")
Back to Journals » Advances in Medical Education and Practice » Volume 16
Enhancing Pediatric Interns’ Clinical Skills Through Simulation-Based Training
Authors Ba H, Xu L , Peng H, Gu Y, Li Y, Jiang X, Li X, Li S
Received 21 March 2025
Accepted for publication 2 July 2025
Published 10 July 2025 Volume 2025:16 Pages 1209—1216
DOI https://doi.org/10.2147/AMEP.S524656
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Hongjun Ba,* Lingling Xu,* Huimin Peng, Yufen Gu, Yijuan Li, Xiaoyun Jiang, Xiaoyu Li, Shujuan Li
Pediatric Department, The First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, 510080, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoyu Li, Email [email protected] Shujuan Li, Email [email protected]
Background: Situational simulation teaching enhances students’ practical skills and clinical decision-making by replicating real-world scenarios. Pediatric practice often involves complex, dynamic situations, making it crucial for students to gain experience in a controlled environment where repeated practice can develop clinical expertise.
Objective: This study aims to evaluate the effectiveness of situational simulation in pediatric clinical practice by comparing its impact on trainees’ skills with that of conventional teaching methods.
Methods: A total of 52 pediatric trainees were randomly assigned to two groups: one participating in situational simulation training and the other receiving traditional instruction over a six-week period. A mixed-method approach, including formal assessments and Mini-Clinical Evaluation Exercises (Mini-CEX), was used to assess knowledge, clinical abilities, and overall competencies. A feedback survey was also administered to the simulation group to evaluate the impact of simulation-based training on their learning outcomes.
Results: Theoretical exam performance was comparable between both groups, with no significant difference (p > 0.05). However, the situational simulation group showed significant improvements in key skills compared to the traditional group: medical history taking (26.92% vs 69.23%, p = 0.005), clinical judgment (19.23% vs 46.15%, p = 0.011), doctor-patient communication (26.92% vs 61.54%, p = 0.025), and overall clinical competence (19.23% vs 57.69%, p = 0.009). The simulation group also reported higher satisfaction and demonstrated superior competency in practical assessments.
Conclusion: This study confirms that situational simulation effectively improves pediatric clinical skills, especially in practical competence and patient communication. The findings support further integration of simulation-based teaching into pediatric training programs to enhance clinical readiness and confidence.
Keywords: situational simulation teaching, pediatric clinical training, medical competencies, medical training, mini-clinical assessment
Introduction
The primary goal of medical education is to cultivate healthcare professionals with a solid theoretical foundation and strong clinical skills.1 However, traditional teaching models often fail to sufficiently prepare students for the complexities of real-world clinical practice, particularly in pediatrics, where students must navigate intricate and unique cases requiring advanced clinical decision-making and practical skills.2
Situational simulation teaching, an innovative pedagogical approach, replicates real-life clinical environments, enabling students to practice in conditions that closely mimic actual medical settings.3 This method allows learners to refine their clinical skills, improve decision-making capabilities, and build confidence through repeated practice. The key advantage is that it provides a controlled, safe environment where mistakes can be corrected without compromising patient safety, thus fostering a deeper learning experience.4
In recent years, situational simulation teaching has gained widespread acceptance in medical education, showing significant success in fields such as emergency care, nursing, and surgery.5,6 These areas have demonstrated improvements in both practical competencies and patient outcomes as a result of simulation-based training. Despite these advancements, research on its specific application and effectiveness in pediatric clinical practice remains limited, leaving a gap in understanding how this method can be optimized for pediatric education.
This study intends to address this gap by thoroughly evaluating the application and effectiveness of situational simulation teaching in pediatric clinical practice. Through this research, we aim to verify its potential in enhancing pediatric trainees’ clinical competencies, offering valuable insights for medical educators, and laying the groundwork for optimizing pediatric clinical teaching models.
Subjects and Study Design
Subjects
This study assessed the effect of situational simulation-based teaching on the clinical abilities of 52 medical interns in the five-year program at the First Affiliated Hospital of Sun Yat-sen University, between February 2023 and August 2024. The cohort, consisting of 26 male and 26 female interns, was randomly allocated to two groups through a computer-generated randomization process. Each group, comprising 26 students, was allocated to either the situational simulation group or the conventional instruction group for a six-week pediatric internship. Stratified allocation was applied according to participants’ initial clinical assessment scores to ensure comparability between the groups.
