")
Back to Journals » Drug Design, Development and Therapy » Volume 18
Intranasal Dexmedetomidine-Esketamine Combination Premedication versus Monotherapy for Reducing Emergence Delirium and Postoperative Behavioral Changes in Pediatric Tonsillectomy and/or Adenoidectomy: A Randomized Controlled Trial
Authors Liao Y , Xie S, Zhuo Y, Chen S , Luo Y, Wei Y, Yao Y
Received 25 July 2024
Accepted for publication 9 October 2024
Published 23 October 2024 Volume 2024:18 Pages 4693—4703
DOI https://doi.org/10.2147/DDDT.S488706
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Yanling Liao,1,* Siyu Xie,2,* Yifen Zhuo,3,* Sisi Chen,1 Yuxin Luo,1 Ying Wei,4 Yusheng Yao1
1Department of Anesthesiology, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, Fuzhou, People’s Republic of China; 2Department of Anesthesiology, Longyan First Affiliated Hospital of Fujian Medical University, Longyan, People’s Republic of China; 3Department of Anesthesiology, Xiamen Haicang Hospital, Xiamen, People’s Republic of China; 4Department of Anesthesiology, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ying Wei, Department of Anesthesiology, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, 18 Daoshan Road, Fuzhou, 350025, People’s Republic of China, Email [email protected] Yusheng Yao, Department of Anesthesiology, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, 134 Dongjie Street, Fuzhou, 350001, People’s Republic of China, Email [email protected]
Purpose: Emergence delirium and postoperative negative behavioral changes (PNBC) are common complications in pediatric anesthesia. This study evaluated whether intranasal premedication combining dexmedetomidine and esketamine more effectively reduces these complications compared to either drug alone in children undergoing tonsillectomy and/or adenoidectomy with sevoflurane anesthesia.
Patients and Methods: This randomized, double-blind trial involved 198 children aged 2− 5 years undergoing tonsillectomy and/or adenoidectomy. Participants received intranasal premedication with either dexmedetomidine (2 μg/kg), esketamine (1 mg/kg), or their combination (dexmedetomidine 1 μg/kg plus esketamine 0.5 mg/kg). The primary outcome was the incidence of emergence delirium, defined as a Pediatric Anesthesia Emergence Delirium (PAED) scale score ≥ 10. Secondary outcomes included the incidence of PNBC, sedation depth, easiness of separation from parents, acceptance of the mask for induction, emergence time, postoperative pain score, parental satisfaction, and adverse events.
Results: The combination premedication significantly reduced emergence delirium incidence (9.4%) compared to esketamine alone (38.1%; relative risk [RR] 0.25, 95% confidence interval [CI] 0.11– 0.57, p < 0.001), but not compared to dexmedetomidine alone (17.2%; RR 0.55, 95% CI 0.21– 1.39, p = 0.193). PNBC incidence at day 7 was lower with the combination (28.1%) versus dexmedetomidine (48.4%; RR 0.58, 95% CI 0.36– 0.93, p = 0.018), but not significantly different from esketamine alone (20.6%; RR 1.38, 95% CI 0.74– 2.58, p = 0.326). The combination also provided significantly superior sedation, improved ease of separation from parents, better acceptance of the mask for induction, shorter emergence time, and higher parental satisfaction than both monotherapies.
Conclusion: In children undergoing tonsillectomy and/or adenoidectomy with sevoflurane anesthesia, intranasal dexmedetomidine-esketamine premedication more effectively reduces emergence delirium compared to esketamine alone and PNBC compared to dexmedetomidine alone. This combination also improves sedation, shortens emergence times, and enhances parental satisfaction compared to monotherapy without significant adverse effects.
Trial Registration: The Chinese Clinical Trial Registry, ChiCTR2300076709.
Keywords: adenoidectomy, dexmedetomidine, emergence delirium, esketamine, intranasal administration, pediatric anesthesia, postoperative complications, tonsillectomy
Graphical Abstract:

Introduction
Sevoflurane, widely used in pediatric anesthesia, is associated with a high incidence of emergence delirium in children, with most studies reporting rates between 30% and 50%.1–3 Although typically transient, emergence delirium raises significant concerns due to potential risks, including self-injury, surgical site disruption, postoperative complications, increased nursing care needs, prolonged post-anesthesia care unit (PACU) stay, and reduced parental satisfaction.4,5 Children experiencing emergence delirium are also at higher risk of developing postoperative negative behavioral changes (PNBC),6 which may persist and impact recovery and well-being. While emergence delirium and PNBC are related phenomena, they have a key distinction. Glumac et al7 demonstrated that PNBC does not affect consciousness, whereas altered consciousness is a defining feature of delirium.
