")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Removal of Chlorhexidine for Ventilator-Associated Pneumonia Prevention with a Dentist Composing the Intensive Care Unit Team
Authors Pains MB , Vieira IV, Figueiredo ARC, Diniz SCB, Figueiredo PTS
Received 30 April 2024
Accepted for publication 16 August 2024
Published 16 November 2024 Volume 2024:17 Pages 5299—5308
DOI https://doi.org/10.2147/JMDH.S476253
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Marcos Barbosa Pains,1– 3 Isabel Verlangeiro Vieira,4 Arthur Rollemberg Cruciol Figueiredo,4 Suzaynne Corrêa Bittencourt Diniz,3 Paulo Tadeu Souza Figueiredo4
1School of Public Health of the Federal District, Foundation for Teaching and Research in Health Sciences, Brasília, Distrito Federal, Brazil; 2Faculty of Health Sciences, University of Brasília, Brasília, Distrito Federal, Brazil; 3Health Department of the Federal District, Government of the Federal District, Brasília, Distrito Federal, Brazil; 4Dentistry Department, University of Brasília, Brasília, Distrito Federal, Brazil
Correspondence: Marcos Barbosa Pains, Email [email protected]
Purpose: An association between the use of chlorhexidine in mechanically ventilated patients for the purpose of oral hygiene and the prevention of ventilator-associated pneumonia (VAP) lacks conclusive evidence in the literature. Therefore, this study aims to assess the clinical impact of such practice. This evaluation will consider that retention factors, infection foci, and oral biofilm will be regularly removed by a dentist.
Patients and Methods: In this retrospective cohort study, a comparison was made between two groups, one using chlorhexidine and the other using saline solution. Patients from both groups included in this study were admitted between January 2016 to March 2018. Data such as the incidence of VAP, duration of mechanical ventilation (DMV), length of stay (LOS), and mortality rate (MR) were collected and compared between the groups. Only patients aged 18 or older, under mechanical ventilation for more than 48 consecutive hours were included. Were excluded from this study patients with a diagnosis of VAP or other pulmonary infection upon admission or within the first 48 hours of hospitalization. Also not included were those who stayed in the ICU for less than 48 hours. Dental treatment was carried out addressing the regular removal of retention factors, potential oral infection foci, and oral biofilm by a dentist. Additionally, at each appointment, the visible biofilm was removed by the dentist themselves, and the maintenance of oral hygiene was performed daily by the nursing staff. For the statistical analysis the non-parametric Mann–Whitney test was used for comparisons between groups regarding LOS and DMV. Additionally, the associations between groups and VAP, outcomes (discharge or death), and diseases were analyzed using the chi-square test and Fisher’s exact test. A significance level of 5% was assumed.
Results: In both evaluated groups, each consisting of 36 patients, the incidence of VAP was identical at 2.8%. Specifically, the chlorhexidine group had an incidence of 2.105 VAP cases per 1000 days of mechanical ventilation (MV), while the placebo group had 2.865 VAP cases per 1000 days of MV (p = 1.000). No significant difference between groups regarding LOS (p = 0.5694) and DMV (p = 0.1136) was found. There was also no significant association between the MR in the two groups (47.2% chlorhexidine, 36.1% placebo) (p=0.3390).
Conclusion: When intensive oral care is performed, the use of chlorhexidine shows no significant change in VAP incidence, MR, LOS, and DMV. Therefore, the dentist, as part of the multiprofessional team, should decide on its use.
