")
Back to Journals » Advances in Medical Education and Practice » Volume 15
Medical Healthcare Student’s Knowledge, Attitude, and Practices Regarding Hand Hygiene and Its Relation to Patient Safety – A Global Scoping Review
Authors Shyaka MT, Nzisabira J, Mfura H , Tuli S, Glynn LG
Received 9 August 2023
Accepted for publication 18 July 2024
Published 31 October 2024 Volume 2024:15 Pages 1041—1055
DOI https://doi.org/10.2147/AMEP.S283642
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Modeste Tuyisenge Shyaka,1 Joselyne Nzisabira,1 Heritier Mfura,1 Shagun Tuli,2 Liam G Glynn2
1University of Global Health Equity, School of Medicine, Butaro, Rwanda; 2University of Limerick, School of Medicine, Limerick, Ireland
Correspondence: Modeste Tuyisenge Shyaka, Email [email protected]
Introduction: For more than a century, Hand hygiene (HH) has been known to be the most cost-effective hygienic method to minimize infection transmission and risk in healthcare settings. Even though 50% of healthcare-associated infections (HAIs) can be prevented with proper HH, globally 7 per 100 patients from acute-care hospitals in high-income countries (HIC) and 15 per 100 patients in low and middle-income countries (LMIC) acquire at least one HAI during their hospital stay. Even though medical healthcare students do not have the primary responsibility of providing patient care, it is necessary to train, assess, and monitor HH as their interaction with patients could lead to an increased number of HAIs. By conducting this global scoping review, we aim to summarize the global trends surrounding the knowledge, attitude, and practice (KAP) of medical healthcare students regarding HH, and how it affects patient safety.
Methods: We followed the five stages of Arksey and O’Malley’s Scoping Review Methodology. The literature search was done in three databases, specifically, EMBASE, Web of Science, and PubMed. Original published research in credible journals in English conducted between 2012 and 2023 discussing HH amongst medical healthcare students all over the world were included.
Results: Twenty-three studies were included in the final analysis. The overall knowledge of medical students regarding HH was low, with some studies reporting scores as low as 10.1%. However, the attitude towards HH was generally positive, with mean scores ranging from 55% to 93%. Notably, nursing students and females exhibited better attitudes and self-reported HH practices. Furthermore, studies indicated that providing training on HH resulted in an increase in positive attitudes towards and improved practices of HH.
Conclusion: By focusing on training and facilitating improved HH practices, future generations of doctors and nurses can contribute to minimizing HAIs and enhancing patient safety. Standardized approaches and comprehensive data collection are crucial for implementing effective HH interventions.
Keywords: hand sanitizing, hand washing, undergraduate medical students, healthcare students, patient care
Introduction
For more than a century, hand hygiene (HH) has been known to be the most cost-effective hygienic method to minimize infection transmission and risk in healthcare setting.1 HH is a sanitary, hand cleansing action performed by hand-rubbing and/ or washing using an alcohol-based formulation such alcohol-based sanitizers and antiseptic wipes or detergents such as soap and water or is used as a general term to define any hand cleansing action including alcohol-based hand rub, antimicrobial soap, antiseptic agents, and antiseptic hand wipes.2 However, washing hands with soap and water is proven to be the best way to cleanse the hands.3 Even though 50% of hospital associated infections (HAIs) can be prevented with proper HH in acute-care hospitals 7 per 100 patients in high-income countries (HIC) and 15 per 100 patients in low and middle-income countries (LMIC), acquire at least one HAI during their stay.4,5
In 2009, the World Health Organization (WHO) introduced the “Five Moments of HH” with the aim of reducing HAIs by reiterating the best practices in HH and reminding healthcare providers to clean their hands when it mattered the most.6 Despite not being involved in healthcare decision-making, medical students play an integral part in patient safety owing to their interaction with patients during clinical clerkships.7 Prior to the previous decade, most studies that evaluated the HH of medical students were based on self-reported data and questionnaires but did not evaluate the Five Moments of HH by WHO, until 2012 where it was studied by Al Kadi and Salati8 for the first time.9 This generated further research in the area, where different methodologies have been used to evaluate HH practices in medical students.9
Though medical students are provided with theoretical classes and materials about HH, studies have highlighted low knowledge and practice levels of HH among this group.10 Other factors that attributed to this low adherence included limited access to HH materials, low adherence among their senior mentors, and heavy workload.11 Such improper hygiene practices amongst medical students have led to poor patient outcomes and are not a new occurrence. A study done as early as 1846 found a higher number of maternal deaths in maternity units where medical students were placed for their clerkships as compared to those run only by midwives. The study investigated, identified, and reported the risk factors and patients’ symptoms suggesting infectious disease processes underlying this finding, possibly because the medical students often visited the maternity ward directly after attending autopsies and were transmitting infectious pathogens due to poor HH practices.1 Even though medical students do not have the primary responsibility of providing patient care, it is necessary to train, assess, and monitor HH practices as their interaction with patients could lead to an increased number of HAIs.7
Since the COVID-19 pandemic, multiple studies have highlighted the importance of HH, not just as a best practice for healthcare providers including medical studies, but as a public health priority.12,13 An increased awareness regarding HH has been noticed among medical students and other healthcare providers, which can be attributed to the global campaigns about HH to minimize the transmission of COVID-19 and efforts invested by national healthcare systems in establishing more hand washing stations, with the provision of HH materials.13
With multiple approaches to incorporating HH in medical curricula, it is necessary to establish the knowledge levels, current attitudes, and practices across the globe.11 Studies have discussed targeted improvement programs prior to commencing clinical clerkship and patient interaction to improve HH. One of the most recommended initiatives is providing HH training sessions to students at the beginning of clinical clerkships.14 While such initiatives have the potential to improve HH hence decreasing HAIs, they require regular monitoring and evaluation and must be consistently provided to ensure sustainable outcomes.14 By conducting this scoping review, we aim to gain a cross-sectional picture of the current global knowledge, attitude, and practices of medical students regarding HH while summarizing targeted interventions and their effectiveness geared at improving HH and reducing HAIs attributed to this cohort.