Preoperative anxiety, a key predictor of emergence delirium and PNBC,8,9 is particularly challenging in pediatric surgical patients. Researchers have explored various pharmacological agents as premedication to reduce anxiety and facilitate smooth anesthesia induction.10,11 The ideal premedication should be readily accepted by children, have rapid onset and offset, and produce minimal adverse effects. Intranasal dexmedetomidine, increasingly used in pediatric practice, offers beneficial anxiolytic properties with limited respiratory depression.12 However, it may be associated with delayed onset, bradycardia, and hypotension.13 Esketamine, a ketamine enantiomer, could potentially complement dexmedetomidine by addressing these limitations, offering a balanced approach to pediatric premedication.14
This study aimed to evaluate the efficacy of intranasal dexmedetomidine, esketamine, and their combination as premedication in reducing emergence delirium and PNBC in preschool-aged children undergoing tonsillectomy and/or adenoidectomy with sevoflurane anesthesia. Our primary hypothesis was that the combined intranasal premedication of dexmedetomidine and esketamine would reduce the incidence of emergence delirium and PNBC more effectively compared to either agent alone.
Materials and Methods
Study Setting and Participants
This prospective, randomized, double-blind, three-arm clinical trial was conducted at Fujian Provincial Hospital, a tertiary academic medical center in Fuzhou, China. The Institutional Review Board of Fujian Provincial Hospital approved the study protocol (identifier: K2021−12−068/02). The trial was registered with the Chinese Clinical Trial Registry (https://www.chictr.org.cn/showprojEN.html?proj=208255, identifier: ChiCTR2300076709) on October 17, 2023, and conducted from October 19, 2023, to June 24, 2024. The study adhered to the Declaration of Helsinki, Chinese local regulations, and the Consolidated Standards of Reporting Trials (CONSORT) statement.15 Parents or legal guardians provided written informed consent after being informed of the study’s objectives, procedures, potential risks, and benefits.
The study included children aged 2–5 years with American Society of Anesthesiologists (ASA) physical status I–II, scheduled for tonsillectomy and/or adenoidectomy. Exclusion criteria included acute upper respiratory infections; allergies to study medications; use of sedatives or analgesics within 48 hours pre-procedure; body mass index ≥ 30 kg/m²; developmental delays; mental or neurological disorders; and exposure to significant life stressors (eg, changes in home/school environment, parental divorce or death) within one month before surgery.
Randomization and Blinding
Eligible participants were randomized in a 1:1:1 ratio to receive intranasal premedication with either dexmedetomidine (2 μg/kg), esketamine (1 mg/kg), or their combination (dexmedetomidine 1 μg/kg plus esketamine 0.5 mg/kg). Randomization was conducted using a computer-generated sequence with variable block sizes (4, 6, and 8) to ensure balanced group allocation. A research assistant not involved in patient care or data collection generated the randomization sequence using the “blockrand” package in R version 4.0.5. Allocation concealment was achieved using sequentially numbered, opaque, sealed envelopes. On the day of surgery, an independent assistant opened the envelopes, revealed group assignments, and prepared study medications in identical syringes labeled only with participant numbers. This process ensured the blinding of children’s parents, attending anesthesiologists, nursing staff, and study personnel responsible for data collection and analysis throughout the study.
Study Procedures
Patients fasted according to standard pediatric anesthesia guidelines (8 hours for solids, 2 hours for clear fluids). Standard monitoring (pulse oximetry, electrocardiography, and noninvasive blood pressure) was initiated in the operating room. Intranasal premedication was administered 30 minutes before anesthesia induction, with study medications evenly distributed between nostrils using a mucosal atomization device (MAD 140, Wolfe Tory Medical, Inc., USA).
Anesthesia was induced with 8% sevoflurane in 100% oxygen (fresh gas flow 8 L/min). After establishing intravenous access, sufentanil (0.3 μg/kg), propofol (2.0 mg/kg), and mivacurium (0.2 mg/kg) were administered for intubation. Anesthesia was maintained with 2–4% sevoflurane. Post-intubation, patients received intravenous dexamethasone (0.15 mg/kg) and ondansetron (0.1 mg/kg) for prophylaxis against postoperative nausea and vomiting (PONV). In the PACU, extubated children were accompanied by parents or guardians and received oxygen via nasal cannula until fully alert. The analgesic protocol included intraoperative rectal paracetamol (20 mg/kg) and intravenous flurbiprofen axetil (1 mg/kg), followed by postoperative oral ibuprofen (10 mg/kg every 8 hours) for two days. Rescue analgesia (intravenous morphine 25 μg/kg) was given for Face, Legs, Activity, Cry, and Consolability (FLACC) pain scores > 3.
