")
Back to Journals » International Journal of Nanomedicine » Volume 20
Mesenchymal Stem Cell-Derived Extracellular Vesicles: Emerging Therapies for Neurodegenerative Diseases
Authors Chen P, Wang F, Ling B, Zhu Y, Lin H, Huang J, Wang X
Received 24 March 2025
Accepted for publication 26 June 2025
Published 2 July 2025 Volume 2025:20 Pages 8547—8565
DOI https://doi.org/10.2147/IJN.S526945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Eng San Thian
Puwen Chen,1,2,* Fangsheng Wang,2,* Baodian Ling,2 Yifan Zhu,1,2 Haihong Lin,1,2 Junyun Huang,1 Xiaoling Wang1
1The First School of Clinical Medicine, Gannan Medical University, Ganzhou, 341000, People’s Republic of China; 2Laboratory Medicine, First Affiliated Hospital of Gannan Medical University, Ganzhou, 341000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoling Wang, The First School of Clinical Medicine, Gannan Medical University, Ganzhou, People’s Republic of China, Email [email protected] Junyun Huang, The First School of Clinical Medicine, Gannan Medical University, Ganzhou, People’s Republic of China, Email [email protected]
Abstract: Neurodegenerative diseases are a group of chronic diseases characterized by a gradual loss of neurons that worsens over time and dysfunction. These diseases are extremely harmful, not only affecting the physical health of the patients, but also having a serious impact on their quality of life. They mainly include Alzheimer’s disease (AD), Parkinson’s disease (PD), Huntington’s disease (HD), Amyotrophic lateral sclerosis (ALS), etc. Their pathogenesis is complex, and it is difficult for the existing treatments to effectively slow down the progression of the disease. In recent years, Mesenchymal Stem Cells (MSCs) have received widespread attention for their anti-inflammatory, immunomodulatory and neuroprotective properties. In this context, MSC-derived Extracellular Vesicles (MSC-EVs) have demonstrated unique therapeutic potential as a cell-free therapeutic strategy. MSC-EVs are rich in bioactive substances such as proteins, lipids, mRNAs and miRNAs, which can pass through the blood-brain barrier and be targeted to the diseased area to regulate neuronal survival, synaptic plasticity and neuroinflammatory responses. In addition, compared with stem cell therapy, MSC-EVs have the advantages of low immunogenicity, easy storage and transportation, and avoiding ethical controversies. However, their clinical application still faces challenges: standardized isolation and purification techniques have not been unified, vesicle loading efficiency and targeting need to be further optimized, and long-term safety needs to be systematically evaluated. This review focuses on the role of MSC-EVs in the development of neurological diseases and explores their possible dual roles, both favorable and unfavorable, in the context of neurological diseases. In addition, this review provides a review of current studies on EVs as potential biomarkers for the diagnosis and treatment of neurodegenerative diseases and provides a comprehensive review of the prospects and challenges of MSC-EVs in clinical applications.