Keywords: dental care for chronically ill, chlorhexidine, ventilator-associated pneumonia, mortality, long of stay, duration of mechanical ventilation
Graphical Abstract:

Introduction
Critically ill patients often require ventilatory support and with that comes an increased risk for infection. As such, an important complication of mechanical ventilation (MV) is Ventilator-Associated Pneumonia (VAP), which may occur in those who are already in a critical condition with MV for at least 48 hours.1
To prevent such events, the use of chlorhexidine during oral hygiene in mechanically ventilated patients has been widely disseminated and previous articles have associated it with a reduction in the incidence of VAP ranging from 27% to 40%.1,2 However, such correlation is not a consensus among the established literature. Other articles have not only failed to show a reduction in VAP cases following the use of chlorhexidine but also found no changes in other patient-related outcomes, such as duration of mechanical ventilation (DMV) and length of stay (LOS) in the Intensive Care Unit (ICU). Since 2014, the Society for Healthcare Epidemiology of America has removed chlorhexidine from routine recommendations for all hospitals and categorized it as a special practice for hospitals with persistently high VAP rates despite the implementation of other basic measures.3 In 2022, this same organization, along with others, reiterated this removal in a new publication.4
The mechanisms for the potential increase in mortality are not fully established, but the hypothesis is that some patients may experience micro aspiration of chlorhexidine, leading to acute lung injury in patients under MV.5 It is known that dental biofilms and periodontal pockets serve as reservoirs for both organic matter and high microbial concentrations and that organic burden may inactivate chlorhexidine. In this regard, if good oral hygiene cannot be performed in critically ill patients, the application of any antiseptic may be of little value.6 However, the question still stands if the use of chlorhexidine would be beneficial in patients with regularly removed plaque in which the foci of infection and plaque retention are eliminated, manifesting through indicators such as mortality, incidence of VAP, length of stay (LOS), and duration of mechanical ventilation (DMV). Given these findings, we hypothesize that if effective and rigorous control of oral biofilm is carried out by a specialized professional, along with the elimination of infectious and biofilm-retentive foci, the use of chlorhexidine may be dispensable. If this hypothesis holds true, patients will benefit from not being exposed to antimicrobial agents and their associated risks, such as the potential increase in mortality caused by chlorhexidine and still have their oral infection sites eliminated.
The aim of this study is to assess, whether the removal of chlorhexidine in the oral hygiene of mechanically ventilated patients results in any changes in VAP incidence and mortality, considering that oral biofilm and potential oral infection foci will be regularly removed by a dentist. As secondary objectives, we also analyzed whether there is an indication for the use of chlorhexidine for all mechanically ventilated patients, based on LOS and DMV.
Material and Methods
Retrospective cohort study was conducted comparing two groups (experimental and placebo groups), of which all patients were admitted to the ICU and were on MV. Different solutions were used in both groups in conjunction with biofilm removal: 0.12% chlorhexidine in the experimental group, and saline solution in the placebo group. The sample was convenience-based, involving the investigation of all patients admitted during the study period. Records of admission and discharge from the adult ICU at the Hospital Regional de Ceilândia (HRC) were used to identify patients. For the definition of the control group, all patients admitted from July 2016 to September 2017 were included. During this period, chlorhexidine was not utilized due to the temporary discontinuation of the medication in that service. For the definition of the experimental group, which utilized chlorhexidine as an antiseptic, patients admitted in the six months prior to and six months following the placebo group were analyzed until reaching an equal number of participants. During this six-month period, chlorhexidine was utilized in all patients. A study removing dental care was not conducted because it had already been included in the unit’s protocol for over 5 years, and its removal would raise ethical concerns. After March 2018, changes occurred in the healthcare at HRC, including the addition of other dentists in the assistance unit. Therefore, a period after these changes cannot be considered to reduce the possibility of bias.
The following inclusion criteria was considered: patients over 18 years old; admitted to HRC from January 2016 to March 2018; admitted to the ICU under mechanical ventilation (MV) or with the initiation of ventilatory support after admission and with more than 48 consecutive hours of MV. The following were excluded from the sample: patients admitted with a diagnosis of VAP or other pulmonary infection; those who did not undergo MV; those who developed pneumonia before 48 hours of ventilation or who remained in the ICU for less than 48 hours. Patients with incomplete data were excluded from the sample, and patients with readmissions, regardless of the timeframe, were counted as the same patient if they met the inclusion criteria. The patients were enrolled in the study regardless of the condition of their teeth upon admission. Concerning the diagnosis of VAP, a clinical approach with a highly sensitive strategy was used, where the presence of new or progressive radiographic infiltrate, along with at least one of the clinical findings suggestive of infection (including new onset fever, purulent sputum, leukocytosis, and declining oxygenation) excluded the possibility of infections in other sites.7 The diagnosis was made independently by the team of intensive care physicians from the unit itself. Data collection began in 2020 but was interrupted due to the pandemic and workload overload, and resumed in 2023.
