")
Back to Journals » Journal of Inflammation Research » Volume 17
Impact of Glucocorticoid Therapy on 28-Day Mortality in Patients Having Severe Fever with Thrombocytopenia Syndrome in an Intensive Care Unit: A Retrospective Analysis
Authors Wang G, Liu P, Xie H, Niu C, Lyu J, An Y, Zhao H
Received 12 July 2024
Accepted for publication 8 October 2024
Published 24 October 2024 Volume 2024:17 Pages 7627—7637
DOI https://doi.org/10.2147/JIR.S478520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Guangjie Wang,1,* Puhui Liu,2,* Hui Xie,2 Chuanzhen Niu,2 Jie Lyu,1 Youzhong An,1 Huiying Zhao1
1Department of Critical Care Medicine, Peking University People’s Hospital, Beijing, People’s Republic of China; 2Department of Critical Care Medicine, Yantai Qishan Hospital, Yantai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huiying Zhao, Department of Critical Care Medicine, Peking University People’s Hospital, No. 11, Southern Xizhimen Road, Beijing, 100044, People’s Republic of China, Tel +86 13811088270, Email [email protected]
Purpose: The high mortality rate associated with the critical stages of severe fever with thrombocytopenia syndrome (SFTS) does not have effective treatment. We aimed to evaluate the 28-day mortality and potential impact of glucocorticoid therapy in these patients.
Patients and Methods: This retrospective observational study included participants from the intensive care unit between July 2019 and April 2023. The participants were categorized into glucocorticoid (GC) and non-GC groups. Propensity score matching (PSM) was employed to ensure comparability between groups. We used Cox proportional hazard models to examine mortality risk associated with GC use, Kaplan–Meier survival analyses for overall survival, stratified Cox proportional hazard models for subgroup analyses, and likelihood ratio tests to examine interactions between subgroups.
Results: Of 218 patients with SFTS (median age, 71 years; male, 49.1%), 61.9% required mechanical ventilation, 58.3% received GC treatment, and the 28-day mortality rate was 61.5%. After PSM, there were 58 patients in each group; post-PSM analysis revealed improved 28-day mortality rates with GC treatment, particularly for patients with Glasgow coma scale (GCS) score < 13 (hazard ratio [HR], 95% confidence interval [CI] for GCS score: 9– 12: 0.39, 0.17– 0.88, p=0.024 and for GCS score: 3– 8: 0.09, 0.02– 0.35, p=0.001); lactate levels > 2 mmol/L (0.35, 0.15– 0.83, p=0.017); and norepinephrine usage (0.26, 0.13– 0.49, p< 0.001). Combining antiviral (0.41, 0.22– 0.78, p=0.006) or immunoglobulin therapy (0.22, 0.1– 0.51, p< 0.001) with GC treatment significantly decreased the 28-day mortality rates, compared with GC monotherapy.
Conclusion: Using GCs reduced the high 28-day mortality rate in the patients, especially with low GCS score, high lactate levels, norepinephrine intake, and on antiviral or immunoglobulin therapy.
Keywords: glucocorticoids, mortality, severe fever with thrombocytopenia syndrome, intensive care unit, virus infection
Introduction
Severe fever with thrombocytopenia syndrome (SFTS) is an emerging tick-borne infectious disease that affects both humans and animals and is caused by severe fever with thrombocytopenia syndrome virus (SFTSV). The SFTSV was first isolated from a patient’s blood sample in Henan province in 2009.1 The disease is endemic in several Asian countries, including China, Korea, Vietnam, Pakistan, and Japan, and has been shown to cause high mortality rates across these regions.1–5 The clinical manifestations of SFTSV infection mainly include fever, thrombocytopenia, leukopenia, and gastrointestinal symptoms. Although most patients with SFTSV have mild to moderate symptoms, some may experience severe complications, such as organ failure and blood clotting issues, which can quickly lead to death.6 Once the central nervous system is involved, the mortality rate can reach 44.7%.7 For critically ill patients with SFTSV, no effective drug or intervention has been shown to reduce mortality except life support.
A severe systemic inflammatory response is one of the primary characteristics of this condition.8 Consequently, systemic glucocorticoid (GC) therapy serves as an adjunct treatment in patients with severe SFTS in clinical settings.9–12 However, the effects of GCs on SFTS have been inconsistent across studies,9,11 suggesting the need to understand the specific circumstances that cause variations in treatment efficacy. Notably, the effect of GC therapy may depend on the severity of patient’s condition.