Keywords: Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, amyotrophic lateral sclerosis, mesenchymal stem cell, extracellular vesicles
Introduction
Neurodegenerative diseases (NDs) are a group of complex diseases characterized by progressive neuronal degeneration and loss of function, which are usually closely related to ageing. They mainly include Alzheimer’s disease (AD), Parkinson’s disease (PD), Huntington’s disease (HD), Amyotrophic lateral sclerosis (ALS), etc. Alzheimer’s disease primarily impacts memory and cognitive function. It is characterized by the accumulation of amyloid plaques and tau tangles in the brain, leading to progressive neuronal loss. This degeneration results in a spectrum of symptoms ranging from mild forgetfulness to severe dementia.1 Parkinson’s disease is characterized by the degeneration of neurons that produce dopamine in the substantia nigra. The symptoms include tremors, muscle rigidity, bradykinesia, and balance difficulties, often accompanied by non-motor issues such as depression and sleep disturbances.2 Huntington’s disease is a hereditary neurodegenerative disorder caused by abnormal CAG repeat sequences in the HTT gene, resulting in the production of toxic Huntington protein. It is manifested as involuntary dance movements, cognitive decline and mental symptoms, gradually damaging daily life.3 Amyotrophic lateral sclerosis (ALS) is characterized by attacking motor neurons, resulting in muscle weakness, atrophy and paralysis. It affects the motor neurons in the upper and lower limbs, leading to symptoms ranging from limb stiffness and slurred speech to respiratory failure. As there is currently no cure, patients usually survive for 3 to 5 years after diagnosis.4 With the aging of the global population, their incidence is increasing year by year, and they have become an important public health problem that threatens the health of human beings. The pathogenesis of these diseases is complex and varied, involving the interaction of multiple factors such as protein misfolding and abnormal aggregation, mitochondrial dysfunction, oxidative stress, neuroinflammatory response, and epigenetic regulatory abnormalities. The main manifestations are cognitive decline, motor dysfunction, behavioral abnormalities or autonomic dysregulation, which ultimately lead to the loss of self-care ability. Currently, clinical treatment is based on symptomatic support, but cannot effectively slow down or reverse the disease process. In recent years, with the development of molecular biology and regenerative medicine, novel therapeutic strategies targeting pathological protein clearance, neuroprotection and stem cell therapy have attracted much attention, providing a potential direction for breaking through the bottleneck of traditional treatment.5
Mesenchymal Stem Cells (MSCs) are pluripotent stem cells capable of self-renewal and multidirectional development. In recent years, MSC therapy has demonstrated significant potential across various domains, with numerous clinical studies conducted globally, addressing a diverse array of conditions, including but not limited to osteoarthritis, diabetes, cardiovascular diseases, neurological disorders, hepatic diseases, and pulmonary diseases.6 Numerous clinical studies have demonstrated that MSCs possess multidirectional differentiation potential and immunomodulatory effects, originating from diverse sources and exhibiting a degree of safety and efficacy, thereby offering new hope for the treatment of certain intractable diseases.7 Moreover, there are deficiencies including inconsistent therapeutic efficacy, an incompletely understood mechanism, challenges in quality control, and elevated costs. Nonetheless, MSC therapy, as an emerging treatment modality, retains significant potential for widespread application. Currently, MSC therapy remains in the clinical research phase, necessitating further comprehensive investigation into its therapeutic mechanisms, optimization of treatment protocols, enhancement of efficacy and safety, and simultaneous reduction of costs to facilitate its broad clinical application.8
