")
Back to Journals » Advances in Medical Education and Practice » Volume 15
Evaluation of the Learning Curve of Endotracheal Intubation with Videolaryngoscopes: McGrathMAC, UESCOPE, and Airtraq by Young Anesthesiology Residents - Randomized, Controlled, Blinded Crossover Study
Authors Ratajczyk P, Kluj P, Wasiak K, Strzalek J, Kolodziejska K, Gaszynski T
Received 11 September 2024
Accepted for publication 13 December 2024
Published 25 December 2024 Volume 2024:15 Pages 1299—1312
DOI https://doi.org/10.2147/AMEP.S486331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Pawel Ratajczyk,1 Przemyslaw Kluj,1 Krzysztof Wasiak,1 Jeremi Strzalek,1 Karolina Kolodziejska,2 Tomasz Gaszynski1
1Department of Anesthesiology and Intensive Therapy, Medical University of Lodz, Lodz, Poland; 2II Department of Cardiology, Central University Hospital, Medical University of Lodz, Lodz, Poland
Correspondence: Pawel Ratajczyk; Tomasz Gaszynski, Email [email protected]; [email protected]
Background: Videolaryngoscopes increased the safety of patients requiring endotracheal intubation. Their particular beneficiaries are healthcare providers inexperienced in intubation. We compared the learning curve of McGrath, UESCOPE, and Airtraq VLs among the first-year anesthesiology residents.
Methods: Sixteen residents were qualified for the study, none of whom has ever before used any VL nor had any experience with the Macintosh laryngoscope. The study was conducted during anesthesia without anticipated intubation difficulties and included 288 adult patients with BMI < 25 and ASA ≤ II, without visible intubation difficulties. It was a randomized, controlled, and blinded crossover study. Each resident performed six intubations with a given VL in randomized order.
Results: There were no statistically significant differences in patient characteristics. In McGrath there was observed significant improvement of intubation time, confirmed intubation time, ease, POGO scale, effective intubation, thyroid pressure application, and intubation trauma. Intubation efficacy increased from 12 (75%) at first attempt, to 16 (100%) during third and following attempts. Residents used pressure 6 times (38%) during first attempt and 7 times (44%) during second attempt, and 1 (6%) at last attempt. McGrath traumatism was noticed in 4 (25%) patients at first two attempts, none during third and following attempts. In Airtraq, we observed a significant improvement of intubation time, time of confirmed intubation, force used, ease, effective intubation, and application of pressure to thyroid cartilage. Intubation efficacy increased from 10 (62%) during the first to 16 (100%) during the following attempts. Thyroid pressure was applied 7 times (44%) during first intubation and 0 times during the last two attempts. In the case of UESCOPE VL, we observed a significant improvement of intubation time, time of confirmed intubation, force used, and ease.
Conclusion: Results demonstrated that Airtraq VL having the best learning curve, and UESCOPE having the best first-time use. The results require confirmation in a larger study group. This study was approved on 14 November 2023 by the Medical University of Lodz Bioethics Committee (ref: RNN/160/23/KE).
Keywords: videolaryngoscopy, VL, learning curve, endotracheal intubation, residents, teaching
Introduction
The basic skill that every young anesthesiologist must master is endotracheal intubation.1 It determines the proper opening of airways and reduces the occurrence of complications related to anesthesia.2–4 Since the 1940s, the most common technique used to perform endotracheal intubation is direct laryngoscopy (DL) using a Macintosh blade (MAC).3 It involves direct visualization of the glottis using a laryngoscope and requires alignment of: the axis of the intubator’s eyes, the patient’s oral cavity, pharynx, larynx, and glottis. This is quite a difficult technique that requires constant improvement and constant practice.1,2 At the end of the 20th century, videolaryngoscopes (VL) appeared and gradually became more and more available, which are based on the technique of indirect laryngoscopy utilizing a camera.3,5 To perform endotracheal intubation in this case, it is not necessary to maintain the axis of the intubator’s line of sight and the patient’s glottis.5 The number of new VL models introduced is growing every year, therefore they are becoming more and more available and common in practice.3 In patients with suspected difficult airways, there is no doubt that utilizing a VL is connected with obtaining better visibility of the glottis, increasing the effectiveness of the first intubation attempt and less trauma to the mucous membrane than in the case of classic MAC.2,6 On the other hand, it is worth noting, that better visibility of the glottis does not guarantee easy intubation.5,7,8 Guidelines