaluating cardiovascular risk in OSA patients and provide new insights into the complex mechanisms linking OSA, nocturnal hypoxia, and CMD.
In recent years, OSA has attracted increasing attention as an emerging independent risk factor for cardiovascular disease. OSA is a common sleep-breathing disorder that is highly prevalent in the general population.21 Previous studies have demonstrated that intermittent hypoxemia and hypercapnia resulting from OSA play a critical role in the onset and progression of cardiovascular diseases.22,23 CMD is the crucial component in the pathogenesis of myocardial ischemic disease and is regarded as a significant potential mechanism underlying OSA-related cardiovascular disease.24 Ichikawa et al demonstrated that the OSA is associated with CMD following primary percutaneous coronary intervention in patients with ST-elevation myocardial infarction (STEMI), and may contribute to adverse prognosis.25 Multiple prospective studies have demonstrated that the prevalence of OSA is significantly higher among patients with CMD, consistent with our findings.26,27 However, while the association between OSA and structural cardiovascular disease is well established, the relationship between OSA and CMD remains underexplored.
The AHI is currently employed as a standardized parameter for diagnosing and evaluating the severity of OSA and is defined as the total number of apnea and hypopnea events per hour of sleep.28 Although the AHI is commonly utilized to stratify the severity of OSA, it does not fully capture the cardiovascular disease risk associated with OSA due to its inherent limitations.29 The AHI primarily reflects the frequency of partial and complete respiratory interruptions but does not fully capture the crucial pathophysiological changes associated with OSA, such as the duration of apnea events and the extent of reduced blood oxygen saturation, which are closely linked to nocturnal hypoxemia. The results of multiple randomized controlled trials indicate that treatment for OSA focused on the AHI is insufficient to improve the clinical prognosis of patients with cardiovascular disease.30,31 Therefore, it is essential to investigate more sensitive sleep parameters that more accurately reflect the association between OSA and CMD.
Hypoxia is recognized as the primary pathogenic factor in OSA. Numerous studies have demonstrated that hypoxia indicators can more effectively predict cardiovascular disease risk in patients compared to the AHI.32,33 The study by Zhang et al demonstrated that nocturnal hypoxemia parameters are closely associated with microvascular complications in patients with type 2 diabetes, highlighting the link between hypoxia and the onset and progression of microvascular diseases.34 However, previous clinical studies on the correlation between OSA and CMD rarely analyzed the hypoxemia parameters other than AHI. In our study, we explored the relationship between various OSA parameters and CMD, rather than focusing solely on AHI. Direct indicators of hypoxemia severity, such as minSpO2 and T90, exhibited a stronger correlation with CMD compared to the AHI. After adjusting for all potential confounding factors, minSpO2≤90% and T90≥5% remain significantly and independently associated with CMD, highlighting their considerable clinical research potential.
Although indicators of hypoxemia severity appear to play a more significant role than the AHI in the association between OSA and CMD, the underlying implications and mechanisms have not been thoroughly investigated. Intermittent severe hypoxia in patients with OSA is analogous to ischemia-reperfusion injury, potentially causing mitochondrial dysfunction and increased production of reactive oxygen species, which can impair endothelial function.35 Endothelial dysfunction is a critical pathological mechanism contributing to CMD. Previous study has shown that significant impairment of endothelium-dependent vasodilation is present in patients with OSA.36 Several exploratory studies have demonstrated that continuous positive airway pressure (CPAP) therapy can enhance coronary microcirculatory function in patients with moderate to severe OSA, further illustrating the intricate relationship between these conditions in terms of their pathophysiological mechanisms.37,38 New interventions, such as otolaryngology treatments and oral appliances, require further exploration in the future to better control obstructive sleep apnea and improve cardiovascular outcomes related to CMD.39,40
This study has several limitations that should be noted. First, as a cross-sectional study, this research could not establish a causal relationship between CMD and nocturnal hypoxemia parameters. Prospective studies are necessary to confirm these findings and to further elucidate the underlying mechanisms. Additionally, all participants in this study were hospitalized, which could have introduced selection bias. Although we accounted for multiple confounding factors, complete exclusion of potential residual confounding remains challenging.
