")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Effect of Narrow-Margin Hepatectomy Combined with Intraoperative Radiotherapy on Long-Term Prognosis of Patients with Centrally Located Hepatocellular Carcinoma: A Propensity Score Matching Analysis
Authors Tao C, Liu L, Hu N, Wang H, Zhang K, Liu Y, Wu F, Wang L, Rong W , Wu J
Received 5 October 2024
Accepted for publication 25 January 2025
Published 15 February 2025 Volume 2025:12 Pages 261—274
DOI https://doi.org/10.2147/JHC.S497998
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ali Hosni
Changcheng Tao,1,* Liguo Liu,2,* Nan Hu,1,* Hongwei Wang,1,* Kai Zhang,1 Yue Liu,1 Fan Wu,1 Liming Wang,1 Weiqi Rong,1 Jianxiong Wu1
1Department of Hepatobiliary Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, People’s Republic of China; 2Second Department of Hepatopancreatobiliary Surgery, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weiqi Rong, Email [email protected]; Jianxiong Wu, Email [email protected]
Background: Radiotherapy offers potential benefits for patients with hepatocellular carcinoma (HCC); however, the distinct role of intraoperative radiotherapy (IORT) during narrow-margin hepatectomy remains inadequately defined. This study aims at assessing the safety and effectiveness of IORT for centrally located HCCs during narrow-margin hepatectomy.
Methods: This single-center, retrospective research incorporated 659 patients with centrally located HCCs. After applying exclusion criteria, 607 patients remained and were divided into two groups: IORT integrated with liver resection (IORT+LR, 54 patients) and mere liver resection (LR, 553 patients). Propensity score matching (PSM) was performed to balance baseline characteristics. Post PSM, surgical outcomes, long-term recurrence, survival rates and adverse events were analyzed.
Results: A total of 54 patients were successfully matched, without significant differences upon baseline characteristics (standardized mean difference, SMD < 0.15). Post-matching analysis revealed that overall survival (OS) and disease-free survival (DFS) were notably improved in the IORT+LR group (P =0.027 and 0.015, respectively). Multivariate Cox regression identified IORT as an independent prognostic factor for better DFS and OS. Among the 108 patients included after matching, 57 experienced HCC recurrence, 23 in the IORT group and 34 in the LR group, showing a clear difference in recurrence rates (P =0.034). Also, there were no apparent differences in mild/severe complications between IORT and RT groups (96.3% vs 98.2%, P =0.558, respectively).
Conclusion: IORT is an effective and well-tolerated therapy for HCC patients. The combination of narrow-margin hepatectomy and IORT enhances patient prognosis, with IORT identified as an independent prognostic factor.
Keywords: centrally located hepatocellular carcinoma, intraoperative radiotherapy, hepatectomy, recurrence, prognosis
Introduction
Liver cancer poses a severe global health challenge, ranking as the fourth leading cause of cancer-related mortality worldwide.1 Hepatocellular carcinoma (HCC), the most common form of liver cancer, comprises 80–90% of primary liver malignancies and is primarily associated with chronic viral infections (hepatitis B and C), alcohol abuse, non-alcoholic steatohepatitis, and other factors that contribute to chronic inflammation and cirrhosis.2,3 HCC is particularly prevalent in Asia and Africa, with hepatitis B and C viruses as predominant etiological factors, especially in the Middle East, North Africa, and Asia. Among these regions, China carries the highest global burden of HCC, emphasizing its critical public health impact.2,3
Despite therapeutic advancements, HCC continues to have a high global mortality rate, with a median overall survival (OS) of 6–10 months.3 Early-stage HCC (BCLC 0 or A) is managed with curative-intent treatments such as surgical resection, ablation, or liver transplantation.1 Radiofrequency ablation (RFA) or microwave ablation (MWA) is standard for early-stage HCC patients who are ineligible for surgery or transplantation, while transarterial radioembolization (TARE) and stereotactic body radiotherapy (SBRT) serve as alternative approaches.4–7 Resection and liver transplantation remain the cornerstone curative therapies for HCC, offering median overall survival exceeding 5 years and 10 years, respectively, in carefully selected patients.8,9 Advances in HCC management have expanded eligibility for surgical interventions, refined patient selection for locoregional therapies, and increased systemic options.2,5,10 Nevertheless, recurrence rates remain high, with 5-year recurrence observed in 50–70% of cases, particularly among patients with multi-nodular disease, microvascular invasion (MVI), and poorly differentiated tumors.11–13
Centrally located HCCs, commonly found in Couinaud segments I, IV, V, VIII, or at the junction of these segments, are often in close proximity (with a distance of <1 cm) to critical vascular structures such as the hepatic vein, portal vein, major biliary branches, and retrohepatic inferior vena cava, as confirmed by preoperative imaging, intraoperative assessment, and pathological examination.14,15 These tumors frequently necessitate narrow (<1 cm) or null-margin resections, which are connected with a notably increased risk of recurrence, with disease-free survival (DFS) ranging from 15–30%, underscoring the critical need for effective adjuvant therapies.14,16
In addition, HCC is highly radiosensitive, with local control rates ranging from 71–100% following radical radiotherapy.17,18 Radiotherapy is a critical cancer treatment for primary tumors and metastases, providing symptom relief and local control. Conventional external beam radiotherapy (EBRT) delivers low doses to minimize toxicity, while newer techniques like stereotactic radiosurgery (SRS) and SBRT offer precise, high-dose delivery.19,20 However, SBRT is associated with toxicities, including radiation-induced liver disease (RILD), with classic RILD occurring in <5% of cases and non-classic RILD being more common in cirrhotic patients. The optimal combination and timing of SBRT with other treatments require further research, with close monitoring essential to manage potential complications.21,22 In recent decades, intraoperative radiotherapy (IORT) has been employed in both adjuvant and palliative treatments for various cancers, including those of the pancreas, breast, colorectal, gastric, head and neck, genitourinary, gynecological, and retroperitoneal soft tissue sarcomas.23 IORT is mainly performed with electrons (IOERT), high-dose-rate (HDR)-brachytherapy, or low-kV X-rays.24 IOERT is a specialized treatment that delivers a high-dose, single fraction of radiation directly to the tumor bed during surgery.25,26 IOERT enhances local control by reducing cancer cell spread and protecting healthy structures through direct visualization during surgery.27,28 It is commonly used as an adjunct to preoperative or postoperative EBRT, particularly when there is a high risk of local recurrence but limited capacity for further dose escalation due to the proximity of critical organs, such as the small bowel, stomach, and kidneys. In most cases, IORT, whether administered alone or in combination with EBRT, effectively achieves local control.29 Thus, we carried out a single-center, retrospective study from January 2016 to January 2020 to appraise the safety and effectiveness of IORT in patients undergoing narrow-margin hepatectomy for centrally located HCCs. The study demonstrated that IORT is a safe and effective adjunct in the surgical management of these tumors.