Methodology
Study Design
A scoping review was chosen to perform this study as it assesses the scope, extent, and reach of the available literature allowing us to identify key themes around this research topic. This scoping review followed the five stages of Arksey and O’Malley’s Scoping Review Methodology, namely 1) identifying the research question, 2) identifying relevant studies, 3) selecting studies, 4) charting the data, and 5) summarizing and reporting the data.15
Step 1: Identifying the Research Question
Following the first step of the Arksey O’Malley’s methodology, a research question was developed.15 The research question aims at answering the following questions:
- What is the overall KAP in HH for medical healthcare students?
- What (if any) are the interventions used to increase or assess KAP in HH for medical healthcare students and improve patient safety and what is their effectiveness?
To answer the first and second questions, data including author details, year of publication, country location, research method, study design, participants cohort, sample size, and key results in KAP were summarized. Details regarding types of interventions, their evaluation (if any), and outcomes pertaining to patient safety (if any) were discussed to answer questions 2 and 3.
Step 2: Identifying Relevant Studies
In this step, a set of inclusion and exclusion criteria was employed to focus the scope of the review and extract studies from selected databases. Original published research published in credible journals (in English language) in the past decade (2012–2023) that discussed hand hygiene practices amongst medical healthcare students all over the global were included. Studies in which participants other than medical students were recruited were excluded except when they were compared to medical students. Such participant cohorts include first- and second-year medical students, medical residents, trainees, nursing students, allied health students, and professional healthcare workers.
The team followed an iterative search strategy, whereby more articles were extracted with an expanding search vocabulary. The data search was carried out by four reviewers (JN, ST, SM, HM). The articles were obtained using three bibliographic databases (PubMed, EMBASE, and Web of Science). The team defined key search terms before the extraction to guide narrowing the search results; 1) knowledge/attitude/beliefs/practices 2) hand hygiene/hand sanitizing/hand washing/alcohol-based hand rub/hand rubbing 3) Medical students /undergraduate medical students 4) Patient safety/patient care. MeSH terms included were Attitudes of Health Personnel, HH, Health Knowledge Attitudes and Practice, and Students, Medicine. The search was implemented as: ((knowledge/attitude/beliefs/practices [Title/Abstract]) AND (hand hygiene/hand sanitizing/hand washing/alcohol-based hand rub/hand rubbing [Title/Abstract]) AND (Medical students /undergraduate medical students [Title/Abstract]) AND (Patient safety/patient care [Title/Abstract]). Our search was limited to studies on a population of medical students in English, and supplemented by a manual search for reference lists of identified papers. The PROSPERO database was evaluated using the steps described above (title/abstract section edited) to confirm that there were no systematic reviews or scoping studies on recent or ongoing work that has been completed on the topic. The database search was conducted from November 22, 2022, to June 19, 2023.
Step 3: Selection of Research Results
The studies were imported onto Rayyan software for screening and duplicates were deleted (Figure 1). The abstract screening was conducted by three reviewers (STM, HM, JN), who were blinded by each other’s decisions. Conflicts were resolved by a fourth author (ST). Full-text reviews were conducted by three independent reviewers, and the majority vote was considered for the final decision. Full-text articles included in the list were also evaluated independently for eligibility (Figure 1).
 |
Figure 1 PRISMA Flow diagram of the literature selection procedure. Notes: Adapted from: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–341. doi: 10.1016/j.ijsu.2010.02.007.16 Copyright © 2010 The Authors. Copyright © 2010 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved. Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/legalcode). |
To facilitate calibration, the authors met five times during the process, with the first meeting focused on creating a shared understanding of the inclusion and exclusion criteria. The next meetings compared selected studies and discussed differences in understanding. Throughout this process, one author (ST) monitored each meeting to ensure and verify the accuracy of the work and contributed to the analysis of the results.
Step 4: Data Mapping Process
The data extraction and recording process followed the Arksey and O’Malley’s “descriptive-analytical” approach for data extraction (1), and the information was summarized from selected articles on an Excel spreadsheet. Author ST developed a data extraction form and STM, HM, and JN performed the data extraction. Data extracted was thoroughly reviewed by all authors, and disagreements were resolved by consensus among the group. The information extracted was recorded as follows:
- Author(s)
- Year of publication
- Study location
- Study populations
- Sample size
- Study Design
- Aims of the study
- Methodology
- Important results
- Intervention type, and comparator (if any)
Step 5: Collating, Summarizing Findings, and Reporting the Results
Descriptive statistics were used to describe the review’s characteristics of the data and attention was given to basic numerical analysis of the extent, nature and distribution of the studies included in the review. The authors shared the activity of summarizing the findings and reporting the results by coding the activity to identify the relevance of the article to the research question. Emergent themes were coded separately and discussed between the authors to generate the results.
Results
Overview (Table 1)
The process of identifying relevant articles and abstract screening was rigorous; out of 806 abstracts screened, 751 were excluded. Twenty-three studies were included as part of the final analysis based on the inclusion and exclusion criteria. Most of the studies were conducted in South & East-Asian countries (n = 15) of which 7 were from India. The remaining studies were from Europe (n = 6), Africa (n = 1), and the USA (n = 1). Of these, 13 fall under low-middle-income countries (LMICs), and 10 are high-income countries (HICs). Most studies were published prior to 2019, and COVID (n = 17) and 6 were published since 2019.