Outcome Measures
The primary outcome was the incidence of emergence delirium, defined as a peak Pediatric Anesthesia Emergence Delirium (PAED) scale score ≥ 10.16 The PAED scale assesses five items (eye contact, purposefulness of actions, awareness of surroundings, restlessness, and inconsolability) on a 0−4 scale, yielding total scores from 0 to 20. Secondary outcomes included incidence of PNBC, sedation level, ease of parental separation, mask acceptance during induction, emergence time, postoperative pain score, parental satisfaction with anesthesia, and adverse events.
PNBC was assessed using the 11-item Post-Hospitalisation Behaviour Questionnaire for Ambulatory Surgery (PHBQ-AS) postoperatively on days 1, 3, and 7.17 PHBQ-AS scores were averaged from item scores (1–5 per item; “not applicable” or missing data = 3), with scores > 3 indicating PNBC. Preoperative anxiety was assessed using the modified Yale Preoperative Anxiety Scale (m-YPAS).18 The sedation depth was evaluated 30 minutes after premedication administration using the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) Scale.19 Parental separation ease was rated on the Parental Separation Anxiety Scale (PSAS): 1 (easy) to 4 (crying/clinging).20 Mask acceptance during induction was categorized as: 1 (willingly accepts), 2 (mild resistance), or 3 (refuses/requires persuasion). Postoperative pain was assessed in the PACU using the FLACC scale (0 = no pain, 10 = severe pain).21 Emergence time was measured from anesthesia cessation to verbal command response. Parental satisfaction with anesthesia was reported at 24 hours using a 5-point Likert scale (1 = strongly dissatisfied; 5 = strongly satisfied). A single, blinded research nurse collected all the data.
Sample Size Calculation
The primary objective was to determine whether the combination of dexmedetomidine and esketamine premedication would reduce the incidence of emergence delirium more effectively than either drug administered alone. A pilot study (n = 10 per group) indicated emergence delirium rates of 30% for dexmedetomidine, 40% for esketamine, and 10% for the combination. To detect a difference in emergence delirium incidence between the combination and each monotherapy, we calculated a required sample size of 62 patients per group. This sample size provided 80% power compared to dexmedetomidine and over 90% power compared to esketamine (two-sided Z-test with pooled variance, α = 0.05). Accounting for a 5% attrition rate, we enrolled 66 patients per group, totaling 198 patients.
Statistical Analysis
Data analysis was performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA) based on the modified intention-to-treat principle. Missing data were handled through multiple imputations using chained equations under a missing at random assumption, implemented in R version 4.3.1 (package “mice”) with 10 imputations generated for each missing value. We assessed the normality of continuous variables’ distribution using the Shapiro–Wilk test. Variables were presented as mean ± standard deviation (SD) for normally distributed data, median (interquartile range, IQR) for non-normally distributed data, or number (proportion) for categorical data.
Statistical analysis of continuous variables utilized one-way ANOVA for normally distributed data, with Tukey’s HSD test for post-hoc comparisons when significant. Non-normally distributed data were analyzed using the Kruskal–Wallis test, followed by Dunn’s test with Bonferroni correction for post-hoc comparisons when significant. The Mann–Whitney U-test compared non-normally distributed variables between two groups, with median differences and 95% confidence intervals (CIs) estimated using the Hodges-Lehmann method. Categorical data were analyzed using Chi-square or Fisher’s exact test, as appropriate.
Statistical significance was set at p < 0.05 (two-tailed). Apart from the Bonferroni correction in post-hoc tests, no adjustments were made for multiple comparisons across outcomes. All CIs were calculated at the 95% level without adjustment for multiple comparisons. This approach maintains sensitivity to potential effects but may increase the overall Type I error rate given the multiple outcomes analyzed.
Results
Between October 19, 2023, and June 24, 2024, we enrolled 198 of 206 eligible patients. After excluding 7 patients due to procedure cancellations, the final analysis included 64 patients in the dexmedetomidine group, 63 in the esketamine group, and 64 in the combination group (Figure 1). Demographic and procedural characteristics were comparable across groups (Table 1).