Study Design
This study utilized an experimental design with a control group and blinded assessment to evaluate the impact of two teaching methods. A total of 52 interns were randomly allocated to one of two groups: the situational simulation teaching group (n = 26) and the traditional teaching group (n = 26). The sample size of 52 participants (26 in each group) was determined based on a power calculation performed using G*Power software.7 With an expected medium effect size (Cohen’s d = 0.5), an alpha level of 0.05, and a desired power of 0.80, the sample size of 52 was sufficient to detect significant differences between the two groups.
Participants were randomly allocated to either the situational simulation teaching group or the traditional teaching group using a computer-generated randomization sequence. To ensure allocation concealment, the randomization sequence was stratified based on participants’ initial clinical assessment scores. The allocation sequence was stored in a secure, password-protected file, and the research staff responsible for enrolling participants were blinded to the group allocation until the moment of assignment. This stratified randomization ensured comparability between the groups in terms of clinical assessment scores, while maintaining the blinding process to prevent allocation bias. No substantial differences were detected between the groups in terms of gender, age, or initial clinical assessment scores (p > 0.05). The simulation group participated in training through simulated clinical scenarios, while the conventional group underwent standard bedside instruction (as illustrated in Figure 1).
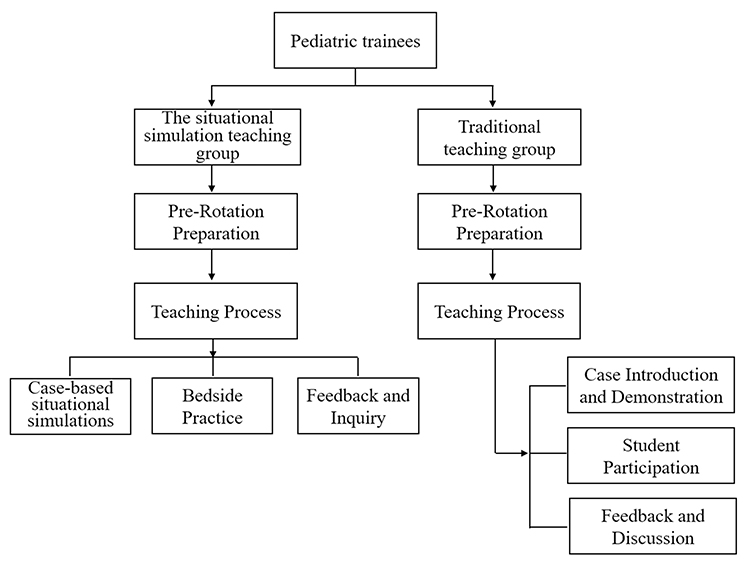 |
Figure 1 Experimental design and process chart. |
Both groups were exposed to the same pediatric case scenarios, including Kawasaki disease, pneumonia, congenital heart disease, diarrhea, and febrile convulsions. All participants were granted equal access to identical learning resources, trainers, and course intensity. Both groups used the same key textbook, the 9th edition of Pediatrics, Issued by the People’s Health Publishing House.
The study received certification from the ethics advisory board, and all participants provided informed agreement. Extra care was taken to assure the confidentiality of pediatric patient data used in the training scenarios.
Teaching Implementation
Traditional Teaching Group
Preparation Before Rotation
Teachers crafted case scenarios that represented common pediatric conditions, integrating the latest updates on diagnostic criteria and treatment strategies. Multimedia presentations were developed to highlight the clinical features, diagnostic guidelines, and therapeutic approaches for all diseases.
Teaching Framework
The teaching framework throughout the rotation period was structured in three distinct phases:
Case Presentation and Showcase
Each session started with a comprehensive overview of medical cases, where instructors explained the diagnostic process and emphasized essential skills in history-taking and physical assessment techniques.
Student Engagement
Students took an active role in conducting patient interviews and performing physical examinations, under the observation of the instructor. In pediatric cases, particularly for infants, patient histories were provided by the guardians.
Feedback and Discussion
After every session, teachers delivered individualized comments on student performance and led a discussion to address any questions, promoting an engaging and thoughtful learning atmosphere.
