")
Back to Journals » Advances in Medical Education and Practice » Volume 16
Bridging Bioscience to Practice: The Significance of Clinical Simulation Training for Novice Nursing Students
Authors Grønlien HK , Wevling A, Arntsen MB, Haug E
Received 12 June 2024
Accepted for publication 23 April 2025
Published 29 May 2025 Volume 2025:16 Pages 927—941
DOI https://doi.org/10.2147/AMEP.S482384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Heidi Kristine Grønlien,1 Astrid Wevling,1 Marian Bringa Arntsen,2 Erna Haug3
1Department of Nursing, Health and Laboratory Science, Faculty of Health, Welfare and Organisation, Østfold University College, Halden, Norway; 2Department SimFredrikstad, Faculty of Health, Welfare and Organisation, Østfold University College, Halden, Norway; 3Department of Welfare, Management and Organisation, Faculty of Health, Welfare and Organisation, Østfold University College, Halden, Norway
Correspondence: Heidi Kristine Grønlien, Department of Nursing, Health and Laboratory Science, Faculty of Health, Welfare and Organisation, Østfold University College, PO Box 700, Halden, NO-1757, Norway, Tel +4795922021, Email [email protected]
Purpose: This study aims to investigate clinical simulation as a learning method to enhance the relevance of bioscience in nursing practice for novice nursing students.
Methods: This study utilizes a semi-experimental multi-method design involving 194 novice bachelor nursing students at a Norwegian university college, marking the program’s inaugural simulation training. The students were divided into Group 1 and Group 2. Both groups underwent simulation-based training, but Group 2 received an additional extended debriefing where a bioscience specialist linked patient observations with physiological processes. Data collection occurred in two phases: quantitative data were collected on simulation day through a questionnaire and structured observation, and qualitative data from two reflection questions, supplemented with quantitative data from a questionnaire, were collected one week later.
Results: The findings revealed that students’ emotional states are highly activated during simulation training. Despite this, the students reported that their overall simulation experience was positive. A deficiency in the use of bioscience terminology was identified during debriefing to explain observations, assessments, and actions. The students’ reflections on the benefits from simulation training showed that it provides them with practical experience in visualizing real-world scenarios, fostering readiness for action as a nurse, and metacognition of their learning process. Moreover, the findings indicated that students in Group 2 (extended debriefing) were more inclined to incorporate bioscience terminology in their reflective responses, particularly considering the impact of bioscience knowledge on nursing practice.
Conclusion: Clinical simulation training provides novice nursing students with clinical experience and an opportunity to connect bioscience with practice. Although the students insufficiently used bioscientific concepts during debriefing, they evaluated the relevance of bioscience in practice highly. Our findings carry significant implications for structuring simulation training, emphasizing the necessity of specialists in both debriefing techniques and bioscience to bridge the gap between theory and practice.
Keywords: anatomy, physiology, biochemistry, nurse education, theory-practice gap
Introduction
The nursing profession’s competence base draws from various subject areas, forming a meaningful and comprehensive qualification for entry and practice. Bioscience subjects like anatomy, physiology, and biochemistry constitute an important part of this competence1–3 and are of great importance for understanding symptoms and what they can indicate of illness and health challenges.3,4 Bioscience subjects are taught separately from the overall nursing competence,1,4,5 resulting in bioscience topics appearing fragmented and poorly integrated into the overall nursing competence.4,6,7 However, integrated into the overall nursing competence and connected to practical issues, they become invaluable in providing assessment and decision-making support, facilitating the detection of deviations, and implementation of adequate measures.8–10 Given the high demands and expectations of nurses’ independence and knowledge-based services, mastering bioscience subjects is vital for students.
Studies have shown that it is challenging for nursing students to acquire bioscience subjects, and a lack of competence will again represent a concern for the effective management of patient signs, symptoms, and patient outcomes.1,11,12 The students themselves express that it is challenging to integrate this knowledge in nursing,2 and they want more pedagogical support in biological sciences.9 It can be difficult for students on their own to relate knowledge in bioscience subjects and practical skills when transitioning from the classroom to professional practice.6,13 Especially as biosciences are often introduced in the first-year nursing curriculum and the students have different professional entry levels.1,2 Manchester and Roberts14 conducted a systematic review on bioscience teaching and learning in nursing education, revealing that diverse student preferences make it difficult to pinpoint a single best method. They concluded that employing multiple educational strategies may better address student needs. Complementing these findings, Madhuvu15 explored the influence of various teaching methods used to integrate bioscience in first-year nursing curricula on nursing students’ bioscience achievement and learning. Teaching bioscience concepts within the context of clinically relevant nursing cases not only contributed to the body of knowledge but also enhanced students’ motivation and inspiration to learn.15 It is important to motivate and facilitate nursing students to master the transfer of bioscience subjects to clinical practice in order to develop nursing skills.4,8 By applying bioscience topics in clinical situations such as in clinical simulation, the theory-practice relationship can be strengthened.11 Simulation allows students to bridge the gap between theoretical knowledge and practical clinical application, enabling them to convert abstract concepts into meaningful patient data.16 Through this experience, students can connect their observations of a simulated patient with the underlying physiological processes, empowering them to actively respond to changes in the patient’s condition. Research indicates that simulation is a highly effective approach for enhancing nurses’ knowledge, critical thinking, and decision-making skills.17 As an educational tool, simulation replicates real-world clinical scenarios, providing opportunities to practice patient care, decision-making, and critical thinking in a controlled environment.18 Reflection is essential for building a bridge between theory and practice, and the students’ perception of the connection between theory and practice is directly influenced by reflective skills.19,20 Reflection on clinical experiences and theory demonstrates connections between education and practice that promote understanding and thereby contribute to nursing students being able to transfer theory to practice.8,21
The aim of this study is to explore the novice nursing students’ emotional experiences and perspectives on the benefits of clinical simulation as a learning method during the initial phase of their bachelor nursing study program, to examine their use of bioscience terminology, and to understand the impact of different teaching strategies on their perception of the relevance of bioscience into nursing practice.
Materials and Methods
Participants and Settings
This study was conducted at a university college in south-east of Norway. Participants were recruited from a nursing program during third month of their first semester (bachelor’s level; n = 206, age range = 19–49 years; 89% female; year 2018). An allocation of students into four classes of approximately equal size was randomly conducted by university administration prior to the commencement of the study. In this study, two classes were randomly combined to form either Group 1 or Group 2. The Bachelor nursing students have two courses that run in parallel first semester: Course 101 Basic nursing and Course 102 Anatomy, physiology, and biochemistry. This is the first time the students participated in a clinical simulation in their bachelor nursing study program. The practical skills and theoretical underpinnings for the simulation have previously been taught, both nursing concepts and anatomy, physiology, and biochemistry concepts.