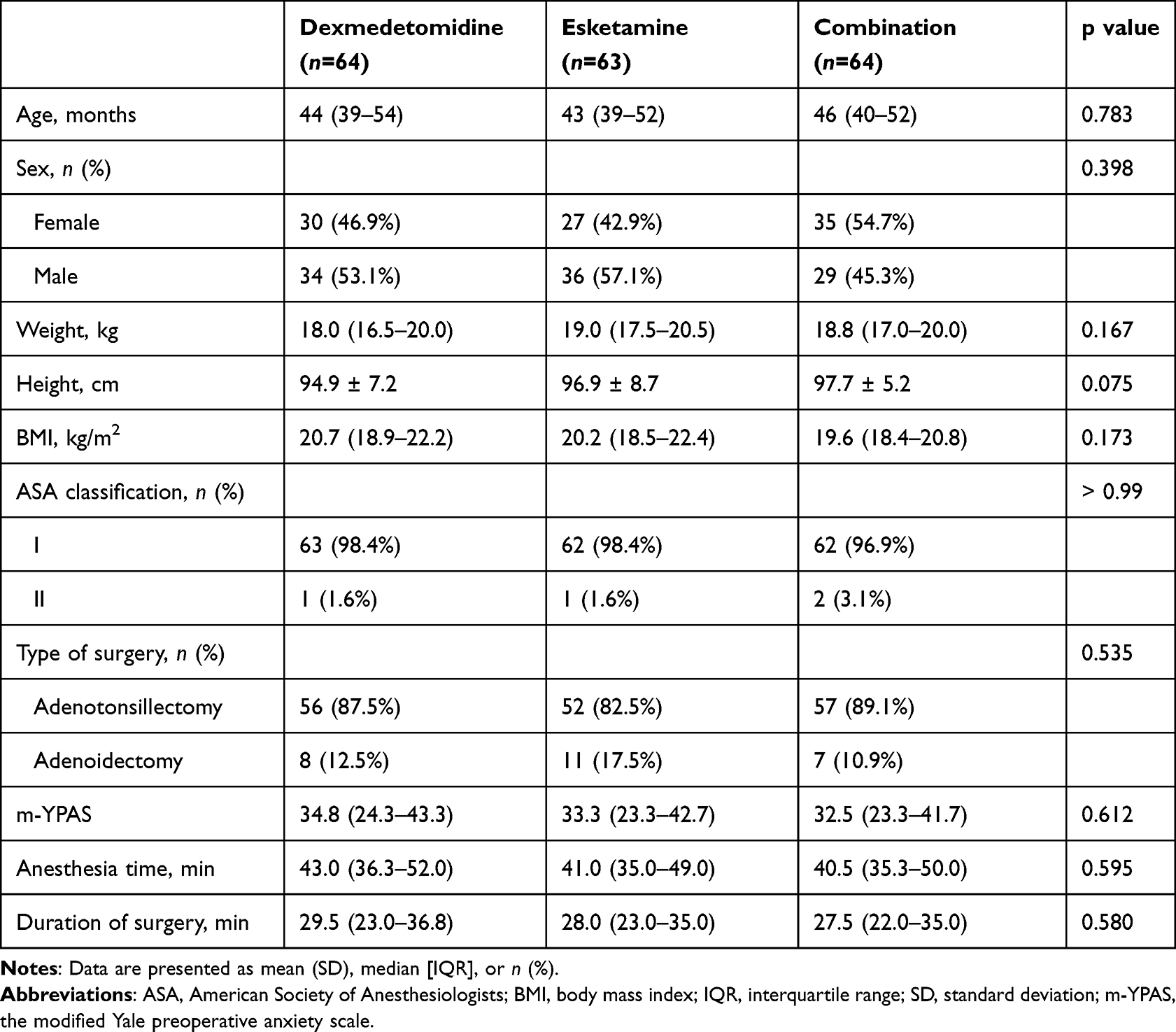 |
Table 1 Baseline Demographic and Clinical Characteristics |
 |
Figure 1 Consolidated Standards of Reporting Trials (CONSORT) flow diagram. |
The combination premedication demonstrated superior efficacy in reducing emergence delirium compared to esketamine alone. Peak PAED scores (median [IQR]) were lower in the combination group (6.0 [4.0–8.0]) compared to dexmedetomidine (7.0 [5.0–8.8]) and esketamine (8.0 [6.0–10.0]) groups (Figure 2A). The combination significantly reduced PAED scores compared to esketamine alone (median difference −2, 95% CI: −3 to −1, p < 0.001), but not dexmedetomidine alone (median difference 0, 95% CI: −1 to 1, p = 0.492). Emergence delirium incidence was lowest in the combination group (9.4%, 6/64), compared to dexmedetomidine (17.2%, 11/64) and esketamine (38.1%, 24/63) groups (Figure 2B). The combination therapy significantly reduced emergence delirium incidence compared to esketamine (RR = 0.25, 95% CI: 0.11–0.57, p < 0.001) but not dexmedetomidine (RR = 0.55, 95% CI: 0.21–1.39, p = 0.193).