Materials and Methods
Selection of Patients
We retrospectively analyzed patients who underwent surgical resection for HCC at Cancer Hospital, Chinese Academy of Medical Sciences between January 2016 and January 2020. Inclusion criteria included: (1) Age ≥18 years; (2) Histologically confirmed HCC; (3) Centrally located HCC within <1 cm or adhered to the hepatic vein, portal vein, primary biliary branches, or retrohepatic inferior vena cava, verified by preoperative imaging, intraoperative examination, and postoperative pathology; (4) R0 resection status; (5) Child-Pugh class A liver function; (6) Eastern Cooperative Oncology Group Performance Status (ECOG PS) score of 0 or 1; (7) Availability of comprehensive clinical and pathological data. Exclusion criteria were: (1) Presence of multiple liver tumors; (2) Preoperative or postoperative radiotherapy.
Enrollment of all subjects, including inclusion and exclusion criteria, was determined by a multidisciplinary team (MDT) comprising surgeons, physicians, radiologists, and pathologists who jointly decided on patient treatment.
Treatment
Surgical Treatment
Exploratory laparotomy of the abdomen and pelvis was initially conducted to exclude distant metastases, with intraoperative ultrasound employed when necessary for tumor evaluation. The extent of liver resection was decided by a comprehensive assessment of tumor characteristics and the degree of liver cirrhosis. Individualized accurate liver resection was performed using the selective and dynamic region-specific vascular occlusion (SDRVO) technique. Surgical approaches included both anatomic and non-anatomic hepatectomy. For cases where tumors were adhered to major vascular or biliary structures, resection was performed without a margin, meticulously dissecting the tumor from the surface of these critical structures.
Intraoperative Radiotherapy
Patients were allocated to the IORT arm based on an MDT discussion. Those who met the inclusion criteria and voluntarily opted for IORT were included in the IORT group. For patients scheduled to receive IORT, intraoperative rapid pathological examination was required to confirm HCC. The treatment plan was developed collaboratively by radiation oncologists and surgeons, based on tumor location and size, proximity to critical structures, surgical resection extent, potential sites of minimal residual disease (MRD), and the condition of adjacent normal tissues. Key parameters, including the target area, radiation dose, and electron beam applicator system (diameter: 3.0–9.0 cm; angles: 0°, 15°, or 30°), were established. The target area comprised a 1.0 cm margin surrounding the tumor with a depth radiated by 90% of the intended dose (0.5–1.5 cm, median 1.0 cm), adjusted using a Bolus sheet (0.5 or 1.0 cm thickness). Two lead plates were employed to shield perihepatic normal tissues and organs outside the radiation field. IORT was administered via the Mobetron intraoperative electron beam accelerator (IntraOp Medical Corporation, Sunnyvale, CA, USA), with a median radiation dose of 15 Gy (range 15–17 Gy) and an exposure duration of approximately 3 minutes. The applicator is removed after the procedure, allowing the surgical team to proceed with standard closure.
Follow-Up
Relapse was defined by imaging evidence of hepatocellular nodules (≥2 cm) with fast-in and fast-out characteristics or confirmed HCC through cytological or histological analysis. Routine evaluations included serum AFP measurement, liver and kidney functional tests, complete blood counts, and abdominal imaging with enhanced magnetic resonance imaging (MRI) or computed tomography (CT) scans, alongside chest X-rays. For patients with suspected metastases, chest CT, whole-body bone scans, and brain MRI were conducted for potential lung, bone, and brain lesions, respectively. Follow-up assessments were scheduled every 3 months within the first 2 years post-surgery, every 4–6 months during years 2–5, and every 6–12 months thereafter, or as clinically indicated by symptoms. All patients were monitored until January 2023.
The study obtained approval from the Ethics Committee of the Cancer Hospital, Chinese Academy of Medical Sciences. It was a retrospective, non-interventional research that did not affect the diagnosis or treatment of patients. Results were presented as statistical analyses without any identifiable patient information, in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants.
Definition and Analysis
OS was defined as the interval from the date of surgery to the date of follow-up or death. DFS was defined as the time from surgery to the date of HCC recurrence. To identify potential confounders, associations with outcomes were evaluated, and any changes in effect estimates exceeding 10% were noted. Matching analysis was utilized to mitigate selection bias, accounting for variables such as sex, age, ALT, AST, ALB, TBIL, BMI, MVI, HBV-Ag, tumor size, satellite nodules, and hepatic capsule invasion. The matching process was conducted in a 1:1 ratio with a propensity score difference of less than 0.01 to ensure minimized selection bias. Patient characteristics used to generate and distribute propensity scores were evaluated both pre- and post-matching using standardized mean differences (SMD). A threshold SMD of less than 0.15 was considered acceptable Complications during hospitalization were assessed using the Clavien grading system: Grade I: Minor complications managed with medications (eg, antiemetics, antipyretics, analgesics) and non-invasive measures, with no requirement for surgical or radiological interventions; Grade II: Moderate complications requiring additional treatments such as blood transfusions or parenteral nutrition; Grade III: Severe complications necessitating surgical, endoscopic, or radiological interventions; Grade IV: Life-threatening complications, including central nervous system disorders, requiring intensive care unit (ICU) admission; Grade V: Death during hospitalization. Grades I and II were categorized as mild complications, while Grades III, IV, and V were classified as severe complications.
