")
Back to Journals » Advances in Medical Education and Practice » Volume 16
How Preceptor Behaviour Shapes the Future of Medical Professionals
Authors Alshareef MH , Flemban AF
Received 6 June 2024
Accepted for publication 12 January 2025
Published 30 January 2025 Volume 2025:16 Pages 135—144
DOI https://doi.org/10.2147/AMEP.S481620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Maram H Alshareef,1 Arwa F Flemban2
1Department of Community Medicine and Pilgrims Health, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 2Department of Pathology, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Maram H Alshareef, Department of Community Medicine and Pilgrims Health, Faculty of Medicine, Umm Al-Qura University, Makkah, 21955, Saudi Arabia, Email [email protected]
Abstract: Preceptors play an indispensable role in shaping the future of healthcare. They bridge theoretical learning and practical clinical expertise in a rapidly evolving medical education landscape. Their influence extends beyond knowledge transfer, embodying the values, attitudes, and professionalism essential to competent medical practice. Bandura’s Social Learning Theory posits that individuals learn through observation and modelling. Applying this theory supports the assumption that trainees acquire skills and professional norms by observing preceptor behaviour, a process known as vicarious learning. They transmit clinical competencies, ethical standards, and interpersonal skills critical for patient-centred care. Despite their significance, challenges such as increasing workloads, diverse trainee needs, and the complexities of modern healthcare often impede their ability to mentor effectively. Preceptors shape trainees’ professional identities and ethical standards, which are significantly influenced by the hidden curriculum, the set of unspoken or implicit lessons conveyed outside the formal curriculum. Globally, there is growing recognition of the need to support and enhance the role of preceptors in medical education. Due to several challenges, some factors might prevent preceptors from maintaining their role model status, including the need for experience, continuous learning, and adaptation to diverse trainee needs. Strategies such as engaging in reflective practices and implementing effective stress management techniques are crucial for preceptors to navigate these barriers and uphold their status. However, few studies have synthesised the various dimensions of preceptor influence, including role modelling, communication skills, and the hidden curriculum. This review aims to fill this gap by exploring the variable role of preceptors in shaping medical trainees’ professional development. It highlights the theoretical underpinnings of preceptorship, discusses the challenges preceptors face, and proposes evidence-based strategies to enhance their impact on future healthcare professionals.
Keywords: trainee, role model, communication, hidden curriculum
Introduction
Preceptors play an indispensable role in shaping the future of healthcare, acting as the bridge between theoretical learning and practical clinical expertise in a rapidly evolving medical education landscape. The landscape of medical education is undergoing a profound transformation globally, driven by rapid advancements in medical science, shifting community needs, and the integration of innovative teaching methodologies. This evolution reflects the growing recognition of the importance of a well-rounded medical education framework incorporating clinical competence, professionalism, and interpersonal skills.1
Preceptors are central to this transformative journey as their roles have expanded significantly beyond the traditional confines of medical education. They are foundational to medical education, serving as educators, mentors, and role models who shape medical trainees’ professional competencies and identities.2,3 Their influence extends far beyond the clinical setting, as they act as anchors in the complex machinery of medical education (Figure 1). They ensure a smooth transition from academic knowledge to practical competence, fostering an environment where trainees can develop critical skills necessary for patient care.4 Transition to Practice, traditionally associated with residency education, is now being integrated into undergraduate medical education. Preceptors play a critical role in guiding students through early experiential learning and preparing them for the realities of clinical practice.5
 |
Figure 1 The preceptor role to shape the trainee future. |
This review is grounded in Bandura’s Social Learning Theory, which emphasises that individuals learn behaviours, skills, and values through observation and modelling. Highlighting the preceptor’s role as a critical influence. This role aligns closely with Bandura’s Social Learning Theory, a cornerstone for understanding how observational learning influences behaviour and identity formation. It posits that individuals learn behaviours, skills, and attitudes through observation, imitation, and modelling.6 Bandura’s framework highlights that these behaviours are internalised through cognitive processes involved in learning within social contexts. It emphasises that role models, like preceptors, are instrumental in shaping technical competencies, their trainees’ values, and ethical standards.7 In medical education, preceptors’ observable behaviours, communication styles, and attitudes contribute significantly to students’ professional identity formation.8 As medical trainees observe their preceptors, they internalise these behaviours and attitudes, shaping their future interactions with patients and colleagues.9