of many anesthesiology societies recommend that all anesthesiologists be trained in the use of VL, so that they are widely accessible and always used in the event of intubation difficulties.3 Some societies even recommend using VL as the primary instrument in all cases of extramural intubation.9 For young anesthesiology residents, episodes of difficult airway management should be expected to occur more frequently than in experienced intubators.10 Therefore, it is necessary to implement the process of teaching them [using these devices] as soon as possible to try to eliminate cases of prolonged or ineffective intubation. This will reduce the number of potential complications and improve the safety of anesthesia, especially since the presence of a monitor and simultaneous view of the airway structures by the supervising and intubating person also allows for quick correction of errors made by those learning.5 This is particularly important because the greatest benefits are expected when VL are used by inexperienced intubators.7,10–14 The effectiveness of various VLs can vary significantly and may depend on prior experience and individual intubator predispositions, particularly on the level of visual-motor coordination.6,15 Both the learners themselves and, even more so, experienced anesthesiologists supervising them often do not know about the presence of many of these variables.5 Therefore, at the initial stage of training, it is necessary to choose a VL, among many available on the market, that will ensure the fastest learning curve for young anesthesiology residents. This will impact the speed of intubation and reduce the possibility of complications.2,10,16
In our study, we evaluated the learning curve of CL among young anesthesiology residents (first-year residents), who have previously not used VL, lacking experience using a classical MAC laryngoscope. For this study, we utilized one of the three VL’s available on the market, those being: Macintosh-style - McGrath MAC (MGT), Hyperangulated - UESCOPE (UES) and Channelled - Airtraq (ARQ).14 The selected VLs are among the most frequently used in everyday clinical practice.17 Assessment of the learning curve in this group of intubators and the selection of the most optimal VL are important because currently available VLs do not ensure 100% intubation effectiveness and are not a cure for all airway problems in patients. Observational studies have shown that the effectiveness of intubation using VL among all healthcare providers ranges from 85% to 100%, and the effectiveness of first-time intubation ranges from 51% to 100%.18
The aim of our study was to assess the learning curve of VL subjects, based on the results obtained, by young anesthesiology residents. We presented a research hypothesis that the speed of learning videolaryngoscopes among young anesthesiology residents is not influenced by the device they start learning with. The primary outcome of the study was successful intubation in the shortest time.
Materials and Methods
Study Settings
The study was approved by the Bioethics Committee of the Medical University of Lodz (No RNN/160/23/KE from 14.11.2023). It was carried out in the Central Operating Block of the University Clinical Hospital No. 1. Norbert Barlicki in Łódź. VL learning curve assessment was performed among 16 young anesthesiology residents (first year of specialization) who had never used VL before and had no experience with clinical MAC. Each assessed resident performed six intubations with a given VL in a randomized order. For the study, we used one of the three types of VL available on the market, namely: Macintosh-style - McGrath MAC (MGT) (Aircraft Medical ltd. Edinburgh, Great Britain), Hyperangulated - UESCOPE (UES) (Zhejiang UE Medical Corp. Zhejiang, China), Channelled - Airtraq (ARQ) (Prodol Meditec S.A., Vizcaya, Spain). The study was a randomized, controlled, blinded crossover study. No. 7 Covidien LLc endotracheal tubes, Hampshire Street, Mansfield, MA 02048 USA, were used for intubation. An intubation guide from Sumi ® sp. z o.o. ul. was prepared as a stylet for the endotracheal tube Drobiarska 35, 05–070 Sulejówek, Poland. In each case, the endotracheal tubes were used in conjunction with standard lubricant. In the case of channelled VL ARQ, in order to standardize the examination protocol, it would be possible to use an intubation guide located in the lumen of the endotracheal tube at the intubator’s request; contrary to the manufacturer’s recommendations.
The order in which VLs were used was randomly selected each time using sealed opaque envelopes. The blocked randomization strategy was generated using the Randomizer program (randomizer.org). To ensure the proper course of the study and safety of patients, oversight was provided by two anesthesiologists with over 20 years of experience.