Despite the known inconsistencies and the potential impact of patient conditions on therapy outcomes, to the best of our knowledge, no studies have specifically addressed the use of GCs in critically ill patients with SFTS in the intensive care unit (ICU). Therefore, this study aimed to evaluate the 28-day mortality and potential impact of glucocorticoid therapy in these patients.
Materials and Methods
Data Source and Study Population
This study employed a retrospective observational design, selecting patients aged ≥18 years with SFTS admitted to the ICU of Yantai Qishan Hospital in Yantai City from July 2019 to April 2023. This study was approved by the Ethics Committee of Qishan Hospital (202401). Informed consent was waived by ethics committee due to its retrospective design. In accordance with the guidelines set forth by the Declaration of Helsinki, this study was conducted with the utmost respect for patient confidentiality and ethical standards. Every case was meticulously confirmed in the laboratory center at Qishan Hospital. The diagnosis of SFTS was ascertained by detecting the ribonucleic acid (RNA) of the SFTSV in patients’ blood samples. This was accomplished using real-time reverse transcription-polymerase chain reaction.13 Following the successful identification of SFTSV RNA, we accurately quantified the viral load in each sample. This rigorous approach ensured a precise and reliable diagnosis of SFTS in all examined cases. The exclusion criteria included individuals with incomplete clinical data, hematological disorders, and an ICU stay of less than 24 hours.
Study Definition
The study was started with patient data from the first day of ICU admission, and the worst value within 24 h was recorded. The severity of the condition was quantitatively assessed using the sequential organ failure assessment (SOFA) score. The SOFA score represents indicators of different organ functions. The Grading was conducted based on the viral load, which was categorized into three levels: low viremia (<106 copies per mL), intermediate viremia (106–107 copies per mL), and high viremia (>107 copies per mL).14 The definition of GC use included the administration of methylprednisolone and/or hydrocortisone. The primary outcome was 28-day mortality from ICU admission, and secondary outcomes included bleeding sites, secondary infections, mechanical ventilation, arrhythmia, continuous renal replacement therapy (CRRT), ICU stay, and hospital stay. We recorded the duration from symptom onset to ICU admission (time from symptom onset to ICU admission, T-SO-ICUA).
Statistical Analysis
Categorical variables were described as frequencies, whereas continuous variables were presented as either mean ± standard deviation or median (range). To evaluate statistical significance, Student’s t-test or analysis of variance was applied, as appropriate. For categorical variable comparisons, the chi-square (χ2) test was used along with Fisher’s exact test. After analyzing baseline data, the participants were categorized into GC and non-GC groups based on GC usage. Propensity score matching (PSM) was based primarily on demographic and clinical characteristics excluding vital signs and investigations, with the exception of viral load. The results were compared between the GC and non-GC groups using 1:1 matching with a caliper value of 0.02. This method successfully neutralized pre-existing disparities between the groups. Kaplan–Meier survival analysis was used to evaluate the duration from SFTS onset to mortality and subsequent comparisons between the groups. A Cox proportional hazards model was used to assess the mortality risk associated with GC treatment. Subgroup analyses were conducted using a stratified Cox proportional hazards model based on the Glasgow coma scale (GCS) score; lactate levels; use of immunoglobulin, norepinephrine, and antiviral drugs; and partial pressure of oxygen in the alveoli/ fraction of inspired oxygen levels. Likelihood ratio tests were used to examine the interactions between the subgroups. The R statistical software (version 4.2.2, The R Foundation) was used for all statistical analyses. All tests were two-sided, and statistical significance was set at p<0.05.
Results
Baseline Characteristics
Between July 2019 and April 2023, a total of 231 confirmed cases of SFTS were examined. A total of 218 patients who met the eligibility criteria were enrolled in this study (Figure 1). The median age of the cohort admitted to the ICU was 71 years (interquartile range [IQR]: 65–76 years), and 107 (49.1%) patients were male. The proportions of participants who reported smoking cigarettes and consuming alcohol were 21.1% (46/218) and 17.9% (39/218), respectively. The chronic comorbidities observed included hypertension, diabetes, coronary heart disease (CHD), and chronic obstructive pulmonary disease (COPD). These conditions were present in 57 (26.1%), 46 (21.1%), 15 (6.9%), and 5 patients (2.3%), respectively. The median of T-SO-ICUA was 7.0 days (IQR: 6.0–8.0 days). According to the viral load, the distribution of the patients in the categories of low, medium, and high viremia were 173 (79.4%), 27 (12.4%), and 18 (8.2%), respectively. The median SOFA score was 10.5 (IQR: 6.2–13.0), indicating a considerable degree of critical illness among the patients (Table 1).