 |
Figure 2 Effects of dexmedetomidine, esketamine, and their combination on emergence delirium in pediatric tonsillectomy patients under sevoflurane anesthesia. (A) Raincloud plots of peak Pediatric Anesthesia Emergence Delirium (PAED) scale scores. Box plots show median (horizontal line), interquartile range (box boundaries), and range (whiskers). Scatter plots (left) show individual values; density plots (right) illustrate value distribution. (B) Lollipop plots of emergence delirium (ED) incidence (defined as PAED scale score ≥ 10) across groups. Abbreviations: ED, emergence delirium; PAED, Pediatric Anesthesia Emergence Delirium. |
The incidence of PNBC decreased over time in all groups (Figure 3). On postoperative day 7, the combination group showed a significantly lower PNBC incidence compared to the dexmedetomidine group (28.1% vs 48.4%, RR = 0.58, 95% CI: 0.36–0.93, p = 0.018), but not the esketamine group (28.1% vs 20.6%, RR = 1.38, 95% CI: 0.74–2.58, p = 0.326). The combination also provided significantly deeper sedation, improved ease of separation from parents, better acceptance of the mask for induction, shorter emergence time, and higher parental satisfaction than both monotherapies (Table 2).
 |
Table 2 Secondary Outcomes |
 |
Figure 3 Effects of dexmedetomidine, esketamine, and their combination on emergence delirium and postoperative negative behavioral changes in pediatric tonsillectomy patients under sevoflurane anesthesia. (A) Comparison between combination and dexmedetomidine groups. (B) Comparison between combination and esketamine groups. Abbreviations: CI, confidence interval; POD, postoperative day; RR, relative risk. |
Adverse events were mild and infrequent across all groups. PONV occurred in 4.7%, 7.9%, and 6.3% of patients in the dexmedetomidine, esketamine, and combination groups, respectively. Bradycardia and hypotension were observed only in the dexmedetomidine group, while laryngospasm occurred in one patient in the esketamine group. Nightmare incidence was 21.8%, 25.4%, and 20.3% of patients in the dexmedetomidine, esketamine, and combination groups, respectively. Despite these variations, no statistically significant differences in adverse event frequencies were found among the three groups (all p > 0.05, Table 2).
Discussion
This study assessed the efficacy of intranasal dexmedetomidine-esketamine combination premedication in children aged 2−5 years undergoing tonsillectomy and/or adenoidectomy with sevoflurane anesthesia. Our findings reveal significant advantages of combination therapy over monotherapy. The combined approach more effectively reduced emergence delirium compared to esketamine alone and decreased PNBC at day 7 compared to dexmedetomidine alone. Furthermore, the combination regimen provided superior preoperative sedation, faster emergence from anesthesia, and higher parental satisfaction than either drug administered individually.
Pediatric preoperative sedation and analgesia remain challenging in clinical practice. Intranasal premedication has emerged as a promising, noninvasive method, particularly beneficial for anxious or uncooperative children. This approach utilizes the highly vascular nasal mucosa, allowing rapid drug absorption while bypassing first-pass metabolism.22 Mucosal atomization devices enhance drug delivery by producing a fine mist (30−100 μm), significantly increasing mucosal surface coverage compared to conventional droppers.23
Based on previous research, intranasal dexmedetomidine was administered at 2 μg/kg.24 Its sedative properties primarily stem from α2-adrenoreceptor activation in the locus coeruleus, inducing sleep-like electroencephalogram patterns. Our results confirm dexmedetomidine’s efficacy in reducing emergence delirium, which is consistent with previous studies.25 This effect may be attributed to its lingering pharmacological action. A recent pharmacokinetic study found that intranasal dexmedetomidine 2 μg/kg can achieve mild to moderate sedation lasting up to 2 hours, the targeted therapeutic level.26 However, dexmedetomidine alone showed limitations in addressing PNBC beyond the immediate postoperative period. Aligning with our findings, Lee-Archer et al27 reported no significant difference in PNBC incidence between children receiving 2 μg/kg intranasal dexmedetomidine and those receiving placebo.