Before partaking in the study, all participants listened to a 30-minute lecture on the structure of VLs, the rules of using them, as well as the anatomical structure and the method and technique of intubation. After the presentation, the instructor demonstrated the correct intubation for each of the 3 VLs tested. Then, under the supervision of the instructor, the young residents participated in the workshop portion, where they had the opportunity to intubate each of the examined VL manikins (Laerdal Airway Management Trainer Stavanger Norway with a universal level of difficulty) placed on the operating table at the optimal height for each participant in the study. If necessary, participants of the study were able to use the standard intubation guide and apply pressure to the thyroid cartilage to improve visualization of the glottis and make intubation of the patient easier. The study included adult patients (over 18 years of age), with BMI <25 and ASA ≤ II, without visible intubation difficulties, who qualified for planned surgical procedures under general anesthesia with endotracheal intubation, who gave informed, voluntary consent to participate in the study. Patients: with BMI ≥ 25, ASA III, and above, Mallampati scale ≥3, with an oral fissure opening less than 4 cm, with injuries of the cervical spine or for surgery on the cervical spine, with increased intraocular and intracranial pressure, with vascular changes in the CNS and other parts of the body, with diagnosed pathology of the respiratory tract, after surgery of the mouth, throat, larynx, during pregnancy, with indications for urgent surgical intervention, who do not consent to participate in the study will be excluded from participation in the study. The following were measured in patients: weight, height, BMI, mouth opening, Mallampati scale. To assess the visibility of the glottis, the Cormack-Lehane scales and the percentage of glottal opening (POGO scale) were used, which allows for a better assessment of the entry into the airway in patients with partial glottic visibility, which may also provide a better assessment of the results obtained by the tested VL.
After transporting the patient to the operating theatre, the envelope was opened, and the patient was qualified for the first intubation with one of the three VLs: MGT, UES, or ARQ. All patients during induction of anesthesia were under standard monitoring: heart rate (HR), non-invasive blood pressure measurement (NIPC), blood saturation (SpO2). Those qualified for the study were subjected to a standardized technique of induction of anesthesia: preoxygenation 100% oxygen for 3 min, fentanyl (FNT) 1.5 µg/kg iv, Propofol 2.5 mg/kg iv, and rocuronium bromide 0.6 mg/kg iv after confirming adequate ventilation through the face mask. Bag-mask ventilation with 100% oxygen and 2% inhaled sevoflurane was continued for 3 min. After achieving complete neuromuscular blockade, confirmed by the loss of the entire sequence of four responses using a peripheral nerve stimulator (Innervator Constant Current Peripheral Nerve Stimulator, Fisher & Paykel Health Care System, New Zealand), the intubator began to perform endotracheal intubation with one of the three randomly selected VLs. Once the patient was intubated, they were connected to an anesthesia machine, and anesthesia was continued. If the patient was not intubated, the attempt was recorded as unsuccessful and the patient was intubated by an anesthesiologist with twenty years of clinical experience who supervised the entire course of anesthesia. The intubation attempt was interrupted and recorded as unsuccessful if, at any stage, the anesthesiologist supervising the patient’s safety considered that the patient’s life and/or health could be threatened. The following data was registered in a pseudonymized manner for all simulations: intubation time (Ti) - from the moment the VL blade is placed between the patient’s teeth until the patient is intubated, total intubation time (Tt) - from the moment of placing the laryngoscope blade between the patient’s teeth to confirming the patient’s intubation by assessing chest respiratory movements and exhaled CO2 level, effectiveness of intubation (Ei) (yes/no) by assessing chest respiratory movements and expiratory CO2 level, instrument trauma - presence of blood-stained blood secretions on the VL blade after removing it from the patient’s mouth, assessment of the visibility of the glottal gap based on the Cormack-Lehane scale and the percentage of glottal opening scale (POGO scale), the use or not of a guide during intubation, and the need to put pressure on the thyroid cartilage. After completing the study, the intubators were also asked about their impressions: the force necessary to intubate the patient (on a scale from 1 to 10, where 1 - no strength, 10 - maximum force) and the ease of using the VL (on a scale from 1 to 6, where 1 - The greatest ease, 6 - The greatest difficulty). The obtained data were saved and subjected to statistical analysis.
The aim of our study was to assess the learning curve of VL subjects, based on the results obtained, by young anesthesiology residents.
Safety Conditions
In addition to the experienced team, all available devices were prepared for the intubation of patients with typical and difficult airways. Additionally, to prevent desaturation during endotracheal intubation, we used a high-flow nasal catheter. This method is used to extend the safe apnea time during endotracheal intubation. In the event of any difficulties and if the patient’s health and life were at risk, a second anesthesiologist with over 20 years of clinical experience supervising the patient’s safety could interrupt the examination at any stage of its duration and intubate the patient and connect him/her to an anesthesia machine. In addition, a set was prepared for the difficult airways with supraglottic devices, videolaryngoscopes and intubation guides. If intubation failed, Sugammadex was prepared to quickly reverse the neuromuscular blockade.
Statistical Analysis
Nominal data were presented as n (% of total) and tested using online tools: https://quantpsy.org/. As the distribution of all continuous variables was other than normal (Shapiro Wilk’s test <0.05), they were shown as median with interquartile range (IQR) and were further tested with Kruskal-Wallis test with Dunn’s post hoc test for the comparison of independent variables and The Friedman ANOVA with proper post hoc test otherwise. All calculations were made using Statistica 13.1PL (StatSoft, Tulsa, OK, USA). P < 0.05 was considered statistically significant unless otherwise stated.