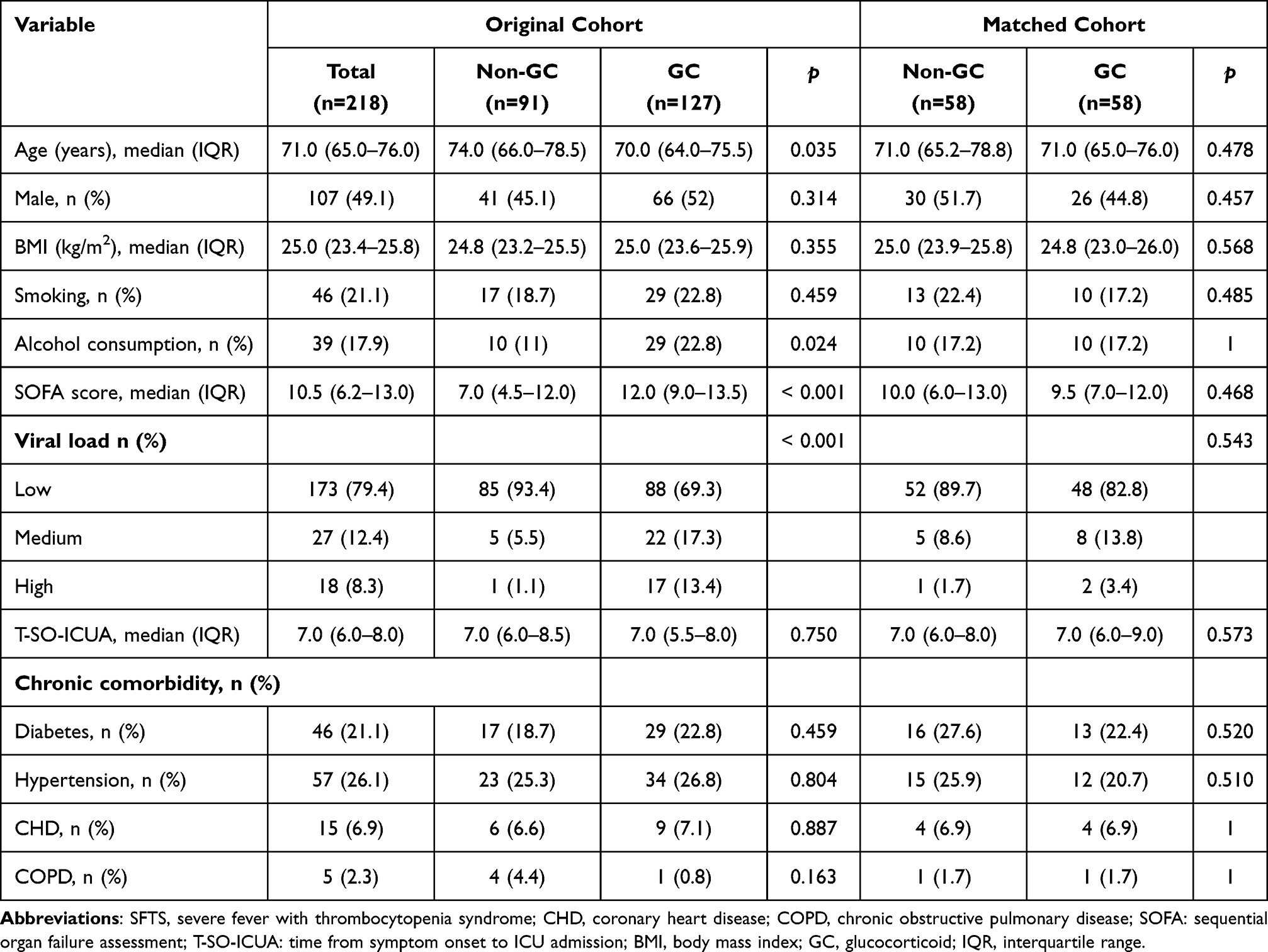 |
Table 1 Clinical Characteristics of Patients with SFTS in the Non-GC and GC Groups in the Original and Matched Cohorts |
 |
Figure 1 Flow chart of the study. Abbreviations: SFTS, severe fever with thrombocytopenia syndrome; GC, glucocorticoid; ICU, intensive care unit. |
A total of 127 patients (58.3%) received GC treatment in the ICU. In the unmatched cohorts, individuals who received GCs were younger (70 [64–75.5] vs 74 [66–78.5] years, p=0.035) and had higher SOFA scores (12.0 [9.0–13.5] vs 7.0 [4.5–12.0], p<0.001). However, factors such as sex, BMI, smoking status, T-SO-ICUA, and chronic comorbidities were not significantly different between the cohorts. After PSM, there were 58 patients in each group and there were no significant differences in the vital signs or laboratory variables between the GC and non-GC groups(Table 2).