In addition to their roles as educators and mentors, preceptors are pivotal in instilling values and ethical reasoning within trainees, ensuring that they embody the principles of medical professionalism. A longitudinal survey conducted in the US found that over 40% of medical students reported experiences of belittlement or harassment, which correlated with feelings of isolation and impacted their career decisions. 10 Similarly, a systematic review in academic medicine revealed high prevalence rates of academic bullying, including overwork, public humiliation, and undermining professional status, particularly during early training phases.11 These patterns erode students’ confidence and create a toxic learning environment that perpetuates poor professional behaviours in their future roles.12 Such an influence is relevant in the hidden curriculum, which refers to the implicit lessons conveyed through behaviours, organisational culture, and informal interactions within the medical environment.13 Through their actions, preceptors serve as interpreters of this hidden curriculum, transmitting lessons on professionalism, ethical decision-making, and interpersonal skills crucial to shaping a competent and ethical medical workforce.14
Globally, there is an increasing emphasis on competency-based training in medical education, which focuses on developing a diverse skill set that encompasses clinical expertise, cultural competence, and effective communication.15 This shift has placed additional responsibilities on preceptors, requiring them to integrate traditional teaching methods with modern, competency-based approaches while respecting the cultural and religious ethos of the region.16
Preceptors face unique challenges in maintaining their dual roles as clinicians and educators. Balancing the demands of daily clinical practice with teaching responsibilities requires adaptability, resilience, and ongoing professional development.17 Despite these challenges, their role in bridging the gap between theoretical knowledge and practical application remains indispensable. As role models, preceptors demonstrate how to balance professional demands with ethical considerations and personal well-being, guiding trainees to navigate the complexities of medical practice.18 Despite their essential role, limited research synthesises the various ways preceptors influence trainee development, mainly through role modelling, communication skills, and the hidden curriculum. This review aimed to explain the importance of preceptors as role models in medical education and shaping future trainees by examining their duties and responsibilities.
This review article aims to address several key aspects driven by the authors observations through the lens of Bandura’s social learning theory, including role modelling as a cornerstone for learning, the behaviour of preceptors outside the classroom as a representation of the learning environment, the importance of effective communication skills within the institute, and the implicit lessons conveyed through the hidden curriculum. Furthermore, the article explores the challenges preceptors face in balancing their responsibilities as role models while keeping up with the demands of daily clinical practice and teaching. This review examines the several role of preceptors in medical education, focusing on their influence through role modelling, communication, and the hidden curriculum while addressing the challenges they face and proposing strategies for their enhancement.
Methods
Study Design
This review adopts a narrative approach to synthesising and evaluating the role of preceptors in medical education, particularly within the context of Bandura’s Social Learning Theory. It examines how preceptors influence medical trainees’ professional development and addresses critical areas such as role modelling, communication, and the hidden curriculum.
Data Sources
Two primary databases, PubMed and Google Scholar, were utilised. A search was conducted between October 2024 and November 2024. Additional relevant articles were identified through reference screening of included studies.
Search Strategy
The following search terms were used individually and in combination:
Keywords
“Preceptor” OR “mentor” OR “clinical teacher”
“Role model” OR “modelling behaviour”
“Medical education” OR “clinical training”
“Communication skills” OR “hidden curriculum”
“Bandura’s Social Learning Theory” OR “observational learning”
“Professional identity formation” OR “trainee development”
Inclusion and Exclusion Criteria
Inclusion Criteria
- Articles published between 2000 and 2023.
- Peer-reviewed studies, reviews, and meta-analyses focusing on the role of preceptors in medical education.
- Research discussing role modelling, communication, and the hidden curriculum.
- Studies conducted in medical or healthcare education settings.
Exclusion Criteria
- Articles not written in English.