Situational Simulation Training Group
Course Plan for Situational Simulation Teaching in Pediatric Clinical Internship
The objective of this course is to enhance pediatric interns’ clinical skills, focusing on non-operational competencies like history taking, patient education, image interpretation, and interprofessional communication. Twenty-six pediatric interns will participate in the simulation group for six weeks, while the control group receives traditional teaching. The course includes one simulation session per week, covering 6 cases, with each session lasting 30 minutes and involving pairs of students. The implementation phases consist of preparation (acquiring foundational knowledge), briefing (providing key information and learning outcomes), simulation activity (engaging in realistic clinical scenarios with standardized patients), feedback (immediate post-simulation performance review), debriefing (consolidating learning and reflection), and evaluation (assessing performance against learning objectives).
The course content involves effective communication for comprehensive medical histories, patient education on diseases, treatments, and home care, and reading and interpreting pediatric imaging studies. Sample cases include managing Kawasaki disease with history taking, educating on congenital heart disease care, and interpreting imaging for pediatric bronchopneumonia. This structured, simulation-based approach ensures pediatric interns effectively master and apply key clinical skills.
The simulation cases are meticulously chosen and designed to mirror common pediatric scenarios that interns are likely to encounter. The cases and their scripts have been reviewed and approved by three pediatric teaching experts, each with over 15 years of experience in clinical teaching. This ensures the scenarios are realistic, educationally effective, and aligned with current pediatric practices. For detailed examples of the simulation scenarios used in this course, please see Supplementary Attachment 1.
Assessment Methods
The interns’ performance after the rotation was assessed using three evaluation methods:
Pediatric Knowledge Exam
Both groups participated in an identical closed-book test, designed to assess their theoretical understanding of pediatrics, guaranteeing uniformity in cognitive evaluation.
Mini-CEX Assessment
The Mini-CEX, a generally acknowledged tool for evaluating clinical skills,7,8 was used to assess practical competencies. Students took medical histories from pediatric patients’ guardians and conducted physical exams on infants, under instructor supervision. The Mini-CEX assessed students across seven criteria, using a nine-point scale:
History Taking
Accuracy in gathering patient history, responding to non-verbal cues, and demonstrating empathy.
Physical Examination
Competence in conducting exams in an organized manner, maintaining patient privacy, and managing discomfort.
Professionalism
Respect, compassion, ethical standards, and confidentiality.
Clinical Judgment
Evaluates the student’s ability to choose and perform relevant diagnostic tests, as well as evaluate the potential pros and cons of various treatment modalities.
Doctor-Patient Communication
Clarity in interpreting medical tests, obtaining consent, and educating patients.
Organizational Efficiency
Skill in prioritizing patient care and effectively utilizing resources.
Overall Competence
Integration of clinical knowledge and overall patient care effectiveness.
The Mini-CEX scores were categorized into three levels: 1–3 points: Below Expectations;4–6 points: Meeting Expectations;7–9 points: Exceeding Expectations. All evaluations were carried out by a single evaluator to ensure consistency.
Situational Simulation Teaching Method Feedback Survey
A feedback survey was conducted exclusively for the simulation group to evaluate the Teaching efficacy of the simulation method. The survey, with a Cronbach’s Alpha coefficient of 0.822 (indicating strong reliability), assessed various items such as active learning engagement, communication skills, feedback Quality, and overall Satisfaction. A Likert scale, with values from 1 (strongly disagree) to 5 (strongly agree), was used in the survey for a variety of statements.
To improve the validity of the satisfaction survey, it was pilot tested with a similar cohort to refine question clarity and response consistency.
The survey assessed the following items:
Engagement
“The situational simulation teaching is engaging and makes me more involved in the learning process”.
Development of Clinical Skills
“The situational simulation teaching enables me to develop my clinical skills effectively”.
Communication Skills Improvement
“I feel more confident in communicating with patients due to the situational simulation teaching”.
Feedback Quality
“The situational simulation teaching provides me with appropriate feedback on my performance”.
Overall Satisfaction
“I am generally satisfied with the overall effectiveness of the situational simulation teaching method”.
Statistical Analysis
Using SPSS (version 25.0), the data were processed, and descriptive statistics are described as mean ± standard deviation (x ± s). To compare continuous variables between groups, independent t-tests were conducted, whereas categorical variables are expressed as frequencies and percentages (n [%]), applying chi-square tests as needed. A P-value of less than 0.05 was deemed statistically differentiated. To minimize bias, all Mini-CEX evaluators were kept unaware of group allocation.