Results
Sixteen first-year anesthesiology residents were asked to intubate 18 patients with 3 different laryngoscopes (McGrath, Airtraq, and UESCOPE) 6 times each. Laryngoscopes for every single intubation were selected randomly. Two hundred eighty-eight patients (164, 56.94% females) with a median age of 47.00 years (IQR:37.00–58.00) were enrolled in the study (see Figure 1 for inclusion and exclusion criteria and Tables 1 and 2 for further details).
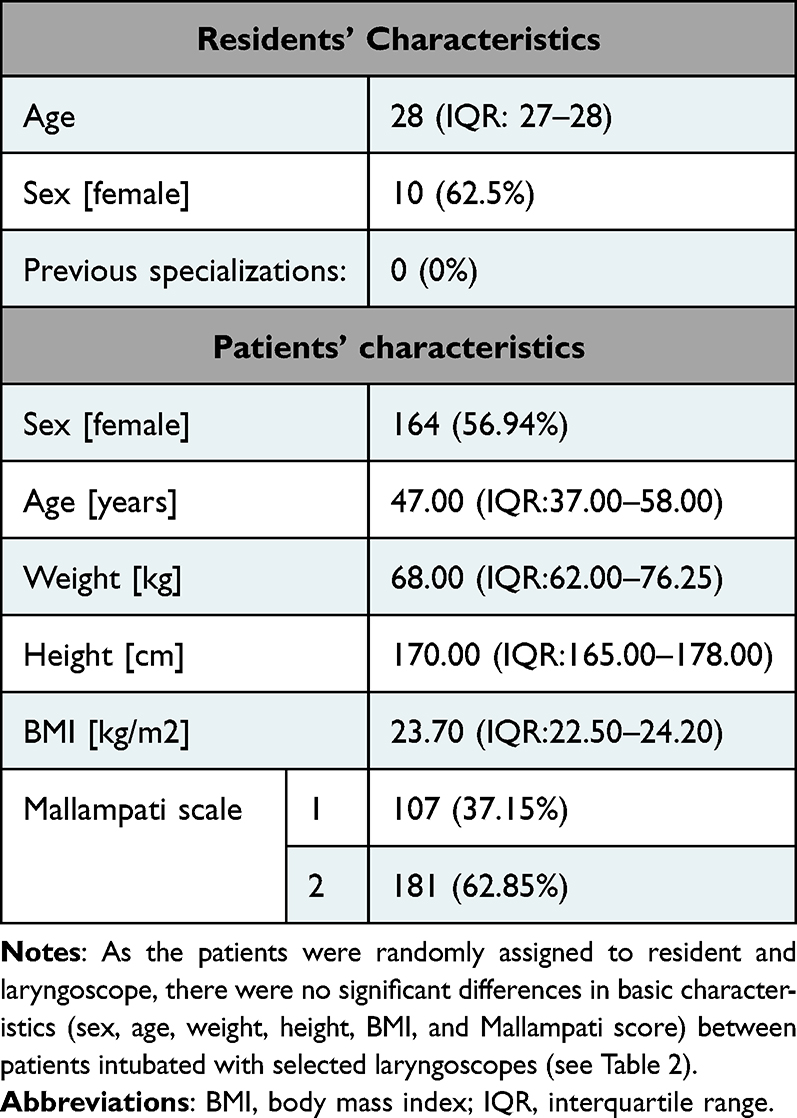 |
Table 1 The Study Group Characteristics |
 |
Table 2 The Differences in Basic Group Characteristics Between Groups of Patients Intubated with the Usage of Tested Laryngoscopes: McGrath, Airtraq, and UESCOPE |
 |
Figure 1 The study flow-chart. |
McGrath Learning Curve
Regarding McGrath laryngoscope, we observed significant improvement in intubation time (p < 0.001), time to confirm intubation (p < 0.001), ease of use (p = 0.001), POGO scale (p = 0.018), intubation effectiveness (p = 0.011), the need to use compression of the thyroid cartilage (p = 0.004), and intubation traumatism (p = 0.024). The differences for continuous variables are shown in Figure 2. Intubation effectiveness increased from 12 (75%) in the first to 16 (100%) in the third and subsequent intubations. Residents required usage of compression of the thyroid cartilage 6 times (38%) in the first and 7 times (44%) in the second attempt to 1 (6%) in the last one. Finally, intubation traumatism was observed in 4 (25%) patients during both the first and second intubation and none (0%) in the third and subsequent intubations.