- Studies focused exclusively on nursing or allied health professions without relevance to medical trainees.
- Opinion pieces, editorials, and non-peer-reviewed sources unless highly relevant.
Study Selection and Data Extraction
- Titles and abstracts were screened independently by two reviewers to ensure relevance.
- Full-text articles meeting the inclusion criteria were reviewed for content.
- The key data extracted included the study design, sample size, research focus, and outcomes related to preceptor behaviour and trainee development.
Ethical Considerations
No ethical approval was required for this literature review. However, efforts were made to ensure accurate citation and acknowledgement of all referenced works.
Statistical Analysis
This review does not include statistical analysis; instead, it synthesises findings qualitatively to conclude the role of preceptors in medical education. This method section strengthens the credibility by outlining the methodology and creating a clear, reproducible framework.
Results
The review identified 25 studies that met the inclusion criteria. These studies provide insights into the role of preceptors in medical education, mainly through the lens of Bandura’s Social Learning Theory. The findings are categorised into four primary themes: Role Modelling, Communication Skills, hidden curriculum, and Challenges and summarised in Table 1.
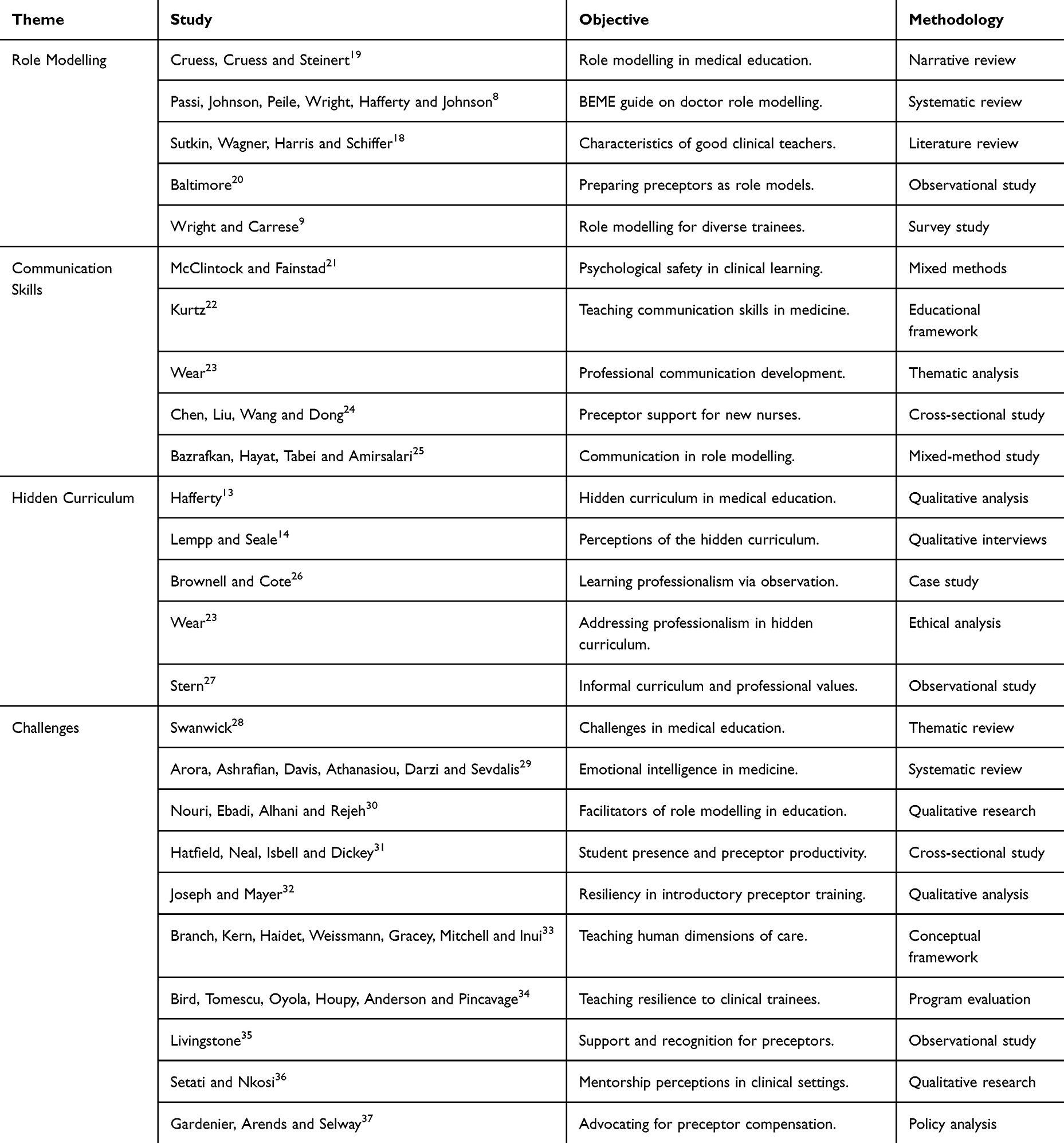 |
Table 1 Summary of Studies Used to Review the Role of Preceptors in Medical Education and the General Theme |
Role Modelling
Preceptors serve as vital role models, significantly influencing the professional development of medical trainees. Positive role modelling by preceptors has been associated with enhanced professionalism, ethical decision-making, and clinical competence among trainees. For instance, a study by Cruess, Cruess and Steinert19 highlighted that trainees often emulate the behaviours and attitudes of their preceptors, underscoring the importance of exemplary conduct in clinical settings.
Communication Skills
Effective communication between preceptors and trainees fosters a supportive learning environment, promoting open dialogue and feedback. Studies indicate that preceptors who demonstrate strong communication skills enhance trainee engagement and reduce anxiety. McClintock and Fainstad21 found that structured communication training improved trainee satisfaction and performance for preceptors.
Hidden Curriculum
The hidden curriculum encompasses the implicit lessons conveyed through the culture and practices within medical education. Preceptors are crucial in shaping this hidden curriculum, influencing trainees’ perceptions of professionalism and ethical behaviour. Lempp and Seale14 reported that trainees often internalise the unspoken norms exhibited by their preceptors, which can significantly impact their professional identity formation.
Challenges