Following our established institutional protocol, we administered intranasal esketamine at 1 mg/kg. Esketamine primarily acts as an N-methyl-D-aspartate (NMDA) receptor antagonist. Our findings indicate that esketamine premedication was associated with reduced PNBC on day 7 compared to dexmedetomidine, possibly due to its efficacy in alleviating symptoms akin to post-traumatic stress disorder. Extensive clinical research supports subanesthetic-dose esketamine use in various neuropsychiatric conditions, including depression, anxiety spectrum disorders, and bipolar disorder.28 However, esketamine premedication resulted in higher emergence delirium incidence, prolonged emergence times, and lower parental satisfaction scores compared to both dexmedetomidine and the combination regimen. The increased emergence delirium may be attributed to esketamine’s psychiatric and psychotomimetic side effects, a hypothesis supported by a recent observational study. This study found that esketamine for anesthesia induction was associated with increased emergence delirium in preschool children undergoing minor surgery.29
The combination of dexmedetomidine and esketamine leverages their complementary pharmacological profiles. Consistent with prior research,30,31 this combination yields enhanced sedative effects, smoother anesthesia induction, and faster recovery times without increased adverse events. This synergistic interaction likely arises from the balanced modulation of diverse neurotransmitter systems, potentially mitigating the side effects of higher doses of either agent alone. Specifically, dexmedetomidine counteracts esketamine’s potential for emergence phenomena, while esketamine may compensate for dexmedetomidine’s slower onset of action.
This study has several limitations that warrant consideration. First, ethical considerations precluded the inclusion of a placebo group, making it challenging to attribute observed effects solely to the investigated medications. Second, we did not assess baseline child temperament, which could have influenced premedication response and postoperative behavior, potentially confounding our results. Third, we did not explore the dose-response relationship of the dexmedetomidine-esketamine combination; dosages were based on existing literature and clinical practice, given the limited data on intranasal pharmacokinetics of these agents. Lastly, our single-center design and strict inclusion criteria may limit the broader applicability of our findings to the general pediatric population.
Conclusion
Our study demonstrates that combining intranasal dexmedetomidine and esketamine is a promising premedication strategy for pediatric tonsillectomy and/or adenoidectomy patients. This approach effectively addresses multiple perioperative concerns, potentially improving patient outcomes and parental satisfaction. The synergistic effects of these agents offer advantages over monotherapy in reducing emergence delirium and PNBC. Nevertheless, additional studies are needed to confirm these findings and optimize the premedication protocol.
Data Sharing Statement
The individual deidentified participant data, the study protocol, and the statistical analysis plan can be accessed from the corresponding author upon reasonable request.
Acknowledgments
We extend our sincere gratitude to all the patients and their families for their participation in this study. We also thank the anesthesiologists, surgeons, and nursing staff at Fujian Provincial Hospital for their invaluable support throughout the research process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Program of Haicang District of Xiamen, China (No. 350205Z20232004), Natural Science Foundation of Xiamen, China (No. 3502Z202374068), the Natural Science Foundation of Fujian Province (No. 2022J01407), and the Joint Funds for the Innovation of Science and Technology, Fujian Province (No. 2023Y9275, 2023Y9309). The funders had no role in study design, data collection and analysis, publication decisions, or manuscript preparation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Urits I, Peck J, Giacomazzi S, et al. Emergence delirium in perioperative pediatric care: a review of current evidence and new directions. Adv Ther. 2020;37(5):1897–1909. doi:10.1007/s12325-020-01317-x
2. Aldecoa C, Bettelli G, Bilotta F, et al. European Society of Anesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur J Anaesthesiol. 2017;34(4):192–214. doi:10.1097/EJA.0000000000000594
3. Yang X, Lin C, Chen S, et al. Remimazolam for the prevention of emergence delirium in children following tonsillectomy and adenoidectomy under sevoflurane anesthesia: a randomized controlled study. Drug Des Devel Ther. 2022;16:3413–3420. doi:10.2147/DDDT.S381611
4. Mason KP. Pediatric emergence delirium: a comprehensive review and interpretation of the literature. Br J Anaesth. 2017;118(3):335–343. doi:10.1093/bja/aew477
5. Lee SJ, Sung TY. Emergence agitation: current knowledge and unresolved questions. Korean J Anesthesiol. 2020;73(6):471–485. doi:10.4097/kja.20097
6. Kim J, Byun SH, Kim JW, et al. Behavioral changes after hospital discharge in preschool children experiencing emergence delirium after general anesthesia: a prospective observational study. Paediatr Anaesth. 2021;31(10):1056–1064. doi:10.1111/pan.14259
7. Glumac S, Kardum G, Karanovic N. Postoperative cognitive decline after cardiac surgery: a narrative review of current knowledge in 2019. Med Sci Monit. 2019;25:3262–3270. doi:10.12659/MSM.914435
8. Eijlers R, Dierckx B, Staals LM, et al. Virtual reality exposure before elective day care surgery to reduce anxiety and pain in children: a randomized controlled trial. Eur J Anaesthesiol. 2019;36(10):728–737. doi:10.1097/EJA.0000000000001059
9. Batuman A, Gulec E, Turktan M, et al. Preoperative informational video reduces preoperative anxiety and postoperative negative behavioral changes in children. Minerva Anestesiol. 2016;82(5):534–542.