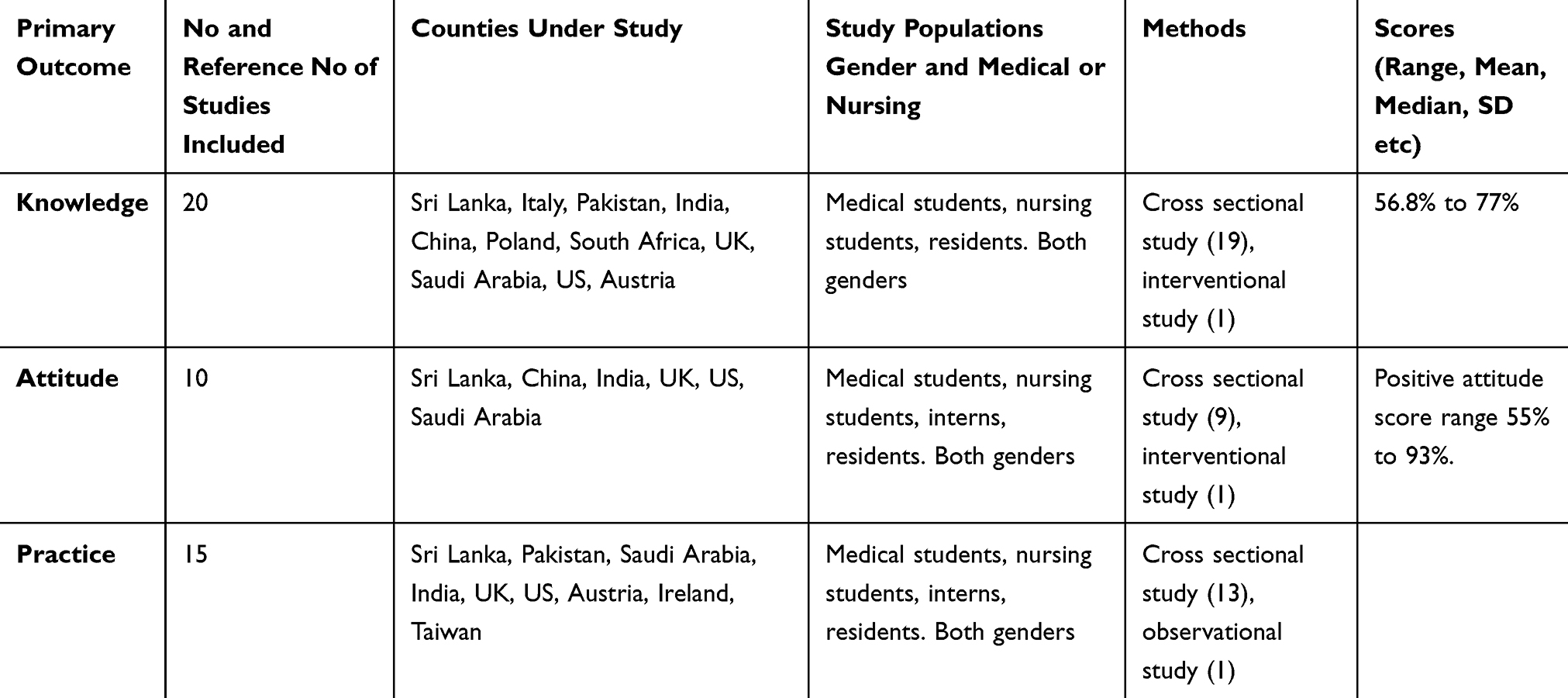 |
Table 1 Primary Outcome: Knowledge, Attitude, and Practice |
All studies were cross-sectional and all barring 1 were quantitative (n = 1 qualitative). Two studies were observational, 2 were comparative (one comparing medical and nursing students, one comparing male and female medical students), and one was an interventional study evaluating the knowledge pre and post-training for HH and the other measured the hand bacterial contamination in medical and nursing students to verify the HH adherence. All studies included medical students as their participant cohort (n = 13 included only medical students, n = 7 included medical and nursing students, n = 4 included medical students, residents, and other groups).
Almost all studies used a self-administered questionnaire as a study tool (n = 18) of which 2 studies adapted theirs from the WHO hand hygiene knowledge questionnaire for healthcare workers. One study used this WHO hand hygiene knowledge questionnaire for healthcare workers tool itself, whereas one used a validated scoring sheet to assess the quality of HH amongst medical students. The qualitative study conducted narrative interviews using a semi-structured interview guide. All studies were conducted with the aim of evaluating either the knowledge, attitude, or practice of medical students regarding hand hygiene or a combination of the above (n = 23).
Knowledge Regarding Hand Hygiene (Table 2)
Almost all studies evaluated the knowledge regarding HH (n = 20). Most studies reported an overall low score regarding the knowledge of HH with scores as low as 10.1%; the individual scores % were reported on administered questionnaires. The studies’ participants’ mean scores reported regarding their knowledge about hand hygiene ranged from 56.8% to 77%.2,17 A total of five studies reported that nursing students had a higher level of knowledge compared to medical students regarding HH.2,3,18–20 Two studies also found that female medical students had better knowledge as compared to male students (Jayarajah et al, 2019; Azzam & Ahmad, 2012) while two other studies concluded that there was no significant difference between male and female medical students’ knowledge regarding hand hygiene.14,21,22 However, there was no study that demonstrated a higher level of knowledge among male medical students compared to female medical students.