Preceptors face several challenges that can impede their effectiveness, including heavy workloads, diverse trainee backgrounds, and varying levels of emotional intelligence. Swanwick28 emphasised the need for institutional support to address these challenges, suggesting that targeted training and resources can enhance preceptor performance and trainee development.
Discussion
Role Modelling: The Cornerstone of Learning
Role modelling is fundamental to Bandura’s Social Learning Theory,7 which emphasises observational learning. Preceptors serve as role models by exhibiting behaviours, values, and attitudes that trainees internalise, shaping their professional identity.6 Studies confirm that positive role modelling is characterised by empathy, professionalism, and resilience. These characteristics correlate with enhanced professionalism, ethical behaviour, and teamwork among trainees. This ripple effect strengthens healthcare delivery by fostering a culture of patient-centred care and collaboration.18–20,38,39
Conversely, negative role modelling, such as unprofessional or abusive behaviour, risks perpetuating undesirable traits. Exposure to such behaviours during training is linked to future professional misconduct.40 It indicates the need for vigilant monitoring of preceptor conduct issues requires institutions to emphasise training programs that foster emotional intelligence, reflective practices, and effective feedback mechanisms. Such initiatives empower preceptors to serve as ethical and professional exemplars.13
The Foundation of Effective Role Modelling
Effective communication is crucial in medical education, serving as a bridge between teaching and mentorship. Preceptors who model clear, empathetic communication create supportive learning environments, boosting trainees’ confidence and engagement. Constructive cues, such as actionable feedback and active listening, are critical for building trust and psychological safety, essential for professional growth.41
Research highlights that poor communication, characterised by dismissive or abrasive behaviours, can lead to trainee disengagement, burnout, and reduced self-esteem. Institutions must prioritise communication training, emphasising conflict resolution and mentorship skills. Regular workshops, peer evaluations, and trainee feedback can enhance communication effectiveness and positively impact trainee development.42
The Hidden Curriculum
The unspoken lessons in the professional curriculum are those trainees absorb in clinical and educational settings.6,23 These lessons shape their professional values and ethical reasoning.23,43 Preceptors play a pivotal role in modelling the hidden curriculum, influencing trainees’ perceptions of accountability, cultural competence, and empathy.18,21
Positive aspects of the hidden curriculum, such as compassese, enforce professionalism. On the other hand, negative elements, like favouritism or cynicism, may erode professional identity formation.27 Addressing the hidden curriculum requires fostering open dialogue, reflective practices, and safe feedback channels.14,22,44,45 Leadership must advocate for policies prioritising ethical behaviour and professional conduct to create an environment that aligns with educational objectives14,46 (Figure 2).