 |
Table 2 Vital Signs and Lab Results of SFTS Patients in Non-GC and GC Groups in the Original and Matched Cohorts |
Clinical Outcomes with Propensity Score-Matched Cohorts
In our study of 218 patients, we observed a 28-day mortality rate of 61.5% (134 patients), mechanical ventilation in 61.9% (135 patients), CRRT in 21.1% (46 patients), median ICU stay of 4.0 days (range: 2.0–9.8 days), and median hospital stay of 8.0 days (range: 4.0–16.8 days). Complications, such as bleeding sites, secondary infections, and arrhythmias, are detailed in Table 3. Further analyses before PSM indicated that the GC group had higher rates of mortality (68.5% vs 51.6%; p=0.012), secondary infections (68.5% vs 51.6%; p=0.012), mechanical ventilation (79.5% vs 37.4%; p<0.001), CRRT (31.5% vs 6.6%; p<0.001), and arrhythmias (49.6% vs 35.2%; p=0.034) than the non-GC group did, highlighting the potential risks associated with GC treatment.
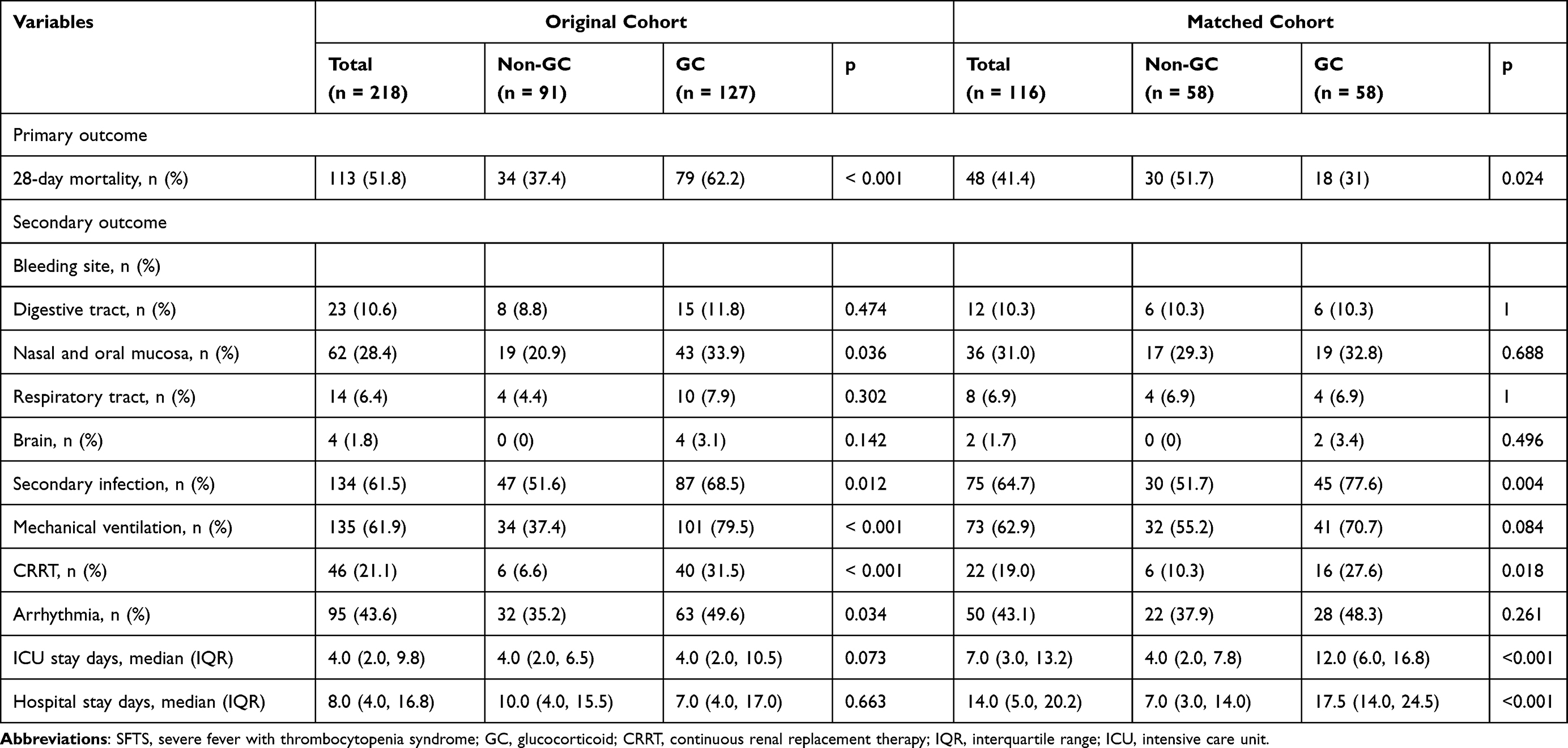 |
Table 3 Clinical Outcomes of Patients with SFTS in the Non-GC and GC Groups in the Original and Matched Cohorts |
Following PSM, we compared the clinical outcomes between the GC and non-GC groups (Table 3). The GC group demonstrated a significantly lower 28-day mortality rate compared to the non-GC group (31% vs 51.7%; p=0.024). The GC group exhibited significantly higher rates of secondary infections (77.6% vs 51.7%, p=0.004) and a greater likelihood of requiring CRRT (27.6% vs 10.3%, p=0.018) than the non-GC group did. Additionally, compared with the non-GC group, the GC group experienced longer ICU stays (12.0 days [range: 6.0–16.8] vs 4.0 days [range: 2.0–7.8], p<0.001) and hospital stays (17.5 days (range 14.0–24.5) vs 7.0 days (range 3.0–14.0), p<0.001), suggesting the association of complex outcomes with GC treatment. The post-PSM analysis further elucidated survival differences between the groups ([HR] 0.42, 95% confidence interval [CI]: 0.24–0.76, p=0.004), as shown in Figure 2.
 |
Figure 2 Kaplan–Meier survival plots differentiated by the administration of glucocorticoids. The survival curves of 58 patients with severe fever with thrombocytopenia syndrome who received glucocorticoids (illustrated using the red dashed line) compared with those of a matched group of 58 individuals who did not receive corticosteroid therapy (shown using the blue solid line). |
Subgroup Analyses