According the MISEV2023 standards, extracellular vesicles (EVs) are lipid bilayer-encased particles released from cells that lack self-replication capabilities (ie, they do not possess a functional nucleus) and play significant roles in intercellular communication, disease diagnostics, and therapeutic applications. EVs comprise small extracellular vesicles (sEVs), microvesicles (MVs), and apoptotic bodies.9 sEVs are extracellular vesicles that are secreted from the interior of the cell via multivesicular bodies (MVBs). They range from 30 to 150 nm in diameter and are extruded from the cell through the fusion of intracellular multivesicular structures with the cell membrane. sEVs are abundant in physiologically active compounds, including proteins, nucleic acids (eg, microRNAs, messenger RNAs, long non-coding RNAs), and lipids.10 MVs denote EVs that are expelled from the cell membrane. sEVs range from 100 to 1000 nanometers in diameter and are generated straight from the cell membrane. Microvesicles encompass an array of bioactive substances, including proteins, nucleic acids, and lipids. Apoptotic bodies are membrane entities, ranging from 500 to 2000 nm in diameter, that are vesicles generated during apoptosis. Apoptotic bodies comprise cellular detritus, nucleic acids, and proteins.9,11 Extracellular vesicles have been linked in studies to the onset and progression of neurodegenerative disorders like Parkinson’s and Alzheimer’s. It might emerge as a novel therapeutic target for neurodegenerative illnesses.12
Biogenesis of EVs
EVs mainly include sEVs, MVs, and Apoptotic bodies. The synthesis of sEVs commences with the invagination of the cell membrane, resulting in the creation of early endosomes that mature within the cell and aggregate tiny vesicles to develop MVBs.13 Small vesicles within multivesicular bodies (MVBs) can undergo degradation by fusion with lysosomes or can merge with the cell membrane. Fusion with the cell membrane results in the release of vesicles into the extracellular environment, which are identified as sEVs. MVs are generated directly from the cell membrane through cellular detachment, and the architecture of the phospholipid bilayer is modified when the cell encounters external stimuli (eg, mechanical stress, oxidative stress, inflammatory factors) or internal signals (eg, calcium signals).14 The cytoskeleton, such as actin, also contributes to this process beneath the cell membrane. The reorganization of the cytoskeleton induces localized protrusions of the cell membrane, which, when reaching a specific threshold, detach and create microvesicles. During platelet activation, elevated calcium signaling induces actin reorganization, resulting in the creation of microvesicles in the platelet cell membrane, which are crucial to the coagulation process.10 Apoptotic vesicles are byproducts of apoptosis. During apoptosis, cells experience a sequence of systematic morphological alterations. Initially, alterations occur in the nucleus, characterized by the coalescence and margination of chromatin, subsequent rupture of the nuclear membrane, along with cytoplasmic contraction, invagination of the cell membrane, and segmentation of the cell.15 The segmentation of the cell membrane is accomplished through the activation of a succession of cysteine asparaginases (caspases). These enzymes degrade various proteins within the cell, resulting in the disintegration of the cellular structure. Ultimately, the cell membrane separates the cell into many apoptotic vesicles of varied sizes, each containing components such as cellular debris, organelles, and chromatin.16,17
Neurodegenerative Disease
Alzheimer’s Disease
The pathophysiology of AD is intricate and not yet completely elucidated. The hypotheses encompass the amyloid cascade hypothesis, the tau protein hypothesis, the neuroinflammation hypothesis, and the oxidative stress hypothesis. (Figure 1) The amyloid cascade hypothesis posits that β-amyloid (Aβ) is generated through the enzymatic cleavage of amyloid precursor proteins. Aβ42 readily aggregates and precipitates to form senile plaques, and its oligomers are neurotoxic, capable of damaging cell membranes, inducing inflammation, disrupting synaptic function, and resulting in synaptic loss.1 The neuroinflammation hypothesis suggests that microglia are activated in the brain, and over-activation releases inflammatory mediators that damage neurons, and inflammation also promotes abnormal changes in Aβ and tau proteins, creating a vicious cycle; the oxidative stress hypothesis suggests that an imbalance between oxidative and antioxidative oxidation leads to neuronal biomolecule damage and death,18 due to increased production of reactive oxygen species and impaired antioxidant defenses due to mitochondrial dysfunction and Aβ toxicity.19,20 The integrity of the blood-brain barrier (BBB) is compromised by the deposition of Aβ proteins, inflammatory responses, or damage to the vascular endothelium, facilitating the entry of peripheral blood components into the brain and allowing substances within the brain to leak into the peripheral bloodstream.21 Abnormal vascular function manifests as endothelial cell dysfunction, altered vascular smooth muscle cell activity, and irregularities in perivascular cells. Impaired vascular function compromises cerebral blood circulation, depriving the brain of essential nutrients and oxygen.22 The disturbance of the neurovascular unit impairs the brain’s waste elimination function. Metabolic waste products in the brain, including Aβ protein, are typically eliminated via the perivascular system. The failure of the neurovascular unit diminishes the clearance of Aβ protein, resulting in its accumulation in the brain and exacerbating the condition of AD.23