 |
Figure 2 Maintaining role model status. |
Navigating Challenges to Maintain Role Model Status
Preceptors face numerous challenges, time constraints, and administrative burdens.28,47 Balancing these demands often limits meaningful engagement with trainees.48 Research shows that burnout and stress among preceptors negatively impact their ability to mentor effectively, highlighting the need for structured support systems.30,31
To Address These Challenges
Reflective practices and continuous self-evaluation help preceptors gain insight into their teaching styles, professional interactions, and personal biases.49 This allows them to refine their approaches and better align themselves with the profession’s ideals. Stress management strategies like mindfulness, work-life balance, and peer support can mitigate burnout and promote resilience.32 In addition, staying abreast of advancements ensures preceptors impart evidence-based practices, reinforcing the importance of continual professional growth.33 Additionally, diversity among trainees requires preceptors to adopt personalised mentorship approaches, incorporating cultural values and diversity and encouraging academic and professional excellence in the medical field.50 This adaptability enhances mentorship effectiveness, fostering an inclusive learning environment.34,51
Addressing Institutional Barriers
Administrative responsibilities often overshadow educational priorities, detracting from preceptor performance.52 Engaging preceptors in decision-making processes ensures alignment between institutional and academic goals. Administrative duties, including documentation, evaluation of trainees, and participation in institutional committees, pose significant challenges for preceptors. These tasks can consume valuable time that could otherwise be spent on teaching or professional development.52 Moreover, the bureaucratic nature of some administrative processes adds to preceptors’ stress and reduces job satisfaction.53
Institutions can address this issue by streamlining administrative workflows and providing administrative support, such as dedicated coordinators or digital platforms to manage evaluations and documentation.45 Reducing paperwork and offering clear guidelines can help preceptors focus on their core educational responsibilities.
Conclusion
This comprehensive review explored the multifaceted role of preceptors in medical education, highlighting their pivotal role in shaping the future of healthcare professionals. The key points discussed here underscore the significance of preceptors not only as transmitters of clinical knowledge but also as influential role models, mentors, and architects of the learning environment. As part of Bandura’s social learning theory, the concept of vicarious learning emphasises the profound impact of preceptors on trainees through observation and emulation. Preceptors’ positive and negative behaviours are critical in shaping medical trainees’ professional identity and ethical standards, as evidenced by the hidden curriculum.
The challenges preceptors face in maintaining their role model status, including the need for continuous learning and adaptation to diverse trainee needs, highlight the dynamic nature of their roles. This demands a lifelong commitment to education, emotional intelligence, and cultural competence to mentor and model desired behaviours within the healthcare setting effectively. The additional pressures of stress and time constraints in high-demand environments further test their resilience. However, through reflective practice, stress management, and seeking feedback, preceptors can navigate these challenges, reinforcing their role as pivotal mentors. These strategies aid in their personal and professional growth and exemplify the importance of adaptability and self-care to their trainees, thereby shaping the future of healthcare professionalism.
Looking to the future, there is a need for ongoing research and development in preceptor training and support. Medical education must focus more on cultivating effective role models and facilitating meaningful interactions between these role models and trainees. Medical education can emphasise the significance of positive mentorship, professionalism, and ethical behaviour by viewing role models as mirrors for future trainees.