The Trakcare-InterSystems (Cambridge, MA, USA) database provided information about the patients, including data related to gender, age, date of admission, date of ICU discharge, DMV, time until ICU discharge, presence or absence of VAP, outcome (discharge or death), and reasons for each patient’s hospitalization. The incidence density rate of VAP (number of VAP episodes per 1000 ventilator days) eliminated two biases: the days when the patient was not under MV and the equalization between patients who spent a few days and those who spent many days on MV, with the latter having a higher likelihood of developing an infection. Regarding the bias caused by waiting for the availability of ward beds after actual ICU departure, ICU discharge was considered as soon as the term appeared in the medical record for the first time.
To assess whether the groups were balanced in terms of mortality risk, we utilized the Acute Physiology and Chronic Health Evaluation II (APACHE II) score. This index considers various patient data, examinations, vital signs and pre-existing chronic conditions on the day of admission. The APACHE II index was used to define the risk of mortality for patients after 24 hours of admission to the unit, with data collected or calculated based on the information presented in the medical records. It is necessary for the groups to have similar average APACHE II scores because different mortalities in groups with different mortality risks can be a potential bias factor.
All patients were treated in the ICU bed by the same dentist, who routinely (an average of 3 visits per week) performed diagnostic evaluation, prophylactic removal of visible biofilm, and aspiration of oral and oropharyngeal secretions. The mechanical removal of biofilm was performed using gauze soaked in chlorhexidine or saline solution, pinched with metal instruments with a ratchet mechanism, similar to needle holders, and oral suction with a dental aspirator and oropharyngeal suction with a tracheal suction catheter. Additionally, when necessary, the dentist performed specific dental procedures to control potential oral infection foci, such as restorations or cavity sealing, extractions, and scaling, for example. All dental procedures were performed at the bedside, in the ICU environment itself. The protocol followed by the nursing team involved maintaining oral hygiene at least once a day using gauze soaked in 0.12% chlorhexidine or saline solution, depending on the group, secured with adhesive tape to a wooden tongue depressor, and oral and oropharyngeal suction with a tracheal suction catheter.
Regarding the statistical analysis, descriptive and exploratory analyses of the data were initially performed. The results of quantitative variables portrayed means, standard deviations, medians, minimum values, and maximum values. For categorical variables, frequencies and percentages were presented. Since the data did not meet the assumptions of parametric analysis, the non-parametric Mann–Whitney test was applied for comparisons between groups regarding time until ICU discharge and DMV. Additionally, the associations between groups and VAP, outcomes (discharge or death), and diseases were analyzed using the chi-square test and Fisher’s exact test. A significance level of 5% was assumed, and the analyses were performed using the R software (R Core Team, 2023. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria). The research was approved by the Ethics Committee of the FEPECS (CAAE 73879423.4.0000.5553). The link to the protocol is: DOI: dx.doi.org/10.17504/protocols.io.3byl49k4rgo5/v1.
Results
Initially, 165 patient records were assessed for analysis of the inclusion and exclusion criteria. Of those, 93 records were excluded, mainly due to patients being admitted with pulmonary infections or having a duration of less than 48 hours on MV, leaving 72 records to be evaluated, with 36 in the chlorhexidine group and 36 in the placebo group.
Considering the total sample of 72 patients, 59.7% were admitted on account of infectious diseases (p=0.2296), 56.9% had renal diseases (p=0.2340), 44.4% had pulmonary diseases (p=0.6353), 40.3% had cardiovascular diseases (p=0.0306), 31.9% had postoperative conditions (p=0.0001), 16.7% had digestive diseases (p=0.0578), 15.3% had electrolyte imbalances (p=0.3257), 11.1% had blood disorders (p=0.7101), 8.3% had external causes diseases (p=0.6737), 8.3% had neurological diseases (p=0.6737), and 4.2% had other diseases (p=0.2394), as shown in Table 1. Cardiovascular disease was significant in the placebo group, and postoperative conditions were significant in the chlorhexidine group.
 |
Table 1 Frequency (%) of Patients According to Diseases in the Two Groups |
In both evaluated groups, only one patient from each group presented VAP, representing 2.8% of the patients (p=1.000), as shown in Table 2. In the chlorhexidine group, a total of 475 days of mechanical ventilation were recorded, with one case of VAP, resulting in an incidence rate of 2.105 VAP cases per 1000 days of mechanical ventilation. In the saline solution group, a total of 349 days of mechanical ventilation were recorded, also with one case of VAP, resulting in an incidence rate of 2.865 VAP cases per 1000 days of mechanical ventilation.
 |
Table 2 Incidence Rate for Ventilator-Associated Pneumonia |
There was no significant difference between the groups regarding time until ICU discharge (LOS) (p=0.5694) and DMV (p=0.1136), as shown in Table 3.