Design
This study employs a semi-experimental multi-method design, combining both quantitative and qualitative data collected in succession during a clinical simulation to provide a comprehensive understanding of novice nursing students’ emotional experiences, perceived benefits, and connections of bioscience in the simulation context. The qualitative and quantitative findings have been meticulously integrated in the discussion to offer a holistic interpretation.
To narrow the focus of the study, the following research questions (RQ) are proposed:
- RQ1: What are the novice nursing students’ emotional experiences when using clinical simulation as a learning method?
- RQ2: What are the novice nursing students’ perspectives on the perceived benefits from simulation training in their future professional career as a nurse?
- RQ3: To what extent do novice nursing students use bioscience terminology in the debriefing session of the clinical simulation?
- RQ4: What is the impact of various teaching strategies used in clinical simulation on novice nursing students’ perception of the relevance of bioscience in nursing practice?
Simulation Procedure
In this study, we employed simulation as valuable learning method and sought to align our simulation design with the criteria outlined in the Healthcare Simulation Standards of Best Practice.22–24 By adhering to these criteria, we aimed to ensure the authenticity, validity, and educational value of our simulation-based research. The scenarios were previously tested on a similar group of students and are extensively described in Table 1. The simulation was conducted at the university’s clinical simulation center, and Figure 1 illustrates the timeline for the different sessions (prebriefing, briefing, scenario-play, debriefing, evaluation) included in the clinical simulation. The simulation involved a prebriefing session that was provided one week in advance. The preparation was delivered through oral information in a lecture, along with materials posted on the students’ learning platform, such as a video on simulation as a learning method, the schedule for the different student groups, the expected learning outcomes, and the scenarios that would be encountered. On the simulation day the students were randomly divided into simulation groups consisting of approximately ten students. To provide students with an authentic experience of the situation, the briefing session was designed to resemble a hospital report before a workday. The simulation comprised five scenarios. Two students were assigned as care providers to ensure all students had the chance to train in that role. The remaining students were assigned observers in each scenario. The student roles were rotated after each scenario. In the scenario-play, the observers initially entered the room, taking their designated places to ensure a good view of the simulation scene. Subsequently, the two care providers then entered, and the simulation commenced. Each scenario session lasted 15 minutes, with 7 minutes dedicated to scenario-play and 8 minutes allocated for debriefing. The academic staff facilitating the simulation were nursing faculty members with extensive clinical experience, and they were instructed and trained before the simulation.
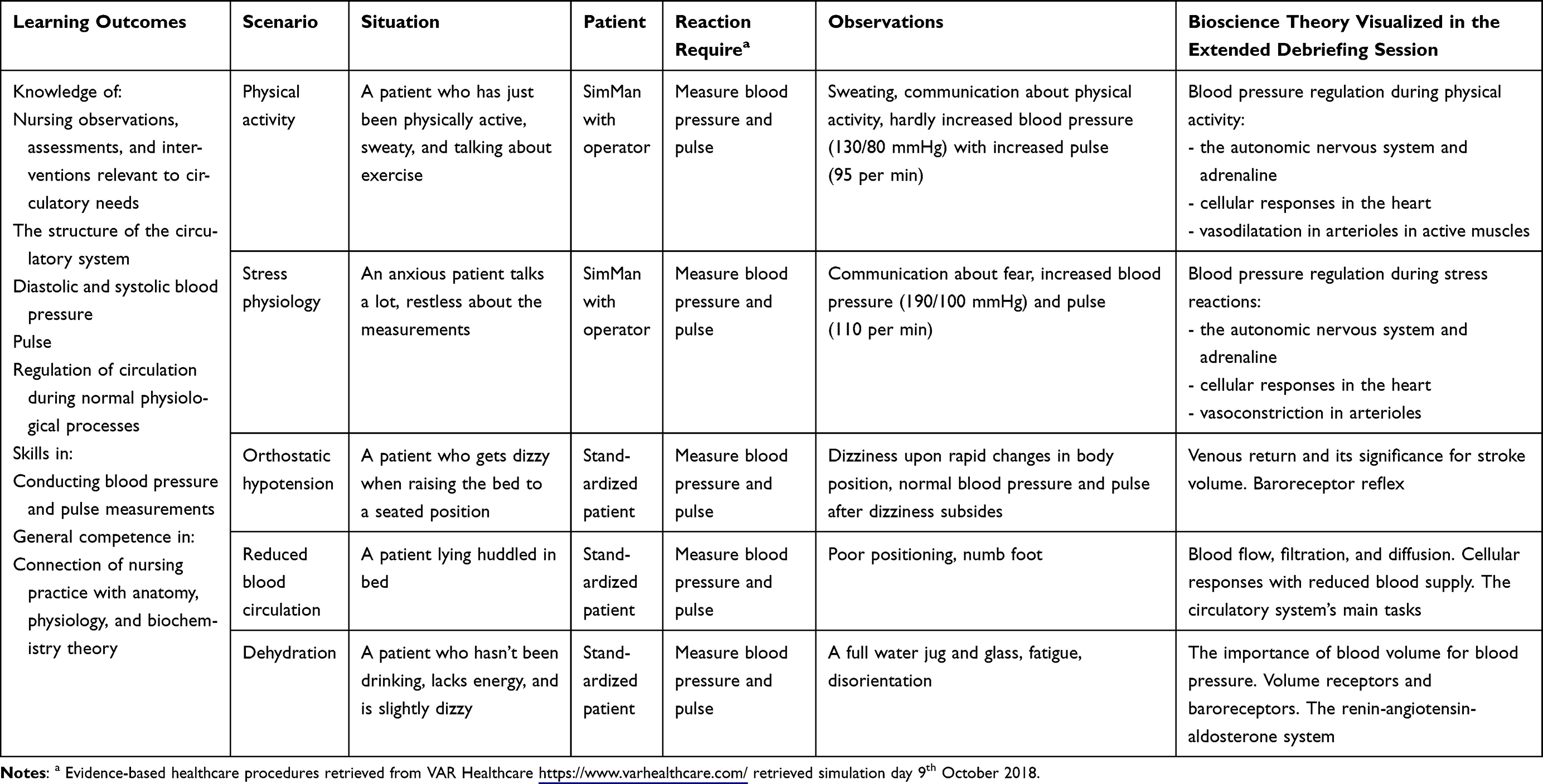 |
Table 1 Scenario Description |
 |
Figure 1 Overview of the sessions in the clinical simulation and data collection instruments application. This figure illustrates a timeline for the clinical simulation sessions, demonstrating the application of the data collection instruments used in this study. The timeline commences with the prebriefing preparation session, followed by a briefing session that took place one week later on the simulation day. Following the briefing, the students were divided into smaller groups and transferred to separate rooms with patients to enter the scenario-play session. Each scenario-play session was followed by a debriefing session. Following the completion of five scenarios with debriefing, Group 1 concluded the simulation day, while Group 2 participated in an extended debriefing with guided bioscientific reflections aimed at supporting their clinical observations. One week later, the evaluation session was conducted, in which both groups participated. |
Once all the scenarios with debriefing were completed, the day concluded for the students in Group 1. For the students in Group 2, they were gathered for a 30-minute joint extended debriefing session where a bioscience educator guided them through how the clinical observations in the simulation correlated with the underlying anatomical, physiological, and biochemical processes in the body. The bioscience educator employed reflection-guiding techniques while teaching on the whiteboard using simple anatomical drawings of the heart, blood vessels, and the sympathetic nervous system to enhance visualization and better illustrate these links between theory and practice. A more comprehensive outline of the bioscience theory underpinning these explanations is presented in Table 1.