 |
Figure 1 Pathogenesis of Alzheimer’s disease (AD), Parkinson’s disease (PD), Huntington’s disease (HD), Amyotrophic lateral sclerosis (ALS). |
Parkinson’s Disease
α-synuclein (α-syn), which is crucial for normal physiological function, undergoes structural modifications in individuals with PD.2,24 (Figure 1) These alterations in the N-terminal and non-Aβ component regions result in protein misfolding and aggregation, forming Lewy bodies that accumulate in nigrostriatal dopaminergic neurons.2 This accumulation obstructs the transport of substances that influence neurotransmitter connections, simultaneously activating stress response and inflammatory pathways, ultimately causing neuronal dysfunction and death. The mitochondria in neurons exhibit structural abnormalities, including swelling, cristae disruption, and diminished functionality of the respiratory chain complexes, resulting in decreased ATP production and impaired neuronal function.24 Additionally, this dysfunction elevates the generation of reactive oxygen species beyond the cells’ antioxidant capacity due to increased electron leakage, causing oxidative damage to biomolecules and further compromising mitochondrial integrity, thereby establishing a detrimental feedback loop. Furthermore, excessive activation of microglial cells incites neuroinflammation, alongside the activation of α-synuclein.25 Furthermore, neuronal damage reveals antigens and initiates an autoimmune response, wherein T cells activate cytotoxic T lymphocytes to assault neurons, B cells produce antibodies that, when activated by complement, harm neurons, and immune cell infiltration along with inflammation leads to the destruction of neural tissues. The microenvironment influences neuronal viability and functionality.26
Huntington’s Disease
HD is an autosomal dominant neurodegenerative disorder caused by the abnormal amplification of CAG trinucleotide repeats in the first exon of the Huntington gene located on the short arm of chromosome 4.3(Figure 1) This leads to the elongation of the N-terminal polyglutamine chain of the Huntington protein, resulting in aggregate formation and increased toxicity.3,27,28 The aberrant Huntington protein accumulates excessively within the cell and is challenging to eliminate due to its interference with the normal functioning of the ubiquitin-proteasome system and the autophagy-lysosome system.29 Huntington’s proteins amass excessively within cells and are challenging to eliminate due to their disruption of the ubiquitin-proteasome system and autophagy-lysosome system, while concurrently affecting gene transcription regulation and impeding the cytoskeleton-associated axonal transport system, thereby obstructing inter-neuronal signaling and synaptic functionality.30 The striatal neurons exhibit sensitivity to Huntington’s proteins, and the demise of a significant quantity of these neurons results in the impairment of neural circuits connecting the striatum to other brain regions, hence impacting motor, cognitive, and emotional functioning. The aberrant Huntington’s protein adversely influences neuroplasticity, hindering synaptic plasticity, long-term potentiation, and long-term inhibition, hence aggravating cognitive impairments in patients.28,31
Amyotrophic Lateral Sclerosis
ALS is a complicated neurodegenerative disease whose pathophysiology is not fully understood.(Figure 1) Approximately 10–15% of familial ALS cases are attributed to gene mutations, including those in superoxide dismutase 1 (SOD1), TAR DNA binding protein 43 (TDP43), and sarcoma fusion proteins. These mutations alter the structure and function of the respective proteins, thereby disrupting normal neuronal physiology and leading to cell death or interference with RNA-related processes that initiate neurodegenerative changes.32 Additionally, sporadic ALS is characterized by protein misfolding and aggregation, which disrupt normal cellular functions and provoke a stress response when the protective mechanisms fail to eliminate the aggregates. Sporadic ALS is characterized by protein misfolding and aggregation, which disrupt normal cellular physiology and initiate a stress