We conducted stratified and interaction analyses to examine the stability of the effect of GC treatment on 28-day mortality across different subgroups. Stratification using the GCS score, lactate levels, and use of immunoglobulin, norepinephrine, and antiviral drugs yielded consistent results (Figure 3). Significant improvements in the 28-day mortality rates with GCs were observed when the GCS score was below 13 (GCS score: 9–12, HR: 0.39, 95% CI: 0.17–0.88, p=0.024; GCS score: 3–8, HR: 0.09, 95% CI: 0.02–0.35, p=0.001), lactate levels exceeded 2 mmol/L (HR: 0.35, 95% CI: 0.15–0.83, p=0.017), and norepinephrine (HR: 0.26, 95% CI: 0.13–0.49, p<0.001) was used. Combining antiviral (HR: 0.41, 95% CI: 0.22–0.78, p=0.006) or immunoglobulin therapy (HR: 0.22, 95% CI: 0.1–0.51, p<0.001) with GC treatment significantly decreased the 28-day mortality rates, in contrast to GC monotherapy, which showed no such effect.
 |
Figure 3 Stratified analyses of the associations between GC use and 28-day mortality. Abbreviations: GC, glucocorticoid; HR, hazard ratio; CI, confidence interval. |
Discussion
In our investigation, we documented a mortality rate of 61.5% among patients with SFTS, the highest mortality rate ever reported. This finding underscores the pioneering nature of our research, as it represents the first comprehensive analysis of data from critically ill patients in an ICU setting. Our study not only highlights the acute challenges faced in managing severe SFTS cases but also sets a critical benchmark for future research and underscores the urgent need for enhanced clinical strategies in the ICU.
This study showed a balanced sex ratio, a median ICU admission duration of 7 days, and high SOFA scores. Older individuals were found to have an increased risk of mortality, a finding that aligns with those from prior research.10,15,16 High SOFA scores in ICU patients indicate poor organ function and are associated with a higher mortality risk.17 This study supports the idea that the severity of organ dysfunction, as measured using SOFA scores, is a key factor in determining outcomes in critically ill patients, including those with severe systemic inflammatory responses such as SFTS. When considering corticosteroid therapy in critically ill patients with SFTS, the effects of organ function on treatment effectiveness and patient survival must be considered.