One week later, all students were assembled for the evaluation session of the simulation. Upon completing the evaluation, Group 1 was offered the same extended debriefing session with guided reflection as Group 2 received.
Data Collection Instruments
In this study, we used multiple instruments in combination for data collection to triangulate findings and enhance validity and reliability of the data. The timeline for application of an instrument during the clinical simulation is presented in Figure 1. The instruments were distributed in paper format and collected manually after completion.
Questionnaire-1
During the scenario-play session of the simulation, we aimed to gain insights into the students’ experiences by assessing their emotional situational experience immediately before and after the simulation. To achieve this, we utilized Questionnaire-1, which included Bradley and Lang’s self-assessment manikins (SAM) for rating physiological emotional states,25 and two self-reported items to assess participants’ situational self-efficacy (SE) through sense of mastery and confidence in self-reporting, see Table 2 for item descriptions. The items of SAM were rated on a figure scale of 1 to 9. For the mood item, a score of 1 represents a very negative mood, while a score of 9 represents a very positive mood. For the physiological activation item, a score of 1 represents a calm state, while a score of 9 represents a highly excited state. Similarly, for the control item, a score of 1 represents a state of being suppressed, while a score of 9 a state of being dominating. The items of SE were scored on a scale ranging from 0 to 100%, with 0 indicating “not at all” and a score of 100 representing “completely”. The instrument has previously been validated in a simulation setting.26 Questionnaire-1 was applied immediately before (pre) and after (post) the scenario-play session for students who played the role as a nurse in the scenario. Reliability analysis for the SAM items and SE items showed moderate to good levels (Cronbach’s α = 0.91 and α = 0.73, respectively).
 |
Table 2 Nursing Students Self-Reported Situational Emotional States and Self-Efficacy Immediately Before and After Scenario-Play Session |
Structured Observation
In four of the five scenarios, a researcher with clinical and educational background adopted a passive non-intrusive role to conduct structured, systematic observations of the simulation. In the scenario-play, the researcher rated the performance of the students on a scale from 0 to 100% in accordance with the learning outcomes of skills. The scores were then averaged. The instrument has previously been validated.26
In the debriefing session of the simulation, the researcher observed the bioscientific terms used by the students in their reflection to generate numerical data from observations.27 In advance of the simulation, the research team discussed the sign system of the observation, which consisted of anatomical, physiological, and biochemical terms relevant to the scenario. The sign system included an open line for listing other bioscience terms that appeared in the debriefing.
Reflection Questions and Questionnaire-2
One week after the simulation, all students engaged in the evaluation session of the simulation. The students were asked to respond to two reflection questions. The questions were designed to allow the students to express themselves freely and thoroughly. The questions were: «What thoughts and feelings did you have during the simulation» and «What benefits do you expect to drive from the simulation in your nursing profession». After providing handwritten responses to the two questions, the forms were handed in.
Subsequently, participants were presented with a Questionnaire-2 consisting of three items: 1. “To what extent has the simulation increased your confidence”, 2. “To what extent has the simulation provided you with an understanding of your strengths and weaknesses”, and item 3. “To what extent do you find knowledge of the circulatory system useful in your nursing practice”. Reliability analysis for the items showed moderate level (Cronbach’s α = 0.60). Questionnaire-2 also encompassed one demographic item pertaining to previous practical experience. The answers were recorded on a 5-point Likert scale with “1” (to no extent) and “5” (to a great extent) as endpoints.
The reflection questions and the items in Questionnaire-2 were piloted on three nursing faculty members and three 2nd year nursing students. They expressed their view on the relevance, acceptability, and understandability of the items. The findings from the pilot evaluation indicated that the items, with small adjustments, contribute to the quality of evaluation of the simulation and that they, along with the instructions, are comprehensible.
Analysis
Statistical analysis was done with the IBM SPSS software version 24. Alpha (α) levels for hypothesis testing were set at the 0.05 level (two-tailed). Appropriate statistical analysis was tailored to the different collected datasets, and we verified normality assumptions before conducting the analysis. Parametric test (Student’s t-test and Pearson’s correlation) was used for normally distributed data, while non-parametric test (Mann–Whitney U-test) were used for skewed data. For categorical data, frequency analysis and Chi-square test for independence were performed.
The units of analysis, the students’ responses to the two reflection questions in the evaluation session of the simulation were subjected to a manifest qualitative content analysis method, guided by Graneheim and Lundman.28 The handwritten responses were transcribed and uploaded to the computer-assisted analysis platform NVivo (version 1.6). To obtain an unbiased overall impression, three researchers (a nurse scientist, a bioscientist, and a social scientist) independently reviewed the reflective responses provided by the student. Further analysis of the content in the students’ reflective response was conducted by the research team collectively, without knowledge of student group affiliation. All meaning units in each response were identified and then coded. The analysis was exhaustive by thoroughly examining and coding all relevant textual data. The analysis process was characterized by the fact that we went back and forth between meaning units, codes, categories, and subcategories. The advantage of using manifest content analysis for this objective is to gain direct information from study participants without imposing preconceived categories.
To better understand the bioscience relevance for students in nursing practice, the students’ responses were read line by line by an educator in bioscience. The meaning units with bioscience terms were identified and coded. Terms for measuring blood pressure and/or pulse were excluded from the identification process, as these concepts are inherent to practical nursing execution. The advantage of using this approach was to get an unobtrusive and nonreactive way to study the phenomenon of interest.