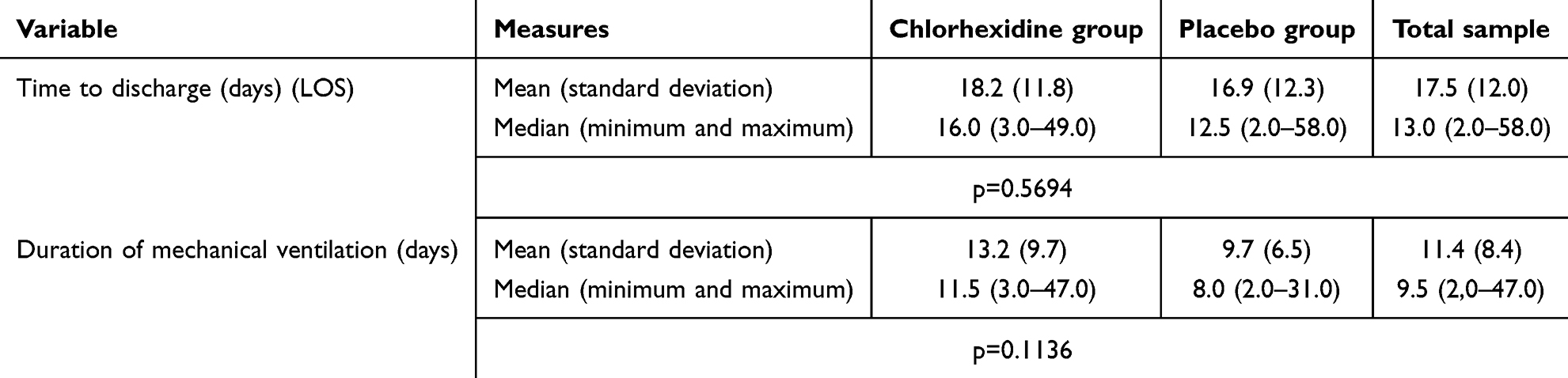 |
Table 3 Measures of Length of Stay and Duration of Mechanical Ventilation by Group |
In addition, it was observed that there was no significant difference between the outcome (discharge or death) between the two groups (p=0.3390), with the percentage of deaths being 47.2% in the chlorhexidine group and 36.1% in the placebo group, as shown in Table 4.
 |
Table 4 Frequency (%) of VAP and Outcome Categories by Group |
The average APACHE II score in the chlorhexidine group was 26.9, and in the placebo group, 25.74. The average risk of death in the chlorhexidine group was 50.26%, and in the placebo group, 49.25%. Furthermore, the MR was similar between the groups, as previously reported.
Discussion
Based on the results, we observed that when the biofilm is regularly removed by a dentist, the discontinuation of chlorhexidine use does not incur in any increase of VAP incidence, DMV, or LOS in the ICU. Additionally, there were no differences in MR associated with the use or non-use of chlorhexidine. In our view, the regular and meticulous removal of the biofilm and buccal potential oral infection foci is capable of effectively controlling the pathogens that cause VAP, resulting in low incidence rates of VAP in both groups. In this regard, we recommend the inclusion of a dentist as part of the multidisciplinary team in the ICU to perform procedures aimed at maintaining biofilm levels as low as possible and to make decisions regarding the use of chlorhexidine.
When comparing our study with the literature, we found incidence rates of VAP ranging from 4.9% to 68.8%.8,9 In this research, in terms of percentages, the incidence was 2.8% for both groups, contrasting with the current literature, which shows higher values, as demonstrated. When the indicator utilized is the incidence rate per 1000 ventilator days, the same authors showed the lowest and highest values, ranging from 7 to 21.8 In relation to this indicator, this research obtained an incidence rate per 1000 ventilator days of 2.105 in the chlorhexidine group and 2.856 in the placebo group. We emphasize that the best indicator to measure VAP incidence is the infection rate per 1000 ventilator days, rather than the percentage, due to biases explained in the methodology of this study. Another factor to consider is the type of ICU being studied. In this regard, the location where the research was conducted is considered a generalist ICU, with an average DMV of 9.5 (2.0–47.0) days. It would be expected to have a higher incidence of VAP compared to specialized ICUs, such as cardiac postoperative ICUs, where the DMV tends to be shorter and the incidence of VAP is also lower.5 Lower-middle-income countries also have more cases of VAP.9 Apparently, the low rates presented in this research, despite the unfavorable characteristics of the studied ICU, may have occurred due to the presence of a dental professional performing the elimination of potential oral infection foci and the meticulous removal of biofilm retention sites as part of the biofilm removal protocol, including the removal of all visible biofilm during each evaluation.