Conclusions
In conclusion, this study provides new insights into the relationship between OSA and CMD, emphasizing that nocturnal hypoxia parameters, rather than AHI alone, may more accurately reflect the underlying pathological mechanisms linking OSA and CMD. Prospective studies are needed to explore the integration of nocturnal hypoxia parameters into clinical practice for improved risk stratification and targeted interventions in OSA patients at risk for cardiovascular diseases.
Funding
This study was supported by the Capital’s Funds for Health Improvement and Research (2024-2-2066), the Coordinated innovation of scientific and technological in Beijing-Tianjin-Hebei Region (Z231100003923008), Beijing Nova Program (20220484222), and the Beijing Hospitals Authority’s Ascent Plan (DFL20220603), High-level public health technical talent construction project of Beijing Municipal Health Commission (Leading Talent-02-01).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mileva N, Nagumo S, Mizukami T, et al. Prevalence of coronary microvascular disease and coronary vasospasm in patients with nonobstructive coronary artery disease: systematic review and meta-analysis. J Am Heart Assoc. 2022;11(7):e023207. doi:10.1161/JAHA.121.023207
2. Gdowski MA, Murthy VL, Doering M, et al. Association of isolated coronary microvascular dysfunction with mortality and major adverse cardiac events: a systematic review and meta-analysis of aggregate data. J Am Heart Assoc. 2020;9(9):e014954. doi:10.1161/JAHA.119.014954
3. Pepine CJ, Anderson RD, Sharaf BL, et al. Coronary microvascular reactivity to adenosine predicts adverse outcome in women evaluated for suspected ischemia results from the National Heart, Lung and Blood Institute WISE (Women’s Ischemia Syndrome Evaluation) study. J Am Coll Cardiol. 2010;55(25):2825–2832. doi:10.1016/j.jacc.2010.01.054
4. Ng MK, Yeung AC, Fearon WF. Invasive assessment of the coronary microcirculation: superior reproducibility and less hemodynamic dependence of index of microcirculatory resistance compared with coronary flow reserve. Circulation. 2006;113(17):2054–2061. doi:10.1161/CIRCULATIONAHA.105.603522
5. Jiang J, Li C, Hu Y, et al. A novel CFD-based computed index of microcirculatory resistance (IMR) derived from coronary angiography to assess coronary microcirculation. Comput Methods Programs Biomed. 2022;221:106897. doi:10.1016/j.cmpb.2022.106897
6. Redline S, Azarbarzin A, Peker Y. Obstructive sleep apnoea heterogeneity and cardiovascular disease. Nat Rev Cardiol. 2023;20(8):560–573. doi:10.1038/s41569-023-00846-6
7. Fan J, Wang X, Ma X, et al. Association of obstructive sleep apnea with cardiovascular outcomes in patients with acute coronary syndrome. J Am Heart Assoc. 2019;8(2):e010826. doi:10.1161/JAHA.118.010826
8. Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;144(3):e56–e67. doi:10.1161/CIR.0000000000000988
9. Zhang RH, Zhao W, Shu LP, et al. Obstructive sleep apnea is associated with coronary microvascular dysfunction: a systematic review from a clinical perspective. J Sleep Res. 2020;29(4):e13046. doi:10.1111/jsr.13046
10. Ooi EL, Rajendran S, Munawar DA, et al. The association of obstructive sleep apnea in ischemia with no obstructive coronary artery disease—a pilot study. Curr Probl Cardiol. 2023;48(5):101111. doi:10.1016/j.cpcardiol.2022.101111