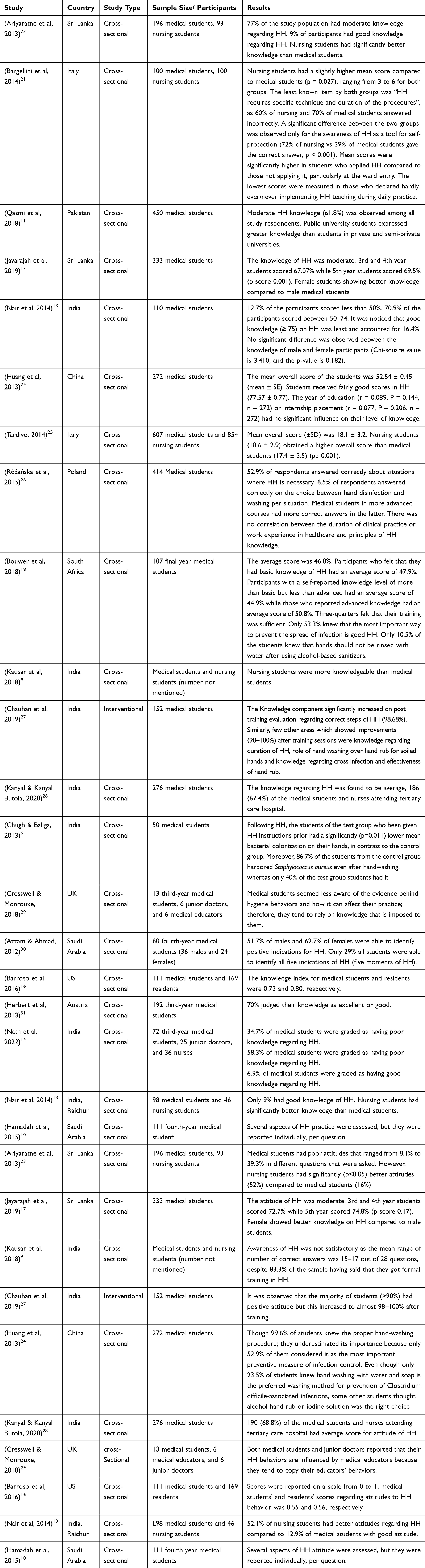 |
Table 2 Summary of the Articles That Discusses Knowledge Regarding Hand Hygiene of Medical Healthcare Students |
Attitude Regarding Hand Hygiene (Table 3)
A total of 10 studies collected data on the attitude regarding HH as compared to knowledge. Most of these reported a positive attitude towards HH with mean scores ranging from 55% to 93%. Ariyaratne et al (2013) and Nair et al (2014) found that nursing students have a better attitude towards hand hygiene; Kanyal & Butola (2020) did not find any significant difference between nursing and medical students regarding their attitude towards hand hygiene.2,19 On the other hand, the positive attitude regarding hand hygiene increased after providing training regarding the topic.7
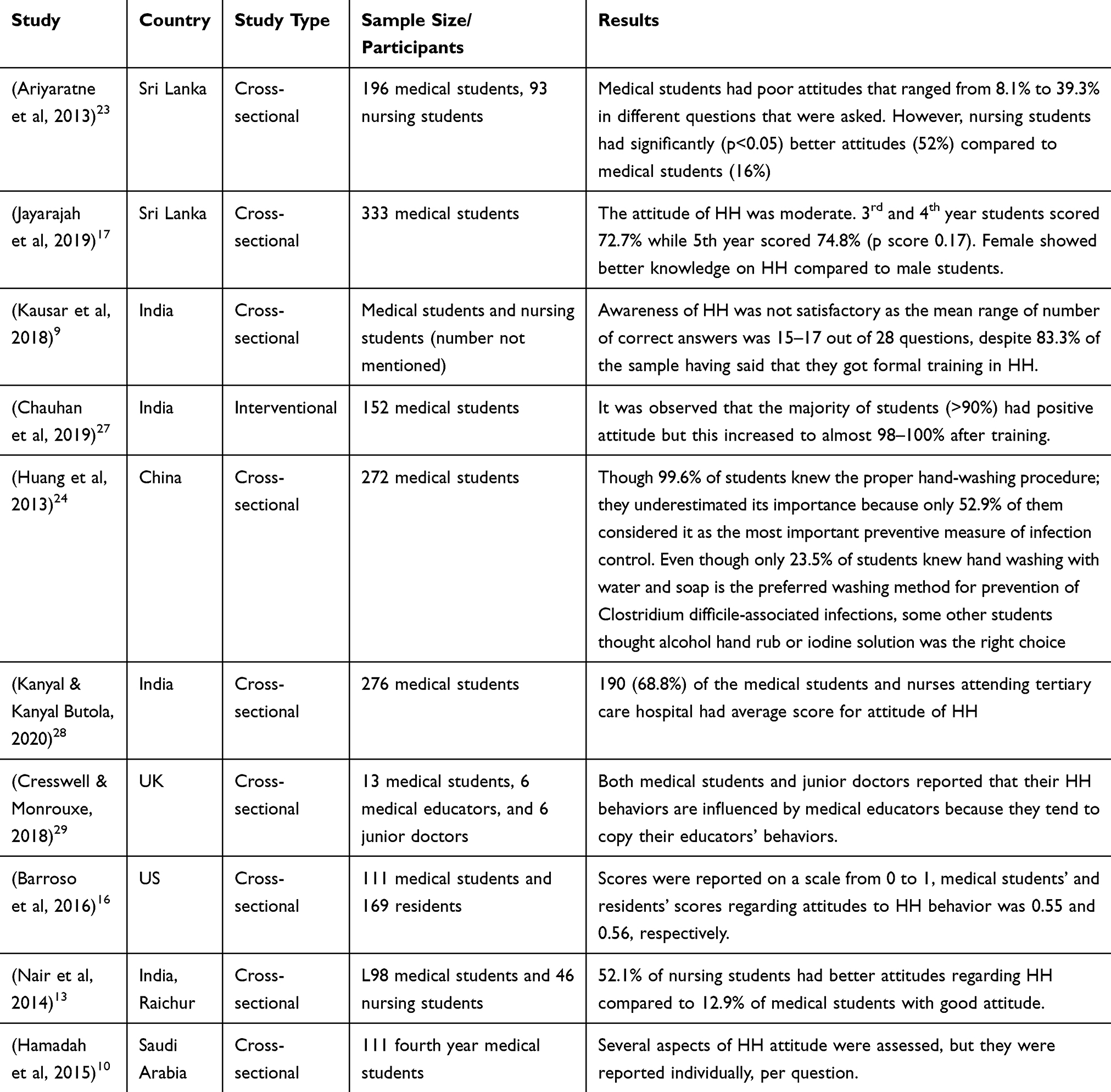 |
Table 3 Summary of the Articles Discussing Attitudes of Medical Healthcare Students Towards Hand Hygiene |
Practices Regarding Hand Hygiene (Table 4)
Similarly, a total of 15 studies reported individual data regarding the practice of HH. Ariyaratne et al (2013), Nair et al (2014), and Kingston et al (2018) found that nursing students have significantly better practices regarding hand hygiene compared to medical students.2,18,29 A study by Kausar et al (2018), on the other hand, did not find any significant difference between nursing and