A comparison between the GC and non-GC groups revealed that patients treated with GCs were younger and had higher SOFA scores. Although the benefits of GC use are inconclusive, GCs are often administered to patients with severe clinical conditions. However, after performing PSM, we observed that GCs lowered the 28-day mortality rate in ICU patients. Patients with lower GCS scores and higher lactate levels and those receiving vasopressors exhibited significantly better outcomes with GCs. This suggests that the effects of GCs are more pronounced in critically ill patients in the ICU with severe conditions.9 Case reports have demonstrated that methylprednisolone is effective in treating patients with SFTS complicated by encephalopathy. In such patients, disturbance of consciousness is suggested to be an indirect consequence of the cytokine storm induced by SFTSV infection.18 The underlying pathophysiological mechanisms contributing to the unfavorable outcomes in patients with SFTS likely involve a cytokine storm associated with hemophagocytic syndrome, bleeding tendencies due to thrombocytopenia, disseminated intravascular coagulation, and multiple organ system dysfunction.8 Thrombocytopenia caused by SFTSV infection is an immune response.19 GCs may also play a role in immune responses. For patients with severe diseases caused by emerging viruses, for which there are no specific drugs, such as coronavirus disease 2019, GCs have been shown to be effective, even reducing the 28-day mortality rates.20,21
The use of GCs for the treatment of SFTS is controversial, with clinical trials across various countries documenting their negative effects.9,11 Corticosteroid treatment can lead to serious side effects, such as osteoporosis, adrenal suppression, cardiac problems, and high blood sugar levels.22 Additionally, the immunosuppressive properties of GCs pose significant risks.23 In a single-center retrospective cohort study,10 GC treatment did not affect the fatality rate in patients with SFTS but increased the risk of secondary infections. Several studies24,25 have identified a significant link between SFTS and invasive pulmonary aspergillosis, with complication rates between 20% and 31.9%. This might explain the beneficial effects of antiviral drugs or immunoglobulins observed in this study. However, the administration of GCs in patients with SFTS requires careful consideration. Research indicates that while glucocorticoids are not advisable for mild cases, they may benefit patients with severe SFTS; however, these studies did not include ICU patients.12
Regarding the strengths of this study, this is the first cohort study on the prognosis of patients with SFTS in the ICU using GCs. Additionally, in contrast to previous studies, we conducted a rigorous evaluation by incorporating the SOFA scores and viral load into the PSM. This methodological approach effectively addressed significant confounding variables, thus providing strong evidence regarding the use of GCs in critically ill patients. Moreover, the efficacy of corticosteroid administration was investigated through stratification of patient situations by analyzing a broader patient cohort.
Our study has some limitations. This was a retrospective cohort study conducted at a single hospital. Although historical data may lack accuracy and completeness and may be subject to selection and information biases, we addressed these issues by applying PSM and the Cox regression model. The PSM was performed based on baseline and clinical characteristics, excluding the vital signs or investigations, with the exception of viral load. Following the reduction in sample size due to the matching process, the likelihood of committing a Type II error in our conclusions is heightened. This article focuses only on four common comorbidities and does not analyse additional comorbidities. Although the findings are promising, they need to be validated by prospective, randomized controlled trials before being widely implemented in clinical practice. Furthermore, patients who were administered GCs on the first day of ICU admission were included in the experimental group. We did not specify the corticosteroid types and dosages, nor did we include subsequent dose adjustments in our analysis. Therefore, future studies should investigate the relationship between corticosteroid therapy duration, dosage, and SFTS outcomes.
Conclusion
Patients with SFTS exhibit a heightened 28-day mortality rate, whereas the administration of GCs decreases the ICU mortality rates. This effect was most pronounced in individuals with low GCS scores, elevated lactate levels, norepinephrine support, and on antiviral or immunoglobulin therapy. These findings suggest a potential avenue for improving outcomes in patients with severe SFTS by identifying high-risk individuals and implementing targeted GC therapy in the ICU.
Abbreviations
SFTS, severe fever with thrombocytopenia syndrome; GC, glucocorticoid; PSM, propensity score matching; GCS, Glasgow coma scale; HR, hazard ratio; CI, confidence interval; SFTSV, severe fever with thrombocytopenia syndrome virus; ICU, intensive care unit; CRRT, continuous renal replacement therapy; T-SO-ICUA, time from symptom onset to ICU admission; SOFA, sequential organ failure assessment; BMI, body mass index; IQR, interquartile range.