response, resulting in neuronal damage and death when the protective mechanisms fail to eliminate the aggregates.32,33 This condition also impairs the axonal transport system, causing abnormal transport molecule function and reduced microtubule stability, thereby obstructing the transport of essential substances within the axon, adversely affecting neuronal signal transmission and nutrient support, ultimately leading to functional impairment and degenerative alterations.33 Glial cells In the course of pathogenesis, glial cells become activated to secrete inflammatory mediators, which exert neurotoxic effects and intensify oxidative stress; this results in an augmented production of reactive oxygen species within neurons and a compromised antioxidant defense system, leading to oxidative damage to cellular structures and functions, ultimately culminating in neuronal death; dysregulation of glutamate metabolism and transporters causes elevated concentrations in synaptic clefts, resulting in excessive receptor activation and calcium ion overload, which initiates a cascade of injuries that further exacerbate neuronal damage; multiple factors instigate apoptosis.34 The neuronal apoptosis process is initiated by various factors, while autophagy dysfunction fails to eliminate abnormal substances, exacerbating the toxic environment. Abnormalities in mitochondrial structure and function, morphological alterations, and diminished activity of respiratory chain complexes lead to decreased ATP production and impaired energy metabolism. This also results in elevated reactive oxygen species, intensifying oxidative stress damage and activating apoptosis signaling pathways that culminate in neuronal death.4
The Role of EVs in Neurodegenerative Diseases
As Marker
In AD, increased concentrations of Aβ42 and phosphorylated tau protein (p-tau) in extracellular vesicles are significant for early detection.1 Aβ protein is produced by a series of enzymatic cleavages of amyloid precursor protein (APP), and under normal physiological conditions its production and clearance are in balance. In the initial phases of AD, this equilibrium is disrupted, resulting in a substantially increased production of Aβ42, which tends to collect; alterations in its percentage within extracellular vesicles manifest prior to neuronal loss and the emergence of clinical symptoms.35 This alteration can be identified in blood or cerebrospinal fluid extracellular vesicles by advanced detection methods, offering insights for early diagnosis. Moreover, phosphorylated tau protein (p-tau) concentrations are heightened in extracellular vesicles during the initial phases of AD.36 The tau protein, which typically serves to stabilize neuronal microtubule structures, is aberrantly phosphorylated in the etiology of AD, leading to its dissociation from microtubules and the formation of neurofibrillary tangles (NFTs). Prior to the production of NFTs, p-tau commences accumulation in EVs. P-tau proteins exhibit distinct characteristics of variation at different phosphorylation sites during the developmental phases of AD.37 For instance, the phosphorylation levels of p-tau181, p-tau217, and other sites exhibit considerable alterations in the initial phases of AD. Utilizing highly specific antibodies or alternative detection methods enables the quantification of p-tau protein at designated phosphorylation sites in extracellular EVs. This test can identify early indicators of AD prior to the emergence of substantial clinical symptoms.38 Alterations in these p-tau proteins within EVs signify aberrant phosphorylation of tau proteins in neurons, which is a critical component of AD pathogenesis.39 Consequently, these EVs containing p-tau may serve as indicators of early AD for screening and diagnosis. As AD progressed, the concentrations of Aβ and p-tau proteins in extracellular EVs escalated, demonstrating a strong link with the extent of cognitive deterioration.37 Minor alterations in Aβ and p-tau concentrations in extracellular vesicles may commence during the mild cognitive impairment (MCI) phase, with these markers exhibiting a substantial increase when the condition advances to the dementia stage. For instance, by consistently quantifying Aβ42 and p-tau protein levels at various phosphorylation sites in blood or cerebrospinal fluid extracellular vesicles, one can delineate the progression of a patient’s condition, comprehend the velocity of transition from mild cognitive impairment to AD dementia, and evaluate the effects of therapeutic interventions on disease advancement.40,41