medical students’ practices regarding hand hygiene; their practices regarding hand hygiene were comparably poor.16 According to gender, Jayarajah et al (2019) found that female students have better practice regarding hand hygiene compared to their male counterparts while Azzam & Ahmad (2012) did not find any significant difference between male and female students’ practices regarding hand hygiene (16.7% and 17.7%, respectively).21,23 One study by Barry et al (2021) reported a combined KAP score where senior medical students (5th year) were found to have higher scores (73%) compared to junior medical students (4th and 3rd year, 72% and 67%, respectively).32
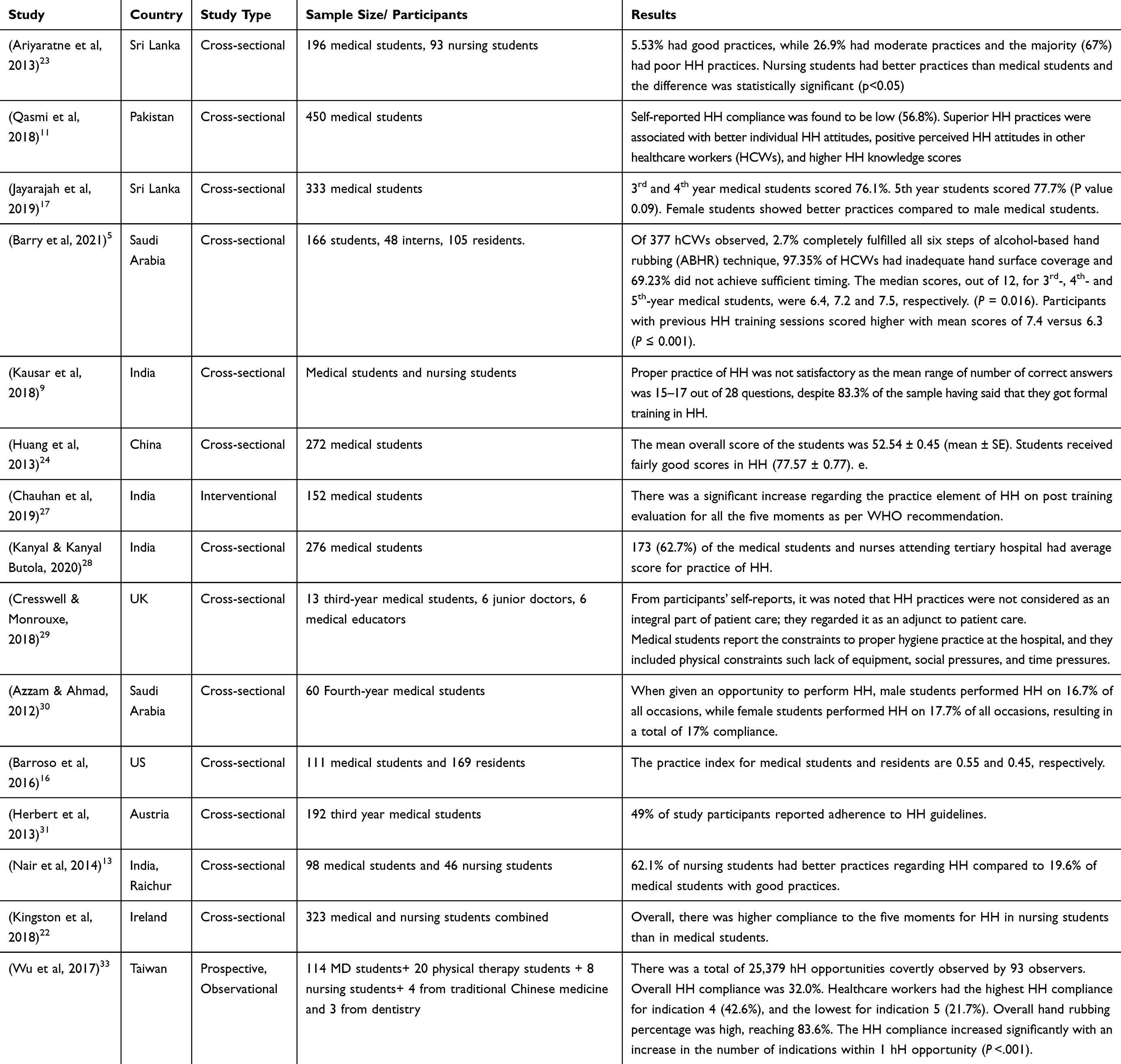 |
Table 4 Summary of the Articles Discussing Hand Hygiene Practices Among Medical Healthcare Students and Their Findings |
Perceptions Around Hand Hygiene
Some studies also inquired about the perceptions surrounding HH and positive factors that could improve the practice amongst medical students (n = 5). When asked about their perceived level of knowledge regarding HH, most students believed they had good knowledge or that their training was sufficient (mean range 90.6% to 50.3%). The 2 most common factors associated with better HH were the availability of working gel sanitizer dispensers (n = 3), and better HH practices modeled by their superiors (n = 4).