Data Sharing Statement
The datasets presented in the current study are available from our database in-hospital system. The raw data required to reproduce the above findings cannot be shared at this time online as the data also forms part of an ongoing study.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Qishan Hospital (202401). Informed consent was not required as this was a retrospective observational study. In accordance with the guidelines set forth by the Declaration of Helsinki, this study was conducted with the utmost respect for patient confidentiality and ethical standards. Although patient consent to review medical records was not required by the Ethics Committee of Qishan Hospital, we have implemented strict measures to ensure that all patient data remains confidential and secure. All personal identifiers have been removed or anonymized to protect patient privacy, and the data will be used solely for the purpose of this study.
Consent for Publication
All authors gave their consent for publication.
Acknowledgments
We express our appreciation to the laboratories and associated researchers who were instrumental in obtaining the original samples and viral load data that were essential to our research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the 2023 Yantai Science and Technology Innovation Development Program (policy-oriented) projects under Grant [2023YD071]; the National Natural Science Foundation of China under Grant [82202366]; and Wu Jieping Medical Foundation Runze Fund for Critical Care Medicine under Grant (320·6750·2022-2-34).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Yu XJ, Liang MF, Zhang SY, et al. Fever with thrombocytopenia associated with a novel bunyavirus in China. N Engl J Med. 2011;364(16):1523–1532. doi:10.1056/NEJMoa1010095
2. Kim KH, Yi J, Kim G, et al. Severe fever with thrombocytopenia syndrome, South Korea, 2012. Emerg Infect Dis. 2013;19(11):1892–1894. doi:10.3201/eid1911.130792
3. Takahashi T, Maeda K, Suzuki T, et al. The first identification and retrospective study of severe fever with thrombocytopenia syndrome in Japan. J Infect Dis. 2014;209(6):816–827. doi:10.1093/infdis/jit603
4. Tran XC, Yun Y, Van An L, et al. Endemic severe fever with thrombocytopenia syndrome, Vietnam. Emerg Infect Dis. 2019;25(5):1029–1031. doi:10.3201/eid2505.181463
5. Zohaib A, Zhang J, Saqib M, et al. Serologic evidence of severe fever with thrombocytopenia syndrome virus and related viruses in Pakistan. Emerg Infect Dis. 2020;26(7):1513–1516. doi:10.3201/eid2607.190611
6. Agrati C, Sacchi A, Bordoni V, et al. Expansion of myeloid-derived suppressor cells in patients with severe coronavirus disease (COVID-19). Cell Death Differ. 2020;27(11):3196–3207. doi:10.1038/s41418-020-0572-6
7. Cui N, Liu R, Lu QB, et al. Severe fever with thrombocytopenia syndrome bunyavirus-related human encephalitis. J Infect. 2015;70(1):52–59. doi:10.1016/j.jinf.2014.08.001
8. Saijo M. Pathophysiology of severe fever with thrombocytopenia syndrome and development of specific antiviral therapy. J Infect Chemother. 2018;24(10):773–781. doi:10.1016/j.jiac.2018.07.009
9. Kawaguchi T, Umekita K, Yamanaka A, et al. Corticosteroids may have negative effects on the management of patients with severe fever with thrombocytopenia syndrome: a case-control study. Viruses. 2021;13(5):785. doi:10.3390/v13050785
10. Xiong L, Xu L, Lv X, Zheng X. Effects of corticosteroid treatment in patients with severe fever with thrombocytopenia syndrome: a single-center retrospective cohort study. Int J Infect Dis. 2022;122:1026–1033. doi:10.1016/j.ijid.2022.07.001
11. Jung SI, Kim YE, Yun NR, et al. Effects of steroid therapy in patients with severe fever with thrombocytopenia syndrome: a multicenter clinical cohort study. PLOS Negl Trop Dis. 2021;15(2):e0009128. doi:10.1371/journal.pntd.0009128
12. Wang G, Xu YL, Zhu Y, et al. Clinical efficacy of low-dose glucocorticoid therapy for critically ill patients with severe fever with thrombocytopenia syndrome: a retrospective cohort study. Int J Infect Dis. 2023;130:153–160. doi:10.1016/j.ijid.2023.03.015