Comparing studies on the use of chlorhexidine versus placebo/saline solution, research shows favorable results for chlorhexidine.5,10 In 2014, despite low rates of VAP associated with the use of chlorhexidine, authors expressed reservations regarding the possibility of increased mortality.5,11 Moreover, some authors conducted meta-analyses and demonstrated that chlorhexidine is associated with a reduction in VAP rates.12–14 This effect occurs when chlorhexidine is combined with mechanical biofilm control techniques.14
In contrast, some studies have failed to show a reduction in VAP when chlorhexidine is used.8,15,16 However, the rates of VAP were significantly higher than those observed in this study. Another review indicated a significant reduction in infections among patients undergoing cardiac surgery who utilized chlorhexidine, but no such decrease was observed in the group without cardiac surgery.5 This data aligns with the findings of our study, which was conducted on patients in non-cardiac surgical ICU, where chlorhexidine did not decrease the risk of VAP compared to placebo. According to the authors of the same review, although the study is not conclusive, it is sufficient to suggest that oral hygiene protocols with chlorhexidine in non-cardiac surgery patients should be reevaluated. They argue that previous meta-analyses showing correlation between chlorhexidine use and decrease in VAP incidence may be flawed. The argument was based in not considering the differences between patients in cardiac surgical and non-cardiac surgical ICUs, lacking blinded and double-blind study designs, and not adequately emphasizing patient-centered outcomes such as ventilation duration, hospital stay, and mortality. More recently, retrospective cohort studies found no significantly lower risk for VAP in patients using chlorhexidine or no reduction in VAP with the removal of chlorhexidine.17,18
Based on current literature, we can notice a tendency to consider chlorhexidine as having low efficacy in reducing VAP in patients who have not undergone cardiac surgery, which is in line with this study. On the other hand, the very low incidence rates of VAP presented here are noteworthy, even though the study was conducted in a developing country, where higher numbers would be expected.19 Apparently, the presence of a dentist providing intensive oral care, including prophylactic removal of visible biofilm three times a week on average and the elimination of potential oral infection foci, along with the removal of sites that promote the accumulation of oral biofilm, such as dental calculus, cavity sealing, and removal of residual roots, were responsible for maintaining infection foci so low that chlorhexidine did not show improvement in the indicators. Based on the above, it is suggested that intensive oral care with excellent biofilm control may be more important than the use of adjunct substances such as chlorhexidine.
Regarding mortality, a trend of increased MR with the use of chlorhexidine was identified in three previous studies. In the first study, no significant difference in mortality was found between the chlorhexidine and placebo groups.5 However, this systematic review demonstrated discrepancies in the results between double-blind studies compared to non-blinded studies. Although not statistically significant, there was a trend towards increased mortality with higher concentrations of chlorhexidine, with greater effect observed in the gel formulation compared to the liquid formulation. Some authors have speculated that some patients may aspirate chlorhexidine, leading to acute lung injury.2,5 In the second study, a review found a ratio of 1.25 (1.05 to 1.50), unfavorable to chlorhexidine, despite a significant increase in mortality observed in only one of the 11 studies included.11,20 In this last study, the group using only chlorhexidine (swab) had a MR of 30%, while the groups with chlorhexidine-associated brushing, brushing alone, and usual care had mortality rates of 25%, 20%, and 18%, respectively.20 In the third study, a retrospective cohort, a higher relative risk for mortality was observed with chlorhexidine (RR, 1.63; 95% CI, 1.15–2.31; P = 0.006), it should be noted that the study design did not allow for the formation of balanced comparison groups with respect to mortality risk.17
In this study, the average risk of mortality in the chlorhexidine group was 50.26% and in the placebo group was 49.25%, based on the admission APACHE II of each individual. Additionally, the MR in the chlorhexidine group was 47.2% and in the placebo group was 36.1% (p=0.339), indicating no statistically significant difference between the groups. Therefore, given the similar risk between the groups and the absence of statistically higher mortality in patients exposed to chlorhexidine, it is not possible to conclude from this study that chlorhexidine is associated with an increased risk of mortality, despite the higher percentage of deaths observed.