Result
Theoretical Knowledge Exam Scores
The scores on knowledge test were comparable in both groups. The situational simulation training group had a mean score of 90.23 ± 2.17, while the traditional training group scored 90.18 ± 2.38. No substantial differences were found between the groups in the independent t-test (p > 0.05), suggesting that both teaching methods were equally effective in supporting theoretical learning.
Mini-CEX Evaluation Results
All participants finished the Mini-CEX assessment in an average of 36 ± 0.5 minutes, with feedback after evaluation averaging 6.6 ± 0.4 minutes per student. Compared to the traditional training group, the situational simulation training group demonstrated statistically significant improvements in key skills, including medical history taking (meets expectation: 7 participants [26.92%] vs 18 participants [69.23%], p = 0.005), clinical judgment (meets expectation: 5 participants [19.23%] vs 12 participants [46.15%], p = 0.011), doctor-patient communication (meets expectation: 7 participants [26.92%] vs 16 participants [61.54%], p = 0.025), and overall clinical competence (meets expectation: 5 participants [19.23%] vs 15 participants [57.69%], p = 0.009), as assessed using the chi-square test. A thorough comparison of CEX scores among the two groups was shown in Figure 2 and Table 1.
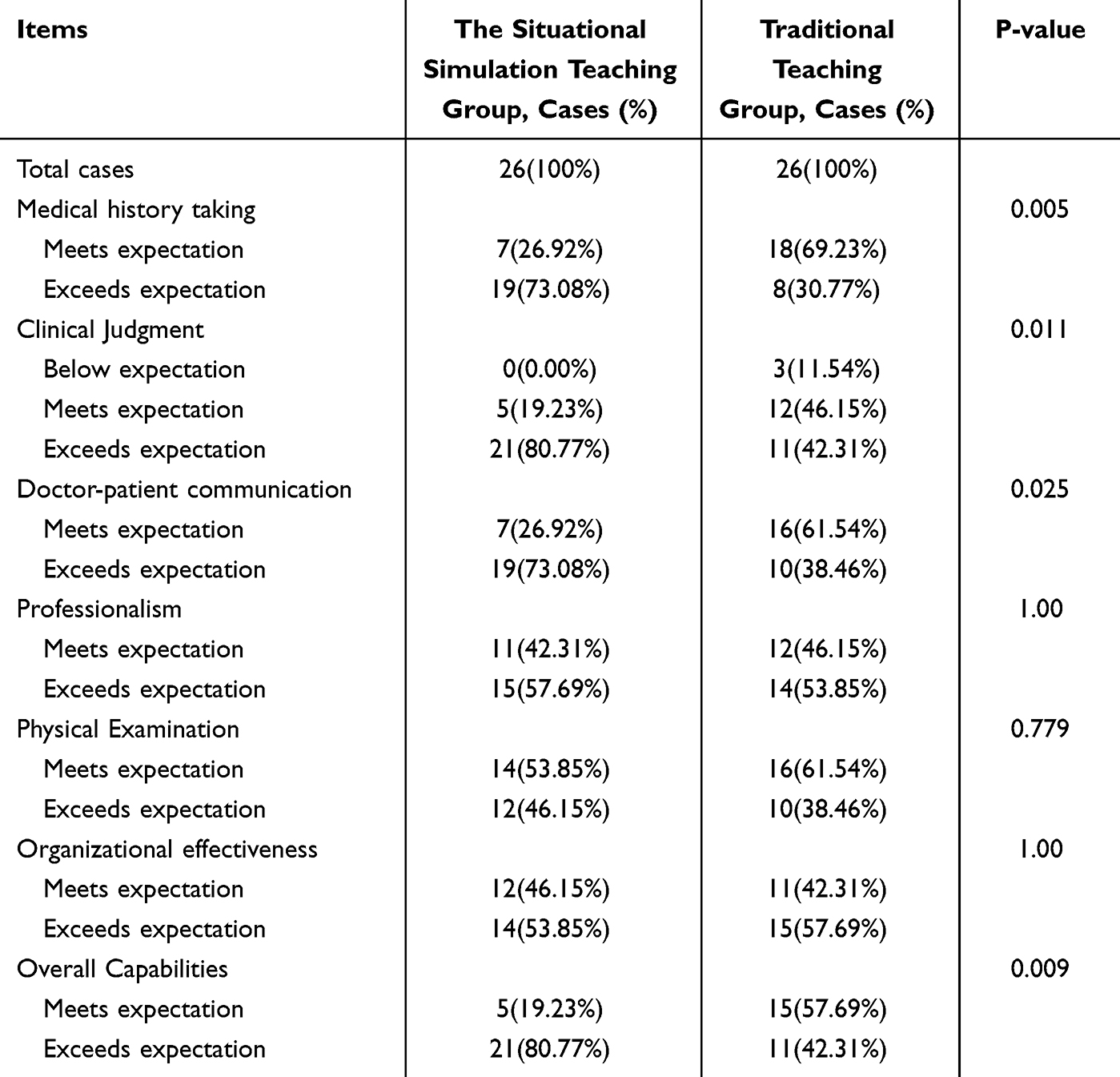 |
Table 1 The Mini-CEX Score Metrics for Each Group |
 |
Figure 2 Mini-CEX scale scores comparison among both groups. (A) Situational simulation teaching group; (B) Traditional teaching group. |
Satisfaction Assessment Results
Feedback from the situational simulation training group was overwhelmingly positive. Trainees expressed high satisfaction and interest in the method, with no reports of dissatisfaction (Table 2). The survey results particularly highlighted active engagement and improvements in clinical skills as the most appreciated aspects of the simulation-based teaching approach.
 |
Table 2 Students Satisfaction Evaluation of the Situational Simulation Teaching Group (n = 26) |
Discussion
The findings of this research emphasize the significant influence of situational simulation teaching on pediatric clinical probation, highlighting its potential as a valuable educational strategy in medical training. The results suggest that situational simulation not only enhances students’ clinical skills but also plays a crucial role in their overall development as future pediatricians.8,9 This approach allows for the repetitive practice of clinical skills across a range of scenarios, which is essential for mastering skills in a controlled, risk-free environment.