Statistical Methods
Statistical analyses were performed using R (http://www.R-project.org, The R Foundation) and IBM SPSS 23. Descriptive statistics outlined demographic and clinical characteristics, with categorical variables reported as frequencies and percentages, and compared using chi-square or Fisher’s exact tests. Continuous variables following a normal distribution were summarized as means and standard deviations and analyzed with Student’s t-test. Variables not normally distributed were presented as medians and interquartile ranges and assessed using the Wilcoxon Signed-Rank Test. OS and DFS were estimated using the Kaplan-Meier method, and group differences were evaluated with the Log rank test. Prognostic factors for DFS were identified through univariate and multivariate Cox regression models, including variables with P <0.05 in univariate analysis in the multivariate analysis. Variables with P <0.05 in multivariate analysis were considered independent prognostic factors. All statistical tests were two-sided, with a significance level set at P <0.05.
Results
A total of 659 patients were initially enrolled based on the inclusion criteria. Following application of the exclusion criteria resulting in 52 patients excluded, 43 patients with other radiotherapy and 9 with multiple liver tumors, leaving 607 patients for final analysis. These patients were then categorized into two groups: those receiving intraoperative radiotherapy combined with liver resection (IORT+LR) (54 patients) and those undergoing liver resection alone (LR) (553 patients). A flowchart of patient screening is presented in Figure 1, and baseline characteristics prior to matching are detailed in Table 1. Standardized mean differences (SMD <0.15) indicated apparent differences within two groups before matching. Variables are expressed as the mean ±SD (mean with standard deviation) or N(%) (number with percentages), unless otherwise indicated.
 |
Table 1 Comparisons of Baseline Demographics and Clinicopathological Characteristics in Patients Undergoing LR+IORT or LR Alone Before and After Propensity Score Matching Analysis |
 |
Figure 1 Flow chart and patient categorization. Abbreviations: HCC, hepatocellular carcinoma; IORT, intraoperative radiotherapy; LR, liver resection. |
Propensity Score Analyses
To address baseline imbalances, propensity-score matching (PSM) was employed to minimize differences within two groups, accounting for variables such as sex, age, ALT, AST, ALB, TBIL, BMI, MVI, HBV-Ag, tumor size, satellite nodules, and hepatic capsule invasion. Successful matching was achieved for 54 patients. As detailed in Table 1, baseline characteristics between the groups were comparable (SMD <0.15). Post-matching analysis demonstrated significant improvements in OS and DFS for the LR+IORT group compared with the LR group (P =0.027 and 0.015, respectively), as depicted in Figure 2. Before PSM, no significant differences in OS were observed between the IORT+LR and LR groups. The 1-, 3-, and 5-year OS rates were 92.6%, 83.1%, and 78.1% in the IORT+LR group compared to 91.5%, 82.0%, and 75.1% in the LR group (P =0.56). Additionally, the IORT+LR group demonstrated superior DFS, with 1-, 3-, and 5-year DFS rates of 77.8%, 62.6%, and 56.5%, respectively, versus 67.3%, 49.4%, and 40.0% in the LR group (P =0.036). After PSM, OS differences became significant, with 1-, 3-, and 5-year OS rates of 92.6%, 83.1%, and 78.1% in the IORT+LR group compared to 83.3%, 70.0%, and 55.7% in the LR group (P =0.027). Similarly, the IORT+LR group maintained significantly higher DFS rates, with 1-, 3-, and 5-year rates of 77.8%, 62.6%, and 56.5%, compared to 63.0%, 40.3%, and 34.9% in the LR group (P =0.015).
 |
Figure 2 Kaplan-Meier curve of OS (A) and DFS (B) after matching in the LR+IORT and LR groups. Abbreviations: DFS, disease free survival; IORT, intraoperative radiotherapy; LR, liver resection; OS, overall survival. |
Cox Regression
The forest plot in Figure 3 demonstrates a significant association between IORT and improved DFS in univariate analysis (HR=0.53, 95% CI [0.31, 0.90], P =0.018). Factors with a p-value <0.05, including IORT, MVI, and hepatic capsule invasion, were selected for inclusion in the multivariate Cox regression model. This analysis confirmed IORT as an independent prognostic factor associated with better DFS (HR=0.53, 95% CI [0.30, 0.92], P =0.024). As shown by forest plot Figure 4 in univariate analysis, there was significant association between IORT and better OS (HR=0.45, 95% CI [0.22, 0.93], P =0.032). 4 variables in the univariate analysis (including IORT, MVI, satellite nodule and hepatic capsule invasion, P <0.05) were included in the multivariate Cox analysis, and the results showed that IORT was the independent prognostic factors for patients (HR=0.47, 95% CI [0.23, 0.99], P =0.047).
 |
Figure 3 Cox proportional-hazards regression in DFS. Abbreviations: ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, Body Mass Index; MVI, Microvascular invasion; TBIL, total bilirubin. |
 |
Figure 4 Cox proportional-hazards regression in OS. Abbreviations: ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, Body Mass Index; MVI, Microvascular invasion; TBIL, total bilirubin. |
Recurrence
Following matching, 108 patients were included in the analysis. Among these, 57 patients experienced recurrence: 23 in the IORT group and 34 in the LR group, indicating a significant difference in recurrence rates (P =0.034). Intrahepatic recurrence occurred in 16 patients in the IORT group and 24 in the LR group, while extrahepatic metastases were observed in 7 and 10 patients, respectively. There was no significant difference in recurrence patterns (P =0.934). The incidence of margin recurrence was 2 in the IORT group and 7 in the LR group, with non-margin recurrences being 21 and 27, respectively. This difference was not statistically significant (P =0.227), as summarized in Table 2. Figure 5 presents the preoperative and postoperative follow-up contrast-enhanced MRI images of the representative patients from the IORT group.
 |
Table 2 Comparisons of Recurrence in Patients Undergoing LR+IORT or LR |
 |
Figure 5 Preoperative and postoperative contrast-enhanced MRI images of representative patients in the IORT group. Left column: preoperative liver MRI images; right column: postoperative images. Panel (A) shows the preoperative and three-month postoperative images of the first patient. Panels (B) and (C) present the preoperative and six-month postoperative images of two other patients. All patients were diagnosed with centrally-located HCC, with no recurrence observed up to follow-up. The distances represent the margin width. |
Sensitivity Analysis
An E-value was computed to appraise the robustness of the findings against unmeasured confounding. The results were robust unless an unmeasured confounder had a relative risk of HR greater than 2.75. The E-value analysis supports the robustness of the findings in the presence of potential unmeasured confounding.