To meet some of the challenges of using qualitative analysis,29 we have throughout the process sought to work systematically to be true to the students’ descriptions without interpreting the underlying opinions. To bolster the study’s reliability and validity, collaborative discussions were held among all the researchers throughout the analysis process. This collective engagement ensured a thorough and comprehensive examination of the data, fostering a more robust and credible research outcome.
For comparative qualitative analysis, numeric data obtained in NVivo was transferred to SPSS for statistical analysis.
Ethical Considerations
The work described has been carried out in accordance with the code of ethics of the World Medical Association (Declaration of Helsinki), institutional ethical guidelines, and the data protection guidelines set by the Norwegian Social Science Data Services (Sikt). According to Norwegian law, our study is exempt from ethical approval by an Ethics Committee due to only anonymized and non-health-related data being collected and processed. Responses to questionnaires and reflection questions were considered voluntary participation. The research ID was created by the student and did not include any identifying information. The participants received written information about the aims and purpose of the study and were informed that they could withdraw and refrain from further participation at any time without any negative consequences.
Results
Description of the Participants
The study involved a total of 194 students on simulation day (n = 93 in Group 1, n = 101 in Group 2). In the evaluation session of the simulation, a total of 149 students took part, where 138 responded to the Reflection questions (n = 58 in Group 1, n = 78 in Group 2) and 148 responded to Questionnaire-2 (n = 64 in Group 1, n = 83 in Group 2). The students were characterized by their age and practical experience. Group 1 comprised individuals with an average age of 23.9 ± 6.6 years (mean ± SD, n = 98) with an average practical experience score of 2.8 ± 1.4 (n = 64), while Group 2 had an average age of 24.1 ± 6.5 years (n = 82) with an average practical experience score 2.8 ± 1.5 (n = 82). Overall, the study participants had comparable ages in both groups, and they exhibited similar levels of practical nurse experience.
Nursing Students’ Emotional Experiences in the Simulation Training
To address RQ1, we employed a mixed-method approach, collecting both quantitative and qualitative data to enhance the robustness of our findings. Prior to and following the scenario-play session, students provided self-reports of their situational emotional states and self-efficacy using questionnaire-1, and the results are summarized in Table 2. There were no differences in score results between Group 1 and Group 2. At this juncture, the students share the same simulation-based experience, allowing us to present their responses as a cohesive group. A paired sample t-test was used to compare self-reported situational emotions before (pre) and after (post) the scenario-play, was performed. Regarding emotional states, the students experienced a significant shift towards a more positive mood (small to medium effect), reduced physiological activation (medium effect), and a greater sense of control during the scenario-play (small effect). The sense of mastery did not exhibit significant changes, however the confidence in the self-reporting measurements increased significantly (medium effect). The observed positive shifts in mood, decreased physiological activation, increased sense of control, and enhanced confidence in self-reporting measurements suggest that the simulation was effective in fostering a supportive learning environment and enhancing student engagement.
In the scenario-play, students acted in pairs, assuming the roles as nurses. Each student was individually rated on their performance, resulting in an average performance score for all students of 74.2 ± 22.9% (n = 134). There was no difference in performance score between Group 1 (74.1 ± 25.6%, n = 63) and Group 2 (72.5 ± 22.0%, n = 71). In this study, the performance scores are not entirely independent. Therefore, caution is taken when comparing performance to other variables. One interesting finding worth noting is that there appears to be a relationship between students’ self-reported mastery of scenario-play and their performance, which was scored by the researcher (Pearson’s r = 0.39, n = 113, p < 0.001). This finding suggests that students’ own sense of mastery in the simulation aligns closely with the expert-assessed scores of their performance, with a medium effect size indicating a moderate correlation.
The students engaged in an evaluation session where they deliberated on their thoughts and feelings during the simulation. The content analysis of the students’ reflective responses revealed a theme of Emotions in simulation generated from two categories: Initial emotional states and Emotional experiences, and the two categories derived from three and four subcategories, respectively, as presented in Figure 2.
 |
Figure 2 Model of the theme “Emotions in simulation” with categories, and associated subcategories. The model resulting from qualitative content analysis of the students’ reflective responses to reflection question one: “What thoughts and feelings did you have during the simulation training?”. |
The most reported initial emotion among the students includes feelings of anxiety, characterized by nervousness, worry and fear. One student wrote:
I was very nervous and excited in the beginning, unsure of what would happen and if I was good enough.
Many students also highlight the feeling of being excited prior to the simulation. However, some students express a sense of calmness feeling relaxed and composed.In the reflective responses students emphasized positive loaded emotional experiences from the simulation training. They report a sense of accomplishments or maintain a positive outlook as enjoyable and educational towards the simulation as illustrated by the student quote:
I thought this was a good challenge that was very educational.
However, some students express negative experiences as being uncomfortable in the simulation setting and finding the simulation stressful. A typical pattern in the students’ responses was that they were initially nervous about the simulation, but the overall experience ended up being positive, as the following quote demonstrates:I was initially nervous about what was to come, but eventually, it felt like real situations with patients. it went well as I naturally immersed myself in the patient situations and what I needed to say and do.
Item 1 and 2 in Questionnaire-2 specifically address the emotional experience from simulation training. The result indicates that novice nursing students do not consider simulation training to provide them with increased confidence, as reflected in their mean score of 3.1 ± 0.9 (n = 148). A Mann–Whitney U-test on frequency score revealed no statistical differences between Group 1 (3.2 ± 1.0, n = 64) and Group 2 (3.0 ± 0.9, n = 83, p = 0.150). The analysis of data regarding item 2 pertains to strengths and weaknesses shows a mean score of 3.6 ± 1.1 (n = 148), with no significant difference in average score between Group 1 (3.6 ± 1.1, n = 64) and Group 2 (3.6 ± 1.1, n = 83, p = 0.752).
Nursing Students’ Perspectives on the Benefits of Simulation Training
To address RQ2, the students engaged in reflection regarding the potential advantages of simulation-based learning method for their prospective career as healthcare professionals in the evaluation session. Utilizing a qualitative content analytic approach, the responses of the students to reflection question two were analyzed and three categories generated from the subcategories were identified: Visualization, Readiness for action, and Metacognition. These categories and corresponding subcategories are presented in Figure 3.
 |
Figure 3 Model of the theme “Perceived benefits from simulation” with categories, and associated subcategories. The model resulting from qualitative content analysis of the students’ reflective responses to reflection question two: “What benefits will you derive from simulation training in your profession as a nurse?”. |
The category of Visualization aims to capture the benefits of the immersive imaging experience a simulation training provides, and it was generated from three subcategories. The subcategory of seeing real-world situations concerns the benefits from imagining actual scenarios in professional practice. The students also express that they experience reality in simulation training, which gives them better understanding of the complexity and nuances of real-life situations, and as an example quote from one student:
It was very useful because you were put in different situations and had to deal with them yourself.