 |
Figure 2 Significant differences in following parameters during intubations with the usage of McGrath laryngoscope: (A) intubation time, (B) time to confirm intubation, (C) easiness, (D) POGO. |
Airtraq Learning Curve
Regarding Airtraq laryngoscope, we observed significant improvement in intubation time (p < 0.001), time to confirm intubation (p < 0.001), used force (p < 0.001), easiness (p < 0.001), intubation effectiveness (p < 0.001), and the need to use of compression of the thyroid cartilage (p = 0.007) (Figure 3). Intubation effectiveness increased from 10 (62.5%) in the first to 16 (100%) in the third and subsequent intubations. The thyroid cartilage compression was used 7 times (44%) during the first and 0 (0%) in the latest two intubations with Airtraq.
 |
Figure 3 Significant differences in following intubations with the usage of Airtraq laryngoscope. (A) intubation time, (B) time to confirm intubation, (C) force, (D) easiness. |
 |
Figure 4 Significant differences in following parameters during intubations with the usage of UESCOPE laryngoscope. (A) intubation time, (B) time to confirm intubation, (C) force, (D) easiness. |
UESCOPE Learning Curve
Regarding UESCOPE laryngoscope, we observed a significant improvement in intubation time (p < 0.001), time to confirm intubation (p < 0.001), used force (p < 0.001), and ease of use (p < 0.001) (Figure 4).
Differences Between Used Laryngoscopes
We observed the following differences between the first usage of selected laryngoscopes: time to confirm intubation (p = 0.022), ease of use (p < 0.001), POGO (p = 0.025; see Figure 5), and the necessity to use laryngoscope guide (0.005).
 |
Figure 5 Significant differences between tested laryngoscopes during first intubation. Dependencies were first tested with the Kruskal–Wallis test and then confirmed in the Dunn test (p-values are presented in Figure). (A) time to confirm intubation, (B) easiness. (C) POGO. |
During the last intubation, the following differences were noted: intubation time (p = 0.019), time to confirm intubation (p = 0.002), force (p < 0.001; see Figure 6), and the necessity to use both thyroid cartilage compression (p = 0.018) and laryngoscope guide (p < 0.001).
 |
Figure 6 Significant differences between tested laryngoscopes during the last, sixth, intubation. Dependencies were first tested with the Kruskal–Wallis test and then confirmed in the Dunn test (p-values are presented in Figure). (A) intubation time, (B) time to confirm intubation, (C) force. |
Regarding, the improvement between the first and last intubation, we observed differences only in intubation easiness – the change was the biggest for Airtraq 2 (IQR: 1–2) vs UESCOPE 0 (IQR: 0–1) and McGrath 1 (IQR: 0–3; p-value of 0.0101 for Kruskal–Wallis test).
Discussion
There are many studies in the available literature, including meta-analyses, comparing the use of DL with different types of VL when used by different users: from experienced anesthesiologists to those with little or no experience in intubation.2,5,8,10,13–15 Older literature contains statements that VL have a significant advantage over DL only in the case of difficult airways.2 In the case of patients with normal airways, especially among experienced intubators, this difference does not exist or is only slightly marked in favor of VL.2 In recent years, the prevailing view is that VLs of all types probably reduce the rate of failed intubations while increasing the rate of successful first-time intubations.14 Thanks to these devices, it is also possible to obtain better visibility of the glottis in various patients and in various clinical situations. This applies to both patients intubated in the operating theater and in intensive care units.14,19 However, it is not possible to clearly indicate on the basis of meta-analyses which type of VL is better than another in patients with normal and difficult airways.8,10,18 Many authors believe that the less experienced in intubating a person, using a VL, the greater the benefit from their use because they provide better visibility of the glottis than DL.20
In literature, it can be found, based on small groups of respondents, indications that one VL may be better than another, and another model is more difficult to use than the next one and requires longer learning time to use it.15,21–23 In most cases, VLs were assessed by anesthesiologists with prior experience with MAC. These experiences and the different intubation technique used when using DL may have influenced the good effectiveness and positive feelings from the use of these VLs with a structure similar to the DL, and discredit those with a different structure.6 However, there is no literature comparing the learning curve of various VLs among young anesthesiology residents whose ability to use them was assessed during anesthesia for planned surgical procedures. In existing works, the reference point was always the MAC laryngoscope and not another VL. There is also no indication of which VL is most beneficial for use among these inexperienced intubators. This is particularly important because, due to their limited experience, representatives of this group of healthcare providers more often encounter intubation difficulties, and sometimes their first use of VL may decide about the patient’s life and health.24