11. Liu W, Zhu Q, Li X, et al. Effects of obstructive sleep apnea on myocardial injury and dysfunction: a review focused on the molecular mechanisms of intermittent hypoxia. Sleep Breath. 2024;28(1):41–51. doi:10.1007/s11325-023-02893-2
12. Fan Y, Li C, Hu Y, et al. Angiography-based index of microcirculatory resistance (AccuIMR) for the assessment of microvascular dysfunction in acute coronary syndrome and chronic coronary syndrome. Quant Imaging Med Surg. 2023;13(6):3556–3568. doi:10.21037/qims-22-961
13. Zhang Y, Pu J, Niu T, et al. Prognostic value of coronary angiography-derived index of microcirculatory resistance in non-ST-segment elevation myocardial infarction patients. JACC Cardiovasc Interv. 2024;17(16):1874–1886. doi:10.1016/j.jcin.2024.04.048
14. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. deliberations of the sleep apnea definitions task force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
15. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479–504. doi:10.5664/jcsm.6506
16. Troy LK, Young IH, Lau E, et al. Nocturnal hypoxaemia is associated with adverse outcomes in interstitial lung disease. Respirology. 2019;24(10):996–1004. doi:10.1111/resp.13549
17. Minai OA, Pandya CM, Golish JA, et al. Predictors of nocturnal oxygen desaturation in pulmonary arterial hypertension. Chest. 2007;131(1):109–117. doi:10.1378/chest.06-1378
18. Huang B, Huang Y, Zhai M, et al. Association of hypoxic burden metrics with cardiovascular outcomes in heart failure and sleep-disordered breathing. ESC Heart Fail. 2023;10(6):3504–3514. doi:10.1002/ehf2.14526
19. Wang L, Wei DH, Zhang J, Cao J. Time under 90% oxygen saturation and systemic hypertension in patients with obstructive sleep apnea syndrome. Nat Sci Sleep. 2022;14:2123–2132. doi:10.2147/NSS.S388238
20. Javaheri S, Barbe F, Campos-Rodriguez F, et al. Sleep apnea: types, mechanisms, and clinical cardiovascular consequences. J Am Coll Cardiol. 2017;69(7):841–858. doi:10.1016/j.jacc.2016.11.069
21. Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet. 2014;383(9918):736–747. doi:10.1016/S0140-6736(13)60734-5
22. Bradley TD, Floras JS. Obstructive sleep apnoea and its cardiovascular consequences. Lancet. 2009;373(9657):82–93. doi:10.1016/S0140-6736(08)61622-0
23. Lévy P, Kohler M, McNicholas WT, et al. Obstructive sleep apnoea syndrome. Nat Rev Dis Primers. 2015;1:15015. doi:10.1038/nrdp.2015.15
24. Morra S, Roubille F. Obstructive sleep apnoea: from respiratory events to coronary microvascular dysfunction. Acta Cardiol. 2018;73(4):319–324. doi:10.1080/00015385.2017.1384183
25. Ichikawa Y, Izumiya Y, Tamita K, et al. Severe obstructive sleep apnea is associated with coronary microvascular dysfunction and obstruction in patients with ST-elevation myocardial infarction. Eur Heart J Acute Cardiovasc Care. 2021;10(6):645–652. doi:10.1177/2048872620919946
26. Ooi EL, Rajendran S, Tavella R, et al. Predictors of Obstructive Sleep Apnoea (OSA) population in the Coronary Angiogram Database of South Australia (CADOSA). Curr Probl Cardiol. 2022;47(6):100846. doi:10.1016/j.cpcardiol.2021.100846
27. Wang N, Li SB, Zhao LS, et al. Relationship between obstructive sleep apnea and coronary microcirculatory function among patients with cardiac syndrome X. Coron Artery Dis. 2014;25(1):35–39. doi:10.1097/MCA.0000000000000058