Additionally, they acknowledge that simulation training has transfer value to the profession by recognizing the inherent values of the profession: “I think simulation is a great tool that gives a more ‘hands on’ feeling of what this will be like when I eventually become employed as a nurse.
The category of Readiness for action encompasses the benefits of simulation training in preparing students to meet the patients’ needs in clinical settings. The category emerged from the fusion of three subcategories. The students highlight that training in practical and communicative skills make them more confident in their nursing role:
It is important to practice procedures and be confident in the performance of various nursing duties.
They also express that they learn to assess situations to identify patients’ conditions, as exemplified in following quote:By checking the pulse, I can find out if the patient is getting better or worse and tell the person what he/she can do next time.
Furthermore, they feel more prepared by being exposed to different clinical scenarios, enabling them to respond in real-world situations, and an example quote from this subcategory is:I think it will reassure me for later situations, because then I have, in a way, been through it before.
The category of Metacognition was delineated by integration of three underlying subcategories. One aspect of metacognition is dealing with the simulation situations itself, reflecting on and adapting one’s strategies by monitoring one’s own performance. A quote illustrating this subcategory is:
Useful with some stress testing to get used to thinking and acting then and there and trusting yourself and the measurements.
Another aspect of metacognition is the recognition of theoretical knowledge, including developing the ability to connect theoretical concepts to clinical practice and recognizing knowledge that is essential to becoming a competent nurse. One student wrote:In order to best understand how the patient is feeling and to help in the best possible way, we depend on understanding what is really happening inside the body.
They also express that simulation training gain new understanding of their own learning process and areas where knowledge and skills are lacking. To give an example, a student expressed:
I get tremendous benefit from this training by considering both physiology, anatomy, and nursing practice. Connecting anatomy to the field of nursing is extremely useful - I can really feel that I need it.
Nursing Students’ Use of Bioscience Terminology in Debriefing
To address RQ3, the debriefing session was subjected to structured observation. At this point, all students had completed the same initial part of the simulation training, which enabled us to compile the results into a unified group presentation. As outlined in Table 3, the frequency analysis indicates a deficient use of bioscience terms during the debriefing session as an explanatory basis for the observations, assessments, and actions made during the simulation in all four scenarios. The average use of bioscience terms used in a debriefing was per simulation group 1.3 ± 0.7 (n = 20). A Student’s t-test revealed no statistical differences between Group 1 (1.1 ± 0.7, n = 10) and Group 2 (1.6 ± 0.7, n = 10) in their use of bioscience terms in debriefing (p = 0.092). These findings indicate that students inadequately use bioscience theory to explain the simulated nursing practice.
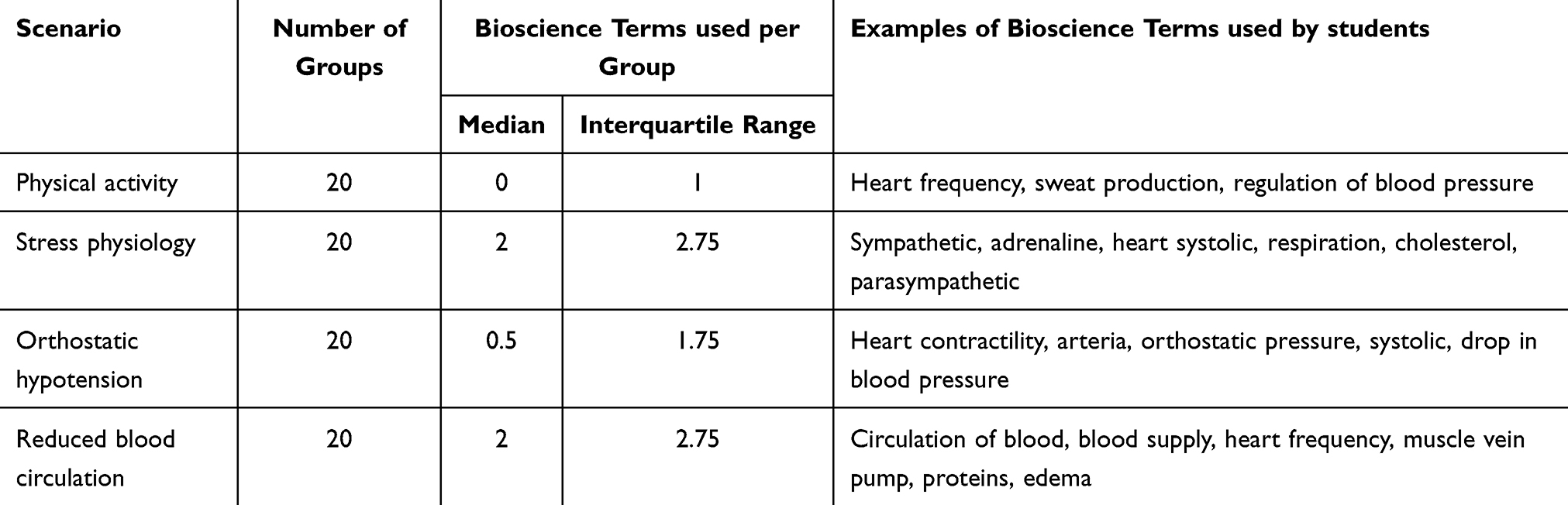 |
Table 3 Descriptive Statistics of Bioscience Terms Used in Debriefing |
Nursing Students’ Perspectives on the Relevance of Bioscience in Nursing Practice
To address RQ4, in the students’ reflective responses in evaluation session, bioscience text was identified and coded. The codes and the corresponding numbers presented in the reflective responses were as follows: anatomy (n = 15), physiology (n = 4), inside body (n = 5), circulation (n = 5), heart (n = 1), arteria (n = 2), and 102, which represents the subject number for anatomy, physiology, and biochemistry (n = 5). By using the matrix coding query in NVivo, the meaning units with a bioscience code were linked to the categories from the manifest content analysis. The results revealed 24 unique meaning units with one or several bioscience codes, originating from 23 individuals. The meanings units with a bioscience code were distributed as follows within the categories: 4.2% in Visualization, 12.5% in Readiness for action, and 83.3% in Metacognition. For the students using bioscience terminology in their responses, they emphasize the significance of engaging in academic reflection to comprehend the interrelation between patient observations and physiological processes. A student’s quote that exemplifies this is:
Very exciting to participate in and see what we have learned in practice. I found the debrief with an expert at the end very helpful, as it helped me a lot to see connections from the subjects in anatomy and physiology to practical applications.