Research in this area can further explore the specific characteristics and behaviours of adequate role models and the impact of mentorship on trainees’ career satisfaction and success. Additionally, medical institutions can implement programs and initiatives to promote mentorship and foster a culture that values the mentorship role of experienced professionals.
This includes exploring innovative methods for preceptor development, such as simulation-based training, digital platforms for continuous learning, and structured feedback mechanisms. Research should also focus on understanding the impact of cultural diversity on the preceptor-trainee relationship and developing strategies to enhance cultural competence among preceptors.
Furthermore, the evolving healthcare and medical education landscape necessitates reevaluating the competencies required for effective preceptorship. This re-evaluation should consider the increasing complexity of healthcare systems, technology integration in medical practice, and the changing dynamics of patient populations.
In conclusion, preceptors play an indispensable and multifaceted role in medical education. Recognising and enhancing this role is crucial for developing a competent, ethical, and professional medical workforce. Preceptors shape trainees’ clinical skills and mould their professional identities and ethical perspectives. As medical education continues to evolve, the support and development of preceptors should be a key focus to ensure that they are well equipped to guide and inspire the next generation of medical professionals.
Acknowledgments
To our students and colleagues in the medical college at Umm Al-Qura University who inspired us to do this research and produce this work.
Author Contributions
Both authors contributed significantly to the work reported, whether in the conception, study design, execution, data acquisition, or all these areas. They drafted, wrote, substantially revised, or critically reviewed the article. Have agreed on the journal to which the article will be submitted. Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. Agree to take responsibility and be accountable for the contents of the article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goodwin AM, Oliver SW, McInnes I, Millar KF, Collins K, Paton C. Professionalism in medical education: the state of the art. Int J Med Educ. 2024;29(15):44–47. doi:10.5116/ijme.6626.583a
2. Cruess RL, Cruess SR. Teaching professionalism: general principles. Med Teach. 2006;28(3):205–208. doi:10.1080/01421590600643653
3. Jochemsen-van der Leeuw HG, van Dijk N, van Etten-Jamaludin FS, Wieringa-de Waard M. The attributes of the clinical trainer as a role model: a systematic review. Acad Med. 2013;88(1):26–34. doi:10.1097/ACM.0b013e318276d070
4. Challa KT, Sayed A, Acharya Y. Modern techniques of teaching and learning in medical education: a descriptive literature review. MedEdPublish. 2021;10:18. doi:10.15694/mep.2021.000018.1
5. Hampton KB, Smeltzer SC, Ross JG. The transition from nursing student to practicing nurse: an integrative review of transition to practice programs. Nurse Educ Pract. 2021;52:103031. doi:10.1016/j.nepr.2021.103031
6. Martin CL, Dinella L. Gender-related Development. In: Smelser NJ, Baltes PB, editors. International Encyclopedia of the Social & Behavioral Sciences. Pergamon. 2001:6020–6027.