According to this criterion, in our study, the fastest learning based on the fastest Ti and Tt (approximately 40s and 60s) in the first attempt is the UES. P with subsequent uses, these times are reduced to approximately 20s and 40s in the last—sixth attempt—respectively. At the same time, when used for the first time, it is the easiest VL to use, which also allows for better visualization on the POGO scale than MGT (and similar to ARQ). It is also the VL that requires the use of the least force when the research participant has learned to use it (sixth attempt). Pan has come to a similar conclusion, who found that UES increases the skills of inexperienced intubators. Pan demonstrated, that for emergency intubation using UES, differences between untrained and experienced providers were not statistically significant with respect to increased esophageal intubation rates, prolonged intubation times, and complications.12 According to other authors, UES provides a better view of the larynx, a higher percentage of successful intubation, shorter time of visualization of the larynx and intubation, and also reduced the need for pressure on the thyroid cartilage compared to DL and other VL.15
If we choose the learning curve as the criterion of usefulness for young anesthesiology residents, ie which of the VL data allows the intubator to learn the technique of using it the fastest in subsequent attempts and which of the tested devices allows obtaining the best parameters in the last, sixth intubation, then in this case the VL ARQ turned out to be the fastest to learn which allows to obtain a much shorter Ti time than UES and Tt shorter than MGT and UES. It is also VL, which in subsequent applications requires the use of less force but achieves similar visibility of the glottis. This is related to faster acquisition of skills in using it. Our data on the learning curve when using the ARQ are similar to those obtained by Di Marco, who showed that the ARQ has a better learning curve than the MAC for young anesthesiology residents and is also easier and faster to use than the DL.11 Similar conclusions were reached by Lu and Nowicki, who believe that among people with little or no experience in intubation, this VL provides a faster learning curve, faster and more effective intubation, reduces the risk of inserting the endotracheal tube into the esophagus, and reduces the risk of complications.25,26 Other authors believe that this VL cannot be recommended for people without experience in intubation because it requires a much longer learning process than indicated in the anesthetic literature. However, they reached their conclusions based on their experience with a study group, which was dominated by healthcare providers with extensive experience in classic DL intubation with a MAC blade, and these experiences had an impact on the use of ARQ, which requires a completely different application technique.27,28
In the case of VL MGT, Ti, and Tt times during the first intubation are similar to ARQ and are above 60s and above 80s, respectively. During subsequent intubation attempts, progress is visible in the achieved times, reaching approximately 20 seconds and approximately 40 seconds during the sixth intubation. Learning to use this VL involves obtaining better visibility of the glottal fissure according to the POGO scale. Obtaining increasingly better intubation times in this VL is associated with the recognition of subsequent intubation approaches as more difficult. This may be related to the structure of this VL, which is most structurally similar to MAC, but requires a different application technique. The inability to intubate the patient as quickly as would result from the increasingly better visibility of the glottis causes subsequent intubations to be considered more difficult. Similarly, in literature, we can find different data on the effectiveness of intubation using MAC and MGT. According to some data, this VL is comparable to MAC and other VLs, has similar effectiveness, and these are complementary devices.24,29 According to others, the use of MGT compared to DL improves the efficacy of first-pass endotracheal intubation in patients undergoing elective surgery and may be considered as the first-choice device during endotracheal intubation.29–32 A similar situation was observed in patients who underwent rapid induction of anesthesia, both by experienced intubators and inexperienced clinicians.30,31 The results obtained when using VL MGT and UES may be influenced by differences in the structure of both VLs, namely a more curved blade and a more movable monitor in the case of UES, as well as a different technique of using them.5 According to Hansel, hyperangulated VLs, which include UES, were more likely to limit esophageal intubation, may increase the effectiveness of the first intubation attempt, and also improve the view of the glottis than other types of VLs.14
Our study has several strengths. These include carrying it out in real conditions, in the operating theater while patients are under anesthesia for surgery. The participants in the study had no experience in using MAC, so the technique of using this DL and previously acquired practices did not affect the reception and technique of use of the tested VL. The assessed group were anesthesiology residents, ie people who, after gaining experience and completing their education, will be the most veritable healthcare providers assessing the usefulness of one or another VL in real conditions.
Our study has several limitations. These include, first of all, a relatively small study group of only 16 anesthesiology residents. Another is to use only three VLs, out of many currently available on the medical market. Another limitation is that only the first six intubations were examined. Perhaps, the learning curve would be different in subsequent uses. Selected VL were assessed only in patients with normal airways. Perhaps, the use of assessed VL in patients with difficult airways would verify the results obtained and the learning curve.
Conclusions
Based on our results, it can be concluded that the best learning curve among young anesthesiology residents is characterized by VL Airtraq and the best first-time use of VL UESCOPE. The results of our study require confirmation in a larger study group of residents and among patients also with difficult airways.