While another student wrote:I understand more about circulation in relation to the patient. Benefit from this knowledge in terms of how a patient may be in relation to complications in the circulatory system.
The content analysis was conducted without knowledge of the group affiliation. To compare the groups in their utilization of bioscience terms in the reflective responses, a comparative qualitative analysis was conducted using NVivo’s cross-tabulation query function. A Chi-square test for independence revealed that the students in Group 2 submitted a significantly higher level of bioscience terms (n = 18) compared to Group 1 (n = 5), with χ2 = 4.84, df = 1, Phi = 0.187, and p = 0.037. These findings suggest that students who emphasize bioscience often do so when reflecting on the importance of theoretical knowledge in their future nursing roles or when underlining the acquisition of new knowledge through clinical simulation training. Additionally, students who undergo debriefing sessions with a bioscientist are more likely, albeit with a small effect size, to recognize the significance of simulation training for their future nursing roles by incorporating bioscience terminology, indicating a heightened awareness among students in Group 2 concerning the value of understanding bioscience to enhance their comprehension of clinical practice.
Item 3 in Questionnaire-2 specifically addresses the relevance of bioscience in nursing practice. The result indicates that novice nursing students consider knowledge of the circulatory system to be very useful in their nursing practice with an average score of 4.7 ± 0.5 (n = 148). The Mann–Whitney U-test revealed a significant difference in score level between Group 1 (4.6 ± 0.5, n = 64) and Group 2 (4.8 ± 0.5, n = 83), supporting the guiding reflection delivery in debriefing with a small effect size (r = 0.162, p = 0.05). These findings underscore the importance of incorporating a visualization of the bioscience theory within the debriefing of a simulation-based experience to enhance the relevance of bioscience in practice.
Discussion
This study presents our findings on novice nursing students’ experiences and perspectives of using clinical simulation as a learning method, aimed at providing clinical experiences that connect bioscience to clinical practice. The participants were in the initial semester of the nursing education program, where the inclusion of bioscience, acknowledged as one of the fundamental pillars in nursing,30 is deemed appropriate within the nursing curriculum.31 A considerable proportion of students enrolled in nursing programs directly after completing high school, with limited prior experience in clinical settings. Based on the students’ reflective responses regarding the simulation training, they expressed that their engagement in the simulation enhanced their comprehension of nursing. Furthermore, the students conveyed a heightened readiness for real-world practice, indicating a strengthened sense of preparedness. This demonstrates that simulation training provided students with hands-on, practical experience in a clinical setting.
It is quite common for students to face challenges when grasping the contents of human bioscience.31,32 To facilitate a better comprehension of the bioscience content, it has been suggested that linking bioscience theory to clinical examples can aid in simplifying the learning process.7,15 Despite the simulation’s primary focus on connecting bioscience to nursing practice, with the learning outcomes encompassing practical skills, nursing theory, and anatomy and physiology theory, the subsequent debriefing sessions generally fell short in emphasizing key concepts related to bioscience. During the debriefing, it may not have occurred naturally to the students and facilitators to delve into anatomic and physiological processes as explanatory factors for clinical observations made during the simulation. A comprehensive review by Jensen and colleagues4 revealed the ongoing challenges within the nursing field concerning the understanding and practical application of bioscience. This is evidenced by research that highlights how nursing students faced difficulties in acquiring and effectively applying biosciences knowledge in clinical practice.11,30
In this study, we employed a teaching strategy during simulation training by including a bioscience educator, rather than solely relying on nurse educators during the debriefing process. The nurse educators facilitated the debriefing process regarding practical nursing skills, while the bioscience educator facilitated the debriefing focusing on the physiological processes within the “patients”. Together, these debriefings aimed to bridge theory to practice, which was one of the learning objectives for the clinical simulation. According to INACSL’s standards of best practice, the facilitator guiding the debrief should have knowledge and skills of the debriefing process as well as theoretical knowledge, which simulated case addresses.33,34 Previous research has demonstrated that students highly value the integration of simulation training alongside essential theoretical teachings from a bioscientist during their nursing education.8 Moreover, an educational approach where a bioscience expert emphasizes the connection between bioscience and clinical situations prior to practice has been shown to have a profound impact on students’ perception, helping them recognize the pivotal role of science in their nursing practice.35 Our findings indicate that the students in Group 2 compared to Group 1, to a greater extent highlighted bioscience in their reflection on how simulation training influenced their future role as a nurse.
In our analysis, the majority of meaning units with bioscience terminology were sorted under the category metacognition. Metacognition encompasses skills that enable learners to understand and monitor their cognitive processes and has been identified as a strong predictor for learning and achievement in the sciences due to its influence on self-regulated learning.36 Self-regulated learning refers to our ability to understand and control our learning environments. While only a minority of students achieve complete self-regulation, those who possess stronger self-regulated skills tend to acquire knowledge more efficiently, expending less effort, and express higher level of academic satisfaction.37 By acknowledging their learning needs in forging connections between bioscience and nursing practice, students in Group 2 may have taken the initial steps towards self-regulated learning of bioscience. This initial awareness and reflection suggest that simulation training can effectively promote the recognition of bioscience as an integral part of nursing practice, thereby supporting the development of self-regulated learning skills.
Another important component of self-regulated learning is self-efficacy, as it significantly influences learners’ engagement and perseverance when dealing with challenging tasks.36 Students with higher self-efficacy are more inclined to actively undertake difficult tasks and demonstrate greater persistence, even in the face of initial setbacks, compared to their low-efficacy counterparts.38–40 In our study, we found that novice nursing students experienced high levels of initial emotional activation during simulation training, as evidenced in their qualitative responses in the evaluation. Despite this, the students expressed a sense of positive mastery that correlated with their performance scores. The use of simulation as a learning method for first-year nursing students is supported by previous studies showing that simulation training provides an opportunity for students to interact with real patients and gain a genuine understanding of their own self-efficacy.11,41
It is crucial to ensure continuous integration of bioscientific theory and nursing practice throughout the nursing curriculum. Jensen and colleagues4 have highlighted the importance of establishing stronger connections between academic staff and real-world practice, allowing students to readily recognize the practical relevance of bioscience content within their clinical placements. The significance of acquiring a deep understanding of bioscience in nursing practice is emphasized by academic staff.42 Collaboration between nursing teachers, teachers from other departments, and professionals is recommended to motivate students by highlighting the relevance of in-depth knowledge of bioscience in nursing through the use of nursing care and clinical cases. Furthermore, the development of educational programs that cater to students’ individual learning needs and enable active engagement in the learning process is deemed necessary.42 In our study, simulation training has successfully offered students valuable practical experience, accompanied by bioscience specialist visualization of the bridge connecting bioscience theory and practice, however, it remains the students’ responsibility to construct this bridge themselves. It has been shown for registered nurses that the application of bioscience acquired during their undergraduate years formed them to rely on their clinical judgment and communicate with confidence.43 The pragmatic value of bioscience knowledge in day-to-day practice empowered registered nurses to contextualize their nursing care plans and customize holistic care provision according to the unique requirements of each patient.43
Recommendations
The pursuit of effective strategies for implementing simulation in education holds significant importance for advancing simulation as a teaching method.44 Based on our findings, we recommend including a specialist alongside the facilitator during debrief session in simulation to bridge the gap between theory and practice. We also recommend implementing the measuring instruments into the simulation procedure to provide students with an opportunity to observe and engage in self-reflection.