7. Bandura A. Social foundations of thought and action: a social cognitive theory.
8. Passi V, Johnson S, Peile E, Wright S, Hafferty F, Johnson N. Doctor role modelling in medical education: BEME Guide No. 27. Med Teach. 2013;35(9):e1422–36. doi:10.3109/0142159X.2013.806982
9. Wright SM, Carrese JA. Serving as a physician role model for a diverse population of medical learners. Acad Med. 2003;78(6):623–628. doi:10.1097/00001888-200306000-00013
10. Frank E, Carrera JS, Stratton T, Bickel J, Nora LM. Experiences of belittlement and harassment and their correlates among medical students in the United States: longitudinal survey. BMJ. 2006;333(7570):682. doi:10.1136/bmj.38924.722037.7C
11. Averbuch T, Eliya Y, Van Spall HGC. Systematic review of academic bullying in medical settings: dynamics and consequences. BMJ Open. 2021;11(7):e043256. doi:10.1136/bmjopen-2020-043256
12. Hicks S, Stavropoulou C. The effect of health care professional disruptive behavior on patient care: a systematic review. J Patient Saf. 2022;18(2):138–143. doi:10.1097/PTS.0000000000000805
13. Hafferty FW. Beyond curriculum reform: confronting medicine’s hidden curriculum. Acad Med. 1998;73(4):403–407. doi:10.1097/00001888-199804000-00013
14. Lempp H, Seale C. The hidden curriculum in undergraduate medical education: qualitative study of medical students’ perceptions of teaching. BMJ. 2004;329(7469):770–773. doi:10.1136/bmj.329.7469.770
15. Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638–645. doi:10.3109/0142159X.2010.501190
16. Khalil MK, Elkhider IA. Applying learning theories and instructional design models for effective instruction. Adv Physiol Educ. 2016;40(2):147–156. doi:10.1152/advan.00138.2015
17. Irby DM. Teaching and learning in ambulatory care settings: a thematic review of the literature. Acad Med. 1995;70(10):898–931. doi:10.1097/00001888-199510000-00014
18. Sutkin G, Wagner E, Harris I, Schiffer R. What makes a good clinical teacher in medicine? A review of the literature. Acad Med. 2008;83(5):452–466. doi:10.1097/ACM.0b013e31816bee61
19. Cruess SR, Cruess RL, Steinert Y. Role modelling--making the most of a powerful teaching strategy. BMJ. 2008;336(7646):718–721. doi:10.1136/bmj.39503.757847.BE
20. Baltimore JJ. The hospital clinical preceptor: essential preparation for success. J Contin Educ Nurs. 2004;35(3):133–140. doi:10.3928/0022-0124-20040501-10
21. McClintock AH, Fainstad T. Growth, engagement, and belonging in the clinical learning environment: the role of psychological safety and the work Ahead. J Gen Intern Med. 2022;37(9):2291–2296. doi:10.1007/s11606-022-07493-6
22. Kurtz S, Draper J, Silverman J. Teaching and Learning Communication Skills in Medicine.
23. Wear D. Professional development of medical students: problems and promises. Acad Med. 1997;72(12):1056–1062. doi:10.1097/00001888-199712000-00015
24. Chen F, Liu Y, Wang X, Dong H. Transition shock, preceptor support and nursing competency among newly graduated registered nurses: a cross-sectional study. Nurse Educ Today. 2021;102:104891. doi:10.1016/j.nedt.2021.104891
25. Bazrafkan L, Hayat AA, Tabei SZ, Amirsalari L. Clinical teachers as positive and negative role models: an explanatory sequential mixed method design. J Med Ethics Hist Med. 2019;12:11. doi:10.18502/jmehm.v12i11.1448
26. Brownell AK, Cote L. Senior residents’ views on the meaning of professionalism and how they learn about it. Acad Med. 2001;76(7):734–737. doi:10.1097/00001888-200107000-00019
27. Stern DT. In search of the informal curriculum: when and where professional values are taught. Acad Med. 1998;73(10 Suppl):S28–30. doi:10.1097/00001888-199810000-00036
28. Swanwick T. Understanding medical education. Understand Med Educat. 2018;2018:1–6.
29. Arora S, Ashrafian H, Davis R, Athanasiou T, Darzi A, Sevdalis N. Emotional intelligence in medicine: a systematic review through the context of the ACGME competencies. Med Educ. 2010;44(8):749–764. doi:10.1111/j.1365-2923.2010.03709.x
30. Nouri JM, Ebadi A, Alhani F, Rejeh N. Experiences of role model instructors and nursing students about facilitator factors of role-modeling process: a qualitative research. Iran J Nurs Midwifery Res. 2014;19(3):248–254.