13. Sun Y, Liang M, Qu J, et al. Early diagnosis of novel SFTS bunyavirus infection by quantitative real-time RT-PCR assay. J Clin Virol. 2012;53(1):48–53. doi:10.1016/j.jcv.2011.09.031
14. Li H, Lu QB, Xing B, et al. Epidemiological and clinical features of laboratory-diagnosed severe fever with thrombocytopenia syndrome in China, 2011-17: a prospective observational study. Lancet Infect Dis. 2018;18(10):1127–1137. doi:10.1016/S1473-3099(18)30293-7
15. Shin J, Kwon D, Youn SK, Park JH. Characteristics and factors associated with death among patients hospitalized for severe fever with thrombocytopenia syndrome, South Korea, 2013. Emerg Infect Dis. 2015;21(10):1704–1710. doi:10.3201/eid2110.141928
16. Li MM, Zhang WJ, Liu J, et al. Dynamic changes in the immunological characteristics of T lymphocytes in surviving patients with severe fever with thrombocytopenia syndrome (SFTS). Int J Infect Dis. 2018;70:72–80. doi:10.1016/j.ijid.2018.03.010
17. Yang K, Chen J, Chen Z, Zheng Y. Risk factors for death in patients with severe fever with thrombocytopenia syndrome. Am J Trop Med Hyg. 2023;109(1):94–100. doi:10.4269/ajtmh.22-0667
18. Nakamura S, Azuma M, Maruhashi T, et al. Steroid pulse therapy in patients with encephalopathy associated with severe fever with thrombocytopenia syndrome. J Infect Chemother. 2018;24(5):389–392. doi:10.1016/j.jiac.2017.11.004
19. Fang L, Yu S, Tian X, et al. Severe fever with thrombocytopenia syndrome virus replicates in platelets and enhances platelet activation. J Thromb Haemost. 2023;21(5):1336–1351. doi:10.1016/j.jtha.2023.02.006
20. Li G, Hilgenfeld R, Whitley R, De Clercq E. Therapeutic strategies for COVID-19: progress and lessons learned. Nat Rev Drug Discov. 2023;22(6):449–475. doi:10.1038/s41573-023-00672-y
21. Horby P, Lim WS, Emberson JR; RECOVERY Collaborative Group, et al. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384:693–704. doi:10.1056/NEJMoa2021436
22. Liu D, Ahmet A, Ward L, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol. 2013;9(1):30. doi:10.1186/1710-1492-9-30
23. Matthay MA, Thompson BT. Dexamethasone in hospitalised patients with COVID-19: addressing uncertainties. Lancet Respir Med. 2020;8(12):1170–1172. doi:10.1016/S2213-2600(20)30503-8
24. Xu Y, Shao M, Liu N, Tang J, Gu Q, Dong D. Invasive pulmonary aspergillosis is a frequent complication in patients with severe fever with thrombocytopenia syndrome: a retrospective study. Int J Infect Dis. 2021;105:646–652. doi:10.1016/j.ijid.2021.02.088
25. Bae S, Hwang HJ, Kim MY, et al. Invasive pulmonary aspergillosis in patients with severe fever with thrombocytopenia syndrome. Clin Infect Dis. 2020;70(7):1491–1494. doi:10.1093/cid/ciz673
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Associations Between Dysphagia and Adverse Health Outcomes in Older Adults with Dementia in Intensive Care Units: A Retrospective Cohort Study
Cheng H, Deng X, Li J, Tang Y, Yuan S, Huang X, Wang Z, Zhou F, Lyu J
Clinical Interventions in Aging 2023, 18:1233-1248
Published Date: 3 August 2023
A Retrospective Cohort Study: Predicting 90-Day Mortality for ICU Trauma Patients with a Machine Learning Algorithm Using XGBoost Using MIMIC-III Database
Yang S, Cao L, Zhou Y, Hu C
Journal of Multidisciplinary Healthcare 2023, 16:2625-2640
Published Date: 6 September 2023
Removal of Chlorhexidine for Ventilator-Associated Pneumonia Prevention with a Dentist Composing the Intensive Care Unit Team

Pains MB, Vieira IV, Figueiredo ARC, Diniz SCB, Figueiredo PTS
Journal of Multidisciplinary Healthcare 2024, 17:5299-5308
Published Date: 16 November 2024
Impact of New-Onset Atrial Fibrillation on Mortality in Critically Ill Patients
Zhang HD, Ding L, Mi LJ, Zhang AK, Liu YD, Li XN, Yan XX, Shen YJ, Tang M
Clinical Epidemiology 2024, 16:811-822
Published Date: 21 November 2024
Mean Systemic Filling Pressure Was Associated with 28-Day Mortality in Patients with Constrictive Pericarditis After Pericardial Stripping: A Retrospective Cohort Study
Chen R, Du W
International Journal of General Medicine 2025, 18:1359-1369
Published Date: 6 March 2025