Institutional Review Board Statement
This study was approved on 14 November 2023 by the Medical University of Lodz Bioethics Committee (ref: RNN/160/23/KE).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the participants to publish this paper.
Data Sharing Statement
Data are contained within the article.
Ethical Statement
This study complies with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest.
References
1. Abhyankar P, Sabharwal N, Gupta A, Das AK. Comparative evaluation of C-MAC and McGrath MAC videolaryngoscopes with Macintosh direct laryngoscope for endotracheal intubation in adult patients undergoing elective surgeries.. J Anaesthesiol Clin Pharmacol. 2023;39(3):422–428. doi:10.4103/joacp.joacp_451_21
2. Lewis SR, Butler A, Parker J, Cook TM, Smith AF. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Database Syst Rev. 2016;2016(11):CD011136.
3. Belze O, Coppere Z, Ouattara J, et al. Influence of videolaryngoscopy using McGrath Mac on the need for a helper to perform intubation during general anaesthesia: a multicentre randomised video-no-video trial.. BMJ Open. 2022;12(1):e049275. doi:10.1136/bmjopen-2021-049275
4. Saracoglu KT, Eti Z, Gogus FY. Airtraq optical laryngoscope: advantages and disadvantages. Middle East J Anaesthesiol. 2013;22:135–141.
5. Xue FS, Yang BQ, Liu YY, Li HX, Yang GZ. Current evidences for the use of UEscope in airway management. Chin Med J. 2017;130:1867–1875. doi:10.4103/0366-6999.211536
6. Tsunoda N, Asai T. A double-curved tube for McGrath® MAC videolaryngoscope-guided tracheal intubation.. Br J Anaesth. 2022;128(1):e14–e16. doi:10.1016/j.bja.2021.09.033
7. Wakabayashi R, Ishida T, Yamada T, Kawamata M. Effect of an aerosol box on tracheal intubation difficulty. J Anesth. 2020;34(5):790–793. doi:10.1007/s00540-020-02835-2
8. Levitan RM, Heitz JW, Sweeney M, Cooper RM. The complexities of tracheal intubation with direct laryngoscopy and alternative intubation devices. Ann Emerg Med. 2011;57:240–247. doi:10.1016/j.annemergmed.2010.05.035
9. Koch DA, Hagebusch P, Faul P, Steinfeldt T, Hoffmann R, Schweigkofler U. Analysis of the primary utilization of videolaryngoscopy in prehospital emergency care in Germany.. Anaesthesiologie. 2023;72(4):245–252. doi:10.1007/s00101-022-01247-z
10. Nalubola S, Jin E, Drugge ED, Weber G, Abramowicz AE. Video versus direct laryngoscopy in novice intubators: a systemic review and meta-analysis. Cureus. 2022;14(9):e29578. doi:10.7759/cureus.29578
11. Di Marco P, Scattoni L, Spinoglio A, et al. Learning curves of the airtraq and Macintosh laryngoscopes for tracheal intubation by novice laryngoscopists: a clinical study. Anesth Analg. 2011;112:122–125. doi:10.1213/ANE.0b013e3182005ef0
12. Pan LF, Yu L, Pei HH, et al. The usage of HC videolaryngoscope for emergency tracheal intubation by unskilled junior emergency resident doctors (in Chinese. Chin J Emerg Med. 2016;25:910–914. doi:10.3760/cma.j.issn.1671-0282.2016.07.013
13. Moritz A, Leonhard V, Prottengier J, Birkholz T, Schmidt J, Irouschek A. Comparison of glidescope® Go™, King Vision™, Dahlhausen VL, IView™ and Macintosh laryngoscope use during difficult airway management simulation by experienced and inexperienced emergency medical staff: a randomized crossover manikin study. PLoS One. 2020;15(7):e0236474. doi:10.1371/journal.pone.0236474
14. Hansel J, Rogers AM, Lewis SR, Cook TM, Smith AF. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation. Cochrane Database Syst Rev. 2022;2022(4):CD011136.