In PD, α-synuclein is a primary pathology marker of the condition. In the initial stages of the disease, neurons secrete increased amounts of α-syn in EVs.42 Typically, α-synuclein participates in neurotransmitter release at the presynaptic terminals of neurons; however, in PD, it misfolds and accumulates.43 The aggregation process initiates locally and disseminates among neurons by EVs, resulting in early alterations in α-synuclein levels in blood or cerebrospinal fluid EVs before the onset of motor symptoms, hence serving as a potential early diagnostic marker.44 In the initial phases of the disease, α-synuclein concentrations in extracellular vesicles increase, despite the absence of pronounced motor symptoms (eg, tremor, myotonia, bradykinesia, etc). The α-syn oligomers transported by these EVs can propagate between neurons, functioning as “seeds” that trigger the aggregation of normal α-syn, so amplifying the extent of the lesion.45 The initial alteration in α-synuclein can be identified by identifying extracellular vesicles in blood or cerebrospinal fluid. This assay possesses significant potential as it can identify abnormalities in the preclinical phase of the disease, facilitating early diagnosis and intervention. Advanced detection techniques, including immunoassay-based methods and innovative biosensor technologies, can sensitively measure α-syn quantities in EVs.44 Moreover, the expression of DJ-1 protein in extracellular vesicles is also modified in patients with PD. The DJ-1 protein performs tasks including antioxidative stress, and its abnormal expression in PD may be associated with oxidative stress imbalance. In the extracellular vesicles of PD patients, the expression level and modification status (eg, oxidation, phosphorylation, etc.) of the DJ-1 protein are altered.46 These alterations, along with anomalies in α-syn, represent critical data for early diagnosis. For instance, when DJ-1 protein undergoes oxidative modification due to oxidative stress, its quantity and active form in EVs may be modified, while the concentration of α-synuclein in EVs increases. This concurrent alteration may more precisely signify the early onset of PD than the detection of α-synuclein in isolation. Furthermore, alterations in DJ-1 protein may indicate, to a certain degree, a disruption in the intracellular redox state, which is associated with the aberrant aggregation of α-syn in relation to pathophysiological causes, offering a more thorough insight for early diagnosis. Moreover, additional elements in EVs, including specific small molecule RNAs or proteins linked to oxidative stress or neuronal function, may interact with DJ-1 protein and α-syn, so enhancing the marker repertoire for early detection.47,48
Mutant Huntington’s protein (mHTT) in EVs is a pivotal biomarker in HD. mHTT arises from an anomalous amplification of the CAG trinucleotide repeat sequence in the Huntington’s gene (HTT),27 resulting in a toxic protein that adversely affects neurons. In the initial stages of the disease, mHTT-containing extracellular vesicles can be identified in blood or cerebrospinal fluid, with these alterations occurring prior to the manifestation of overt clinical symptoms. The expression of HD-associated miRNAs in EVs is concurrently modified. These miRNAs may regulate mHTT expression or be linked to the pathophysiological processes of HD, and alongside mHTT, they function as distinctive markers for the early diagnosis of HD, aiding in the differentiation of HD from other disorders exhibiting similar motor or cognitive symptoms.49 Alterations in the expression of HD-associated miRNAs in extracellular vesicles contribute to early diagnosis. These miRNAs may contribute to the pathophysiology of HD through many mechanisms, including the regulation of mHTT expression and the modulation of neuronal survival and function. Certain miRNAs may interact with the mRNA of mHTT, influencing its translation efficiency or stability. In the initial phase of HD, the expression levels of certain miRNAs may be either upregulated or downregulated in EVs, and these alterations, along with the presence of mHTT in EVs, provide a composite of characteristic indicators for the early diagnosis of HD.50 Detecting alterations in these miRNAs and mHTT within EVs enables more precise identification of patients with HD at an early stage, facilitating subsequent therapy chances.51