31. Hatfield J, Neal G, Isbell T, Dickey D. The effect of a medical student on community preceptor productivity. Med Educ. 2022;56(7):747–753. doi:10.1111/medu.14733
32. Joseph A, Mayer DC. A qualitative analysis of student and preceptor resiliency discussions during introductory pharmacy practice experiences. Am J Pharm Educ. 2023;87(8):100104. doi:10.1016/j.ajpe.2023.100104
33. Branch WT Jr, Kern D, Haidet P, et al. The patient-physician relationship. Teaching the human dimensions of care in clinical settings. JAMA. 2001;286(9):1067–1074. doi:10.1001/jama.286.9.1067
34. Bird A, Tomescu O, Oyola S, Houpy J, Anderson I, Pincavage A. A curriculum to teach resilience skills to medical students during clinical training. MedEdPORTAL. 2020;16:10975. doi:10.15766/mep_2374-8265.10975
35. Livingstone K. How lack of support and recognition for RN preceptors is affecting nursing students’ learning on placement. Nurse Edu Today. 2024;138:106192. doi:10.1016/j.nedt.2024.106192
36. Setati CM, Nkosi ZZ. The perceptions of professional nurses on student mentorship in clinical areas: a study in Polokwane municipality hospitals, Limpopo province. Health SA. 2017;22:130–137. doi:10.1016/j.hsag.2017.01.008
37. Gardenier D, Arends R, Selway J. Should Preceptors Be Paid? J Nurse Practit. 2019;15(8):542–543. doi:10.1016/j.nurpra.2019.06.007
38. Monrouxe LV, Rees CE. ”It’s just a clash of cultures”: emotional talk within medical students’ narratives of professionalism dilemmas. Adv Health Sci Educ Theory Pract. 2012;17(5):671–701. doi:10.1007/s10459-011-9342-z
39. Landberg M, Partsch MV. Perceptions on and attitudes towards lifelong learning in the educational system. Social Sci Humanities Open. 2023;8(1):100534. doi:10.1016/j.ssaho.2023.100534
40. Dcruz MM. The culture of bullying in medical training must stop. World Social Psych. 2022;4(1):4–9. doi:10.4103/wsp.wsp_30_21
41. Swick HM. Toward a normative definition of medical professionalism. Acad Med. 2000;75(6):612–616. doi:10.1097/00001888-200006000-00010
42. Harden RM, Laidlaw JM. Be FAIR to students: four principles that lead to more effective learning. Med Teach. 2013;35(1):27–31. doi:10.3109/0142159X.2012.732717
43. Kärner T, Schneider G. A scoping review on the hidden curriculum in education. Res Edu Curriculum Pedagogy.2024;2024:1
44. Cruess SR, Cruess RL, Steinert Y. Supporting the development of a professional identity: general principles. Med Teach. 2019;41(6):641–649. doi:10.1080/0142159X.2018.1536260
45. Ramani S, Leinster S. AMEE Guide no. 34: teaching in the clinical environment. Med Teach. 2008;30(4):347–364. doi:10.1080/01421590802061613
46. Brown MEL, Coker O, Heybourne A, Finn GM. Exploring the hidden curriculum’s impact on medical students: professionalism, identity formation and the need for transparency. Med Sci Educ. 2020;30(3):1107–1121. doi:10.1007/s40670-020-01021-z
47. Buckley S, Coleman J, Davison I, et al. The educational effects of portfolios on undergraduate student learning: a best evidence medical education (BEME) systematic review. BEME Guide No. 11. Med Teach. 2009;31(4):282–298. doi:10.1080/01421590902889897
48. Billett S. Learning through work: workplace affordances and individual engagement. J Workplace Learning. 2001;13(5):209–214. doi:10.1108/EUM0000000005548
49. Duffy A. Guiding students through reflective practice - The preceptors experiences. A qualitative descriptive study. Nurse Educ Pract. 2009;9(3):166–175. doi:10.1016/j.nepr.2008.07.002
50. Gayef A, Caylan A, Temiz SA. Learning styles of medical students and related factors. BMC Med Educ. 2023;23(1):282. doi:10.1186/s12909-023-04267-4
51. Malouff J, Thorsteinsson E. Increasing emotional intelligence through training: current status and future directions. Int J Emot Edu. 2013;5:56–72.
52. Bsc J, McAllister L. The lived experiences of clinical educators with implications for their preparation, support and professional development. Learn Health Social Care. 2005;4:156–171. doi:10.1111/j.1473-6861.2005.00097.x
53. Kaviani N, Stillwell Y. An evaluative study of clinical preceptorship. Nurse Educ Today. 2000;20(3):218–226. doi:10.1054/nedt.1999.0386
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.