Complications
In regard to safety, all 108 patients successfully completed surgery in both groups. No clear differences were discovered in intraoperative bleeding volumes or in the incidence of mild or severe complications between the IORT and LR groups (300.00 [200.00–500.00] mL vs 175.00 [100.00–300.00] mL, P =0.104; 96.3% vs 98.2%, P =0.558, respectively). Statistical analysis also showed no significant differences in margin width between these two groups (0.2 [0.1–0.4] cm vs 0.3 [0.1–0.575] cm, P =0.127). Moreover, there were no statistically remarkable discrepancy in the rates of specific complications, including infection, liver dysfunction, coagulation disorders, hydrothorax, ascites, bile leakage, and bleeding from the surgical wound. However, the duration of surgery was significantly longer in the IORT+LR group compared to the LR group (280.00 [250.00–327.50] minutes vs 200.00 [151.25–263.75] minutes, P < 0.001), as detailed in Table 3.
 |
Table 3 Operative Variables and Postoperative Complications in Patients Undergoing LR+IORT or LR |
Discussion
This study assessed the impact of IORT in patients with centrally located HCC. Results demonstrated that patients who received IORT had prominently improved prognosis compared to those who did not receive IORT. After PSM, significant differences in OS were noted, with 1-, 3-, and 5-year OS rates of 92.6%, 83.1%, and 78.1% in the IORT+LR group versus 83.3%, 70.0%, and 55.7% in the LR group (P =0.027). Moreover, the IORT+LR group exhibited significantly higher DFS rates at 77.8%, 62.6%, and 56.5%, compared to 63.0%, 40.3%, and 34.9% in the LR group (P =0.015). These findings underscore IORT as an effective and well-tolerated treatment modality that, when combined with narrow-margin hepatectomy, improves prognosis and serves as an independent prognostic factor in HCC management.
HCC predominantly arises in cirrhotic, steatotic, or infected livers, making the preservation of non-tumor liver tissue essential for maintaining liver function.30 Surgical intervention remains the preferred approach for patients with early-stage HCC (BCLC 0 or A). Resection is the primary treatment for patients without cirrhosis and for cirrhotic patients with single tumors and well-preserved liver function (Child-Pugh A without portal hypertension).9,31 Intermediate-stage HCC (BCLC B) is typically managed with locoregional therapies such as transarterial chemoembolization (TACE), TARE with yttrium-90 (Y90), and systemic treatments, while advanced-stage HCC (BCLC C) is primarily treated with systemic therapies include tyrosine kinase inhibitors (TKIs) and immunotherapies such as atezolizumab with bevacizumab.32–34
In HCC, particularly for centrally located tumors, achieving adequate surgical margins is difficult, as tumors are closely adhered to major vascular structures. This results in “null-margin” resections, where no clear margin exists. Studies indicate that narrow surgical margins (<1.0 cm) correlate with poorer prognosis and increased risks of microscopic residual disease and early relapse.15,30 Even after hepatectomy, micro-metastasis may persist in the remnant liver tissue. Adjuvant treatments, such as neoadjuvant intensity-modulated radiation therapy (IMRT) or postoperative IMRT, combined with surgery, have shown promise in controlling residual tumor cells and reducing intrahepatic and extrahepatic recurrence.35 Patients who received IMRT within 4–6 weeks after surgical resection demonstrated encouraging outcomes, with 3-year OS and DFS rates of 88.2% and 68.1%, respectively, and 5-year OS and DFS rates of 72.2% and 51.6%. Intrahepatic recurrence was the primary pattern of relapse, with no marginal recurrence observed. Radiation-related grade-3 toxicities were relatively low, with leukopenia being the most common (7.9%).16 Previous studies have also shown that postoperative radiotherapy can reduce both marginal and intrahepatic or extrahepatic recurrences in patients with narrow margins.36 A study by Shi et al showed significant improvements in OS (89.5% vs 69.4%) and DFS (65.8% vs 36.87%) with postoperative radiotherapy for narrow margins.37
Additionally, combining radiotherapy with TACE significantly enhances long-term survival, improves targeting of hypovascular lesions. SBRT has shown promising synergistic effects when combined with immune checkpoint inhibitors. Radiotherapy increases the efficacy of immunotherapy by releasing antigens in the microenvironment and boosting the expression of immune receptors.38 However, SBRT targeting gastrointestinal structures can lead to toxicities, including gastrointestinal and biliary tract damage, liver injury, and acute toxicities, with the most significant predictor being volumes receiving >35 Gy. Severe complications such as ulcers and fistulas are rare (<5%) but can be life-threatening. A study by Osmundson et al reported grade-2 and grade-3 central hepatobiliary tract (cHBT) toxicities in 24% and 18.8% of patients, respectively.38,39
In this article, we explored adjuvant IORT to reduce recurrence following hepatectomy. IORT with the INTRABEAM system, combined with portal vein infusion chemotherapy, has shown promise in treating portal vein tumor thrombus (PVTT), reducing recurrence rates, and improving survival outcomes.26,40,41 Our study assessed the impact of IORT following narrow-margin resection in patients with centrally located HCC. No standardized guidelines for this treatment approach currently exist. IORT is especially effective in managing abdominopelvic malignancies, including locally advanced or recurrent pancreatic cancer, colorectal cancer, and retroperitoneal soft-tissue sarcomas.29