In ALS, fluctuations in neurofilament proteins and TDP-43 proteins within EVs serve as a crucial foundation for disease diagnosis and monitoring.52 Neurofilament proteins are essential constituents of the neuronal cytoskeleton, and their production, assembly, and transport are meticulously regulated under normal circumstances. Nonetheless, the metabolism of neurofilament proteins is disrupted in the initial phases of ALS onset due to neuronal injury and degeneration, resulting in a marked elevation of their levels in extracellular vesicles.53 This alteration can be identified by analyzing blood or cerebral fluid extracellular vesicles prior to the onset of clinical symptoms, rendering it a prospective biomarker for early identification. TDP-43 protein is pathologically modified in ALS; it is typically localized in the nucleus and participates in RNA metabolism, but in ALS, it is mislocalized to the cytoplasm, forming aberrant aggregates and is discharged encased in extracellular vesicles.54 The identification of phosphorylated or ubiquitinated TDP-43 and its aggregated variant in extracellular vesicles markedly enhances diagnostic sensitivity and specificity. As ALS advanced, indicators inside EVs exhibited dynamic alterations.55 The concentration of neurofilament proteins escalated with the worsening of neuronal injury, while the extent of aberrant aggregation and structural characteristics of TDP-43 concurrently degraded, closely correlating with the severity of muscle atrophy and motor dysfunction in patients. Initially, neurofilament proteins exhibited mild elevation, and a minor quantity of TDP-43 was aberrantly localized in extracellular vesicles; during the intermediate phase, both anomalies were markedly intensified, accompanied by the upregulation of stress-related miRNA expression; in the final stage, the abnormalities of the markers peaked alongside the accumulation of proteins associated with apoptosis or inflammation.56 These stage-specific characteristics not only establish a foundation for illness staging but also inform the formulation of individualized treatment strategies. By consistently monitoring EV indicators, doctors can evaluate illness progression, timely modify intervention tactics, and enhance therapy outcomes. In conclusion, the detection of EVs-based neurofilament protein and TDP-43 facilitates early diagnosis, disease progression monitoring, and targeted treatment of ALS, possessing significant clinical translational value (Table 1).55–58
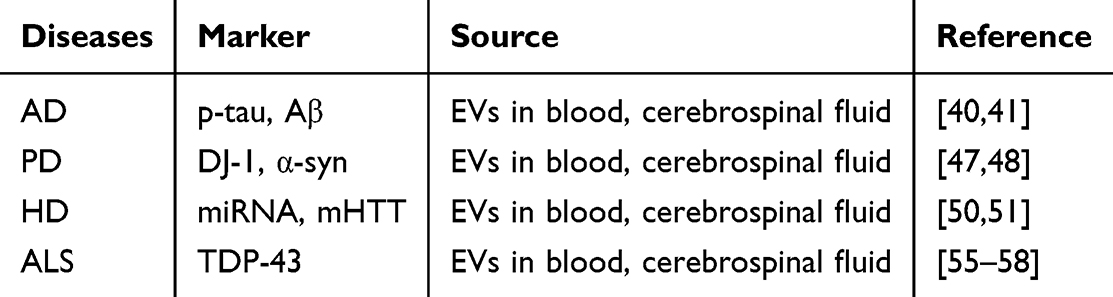 |
Table 1 Markers of Mesenchymal Stem Cell-Derived Extracellular Vesicles in Neurodegenerative Diseases |
As Drug Delivery Systems
EVs are nanoscale lipid bilayer vesicles generated by spontaneous cellular secretion, resembling cell membranes in composition and containing biomolecules like proteins, lipids, and nucleic acids.59 This natural composition provides exceptional biocompatibility, allowing them to function synergistically with cells and tissues in living creatures without provoking significant immune rejection.60 In patients with neurodegenerative disorders, where the condition may induce inappropriate immune system activation, it is crucial to employ medication delivery systems that are hypoimmunogenic to prevent aggravation of the disease due to immunological reactions. In comparison to certain synthetic drug carriers, like liposomes and polymeric nanoparticles, the reduced immunogenicity of EVs enhances their stability in circulation and dissemination throughout the body.60,61 Conventional carriers may incorporate contaminants or immunogenic agents during production, resulting in an immunological response that can impact drug delivery and the patient’s general health. EVs can successfully avoid these difficulties and are more suitable for long-term and recurrent drug administration, offering a trustworthy assurance for the continued treatment of neurodegenerative illnesses.62
Ability to Cross the Blood-Brain Barrier
The blood-brain barrier is a stringent physiological barrier separating the central nervous system from peripheral blood circulation, which limits the passage of most macromolecules and pharmaceuticals from the bloodstream into brain tissue.63 This trait hinders the ability of numerous medications employed in the treatment of neurodegenerative illnesses to access brain lesions, significantly impairing their therapeutic efficacy.61 Certain proteins and nucleic acids with potential therapeutic efficacy are challenging to utilize in the treatment of neurodegenerative illnesses due to their inability to successfully traverse the blood-brain barrier.61 Nevertheless, EVs possess the inherent capacity to traverse the blood-brain barrier, representing a significant advancement in medication delivery for neurodegenerative disorders.64 The mechanisms of crossing are varied: EVs can penetrate endothelial cells through cytotransmission by attaching to specific receptors on the blood-brain barrier and are subsequently released into brain tissue; alternatively, they can utilize intercellular tight junctions to transport drugs into the brain. This distinctive capability enables the successful delivery of medications, which would otherwise struggle to access the affected regions of the brain, via EVs, hence presenting the potential for therapeutic therapy of neurodegenerative illnesses.65