28. Epstein LJ, Kristo D, Strollo PJ, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263–276.
29. Heinzer R, Eckert D. Treatment for obstructive sleep apnoea and cardiovascular diseases: are we aiming at the wrong target? Lancet Respir Med. 2020;8(4):323–325. doi:10.1016/S2213-2600(19)30351-0
30. McEvoy RD, Antic NA, Heeley E, et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med. 2016;375(10):919–931. doi:10.1056/NEJMoa1606599
31. Sánchez-de-la-Torre M, Sánchez-de-la-Torre A, Bertran S, et al. Effect of obstructive sleep apnoea and its treatment with continuous positive airway pressure on the prevalence of cardiovascular events in patients with acute coronary syndrome (ISAACC study): a randomised controlled trial. Lancet Respir Med. 2020;8(4):359–367. doi:10.1016/S2213-2600(19)30271-1
32. Lavie L. Oxidative stress in obstructive sleep apnea and intermittent hypoxia--revisited--the bad ugly and good: implications to the heart and brain. Sleep Med Rev. 2015;20:27–45. doi:10.1016/j.smrv.2014.07.003
33. Azarbarzin A, Sands SA, Stone KL, et al. The hypoxic burden of sleep apnoea predicts cardiovascular disease-related mortality: the osteoporotic fractures in men study and the sleep heart health study. Eur Heart J. 2019;40(14):1149–1157. doi:10.1093/eurheartj/ehy624
34. Zhang R, Zhang P, Zhao F, Han X, Ji L. Association of diabetic microvascular complications and parameters of obstructive sleep apnea in patients with type 2 diabetes. Diabetes Technol Ther. 2016;18(7):415–420. doi:10.1089/dia.2015.0433
35. Lavie L. Oxidative stress--A unifying paradigm in obstructive sleep apnea and comorbidities. Prog Cardiovasc Dis. 2009;51(4):303–312. doi:10.1016/j.pcad.2008.08.003
36. Bruno RM, Rossi L, Fabbrini M, et al. Renal vasodilating capacity and endothelial function are impaired in patients with obstructive sleep apnea syndrome and no traditional cardiovascular risk factors. J Hypertens. 2013;31(7):
37. Butt M, Khair OA, Dwivedi G, et al. Myocardial perfusion by myocardial contrast echocardiography and endothelial dysfunction in obstructive sleep apnea. Hypertension. 2011;58(3):417–424. doi:10.1161/HYPERTENSIONAHA.111.170910
38. Nguyen PK, Katikireddy CK, McConnell MV, Kushida C, Yang PC. Nasal continuous positive airway pressure improves myocardial perfusion reserve and endothelial-dependent vasodilation in patients with obstructive sleep apnea. J Cardiovasc Magn Reson. 2010;12(1):50. doi:10.1186/1532-429X-12-50
39. Lima IM, Aucapiña AD, Vallejo LL. A review on the influence of rapid maxillary expansion and mandibular advancement for treating obstructive sleep apnea in children. J Clin Pediatr Dent. 2023;47(1):9–16.
40. Segù M, Cosi A, Santagostini A, Scribante A. Efficacy of a trial oral appliance in OSAS management: a new protocol to recognize responder/nonresponder patients. Int J Dent. 2021;2021:8811700. doi:10.1155/2021/8811700
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Ring Pulse Oximetry Using Reflective Photoplethysmography and PSG in the Detection of OSA in Chinese Adults: A Pilot Study
Zhao R, Xue J, Zhang X, Peng M, Li J, Zhou B, Zhao L, Penzel T, Kryger M, Dong XS, Gao Z, Han F
Nature and Science of Sleep 2022, 14:1427-1436
Published Date: 18 August 2022
New Metrics from Polysomnography: Precision Medicine for OSA Interventions
Guo J, Xiao Y
Nature and Science of Sleep 2023, 15:69-77
Published Date: 9 March 2023
Association Between Sleep Efficiency and Hypertension in Chinese Obstructive Sleep Apnea Patients
Xia N, Wang H, Chen Y, Fan XJ, Nie XH
Nature and Science of Sleep 2023, 15:79-88
Published Date: 10 March 2023
Waiting for in-Lab Polysomnography May Unnecessarily Prolong Treatment Start in Patients with Moderate or Severe OSA at Home Sleep Apnea Testing
Pordzik J, Seifen C, Ludwig K, Ruckes C, Huppertz T, Matthias C, Gouveris H
Nature and Science of Sleep 2024, 16:1881-1889
Published Date: 5 December 2024
Performance of Four Screening Tools for Identifying Obstructive Sleep Apnea Among Patients with Insomnia
Shi C, Wang Y, Luo J, Huang R, Xiao Y
Nature and Science of Sleep 2025, 17:379-390
Published Date: 3 March 2025