A notable observation is the marked improvement in students’ clinical decision-making abilities. In pediatric settings, where patient conditions can change rapidly, the ability to make quick and accurate decisions is crucial.10,11 Simulation-based teaching prepares students for these real-world situations by providing them with opportunities to engage in decision-making processes, thereby fostering an adaptive mindset. This preparation helps students reduce cognitive load in clinical situations, enhancing their confidence and competence when faced with real-life challenges.
Moreover, the study demonstrates that situational simulation significantly enhances students’ communication skills. Effective communication is essential in clinical practice, influencing students’ ability to interact with patients and families, perform procedures accurately, and collaborate efficiently with healthcare teams.12,13 The safe, controlled environment provided by simulations allows students to practice and refine their communication techniques without the pressure of real-world consequences. By engaging in simulations, students develop a solid foundation in interpersonal skills, which translates into improved performance during clinical rotations. Enhanced communication skills not only improve patient outcomes but also contribute to increased patient satisfaction and stronger interprofessional relationships.14 This underlines the importance of integrating situational simulation into pediatric clinical training to cultivate well-rounded, competent healthcare professionals.
Additionally, the study highlights the enhancement of teamwork among students. Pediatric care often requires a multidisciplinary approach, making effective teamwork essential for high-quality care delivery.15 The simulation scenarios in this study were designed to replicate real-world pediatric cases, promoting collaboration among healthcare professionals. These exercises not only refined students’ technical skills but also developed critical communication and teamwork abilities, which are crucial in pediatric care.16
Despite the positive outcomes, several limitations must be acknowledged. First, while the study highlights the immediate benefits of situational simulation, it does not evaluate the long-term retention of these skills or their applicability to real clinical practice. Future research should focus on assessing the sustainability of skills acquired through simulation, as well as their correlation with clinical performance in actual pediatric settings. Second, the reliance on self-reported measures of confidence and competence introduces a potential source of bias. While practical assessments were used to mitigate this, future studies should incorporate more objective measures of clinical performance, such as direct observation or standardized patient assessments, to provide a more thorough evaluation of the effectiveness of simulation-based teaching.