Interventions Supporting Improved HH and Patient Safety
One study compared medical students’ knowledge, attitude, and practices regarding hand hygiene before and after an intervention. The intervention was to train medical students on hand hygiene using lectures and demonstration scenes followed by hands-on training. There was a significant improvement in students’ knowledge regarding hand hygiene where students scored more than 98% on different questions asked in the post-interventional questions.6 Regarding the evaluation of attitude towards hand hygiene, the majority of students (>90%) had positive attitude, which increased to 98–100% after training. There was also significant increase regarding the practice element of hand hygiene on post-training evaluation for all the five moments as per WHO recommendation.
Discussion
Main Findings
Our results highlight that despite evidence that HH significantly improves patient outcomes, knowledge, attitude, and practices towards HH amongst medical healthcare students remain low; therefore, we need to train and enable. Most studies are cross-sectional using self-administered questionnaires. Few interventions have been employed to improve these practices. Nursing students seem to have better outcomes with regard to HH than medical students. The same is found for female medical students. Lastly, there is a dearth of qualitative evidence that explains the reasons and barriers to HH among this cohort.
Comparison with Existing Literature
The WHO questionnaire is the most standard tool; however, only a few studies have used the tool, making comparison more challenging. Most studies have employed a self-administered questionnaire and the data collected has not been extrapolated to patient safety outcomes. Rather than developing another standardized evaluation method, researchers can be urged to use the WHO tool. Outcome measures can also be expanded to include patient safety outcomes so that the direct impact HH practices have on patient care could be quantified.
Nursing students have been found to have better HH knowledge, attitudes, and practices by some studies. The same is observed to be true for senior nurses and providers.2–5 Studies have found nurses to be intrinsically motivated and adherent to HH practices, whereas one study reports that physicians may be “defiant” to HH or forgetful in other contexts.2–5 Our review also indicates that female students may have better HH practices than males. This finding is consistent with other epidemiological and gender-based studies that analyze HH practices for senior physicians, nurses, and other healthcare providers.6,7,9 Overall, this indicates that individual characteristics could play a role in HH and HAIs and warrants comparative exploration between these cohorts.
Knowledge
Given the burden of transmittable diseases, HH remains one of the most important aspects of prevention among healthcare providers. Unfortunately, the majority of the studies we evaluated in our study highlighted low to moderate knowledge, on such a vital component. This resonates with findings from Zakeri H et al, which revealed more than 60% of healthcare workers had moderate HH knowledge with only 10.6% having good knowledge.34 This consistency in results underlines the persistent knowledge gap that exists within the healthcare community regarding HH. However, it is essential to acknowledge that different studies we evaluated had different methods of evaluating and defining good knowledge ranging from a score of more than 75% being considered to be good to analysis of different factors positively associated with self-reported good knowledge in qualitative studies. Receiving HH training was reported to be among the factors that contributed to high knowledge. This differs from other studies that found no statistical differences in knowledge between participants who received prior HH knowledge and those who did not.34,35
Attitude
The students’ attitude regarding HH was defined as their behavioral and intellectual tendencies towards HH practices at the hospital. Overall, the studies have shown that medical students have an overall poor attitude towards HH than their nursing students’ counterparts (Nair et al, 2014). Ariyarathne et al (2013) tested healthcare students on several topics relevant to HH and found that medical students had poor attitudes that ranged from 8.1% to 39.3%, which is lower than the nurse students’ scores. However, Chauhan et al (2019)27 and Hamadah et al (2015) had a different finding; the majority of the students (90%) had a positive attitude towards HH. Moreover, their attitude improved after a training program on HH, demonstrating the role of education and training on HH and, therefore, patients’ safety. The year of study also affected the overall attitudes of medical students; the more advanced a student was in their medical training, the better the attitude. For instance, fourth-year medical students had a better attitude toward HH than their junior colleagues in the third year. Therefore, training, program, and year of study were good predictors of attitude towards HH. Other predictors include students’ experience at the hospital (Barroso et al, 2016). Having a “role model” or attending physicians who regularly practice HH at the hospital had a positive influence on medical students and other healthcare students such as nurses (Cresswell & Monrouxe, 2018). Hamadah et al (2015) study also elaborates on the influence of good living examples on students’ attitudes towards HH. Moreover, learning in an environment conducive of the practice of HH positively influences the students’ attitude towards HH. Such an environment contains gel dispensers, role models, and other reminders of HH. Interestingly, knowledge regarding HH is not a good predictor of students’ attitudes toward HH. For instance, residents and medical students had comparable attitudes towards HH even though their level of knowledge and compliance were different. This underpins the effectiveness of hands-on practices as a method of training healthcare workers. Unfortunately, though a good example instills a good attitude toward HH, the student’s attitude toward hierarchy has a significant negative impact on HH advocacy (Barroso et al, 2016). Therefore, healthcare workers should be aware of their students’ perception of the difference in the hierarchy and how it affects incidence reports, advocacy, and interaction at the hospital. Finally, Cresswell & Monrouxe (2018) found that medical students did not consider HH to be integral to patient care and were less prioritized. It demonstrates gaps in their understanding regarding the relevance and need for HH in patients. Moreover, it calls for a conscious shift in attitude because some students perceive HH as added unnecessary work or omit it due to unseen direct benefits of HH.