IORT encompasses three primary modalities: IOERT, HDR-IORT, and low kilovoltage IORT.25 In this article, we utilized IOERT, characterized by rapid treatment times, efficient setup, and deep tissue penetration.17 HDR-IORT offers adaptable applicators for anatomically complex areas and delivers highly concentrated doses, though with extended treatment durations. Besides, low kilovoltage IORT, while having limited penetration and longer treatment times, benefits from simpler shielding requirements. In patients with locally advanced (LARC) or locally recurrent rectal cancer (LRRC), HDR-IORT significantly improves local recurrence-free survival, especially in cases with R1 resection margins (<2 mm).17 HDR-IORT demonstrates a reduced risk of local recurrence, with hazard ratios of 0.496 for LARC and 0.567 for LRRC. While preoperative radiation (45–50 Gy) cannot compensate for R1 resection, higher doses (>60 Gy) increase toxicity, which IORT mitigates by delivering concentrated radiation directly to at-risk areas during surgery, sparing surrounding tissues.17 IORT techniques show similar postoperative complication rates, making IORT an effective approach to reduce local recurrence in rectal cancers by targeting microscopic residual disease while minimizing damage to healthy tissues.17,25
Moreover, IORT has demonstrated efficacy in reducing recurrence and improving OS across various malignancies, including rectal, breast, and renal cancers.25,42,43 The biological efficacy of a single IOERT dose is 2–3 times greater than that of the same dose given through conventional fractionation.44 Compared with EBRT, IOERT provides a high dose exposure (10–20 Gy) in a single session that enhances the elimination of residual microscopic disease in the tumor bed, reduces intra- and interfractional movement, and ensures more uniform dose distribution, significantly shortening treatment duration and circumventing prolonged pre- and postoperative radiation schedules.42,44 This targeted approach allows for concentrated radiation delivery to the tumor site while ensuring precision and minimal exposure to adjacent healthy tissues and sparing critical structures such as the heart and lungs.27,28 The observed reduction in postoperative recurrence may prompt some centers to reconsider resection in patients previously deemed at high recurrence risk.
IORT not only induces direct DNA damage to tumor cells but also modifies the tumor microenvironment (TME), contributing to sustained antitumor effects in breast cancer.45 These include anti-angiogenic actions, alterations in postoperative wound fluid composition, and modulation of cancer cell metabolism, thereby inhibiting tumor growth. Furthermore, IORT diminishes the proliferative, invasive, and migratory capabilities of residual cancer cells by reducing the stimulatory effects of wound fluid. The therapeutic efficacy of IORT is optimized when applied during primary surgery, as delayed treatment may impair TME remodeling.45,46 Despite its promising therapeutic outcomes, the complete molecular mechanisms underlying effects remain incompletely understood. Further detailed investigations at the molecular level are essential to elucidate its impact on tumor recurrence, metastasis, and to identify novel therapeutic targets and strategies.
However, in China, HCC is predominantly associated with viral hepatitis and liver cirrhosis, conditions that may render patients vulnerable to compromised liver and coagulation function following IORT.1 This can adversely impact operating time, intraoperative blood loss, and postoperative outcomes. The decision to utilize IORT should be carefully individualized and determined by a multidisciplinary team. HCC commonly develops in the context of chronic liver disease. Radiotherapy for HCC in patients with liver cirrhosis is challenging due to worsened liver function and increased risk of radiation-induced complications, particularly RILD.47 Patients with severe cirrhosis may require more conservative dose tolerances. Although higher radiation doses improve efficacy, they also increase the risk of adverse events, including RILD and gastroduodenal toxicities, with up to 21% of patients experiencing complications like ascites.48,49 Careful dose management and ongoing prospective studies are crucial to minimizing toxicities and improving outcomes for cirrhotic patients undergoing RT for HCC.
This study still has several limitations. Being a single-center, non-randomized, retrospective study, it is subject to potential sampling and selection biases despite the use of propensity score matching. The small sample size of patients receiving IORT further limits the statistical power of the analysis. Nevertheless, the study provides valuable preliminary data on IORT for HCC, highlighting the need for further investigation through prospective, multi-center, randomized controlled trials with enlarged cohorts and extended follow-up periods. In conclusion, our results suggest that IORT following narrow-margin hepatectomy is a feasible and well-tolerated approach with potential clinical benefits for patients with centrally located HCC. However, due to the limited sample size, further large-scale prospective studies are imperative to verify these findings.
Conclusion
IORT is a well-tolerated and reasonable adjunct to narrow-margin hepatectomy in patients with centrally-located HCC, demonstrating improvements in clinical outcomes and functioning as an independent prognostic factor for enhanced survival. Notably, no apparent differences in mild or severe complications were revealed within the IORT and RT groups, underscoring its favorable safety profile.
Abbreviations
cHBT, central hepatobiliary tract; CT, Computed tomography; DFS, Disease-free survival; EBRT, External-beam radiation therapy; ECOG PS, Eastern Cooperative Oncology Group Performance Status; HCC, Hepatocellular carcinoma; HDR, high dose rate; ICU, Intensive care unit; IMRT, Intensity-modulated radiation therapy; IOERT, Intraoperative electron radiotherapy; IORT, Intraoperative radiotherapy; LARC, Locally advanced rectal cancer; LR, Liver resection; LRRC, Locally recurrent rectal cancer; MDT, Multidisciplinary team; MRD, Minimal residual disease; MRI, Magnetic resonance imaging; MVI, Microvascular invasion; MWA, Microwave ablation; OS, Overall survival; PSM, Propensity score matching; PVTT, Portal vein tumor thrombus; RFA, Radiofrequency ablation; RILD, Radiation-induced liver disease; SBRT, Stereotactic body radiotherapy; SDRVO, Selective and dynamic region-specific vascular occlusion; SMD, Standardized mean difference; SRS, Stereotactic radiosurgery; TACE, Transarterial chemoembolization; TARE, Transarterial radioembolization; TKIs, Tyrosine kinase inhibitors; TME, Tumor microenvironment; Y90, Yttrium-90.