In conclusion, this study underscores the efficacy of situational simulation teaching in pediatric clinical probation. By providing a realistic yet controlled environment for students to practice and refine their skills, this teaching method enhances clinical decision-making, boosts confidence, and promotes teamwork. As medical education evolves, situational simulation teaching should be more widely integrated across various disciplines to better prepare students for the complexities of clinical practice, especially in pediatric care.
Human Ethics and Consent to Participate Declarations
The approval was granted by the Committee on Ethics of The First Affiliated Hospital, Sun Yat-sen University. All subjects provided acknowledgment of consent, with particular attention to data protection concerns considering the inclusion of child health data.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
Guangdong Provincial Clinical Teaching Base Teaching Reform Research Project (Yue Jiao Gao Han [2023] No. 32).
Disclosure
All authors report no conflicts of interest in this work.
References
1. Hur Y, Lee K. Identification and evaluation of the core elements of character education for medical students in Korea. J Educ Eval Health Prof. 2019;16:21. doi:10.3352/jeehp.2019.16.21
2. Bright TJ, Wong A, Dhurjati R, et al. Effect of clinical decision-support systems: a systematic review. Ann Intern Med. 2012;157(1):29–43. doi:10.7326/0003-4819-157-1-201207030-00450
3. Kim J, Park JH, Shin S. Effectiveness of simulation-based nursing education depending on fidelity: a meta-analysis. BMC Med Educ. 2016;16:152. doi:10.1186/s12909-016-0672-7
4. Yu M, Jiang L, Yang L, Liu S. Application of situational simulation teaching method in clinical nursing teaching. Minerva Med. 2022;113(1):218–220. doi:10.23736/S0026-4806.21.07519-4
5. Blätzinger M. Simulation in surgery. Chirurgie. 2023;94(4):330–332. doi:10.1007/s00104-023-01841-w
6. Peng M, Su N, Hou R, et al. Evaluation of teaching effect of first-aid comprehensive simulation-based education in clinical medical students. Front Public Health. 2022;10:909889. doi:10.3389/fpubh.2022.909889
7. Kang H. Sample size determination and power analysis using the G*Power software. J Educ Eval Health Prof. 2021;18:17. doi:10.3352/jeehp.2021.18.17
8. Weller JM, Nestel D, Marshall SD, Brooks PM, Conn JJ. Simulation in clinical teaching and learning. Med J Aust. 2012;196(9):594. doi:10.5694/mja10.11474
9. Harder BN. Use of simulation in teaching and learning in health sciences: a systematic review. J Nurs Educ. 2010;49(1):23–28. doi:10.3928/01484834-20090828-08
10. Yousef N, Moreau R, Soghier L. Simulation in neonatal care: towards a change in traditional training? Eur J Pediatr. 2022;181(4):1429–1436. doi:10.1007/s00431-022-04373-3
11. Khan K, Pattison T, Sherwood M. Simulation in medical education. Med Teach. 2011;33(1):1–3. doi:10.3109/0142159X.2010.519412
12. Lee Chang A, Dym AA, Venegas-Borsellino C, et al. Comparison between simulation-based training and lecture-based education in teaching situation awareness. A randomized controlled study. Ann Am Thorac Soc. 2017;14(4):529–535. doi:10.1513/AnnalsATS.201612-950OC
13. Baty A, Matis TI, Griswold J. A simulation study on the association of HRO communication patterns and surgical team performance. Int J Qual Health Care. 2022;34(2):mzac028. doi:10.1093/intqhc/mzac028
14. Foronda C, Gattamorta K, Snowden K, Bauman EB. Use of virtual clinical simulation to improve communication skills of baccalaureate nursing students: a pilot study. Nurse Educ Today. 2014;34(6):e53–e57. doi:10.1016/j.nedt.2013.10.007
15. Weigl M, Heinrich M, Rivas J, et al. Teamwork and mental workload in postsurgical pediatric patient handovers: prospective effect evaluation of an improvement intervention for OR-PICU patient transitions. Eur J Pediatr. 2023;182(12):5637–5647. doi:10.1007/s00431-023-05241-4
16. Hepps JH, Yu CE, Calaman S. Simulation in medical education for the hospitalist: moving beyond the mock code. Pediatr Clin North Am. 2019;66(4):855–866. doi:10.1016/j.pcl.2019.03.014
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.