Practices
Similarly, to the knowledge and attitude of healthcare students towards HH, their practices trends towards average. In most studies, the HH practices among healthcare students were interpreted as a percentage of the moments of HH where healthcare students practiced HH. In other words, this is the compliance rate of healthcare students. For instance, Ariyaratne et al (2013)23 found that, among 259 medical and nursing students, only 5.53% had good HH practices. These findings resonate with the studies by Barry et al (2012), Kanyal and Butola (2020), Azzam and Ahmad (2012), Herbert et al (2013),31 and Wu et al (2017),33 who found that there was an overall unsatisfactory HH practices among healthcare students. Fortunately, some studies highlighted factors that reinforce positive HH practices, and they included role models, attitude towards HH, and prior HH training. Though Qasmi et al (2018) study results highlight an underlying gap in HH practices among healthcare students, they draw an association between good HH practices with students who have a positive attitude towards HH and those who have witnessed positive HH practices in other health workers. This association reinforces the importance of a positive environment in mediating the compliance of HH. On the other hand, a negative environment or negative social pressures were reported as a constraint to proper HH practices among healthcare students (Cresswell & Monrouxe, 2018). Lack of equipment and time pressures were also reported as major constraints to proper HH practices. Other factors that were reported to affect HH compliance include gender, year of study, academic program, and prior HH training. Better HH practices were reported among nursing students compared to medical students, and the difference was statistically significant (Nair et al, 2014). Unfortunately, despite better HH practices among female students, the overall HH practices among students remain inadequate (Azzam & Ahmad, 2012). Additionally, Chauhan et al (2019)27 reported better HH practices among healthcare students after the training. This reinforces the importance of training programs in potentially improving HH practices in healthcare settings. Finally, a positive attitude towards HH was reported among factors that favor good HH practices (Qasmi et al, 2018).11 This partly explains the findings by Cresswell and Monrouxe (2018) who found that students did not consider HH practices as an integral component of patient care. A shift in perspective would shift healthcare students’ attitudes toward HH practices during patient care.
Strengths and Limitations
Qualitative evidence could help guide such research in understanding the motivations, barriers, and challenges certain groups may face in a hospital setting. Some studies have reported recommendations offered by the participant groups. These include having working alcohol-based dispensers and observing good HH practices among senior healthcare providers. Similar findings have been reported by other studies that emphasize the importance of having good role models to improve adherence to HH amongst medical students.10–13 With an overall lower rate of knowledge and dearth of interventions geared at improving HH amongst medical students, such evidence could help guide the creation of future programs and policies that are inclusive of the unique challenges this cohort faces.
This was a comprehensive scoping review collecting global data on this important topic. Most of the studies included in this review are quantitative, have a large sample size, and measure similar outcomes. With representation from most continents, the review produces a global picture of the recent HH knowledge, attitude, and practices amongst medical healthcare students. Lack of standardized definitions for terminology such as “attitudes”, and “practices” make comparisons between studies challenging and is a limitation of the study. Standardized tools such as the WHO questionnaire, while available, have not been incorporated by most studies. Further given the scope of this paper, quality assessment of the individual studies has not been included. A lack of interventional and prospective studies also limits this review’s ability to generate conclusive recommendations for improving HH practices.
Conclusion
This review has demonstrated that knowledge and practices of hand hygiene among healthcare students are low, but attitudes towards hand hygiene are largely positive which presents an opportunity to train and facilitate high-quality hand hygiene practices among future generations and doctors and nurses. While much research has been done around this topic, a focused collection of evidence using standardized tools to implement best practices amongst medical healthcare students is essential to improve HH outcomes globally.
Disclosure
The authors report no conflicts of interest in this work.
References
1. The Global Handwashing Partnership. History; 2015. Available from: https://globalhandwashing.org/about-handwashing/history-of-handwashing/.
2. World Health Organization. Definition of terms; 2009. Available from: https://www.ncbi.nlm.nih.gov/books/NBK144046/.
3. CDC. When and how to wash your hands Handwashing; 2023. Available from: https://www.cdc.gov/handwashing/when-how-handwashing.html.
4. World Health Organization. WHO launches first-ever global report on infection prevention and control; 2023. Available from: https://www.who.int/news/item/06-05-2022-who-launches-first-ever-global-report-on-infection-prevention-and-control.
5. Barry M, Alotaibi R, Alotaibi F, Alotaibi L. Qualitative observational assessment of the recommended hand rubbing technique amongst young healthcare workers at an academic hospital. J Pat Safe Infect Cont. 2021;9(1):8. doi:10.4103/jpsic.jpsic_1_21
6. Chugh Y, Baliga S. Semmelweis’s forgotten gift: has handwashing lost its importance? J Clin Diagn Res. 2013;7(3):434–436. doi:10.7860/JCDR/2013/4779.2792
7. Affairs AC. Medical student involvement in patient care: report of the council on ethical and judicial affairs. AMA J Ethic. 2001;3(3):71–75.