10. Hebbar KC, Reddy A, Luthra A, et al. Comparison of the efficacy of intranasal atomized dexmedetomidine versus intranasal atomized ketamine as a premedication for sedation and anxiolysis in children undergoing spinal dysraphism surgery: a randomized controlled trial. Eur J Anaesthesiol. 2024;41(4):288–295. doi:10.1097/EJA.0000000000001936
11. Qian B, Zheng W, Shi J, et al. Ketamine enhances intranasal dexmedetomidine-induced sedation in children: a randomized, double-blind trial. Drug Des Devel Ther. 2020;14:3559–3565. doi:10.2147/DDDT.S269765
12. Shen F, Zhang Q, Xu Y, et al. Effect of intranasal dexmedetomidine or midazolam for premedication on the occurrence of respiratory adverse events in children undergoing tonsillectomy and adenoidectomy: a randomized clinical trial. JAMA Netw Open. 2022;5(8):e2225473. doi:10.1001/jamanetworkopen.2022.25473
13. Sottas CE, Anderson BJ. Dexmedetomidine: the new all-in-one drug in pediatric anesthesia? Curr Opin Anaesthesiol. 2017;30(4):441–451. doi:10.1097/ACO.0000000000000488
14. Xing F, Zhang TT, Yang Z, et al. Comparison of dexmedetomidine and a dexmedetomidine-esketamine combination for reducing dental anxiety in preschool children undergoing dental treatment under general anesthesia: a randomized controlled trial. J Affect Disord. 2024;347:569–575. doi:10.1016/j.jad.2023.12.011
15. Juszczak E, Altman DG, Hopewell S, et al. Reporting of multi-arm parallel-group randomized trials: extension of the CONSORT 2010 statement. JAMA. 2019;321(16):1610–1620. doi:10.1001/jama.2019.3087
16. Sikich N, Lerman J. Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale. Anesthesiology. 2004;100(5):1138–1145. doi:10.1097/00000542-200405000-00015
17. Jenkins BN, Kain ZN, Kaplan SH, et al. Revisiting a measure of child postoperative recovery: development of the post hospitalization behavior questionnaire for ambulatory surgery. Paediatr Anaesth. 2015;25(7):738–745. doi:10.1111/pan.12678
18. Jenkins BN, Fortier MA, Kaplan SH, et al. Development of a short version of the modified Yale preoperative anxiety scale. Anesth Analg. 2014;119(3):643–650. doi:10.1213/ANE.0000000000000350
19. Qiu L, Cao L, Lang Z, et al. Preoperative sedation in children with congenital heart disease: 50% and 95% effective doses, hemodynamic effects, and safety of intranasal dexmedetomidine. J Clin Anesth. 2022;81:110908. doi:10.1016/j.jclinane.2022.110908
20. Abdel-Ghaffar HS, Kamal SM, El Sherif FA, et al. Comparison of nebulized dexmedetomidine, ketamine, or midazolam for premedication in preschool children undergoing bone marrow biopsy. Br J Anaesth. 2018;121(2):445–452. doi:10.1016/j.bja.2018.03.039
21. Crellin DJ, Harrison D, Santamaria N, et al. Systematic review of the face, legs, activity, cry and consolability scale for assessing pain in infants and children: is it reliable, valid, and feasible for use? Pain. 2015;156(11):2132–2151. doi:10.1097/j.pain.0000000000000305
22. Miller JW, Balyan R, Dong M, et al. Does intranasal dexmedetomidine provide adequate plasma concentrations for sedation in children: a pharmacokinetic study. Br J Anaesth. 2018;120(5):1056–1065. doi:10.1016/j.bja.2018.01.035
23. Rech MA, Barbas B, Chaney W, et al. When to pick the nose: out-of-hospital and emergency department intranasal administration of medications. Ann Emerg Med. 2017;70(2):203–211. doi:10.1016/j.annemergmed.2017.02.015