15. Ratajczyk P, Dolder P, Szmyd B, et al. Comparison of UESCOPE VL 400, I-view, non-channeled airtraq videolaryngoscopes and Macintosh laryngoscope for tracheal intubation in simulated out-of-hospital conditions: a randomized crossover manikin study.. Healthcare. 2024;12(4):452. doi:10.3390/healthcare12040452
16. Malito ML, Mathias LAda ST, Kimura Junior A, Correa GH, Bardauuil VR. The impact of introducing a videolaryngoscope in the initial training of laryngoscopy for undergraduate medical students: a simulation randomized trial.. Braz J Anesthesiol. 2023;73(5):532–538. doi:10.1016/j.bjane.2021.02.048
17. Le Borgne P, Alamé K, Chenou A, et al. Training approaches and devices utilization during endotracheal intubation in French emergency departments: a nationwide survey. Eur J Emerg Med. 2024;31(1):46–52. doi:10.1097/MEJ.0000000000001091
18. Apfelbaum JL, Hagberg CA, Connis RT. American society of anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology. 2022;136:31–81. doi:10.1097/ALN.0000000000004002
19. Azam S, Khan ZZ, Shahbaz H, et al. Goyal A. video versus direct laryngoscopy for intubation: updated systematic review and meta-analysis. Cureus. 2024;16(1):e51720. doi:10.7759/cureus.51720
20. Hoshijima H, Mihara T, Shiga T, Mizuta K. Indirect laryngoscopy is more effective than direct laryngoscopy when tracheal intubation is performed by novice operators: a systematic review, meta-analysis, and trial sequential analysis. Can J Anaesth. 2024;71(2):201–212. doi:10.1007/s12630-023-02642-9
21. Hoshijima H, Mihara T, Denawa Y, Shiga T, Mizuta K. Airtraq® versus GlideScope® for tracheal intubation in adults: a systematic review and meta-analysis with trial sequential analysis. Can J Anaesth. 2022;69(5):605–613. doi:10.1007/s12630-022-02217-0
22. Pieters BM, Wilbers NE, Huijzer M, Winkens B, van Zundert AA. Comparison of seven videolaryngoscopes with the Macintosh laryngoscope in manikins by experienced and novice personnel. Anaesthesia. 2016;71:556–564. doi:10.1111/anae.13413
23. Hodgetts V, Danha RF, Mendonca C, Hillerman C. A randomized comparison of C-MAC videolaryngoscope versus Macintosh laryngoscope for tracheal intubation. J Anesth Clinic Res. 2011;2:163.
24. Sansone P, Giaccari LG, Bonomo A, et al. Comparison of McGrath videolaryngoscope versus Macintosh laryngoscope in tracheal intubation: an updated systematic review. J Clin Med. 2023;12(19):6168. doi:10.3390/jcm12196168
25. Lu Y, Jiang H, Zhu YS. Airtraq laryngoscope versus conventional Macintosh laryngoscope: a systematic review and meta-analysis. Anaesthesia. 2011;66:1160–1167. doi:10.1111/j.1365-2044.2011.06871.x
26. Nowicki TA, Suozzi JS, Dziedzic M, Kamin R, Donahue S, Robinson K. Comparison of use of the Airtraq with direct laryngoscopy by paramedics in the simulated airway. Prehosp Emerg Care. 2009;13:75–80. doi:10.1080/10903120802471881
27. Trimmel H, Kreutziger J, Fertsak G, Fitzka R, Dittrich M, Voelckel WG. Use of the Airtraq laryngoscope for emergency intubation in the prehospital setting: a randomized control trial. Crit Care Med. 2011;39:489–493. doi:10.1097/CCM.0b013e318206b69b
28. Wetsch WA, Spelten O, Hellmich M, et al. Comparison of different video laryngoscopes for emergency intubation in a standardized airway manikin with immobilized cervical spine by experienced anaesthetists. A randomized, controlled crossover trial. Resuscitation. 2012;83(6):740–745. doi:10.1016/j.resuscitation.2011.11.024
29. Lacquiere D, Mazur S, Wilkes A, Pearce A. Comparison of first-pass intubation success rates between two different videolaryngoscopes in an Australian prehospital and retrieval medicine service. Emerg Med Australas. 2023;35(6):941–945. doi:10.1111/1742-6723.14264
30. Kriege M, Noppens RR, Turkstra T, et al. EMMA trail Investigators Group. A multicentre randomised controlled trial of the McGrath™ Mac videolaryngoscope versus conventional laryngoscopy. Anaesthesia. 2023;78(6):722–729. doi:10.1111/anae.15985
31. Kriege M, Lang P, Schmidtmann I, et al. A comparison of the McGrath videolaryngoscope with direct laryngoscopy for rapid sequence intubation in the operating theatre: a multicentre randomised controlled trial. Anaesthesia. 2024. doi:10.1111/anae.16250
32. Kim HJ, Kim HR, Kim SY, et al. Predictors of difficult intubation when using a videolaryngoscope with an intermediate-angled blade during the first attempt: a prospective observational study. J Clin Monit Comput. 2022;36(4):1121–1130. doi:10.1007/s10877-021-00742-9
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.