8. Al Kadi A, Salati SA. Hand hygiene practices among medical students. Interdiscipl Perspect Infect Dis. 2012;2012:e679129. doi:10.1155/2012/679129
9. Kausar H, Kamath R, D’souza B, Kamath S, Kamath R. Self-perceived hand hygiene among student health professionals in a tertiary care teaching hospital in southern India. Indian J Public Health Res Dev. 2018;9(10):116–120. doi:10.5958/0976-5506.2018.01324.4
10. Hamadah R, Kharraz R, Alshanqity A, et al. Hand hygiene: knowledge and attitudes of fourth-year clerkship medical students at Alfaisal University, College of Medicine, Riyadh, Saudi Arabia. Cureus. 2015;7(8). doi:10.7759/cureus.310
11. Qasmi SA, Mahmood Shah SM, Wakil HYI, Pirzada S. Guiding hand hygiene interventions among future healthcare workers: implications of knowledge, attitudes, and social influences. Am J Infect Control. 2018;46(9):1026–1031. doi:10.1016/j.ajic.2018.02.019
12. Mwesigye P, Sekhon B, Punni A, et al. Knowledge, attitudes, and self-reported practices (Kap) towards hand hygiene in medical students versus the public. Ir J Med Sci. 2022;191(6):2797–2802. doi:10.1007/s11845-022-02918-x
13. Nair SS, Hanumantappa R, Hiremath SG, Siraj MA, Knowledge RP. attitude, and practice of hand hygiene among medical and nursing students at a tertiary health care centre in Raichur, India. ISRN Prev Med. 2014;2014:608927. doi:10.1155/2014/608927
14. Nath S, Kumar N, Kumar R. Comparative study on knowledge of hand hygiene among medical students, resident doctors, and nurses at tertiary health institution of Uttar Pradesh. Asian J Pharm Clin Res. 2022;162–166. doi:10.22159/ajpcr.2022.v15i9.45097
15. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
16. Barroso V, Caceres W, Loftus P, Evans KH, Shieh L. Hand hygiene of medical students and resident physicians: predictors of attitudes and behavior. Postgrad Med J. 2016;92(1091):497–500. doi:10.1136/postgradmedj-2015-133509
17. Jayarajah U, Athapathu AS, Jayawardane BA, Prasanth S, Seneviratne SN. Hygiene practices during clinical training: knowledge, attitudes and practice among a cohort of South Asian Medical students. BMC Med Educ. 2019;19(1):157. doi:10.1186/s12909-019-1582-2
18. Bouwer M, Labuschagne S, Spamer S, et al. Knowledge of final-year medical students at the University of the Free State of hand hygiene as a basic infection control measure. S Afr Family Pract. 2018;60(3):74–78. doi:10.1080/20786190.2017.1396789
19. Feather A, Stone SP, Wessier A, Boursicot KA, Pratt C. “Now please wash your hands”: the handwashing behavior of final MBBS candidates. J Hosp Infect. 2000;45(1):62–64. doi:10.1053/jhin.1999.0705
20. Liyanage G, Dewasurendra M, Athapathu A, Magodarathne L. Hand hygiene behavior among Sri Lankan medical students during COVID-19 pandemic. BMC Med Educ. 2021;21(1):333. doi:10.1186/s12909-021-02783-9
21. Bargellini A, Ferranti G, Santangelo M, Venturelli F, Borella P, Marchesi I. Hand hygiene knowledge, hand contamination and practice of Italian nursing and medical students; 2014. Available from: https://www.semanticscholar.org/paper/Hand-Hygiene-Knowledge%2C-Hand-Contamination-and-of-Bargellini-Ferranti/2ff34484b304fd2c23443f7a2b4bc05d7866164f.
22. Kingston LM, O’Connell NH, Dunne CP. A comparative study of hand hygiene and alcohol-based hand rub use among Irish nursing and medical students. Nurse Education Today. 2018;63:112–118. doi:10.1016/j.nedt.2018.01.022
23. Ariyarathne M, Gunasekara T, Weerasekara MM, Kottahachchi J, Kudavidanage BP, Fernando SSN. Knowledge, attitudes and practices of hand hygiene among final year medical and nursing students at the University of Sri Jayewardenepura. Srilankan Journal of Infectious Disease. 2013;3(1):15.
24. Huang Y, Xie W, Zeng J, Law F, Ba-Thein W. Limited knowledge and practice of Chinese medical students regarding healthcare-associated infections. J Infect Dev Ctries. 2013;7(2):144–151. doi:10.3855/jidc.3099
25. Tardivo S. Prevention of healthcare-associated infections: medical and nursing students’ knowledge in Italy; 2014. Available from: https://www.academia.edu/17567136/Prevention_of_healthcare_associated_infections_Medical_and_nursing_students_knowledge_in_Italy.
26. Różańska A, Wójkowska-Mach J, Bulanda M. Medical students’ knowledge of the very basic principles of hand hygiene. Antimicrob Resist Infect Control. 2015;4(1):P286. doi:10.1186/2047-2994-4-S1-P286
27. Chauhan K, Pandey A, Thakuria B. Hand hygiene: an educational intervention targeting grassroots level. J Infect Public Health. 2019;12(3):419–423. doi:10.1016/j.jiph.2018.12.014
28. Kanyal D, Kanyal Butola L. Knowledge, Attitude and Practice regarding hand hygiene among Medical Students and Nurses - A questionnaire based survey in tertiary care hospital. International Journal of Research in Pharmaceutical Sciences. 2020;11:4(SPL)), 2726–2734. Retrieved from https://ijrps.com/home/article/view/2680.
29. Cresswell P, Monrouxe LV. ‘And you’ll suddenly realize ”I’ve not washed my hands”: medical students’, junior doctors’, and medical educators’ narratives of hygiene behaviors. BMJ Open. 2018;8(3):e018156. doi:10.1136/bmjopen-2017-018156
30. Al-Dorzi HM, Matroud A, Al-Khateeb M, et al. Hand hygiene practices and barriers in the adult intensive care unit of a tertiary care center. In: A39. Improving quality in the intensive care unit. American Thoracic Society. In: Am J Infect Control. 2012;45(3):A1451–A1451. doi:10.1164/ajrccm-conference.2012.185.1_MeetingAbstracts.A1451
31. Herbert VG, Schlumm P, Kessler HH, Frings A. Knowledge of and adherence to hygiene guidelines among medical students in Austria. Interdiscipl Perspect Infect Dis. 2013;2013:e802930. doi:10.1155/2013/802930
32. Moinuddin SK; Thirumaran, Karthikeyan. Assessment of knowledge on hand hygiene among final year medical undergraduates. Internat J Res Pharmac Sci. 2020;11(4):5584. doi:10.26452/ijrps.v11i4.3195
33. Wu KS, Chen YS, Lin HS, et al. A nationwide covert observation study using a novel method for hand hygiene compliance in health care. Am J Infect Control. 2017;45(3):240–244. doi:10.1016/j.ajic.2016.10.010
34. Zakeri H, Ahmadi F, Rafeemanesh E, Saleh LA. The knowledge of hand hygiene among the healthcare workers of two teaching hospitals in Mashhad. Electron Physician. 2017;9(8):5159. doi:10.19082/5159
35. Gloria Umuhoza A, Bosco Kamugisha J, Nashwan AJ, Tahuna Soko G. Assessment of knowledge and practices of hand hygiene among health workers in Rwanda. Int J Afr Nurs Sci. 2023;19:100585. doi:10.1016/j.ijans.2023.100585
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.