The literature is abundant when it comes to studies that do not indicate unfavorable results regarding chlorhexidine in relation to mortality in ventilated patients. With various designs, several researchers have reached this conclusion when comparing chlorhexidine to placebo/saline solution.8,10,15,16,21 Finally, three meta-analyses did not find increased mortality in patients who used chlorhexidine.1,12,13 In the most recent one, the authors concluded that prophylactic use of chlorhexidine in critically ill patients admitted to ICU did not have a significant impact on mortality.12 Furthermore, there is a study where a reduction in mortality is reported in the chlorhexidine group.22
An important caveat should be noted regarding the risk of death in patients and the actual MR they experience. When comparing two groups in terms of MR, it is ideal for the risk of death to be similar between them. The risk of mortality can be assessed using various methods, such as APACHE II, APACHE III, APR-DRG and others. Some studies have taken this care, but no increased mortality was observed.8,10,15,20,21 It is important to note that the other articles mentioned here did not require the groups to have similar mortality risks, and therefore, caution should be exercised when interpreting their conclusions regarding the relationship between chlorhexidine and mortality.
Other important data to be considered are the DMV and LOS in the ICU. In this regard, several studies have compared chlorhexidine with placebo, and none of them have demonstrated any favorable benefits of chlorhexidine in terms of DMV and LOS in the ICU.1,2,16 Additionally, other studies concluded that chlorhexidine does not have an impact on the DMV.17,21 Similarly, the present study did not find any differences in the DMV or LOS in the ICU, which is consistent with the current literature.1,2,16,17
In an editorial, it has been suggested that in the current state of scientific knowledge, the best alternative is an individualized approach to oral care that considers the ability to maintain oral health independently and considers the patients’ risk profile.23 Similarly, a study suggests that the use of chlorhexidine should preferably be applied by a dental professional, limited only to those with oral infections such as periodontal disease. For that matter, the proposals of these two authors support the idea that the use of chlorhexidine should be evaluated on a case-by-case basis, and it is obviously necessary for a qualified professional to identify cases where its use is indicated.24
Based on the presented results and considering the current literature, we did not find any advantages in its use of chlorhexidine. In this sense, our results suggest that, even as an external validation, rather than relying on antiseptic agents such chlorhexidine, it is more important to prioritize the complete and continuous removal of all oral biofilm and factors that contribute to its retention. In this context, the role of a dental professional appears to be of utmost importance, and the use of chlorhexidine can be optional, not due to the risk of increased mortality, but because its effectiveness is similar to that of saline solution in reducing VAP, LOS, and duration of mechanical ventilation when the biofilm and its retention factors are eliminated. Seemingly, when there is a dental professional as part of the multidisciplinary team capable of assessing and maintaining oral health, the use of chlorhexidine may be unnecessary. In this context, the decision regarding its use remains at the discretion of the dentist. In addition, it is the dentist’s role to develop, along with the multidisciplinary team, a continuous training program aimed at equipping them to provide oral care focused on the proper removal of biofilm and the maintenance of low plaque indices.25
It is important to note that this study has limitations, such as being retrospective, lack of blinding, absence of randomization, and sample size. However, it provides valuable insights for future research, including the role of dental professionals in ICU teams and the importance of mechanical removal of oral biofilm instead of relying solely on antimicrobial solutions or innovative techniques for biofilm control. To address these questions, it is necessary to conduct large-scale, randomized, prospective, blind clinical studies with a homogenized mortality risk between groups. Furthermore, calculating the incidence of VAP based on 1000 ventilator days rather than the percentage of affected patients is preferable.
Conclusion
When intensive oral care is carried out, including meticulous biofilm removal, elimination of factors contributing to biofilm retention, treatment of potential oral infection foci, and the involvement of a dentist in the multidisciplinary team, the choice of adjunctive substance for biofilm removal may not be crucial, as there is no significant difference in the incidence of VAP, MR, LOS e DMV. However, the decision to use chlorhexidine should be made by the dentist as part of health professionals ICU’s team.