Limitations
When using self-reported data in our research, it is essential to acknowledge several limitations that may affect the study’s outcomes. To conscientiously address these limitations, we employed various strategies, including the use of validated measurement instruments, randomized sampling techniques, and to uphold the credibility of our research findings. An inherent limitation of the study was to match students’ handwritten code entries across the stages of the study. A potential limitation of this study is the risk of biases during the coding and interpretation of qualitative content analysis. Despite efforts to anonymize student groups, their reflections often revealed group affiliations, potentially influencing our coding. Researcher biases, such as confirmation and cultural biases, may have inadvertently affected the coding process and data interpretation. Additionally, the subjective nature of qualitative analysis can introduce interpretation bias, impacting the accuracy and reliability of the findings.
Due to the high number of students and limited bioscientist available, the guided reflection in debriefing was conducted collectively for 1/4 of the total of students rather than individually for each simulation group. Ideally, the nurse and bioscience educators would facilitate collaboratively in the debriefing session.
We considered including knowledge assessments to enhance the study. However, we were concerned that students might perceive the reflection process as a test rather than a genuine reflective exercise. Additionally, the students had only been in the program for two months, and the focus of the simulation was not specifically on learning bioscience per se but rather on experiencing the relevance of bioscience in clinical practice.
Conclusion
Overall, clinical simulation training has a multifaceted impact on novice nursing students. This educational approach activates situational emotions that many students find beneficial during the simulation process. The students view simulation training not only as a means to enhance visualization by experiencing real-world scenarios, and as a way to bolster their readiness for action in nursing practice, but also as an opportunity to foster metacognition, allowing the students to reflect on their learning process.
This study also examined how bioscience was expressed in the different phases of simulation training. It appears that during the debriefing phase, students made limited use of bioscientific theory. On the other hand, during the evaluation phase, several students used bioscientific terminology in their reflections on the usefulness of the simulation training, with the majority categorized under metacognition, specifically underscoring the importance of theoretical knowledge in practice. The expression of bioscience relevance in nursing practice was particularly evident when the students received guidance in bioscience that linked the clinical observations in the simulations with physiological processes in the human body. These results suggest considerations for refining debriefing approaches in simulation, emphasizing the value of including a bioscience specialist to harmonize bioscience theory and practice effectively. In future research, it would be interesting to explore how repeated exposure to simulation with this type of extended debriefing impacts long-term learning of bioscience and whether the improved use of bioscience terminology translates into better clinical decision-making.
Acknowledgments
The authors gratefully acknowledge the participation of students and staff at SimFredrikstad, as well as the valuable contribution of statistician Aliaksandr Hubin. During the preparation of this work, the authors used GPT UiO in order to improve readability and language. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kyte L, Lindaas I, Dahl H, Valaker I, Kleiven OT, Sægrov S. Nursing students’ preferences for learning medical and bioscience subjects: a qualitative study. Nurs Rep. 2023;13(2):622–633. doi:10.3390/nursrep13020055
2. McVicar A, Andrew S, Kemble R. The ‘bioscience problem’ for nursing students: an integrative review of published evaluations of Year 1 bioscience, and proposed directions for curriculum development. Nurse Educ Today. 2015;35(3):500–509. doi:10.1016/j.nedt.2014.11.003
3. Knutstad U, Småstuen MC, Jensen KT. Teaching bioscience to nursing students—What works? Nursing Open. 2021;8(2):990–996. doi:10.1002/nop2.709
4. Jensen KT, Knutstad U, Fawcett TN. The challenge of the biosciences in nurse education: a literature review. J Clinic Nurs. 2018;27(9–10):1793–1802. doi:10.1111/jocn.14358
5. Craft J, Hudson P, Plenderleith M, Wirihana L, Gordon C. Commencing nursing students’ perceptions and anxiety of bioscience. Nurse Educ Today. 2013;33(11):1399–1405. doi:10.1016/j.nedt.2012.10.020
6. Smeby J-C, Heggen K. Coherence and the development of professional knowledge and skills. J Educ Work. 2014;27(1):71–91. doi:10.1080/13639080.2012.718749
7. Gordon CJ, Hudson PB, Plenderleith MB, Fisher M, Craft JA. Final year Australian nursing students’ experiences with bioscience: a cross-sectional survey. Nurs Health Sci. 2017;19(1):22–28. doi:10.1111/nhs.12310
8. Bevan AL, Joy R, Keeley S, Brown P. Learning to nurse: combining simulation with key theory. Br J Nurs. 2015;24(15):781–785. doi:10.12968/bjon.2015.24.15.781
9. Molesworth M, Lewitt M. Preregistration nursing students’ perspectives on the learning, teaching and application of bioscience knowledge within practice. J Clinic Nurs. 2016;25(5–6):725–732. doi:10.1111/jocn.13020
10. Unsworth J, Melling A, Tuffnell C, Allan J. Improving performance amongst nursing students through the discovery of discrepancies during simulation. Nurse Educ Pract. 2016;16(1):47–53. doi:10.1016/j.nepr.2015.07.003
11. Bakon S, Craft J, Christensen M, Wirihana L. Can active learning principles be applied to the bioscience assessments of nursing students? A review of the literature. Nurse Educ Today. 2016;37:123–127. doi:10.1016/j.nedt.2015.11.030
12. Rafferty B, Mthimunye K, Bimerew M. Theory-practice gap: nursing students’ self-reported depth of understanding of bioscience and its relevance to clinical practice. PLoS One. 2023;18(11):e0294319. doi:10.1371/journal.pone.0294319
13. Eraut M. Transfer of knowledge between education and workplace settings. In: Rainbird H, Fuller A, Munro A, editors. Workplace Learning in Context. Routledge; 2004:chap201–221.