Data Sharing Statement
All data related to this study are included in this paper. Details are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study had been approved by the Ethics Committee of Cancer Hospital of Chinese Academy of Medical Science. Informed consent was obtained from all participants. All reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Author Contributions
All authors made a significant contribution to the work reported. WJ and RW conceived and designed the study. TC, LL, HN and WH gathered data, analyzed the data, wrote the first manuscript draft, and provided the literature search. WJ, RW, WH, LY, WL and ZK revised or critically reviewed the article. All authors gave final approval of the version to be published. All authors have agreed on the journal to which the article has been submitted. All authors have agreed to be accountable for all aspects of the work.
Funding
This study was supported by Beijing Hope Run Special Fund of Cancer Foundation of China (LC2020L05).
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
References
1. Sankar K, Gong J, Osipov A, et al. Recent advances in the management of hepatocellular carcinoma. Clin Mol Hepatol. 2024;30(1):1–15. doi:10.3350/cmh.2023.0125
2. Singal AG, Kanwal F, Llovet JM. Global trends in hepatocellular carcinoma epidemiology: implications for screening, prevention and therapy.. Nat Rev Clin Oncol. 2023;20(12):864–884. doi:10.1038/s41571-023-00825-3
3. Toh MR, Wong EYT, Wong SH, et al. Global Epidemiology and Genetics of Hepatocellular Carcinoma. Gastroenterology. 2023;164(5):766–782. doi:10.1053/j.gastro.2023.01.033
4. Yang JD, Heimbach JK. New advances in the diagnosis and management of hepatocellular carcinoma. BMJ. 2020;371:m3544. doi:10.1136/bmj.m3544
5. Singal AG, Llovet JM, Yarchoan M. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922–1965. doi:10.1097/HEP.0000000000000466
6. Ohri N, Dawson LA, Krishnan S. Radiotherapy for Hepatocellular Carcinoma: new Indications and Directions for Future Study. J Natl Cancer Inst. 2016;108(9):133.
7. Li Z, Liu J, Zhang B. Neoadjuvant tislelizumab plus stereotactic body radiotherapy and adjuvant tislelizumab in early-stage resectable hepatocellular carcinoma: the Notable-HCC phase 1b trial. Nat Commun. 2024;15(1):3260. doi:10.1038/s41467-024-47420-3
8. Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693–699. doi:10.1056/NEJM199603143341104
9. Shrager B, Jibara G, Schwartz M, Roayaie S. Resection of hepatocellular carcinoma without cirrhosis. Ann Surg. 2012;255(6):1135–1143. doi:10.1097/SLA.0b013e31823e70a3
10. Vitale A, Cabibbo G, Iavarone M. Personalised management of patients with hepatocellular carcinoma: a multiparametric therapeutic hierarchy concept. Lancet Oncol. 2023;24(7):e312–e322. doi:10.1016/S1470-2045(23)00186-9
11. Roayaie S, Obeidat K, Sposito C, et al. Resection of hepatocellular cancer ≤2 cm: results from two Western centers. Hepatology. 2013;57(4):1426–1435. doi:10.1002/hep.25832
12. PR Galle, A Forner, JM Llovet, et al. EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
13. Li K, Zhang R, Wen F. Single-cell dissection of the multicellular ecosystem and molecular features underlying microvascular invasion in HCC. Hepatology. 2024;79(6):1293–1309. doi:10.1097/HEP.0000000000000673
14. Wu F, Chen B, Dong D. Phase 2 Evaluation of Neoadjuvant Intensity-Modulated Radiotherapy in Centrally Located Hepatocellular Carcinoma: a Nonrandomized Controlled Trial. JAMA Surgery. 2022;157(12):1089–1096. doi:10.1001/jamasurg.2022.4702
15. Tao C, Wu F, Wang H. Clinical Benefits of Neoadjuvant Radiotherapy on the Postoperative Recurrence of Centrally Located Hepatocellular Carcinoma: a Real-World Evidence Based on Phase II Clinical Trial. J Hepatocell Carcinoma. 2023;10:753–764. doi:10.2147/JHC.S403287
16. Chen B, Wu J-X, Cheng S-H. Phase 2 Study of Adjuvant Radiotherapy Following Narrow-Margin Hepatectomy in Patients With HCC. Hepatology. 2021;74(5):2595–2604. doi:10.1002/hep.31993
17. Voogt ELK, van Rees JM, Hagemans JAW. Intraoperative Electron Beam Radiation Therapy (IOERT) Versus High-Dose-Rate Intraoperative Brachytherapy (HDR-IORT) in Patients With an R1 Resection for Locally Advanced or Locally Recurrent Rectal Cancer. Int J Radiat Oncol Biol Phys. 2021;110(4):1032–1043. doi:10.1016/j.ijrobp.2021.02.006