Abbreviations
APACHE, Acute Physiology and Chronic Health Evaluation; APR-DRG, All Patient-Refined Diagnosis-Related Groups; HRC, Regional Hospital of Ceilândia; MA, Massachusetts; VAP, Ventilator-associated pneumonia; RR, Relative risk; MR, Mortality rate; LOS, Length of stay; DMV, Duration of mechanical ventilation; ICU, Intensive Care Unit; MV, Mechanical ventilation.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due individual privacy could be compromised but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by Comitê de Ética em Pesquisa da Fundação de Ensino e Pesquisa em Ciências da Saúde (FEPECS) registration code: CAAE 73879423.4.0000.5553. All the procedures were performed in accordance with the ethical standards on human experimentation and with the Helsinki Declaration of 1975 and its later amendments. Patients or family members whose contact could not be established (due to outdated registration data) did not provide consent (according to permission from the Research Ethics Committee), but the others consented to participate in the research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
All the study was carried out with the authors’ own resources, not obtaining any type of external funding.
Disclosure
The authors declare that they have no competing interests.
References
1. Shi Z, Xie H, Wang P, et al. Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia. Cochrane Database Syst Rev. 2013;(8):CD008367.
2. Klompas M. Oropharyngeal Decontamination with Antiseptics to Prevent Ventilator-Associated Pneumonia: rethinking the Benefits of Chlorhexidine. Semin Respir Crit Care Med. 2017;38(3):381–390.
3. Klompas M, Branson R, Eichenwald EC, et al. Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(2):S133–54.
4. Klompas M, Branson R, Cawcutt K, et al. Strategies to prevent ventilator-associated pneumonia, ventilator-associated events, and nonventilator hospital-acquired pneumonia in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol. 2022;43(6):687–713.
5. Klompas M, Speck K, Howell MD, Greene LR, Berenholtz SM. Reappraisal of routine oral care with chlorhexidine gluconate for patients receiving mechanical ventilation: systematic review and meta-analysis. JAMA Intern Med. 2014;174(5):751–761.
6. Bellissimo-Rodrigues WT, Menegueti MG, Gaspar GG, et al. Effectiveness of a dental care intervention in the prevention of lower respiratory tract nosocomial infections among intensive care patients: a randomized clinical trial. Infect Control Hosp Epidemiol. 2014;35(11):1342–1348.
7. Society AT, IDSo A. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416.
8. Tantipong H, Morkchareonpong C, Jaiyindee S, Thamlikitkul V. Randomized controlled trial and meta-analysis of oral decontamination with 2% chlorhexidine solution for the prevention of ventilator-associated pneumonia. Infect Control Hosp Epidemiol. 2008;29(2):131–136.
9. Papazian L, Klompas M, Luyt CE. Ventilator-associated pneumonia in adults: a narrative review. Intensive Care Med. 2020;46(5):888–906.
10. Özçaka Ö, Başoğlu ÖK, Buduneli N, Taşbakan MS, Bacakoğlu F, Kinane DF. Chlorhexidine decreases the risk of ventilator-associated pneumonia in intensive care unit patients: a randomized clinical trial. J Periodontal Res. 2012;47(5):584–592. doi:10.1111/j.1600-0765.2012.01470.x
11. Price R, MacLennan G, Glen J, Collaboration S. Selective digestive or oropharyngeal decontamination and topical oropharyngeal chlorhexidine for prevention of death in general intensive care: systematic review and network meta-analysis. BMJ. 2014; 348:g2197.
12. Lee S, Lighvan NL, McCredie V, et al. Chlorhexidine-Related Mortality Rate in Critically Ill Subjects in Intensive Care Units: a Systematic Review and Meta-Analysis. Respir Care. 2019;64(3):337–349.
13. Hua F, Xie H, Worthington HV, Furness S, Zhang Q, Li C. Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia. Cochrane Database Syst Rev. 2016;10:CD008367.
14. Pinto ACDS, Silva BMD, Santiago-Junior JF, Sales-Peres SHC. Efficiency of different protocols for oral hygiene combined with the use of chlorhexidine in the prevention of ventilator-associated pneumonia. J Bras Pneumol. 2021;47(1):e20190286.
15. Scannapieco FA, Yu J, Raghavendran K, et al. A randomized trial of chlorhexidine gluconate on oral bacterial pathogens in mechanically ventilated patients. Crit Care. 2009;13(4):R117.