14. Manchester KR, Roberts D. Bioscience teaching and learning in undergraduate nursing education: a systematic review with narrative synthesis. Nurse Educ Pract. 2025;82:104226. doi:10.1016/j.nepr.2024.104226
15. Madhuvu A, Gao W, Rogers R, O’Halloran M, Bennett N, Morphet J. Horizontal integration of bioscience and nursing in first-year nursing curricula: a systematic review. Nurse Educ Today. 2022;118:105519. doi:10.1016/j.nedt.2022.105519
16. Munazza S, Khan Z. Healthcare simulation: an effective way of learning in health care. Pakistan J Medical Sciences. 2023;39(4). doi:10.12669/pjms.39.4.7145
17. Zhao W, M-m X, Tian Q, Han Y-J, Wang Z-Q, Zhang W. The impact of simulation-based learning on nursing decision-making ability: a meta-analysis. Clinic Simul Nurs. 2024;93. doi:10.1016/j.ecns.2024.101576
18. Jeffries PR. A framework for designing, implementing, and evaluating simulations used as teaching strategies in nursing. Nurs Educ Perspec. 2005;26(2):96–103.
19. Hussein M, Osuji J. Bridging the theory-practice dichotomy in nursing: the role of nurse educators. J Nurs Educ Pract. 2017;7(3):20–25.
20. Naicker K, Van Rensburg GH. Facilitation of reflective learning in nursing: reflective teaching practices of educators. AJNM. 2018;20(2):1–15. doi:10.25159/2520-5293/3386
21. Hatlevik IKR. The theory‐practice relationship: reflective skills and theoretical knowledge as key factors in bridging the gap between theory and practice in initial nursing education. J Adv Nursing. 2012;68(4):868–877. doi:10.1111/j.1365-2648.2011.05789.x
22. Watts PI, McDermott DS, Alinier G, et al. Healthcare simulation standards of best practice simulation design. Clinic Simul Nurs. 2021;58:14–21. doi:10.1016/j.ecns.2021.08.009
23. INACSL Standards Committee. INACSL standards of best practice: simulationsm simulation design. Clinic Simul Nurs. 2016;12:S5–S12. doi:10.1016/j.ecns.2016.09.005
24. Lioce L, Meakim CH, Fey MK, Chmil JV, Mariani B, Alinier G. Standards of best practice: simulation standard IX: simulation design. Clinic Simul Nurs. 2015;11(6):309–315. doi:10.1016/j.ecns.2015.03.005
25. Bradley MM, Lang PJ. Measuring emotion: the self-assessment manikin and the semantic differential. J Behav Ther Exp Psychiatry. 1994;25(1):49–59. doi:10.1016/0005-7916(94)90063-9
26. Lugo RG, Hjelmeland I, Hansen MT, Haug E, Sütterlin S, Grønlien HK. Impact of initial emotional states and self-efficacy changes on nursing students’ practical skills performance in simulation-based education. Nursing Reports. 2021;11(2):267–278. doi:10.3390/nursrep11020026
27. Cohen L, Manion L, Morrison K. Research Methods in Education (8a Edic.). London, New York: Routledge; 2018.
28. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
29. Graneheim UH, Lindgren B-M, Lundman B. Methodological challenges in qualitative content analysis: a discussion paper. Nurse Educ Today. 2017;56:29–34. doi:10.1016/j.nedt.2017.06.002
30. Craft J, Christensen M, Bakon S, Wirihana L. Advancing student nurse knowledge of the biomedical sciences: a mixed methods study. Nurse Educ Today. 2017;48:114–119. doi:10.1016/j.nedt.2016.10.003
31. McVicar A, Andrew S, Kemble R. Biosciences within the pre-registration (pre-requisite) curriculum: an integrative literature review of curriculum interventions 1990–2012. Nurse Educ Today. 2014;34(4):560–568. doi:10.1016/j.nedt.2013.08.012
32. Slominski T, Grindberg S, Momsen J. Physiology is hard: a replication study of students’ perceived learning difficulties. Adv Physiol Educ. 2019;43(2):121–127. doi:10.1152/advan.00040.2018
33. Decker S, Alinier G, Crawford SB, Gordon RM, Jenkins D, Wilson C. Healthcare simulation standards of best practicetm the debriefing process. Clinic Simul Nurs. 2021;58:27–32. doi:10.1016/j.ecns.2021.08.011
34. Persico L, Belle A, DiGregorio H, Wilson-Keates B, Shelton C. Healthcare simulation standards of best practiceTM facilitation. Clinic Simul Nurs. 2021;58:22–26. doi:10.1016/j.ecns.2021.08.010
35. Christensen M, Craft JA, Wirihana L, Gordon CJ. Pathophysiology team teaching: bioscientist contribution to knowledge integration in a nursing subject. J Clinic Nurs. 2015;24(23–24):3739–3741. doi:10.1111/jocn.12959
36. Schraw G, Crippen KJ, Hartley K. Promoting self-regulation in science education: metacognition as part of a broader perspective on learning. Research in Science Education. 2006;36(1):111–139. doi:10.1007/s11165-005-3917-8
37. Zimmerman BJ. Attaining Self-Regulated Learning: A Social-Cognitive Perspective. Handbook of self-regulation Academic Press; 2000.
38. Pajares F. Self-efficacy beliefs in academic settings. Review of Educational Research. 1996;66(4):543–578. doi:10.3102/00346543066004543
39. Bandura A. Self-efficacy: the exercise of control. Freeman. 1997.
40. Bandura A. Social foundations of thought and action. Englewood Cliffs, NJ. 1986;1986(23–28):2.
41. Karabacak U, Unver V, Ugur E, et al. Examining the effect of simulation based learning on self-efficacy and performance of first-year nursing students. Nurse Educ Pract. 2019;36:139–143. doi:10.1016/j.nepr.2019.03.012
42. Satoh M, Fujimura A, Miyagawa S. Difficulties and innovations in teaching anatomy and physiology in nursing. Nurse Educ Pract. 2023;103551. doi:10.1016/j.nepr.2023.103551
43. Montayre J, Ramjan LM, Maneze D, Ho M-H, Maceri A, Salamonson Y. “Connecting the dots” – the transfer of bioscience knowledge by new graduate nurses to the clinical setting: a qualitative study. Nurse Educ Today. 2021;97:104729. doi:10.1016/j.nedt.2020.104729
44. Svellingen AH, Røykenes K, Forstrønen A, Assmus J, Brattebø G. Examining predictive factors of nursing students’ self-confidence in multiple simulation sessions: a randomized controlled study. Nurse Educ Pract. 2021;57:103231. doi:10.1016/j.nepr.2021.103231
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.