18. Klein J, Dawson LA. Hepatocellular carcinoma radiation therapy: review of evidence and future opportunities. Int J Radiat Oncol Biol Phys. 2013;87(1):22–32. doi:10.1016/j.ijrobp.2012.08.043
19. Folkert MR, Timmerman RD. Stereotactic ablative body radiosurgery (SABR) or Stereotactic body radiation therapy (SBRT). Adv Drug Deliv Rev. 2017;109:3–14. doi:10.1016/j.addr.2016.11.005
20. Patel KR, Menon H, Patel RR, Huang EP, Verma V, Escorcia FE. Locoregional Therapies for Hepatocellular Carcinoma: a Systematic Review and Meta-Analysis. JAMA Network Open. 2024;7(11):e2447995. doi:10.1001/jamanetworkopen.2024.47995
21. Kim J, Jung Y. Radiation-induced liver disease: current understanding and future perspectives. Exp Mol Med. 2017;49(7):e359. doi:10.1038/emm.2017.85
22. Hernandez L, Parent L, Molinier V, et al. Stereotactic body radiation therapy in primary liver tumor: local control, outcomes and toxicities. Clin Transl Radiat Oncol. 2025;50(100892). doi:10.1016/j.ctro.2024.100892
23. Masaki T, Calvo FA. Editorial: intraoperative radiotherapy for gastrointestinal malignancy: updated evidence. Front Oncol. 2023;13(1217402). doi:10.3389/fonc.2023.1217402
24. Piqeur F, Peulen HMU, Cnossen JS, et al. Post-operative complications following dose adaptation of intra-operative electron beam radiation therapy in locally advanced or recurrent rectal cancer. J Contemp Brachyther. 2024;16(2):85–94. doi:10.5114/jcb.2024.139276
25. Nimer M, Ali FG. Use of Intraoperative Radiation Therapy in Rectal Cancer. Dis Colon Rectum. 2024;67(9):1101–1105. doi:10.1097/DCR.0000000000003427
26. Wei X, Jiang Y, Zhang X. Neoadjuvant Three-Dimensional Conformal Radiotherapy for Resectable Hepatocellular Carcinoma With Portal Vein Tumor Thrombus: a Randomized, Open-Label, Multicenter Controlled Study. J Clin Oncol. 2019;37(24):2141–2151. doi:10.1200/JCO.18.02184
27. Willett CG, Czito BG, Tyler DS. Intraoperative radiation therapy. J Clin Oncol. 2007;25(8):971–977. doi:10.1200/JCO.2006.10.0255
28. Choi SH, Seong J. Strategic application of radiotherapy for hepatocellular carcinoma. Clin Mol Hepatol. 2018;24(2):114–134. doi:10.3350/cmh.2017.0073
29. Roeder F, Fastner G, Fussl C. First clinical application of image-guided intraoperative electron radiation therapy with real time intraoperative dose calculation in recurrent rectal cancer: technical procedure. Radiat Oncol. 2023;18(1):186. doi:10.1186/s13014-023-02374-6
30. Tabrizian P, Jibara G, Shrager B, Schwartz M, Roayaie S. Recurrence of hepatocellular cancer after resection: patterns, treatments, and prognosis. Ann Surg. 2015;261(5):947–955. doi:10.1097/SLA.0000000000000710
31. Di Benedetto F, Magistri P, Di Sandro S. Safety and Efficacy of Robotic vs Open Liver Resection for Hepatocellular Carcinoma. JAMA Surg. 2023;158(1):46–54. doi:10.1001/jamasurg.2022.5697
32. Yang X, Yang C, Zhang S, et al. Precision treatment in advanced hepatocellular carcinoma. Cancer Cell. 2024;42(2):180–197. doi:10.1016/j.ccell.2024.01.007
33. Salem R, Johnson GE, Kim E, et al. Yttrium-90 Radioembolization for the Treatment of Solitary, Unresectable HCC: the LEGACY Study. Hepatology. 2021;74(5):2342–2352. doi:10.1002/hep.31819
34. Auer TA, Müller L, Schulze D. CT-guided High-Dose-Rate Brachytherapy versus Transarterial Chemoembolization in Patients with Unresectable Hepatocellular Carcinoma. Radiology. 2024;310(2):e232044. doi:10.1148/radiol.232044
35. Long L, Chen B, Wang H, et al. Survival benefit of radiotherapy following narrow-margin hepatectomy in patients with hepatocellular carcinoma: a propensity score-matched analysis based on phase II study. Radiother Oncol. 2023;180(109462):109462. doi:10.1016/j.radonc.2022.109462
36. Wang W-H, Wang Z, Wu J-X. Survival benefit with IMRT following narrow-margin hepatectomy in patients with hepatocellular carcinoma close to major vessels. Liver Int. 2015;35(12):2603–2610. doi:10.1111/liv.12857
37. Shi C, Li Y, Geng L, et al. Adjuvant stereotactic body radiotherapy after marginal resection for hepatocellular carcinoma with microvascular invasion: a randomised controlled trial. Eur J Cancer. 2022;166:176–184. doi:10.1016/j.ejca.2022.02.012
38. Sharma D, Khosla D, Meena BL, Yadav HP, Kapoor R. Exploring the Evolving Landscape of Stereotactic Body Radiation Therapy in Hepatocellular Carcinoma. J Clin Exp Hepatol. 2025;15(1):102386. doi:10.1016/j.jceh.2024.102386