24. Yao Y, Sun Y, Lin J, et al. Intranasal dexmedetomidine versus oral midazolam premedication to prevent emergence delirium in children undergoing strabismus surgery: a randomized controlled trial. Eur J Anaesthesiol. 2020;37(12):1143–1149. doi:10.1097/EJA.0000000000001270
25. He H, Cui Q, Chen H, et al. The effect of intranasal dexmedetomidine on emergence delirium prevention in pediatric ambulatory dental rehabilitation under general anesthesia: a randomized clinical trial. Drug Des Devel Ther. 2023;17:3563–3570. doi:10.2147/DDDT.S427291
26. Li BL, Guan YP, Yuen VM, et al. Population pharmacokinetics of intranasal dexmedetomidine in infants and young children. Anesthesiology. 2022;137(2):163–175. doi:10.1097/ALN.0000000000004258
27. Lee-Archer PF, von Ungern-Sternberg BS, Reade M, et al. The effect of dexmedetomidine on postoperative behavior change in children: a randomized controlled trial. Anaesthesia. 2020;75(11):1461–1468. doi:10.1111/anae.15117
28. Johnston JN, Kadriu B, Kraus C, et al. Ketamine in neuropsychiatric disorders: an update. Neuropsychopharmacology. 2024;49(1):23–40. doi:10.1038/s41386-023-01632-1
29. Chen S, Yang JJ, Zhang Y, et al. Risk of esketamine anesthesia on the emergence delirium in preschool children after minor surgery: a prospective observational clinical study. Eur Arch Psychiatry Clin Neurosci. 2024;274(4):767–775. doi:10.1007/s00406-023-01611-z
30. Zanaty OM, El Metainy SA. A comparative evaluation of nebulized dexmedetomidine, nebulized ketamine, and their combination as premedication for outpatient pediatric dental surgery. Anesth Analg. 2015;121(1):167–171. doi:10.1213/ANE.0000000000000728
31. Lu X, Tang L, Lan H, et al. A comparison of intranasal dexmedetomidine, esketamine or a dexmedetomidine-esketamine combination for induction of anesthesia in children: a randomized controlled double-blind trial. Front Pharmacol. 2022;12:808930. doi:10.3389/fphar.2021.808930
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Dexmedetomidine and Two Different Doses of Esketamine Combined Infusion on the Quality of Recovery in Patients Undergoing Modified Radical Mastectomy for Breast Cancer - A Randomised Controlled Study
Huang Z, Liu N, Hu S, Ju X, Xu S, Wang S
Drug Design, Development and Therapy 2023, 17:2613-2621
Published Date: 28 August 2023
Opioid-Free Anesthesia for Pain Relief After Laparoscopic Cholecystectomy: A Prospective Randomized Controlled Trial
Yu JM, Tao QY, He Y, Liu D, Niu JY, Zhang Y
Journal of Pain Research 2023, 16:3625-3632
Published Date: 30 October 2023
Effects of Esketamine Combined with Dexmedetomidine on Early Postoperative Cognitive Function in Elderly Patients Undergoing Lumbar Spinal Surgery: A Double-Blind Randomized Controlled Clinical Trial
Tao QY, Liu D, Wang SJ, Wang X, Ouyang RN, Niu JY, Ning R, Yu JM
Drug Design, Development and Therapy 2024, 18:5461-5472
Published Date: 27 November 2024
The Effects of Opioid-Free Anesthesia with Dexmedetomidine and Esketamine on Postoperative Anesthetic-Related Complications for Hip Surgery in the Elderly
Ye Q, Hu Y, Xing Q, Wu Y, Zhang Y
International Journal of General Medicine 2024, 17:6291-6302
Published Date: 17 December 2024
Comparison Between Low-Dose Esketamine and Dexmedetomidine on Postoperative Recovery Quality Among Patients Undergoing Humeral Trauma Surgery in Interscalene Brachial Plexus Block: A Randomized, Double-Blind, Controlled Trial
Chen J, Qi Y, Zhang J, Sun B, Zhang M, Meng X, Zhou M, Wang L
Drug Design, Development and Therapy 2025, 19:3645-3655
Published Date: 5 May 2025