16. Kusahara DM, Peterlini MA, Pedreira ML. Oral care with 0.12% chlorhexidine for the prevention of ventilator-associated pneumonia in critically ill children: randomised, controlled and double-blind trial. Int J Nurs Stud. 2012;49(11):1354–1363.
17. Klompas M, Li L, Kleinman K, Szumita PM, Massaro AF. Associations Between Ventilator Bundle Components and Outcomes. JAMA Intern Med. 2016;176(9):1277–1283.
18. Dale CM, Rose L, Carbone S, et al. Effect of oral chlorhexidine de-adoption and implementation of an oral care bundle on mortality for mechanically ventilated patients in the intensive care unit (CHORAL): a multi-center stepped wedge cluster-randomized controlled trial. Intensive Care Med. 2021;47(11):1295–1302.
19. Wu D, Wu C, Zhang S, Zhong Y. Risk Factors of Ventilator-Associated Pneumonia in Critically III Patients. Front Pharmacol. 2019;10:482.
20. Munro CL, Grap MJ, Jones DJ, McClish DK, Sessler CN. Chlorhexidine, toothbrushing, and preventing ventilator-associated pneumonia in critically ill adults. Am J Crit Care. 2009;18(5):428–437.
21. Deschepper M, Waegeman W, Eeckloo K, Vogelaers D, Blot S. Effects of chlorhexidine gluconate oral care on hospital mortality: a hospital-wide, observational cohort study. Intensive Care Med. 2018;44(7):1017–1026.
22. DeRiso AJ, Ladowski JS, Dillon TA, Justice JW, Peterson AC. Chlorhexidine gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory infection and nonprophylactic systemic antibiotic use in patients undergoing heart surgery. Chest. 1996;109(6):1556–1561.
23. Labeau SO, Conoscenti E, Blot SI. Less daily oral hygiene is more in the ICU: not sure. Intensive Care Med. 2021;47(3):334.
24. Bellissimo-Rodrigues WT, Menegueti MG, de Macedo LD, Basile-Filho A, Martinez R, Bellissimo-Rodrigues F. Oral mucositis as a pathway for fatal outcome among critically ill patients exposed to chlorhexidine: post hoc analysis of a randomized clinical trial. Crit Care. 2019;23(1):382.
25. Ribeiro ILA, Bellissimo-Rodrigues WT, Mussolin MG, et al. Impact of a dental care intervention on the hospital mortality of critically ill patients admitted to intensive care units: a quasi-experimental study. Am J Infect Control. 2022;50(10):1156–1161.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Associations Between Dysphagia and Adverse Health Outcomes in Older Adults with Dementia in Intensive Care Units: A Retrospective Cohort Study
Cheng H, Deng X, Li J, Tang Y, Yuan S, Huang X, Wang Z, Zhou F, Lyu J
Clinical Interventions in Aging 2023, 18:1233-1248
Published Date: 3 August 2023
A Retrospective Cohort Study: Predicting 90-Day Mortality for ICU Trauma Patients with a Machine Learning Algorithm Using XGBoost Using MIMIC-III Database
Yang S, Cao L, Zhou Y, Hu C
Journal of Multidisciplinary Healthcare 2023, 16:2625-2640
Published Date: 6 September 2023
Impact of Glucocorticoid Therapy on 28-Day Mortality in Patients Having Severe Fever with Thrombocytopenia Syndrome in an Intensive Care Unit: A Retrospective Analysis
Wang G, Liu P, Xie H, Niu C, Lyu J, An Y, Zhao H
Journal of Inflammation Research 2024, 17:7627-7637
Published Date: 24 October 2024
Impact of New-Onset Atrial Fibrillation on Mortality in Critically Ill Patients
Zhang HD, Ding L, Mi LJ, Zhang AK, Liu YD, Li XN, Yan XX, Shen YJ, Tang M
Clinical Epidemiology 2024, 16:811-822
Published Date: 21 November 2024
A Nomogram for Diagnosing Ventilator-Associated Pneumonia Using Circulating Inflammation Indicators in ICU Patients
Yang J, Bao W, Wang H, Zhou J, Hu Q, Wang Y, Li Y
Journal of Inflammation Research 2025, 18:4615-4625
Published Date: 2 April 2025