39. Osmundson EC, Wu Y, Luxton G, Bazan JG, Koong AC, Chang DT. Predictors of toxicity associated with stereotactic body radiation therapy to the central hepatobiliary tract. Int J Radiat Oncol Biol Phys. 2015;91(5):986–994. doi:10.1016/j.ijrobp.2014.11.028
40. Song X, He Y, Liang H, Han M, Shao Z. INTRABEAM intraoperative radiotherapy combined with portal vein infusion chemotherapy for treating hepatocellular carcinoma with portal vein tumor thrombus. BMC Surg. 2020;20(1):174. doi:10.1186/s12893-020-00836-2
41. Lu J, Zhang XP, Zhong BY, et al. Management of patients with hepatocellular carcinoma and portal vein tumour thrombosis: comparing east and west. Lancet Gastroenterol Hepatol. 2019;4(9):721–730. doi:10.1016/S2468-1253(19)30178-5
42. Ciabattoni A, Gregucci F, Fastner G, et al. IOERT versus external beam electrons for boost radiotherapy in stage I/II breast cancer: 10-year results of a Phase III randomized study. Breast Cancer Res. 2021;23(1):46. doi:10.1186/s13058-021-01424-9
43. Siva S, Louie AV, Kotecha R. Stereotactic body radiotherapy for primary renal cell carcinoma: a systematic review and practice guideline from the International Society of Stereotactic Radiosurgery (ISRS). Lancet Oncol. 2024;25(1):e18–e28. doi:10.1016/S1470-2045(23)00513-2
44. Fastner G, Gaisberger C, Kaiser J. ESTRO IORT Task Force/ACROP recommendations for intraoperative radiation therapy with electrons (IOERT) in breast cancer. Radiother Oncol. 2020;149:150–157. doi:10.1016/j.radonc.2020.04.059
45. Yang Y, Hou X, Kong S, et al. Intraoperative radiotherapy in breast cancer: alterations to the tumor microenvironment and subsequent biological outcomes (Review). Mol Med Rep. 2023;28(6). doi:10.3892/mmr.2023.13118
46. Vaidya JS, Bulsara M, Baum M. Long term survival and local control outcomes from single dose targeted intraoperative radiotherapy during lumpectomy (TARGIT-IORT) for early breast cancer: TARGIT-A randomised clinical trial. BMJ. 2020;370:m2836. doi:10.1136/bmj.m2836
47. Schaub SK, Apisarnthanarax S, Price RG, et al. Functional Liver Imaging and Dosimetry to Predict Hepatotoxicity Risk in Cirrhotic Patients With Primary Liver Cancer. Int J Radiat Oncol Biol Phys. 2018;102(4):1339–1348. doi:10.1016/j.ijrobp.2018.08.029
48. Giudicelli H, Andraud M, Wagner M, et al. Portal-hypertension features are associated with ascites occurrence and survival in patients with hepatocellular carcinoma treated by external radiotherapy. United Eur Gastroenterol J. 2023;11(10):985–997. doi:10.1002/ueg2.12488
49. Kim H, Lim DH, Paik SW. Predictive factors of gastroduodenal toxicity in cirrhotic patients after three-dimensional conformal radiotherapy for hepatocellular carcinoma. Radiother Oncol. 2009;93(2):302–306. doi:10.1016/j.radonc.2009.05.017
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Histological Severity of Cirrhosis Influences Surgical Outcomes of Hepatocellular Carcinoma After Curative Hepatectomy
Liang BY, Gu J, Xiong M, Zhang EL, Zhang ZY, Lau WY, Wang SF, Guan Y, Chen XP, Huang ZY
Journal of Hepatocellular Carcinoma 2022, 9:633-647
Published Date: 23 July 2022
Clinical-Radiological Characteristic for Predicting Ultra-Early Recurrence After Liver Resection in Solitary Hepatocellular Carcinoma Patients
Wang X, Yu Y, Tao Y, Wang Y, Zhang C, Cui Y, Zhou Y
Journal of Hepatocellular Carcinoma 2023, 10:2323-2335
Published Date: 21 December 2023
Portal Venous and Hepatic Arterial Coefficients Predict Post-Hepatectomy Overall and Recurrence-Free Survival in Patients with Hepatocellular Carcinoma: A Retrospective Study
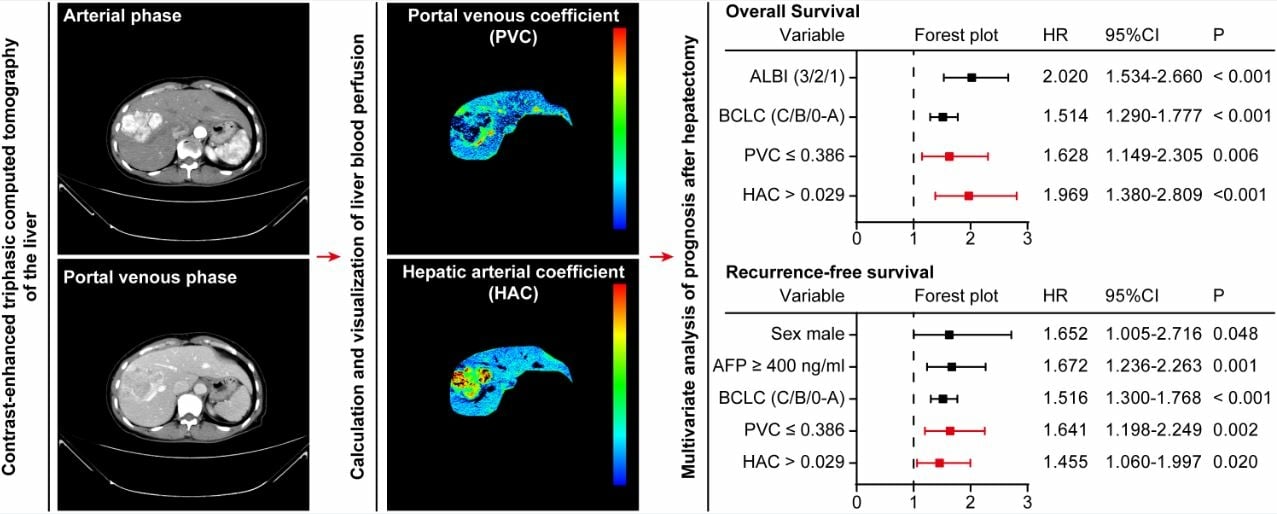
Li YK, Wu S, Wu YS, Zhang WH, Wang Y, Li YH, Kang Q, Huang SQ, Zheng K, Jiang GM, Wang QB, Liang YB, Li J, Lakang Y, Yang C, Li J, Wang JP, Kui X, Ke Y
Journal of Hepatocellular Carcinoma 2024, 11:1389-1402
Published Date: 9 July 2024
Combined Bone Mineral Density (BMD) and Monocyte-to-Lymphocyte Ratio (MLR) Predicts Recurrence and Prognosis in Hepatocellular Carcinoma Patients Following Liver Resection
He ZJ, Hu T, Zhang ZS, Wang TC, Huang W
Risk Management and Healthcare Policy 2024, 17:2741-2754
Published Date: 9 November 2024
Pan-Immune-Inflammation Value as a Prognostic Biomarker for Hepatocellular Carcinoma Patients Undergoing Hepatectomy
Fu H, Wang Y, Xiang B
Journal of Inflammation Research 2025, 18:6411-6425
Published Date: 20 May 2025