Targeted Drug Delivery
EVs are abundant in proteins, lipids, and other surface indicators that can selectively attach to receptors or ligands on sick cells, facilitating precision targeted medication delivery.66 In several neurodegenerative illnesses, the expression of receptors on the surface of affected cells frequently exhibits distinct alterations. In AD, the expression of certain receptors on the surface of affected neurons is upregulated, or novel receptors emerge.63 Electric vehicles can recognize and attach to these receptors via specific surface markers, subsequently delivering drugs directly to lesion neurons, thereby augmenting drug concentration in the lesion area, enhancing therapeutic efficacy, and concurrently minimizing adverse effects on healthy tissues.67 Simultaneously, with genetic engineering technologies, EVs can be tailored to improve their targeting capabilities. By incorporating antibody or ligand genes that precisely recognize sick cells associated with neurodegenerative illnesses into EV-producing cells, relevant targeting molecules can be generated on the surface of EVs.68 Utilizing PD as a case study, ligand genes specific to PD neurons can be incorporated into the cells, allowing extracellular vesicles to transport medications to PD lesions with enhanced accuracy, thereby facilitating personalized drug delivery and augmenting the efficacy and safety of treatment.69
Co-Delivery Capacity of Multiple Drugs
The pathophysiology of neurodegenerative illnesses is intricate and typically encompasses various pathogenic factors, making it challenging to attain optimal therapeutic outcomes with a singular medication. Consequently, synergistic therapy utilizing various pharmaceuticals is a crucial approach to enhance therapeutic efficacy.70 EVs possess substantial internal capacity and favorable hydrodynamic characteristics and stability, enabling them to simultaneously house and transport several medication kinds, including small molecule chemicals, proteins, and nucleic acids.60 The co-delivery of numerous therapeutic agents to the lesion site through extracellular vesicles enables various medications to produce synergistic effects within the same cell, so intervening more comprehensively in the disease’s pathological process.71 In the management of HD, tiny interfering RNAs that diminish the expression of mutant Huntington’s proteins and neuroprotective small molecule medicines can be concurrently encapsulated into extracellular vesicles. Thus, following administration to the afflicted neurons, the small interfering RNA can suppress the synthesis of mutant proteins at the genetic level, while the small molecule drug can directly safeguard the neurons from injury. The synergistic effect of both is anticipated to be more efficacious in decelerating disease progression and offering robust support for the treatment of neurodegenerative disorders.72
Drug Slow Release Function
The lipid bilayer composition of extracellular vesicles is fundamental to their function of gradual drug release.73 This lipid membrane functions as a natural protective barrier that encases the medication, isolating it from the external environment and delaying direct contact with surrounding tissue fluid or extracellular matrix, so impeding the drug’s diffusion outward. Simultaneously, intricate interactions occur between the biomolecules within EVs and the drug, which also influence the drug’s release rate.74 Certain proteins within EVs may interact with drug molecules via electrostatic interactions, hydrogen bonding, or hydrophobic interactions, resulting in a gradual release of the drug molecules from EVs into the surrounding environment over time, rather than an instantaneous release, as these interactions dynamically change. Furthermore, the release profiles of various drug types encapsulated in EVs exhibit distinct variations. Small molecule compound drugs may gradually diffuse through minute pores in the lipid bilayer membrane or during alterations in membrane fluidity.66 In contrast, the release of large molecule protein or nucleic acid drugs is primarily contingent upon the interactions between EVs and target cells, subsequently entering the cells via membrane fusion or endocytosis, and then being gradually released under the influence of the intracellular milieu. The entire process is comparatively sluggish and protracted.75 The consistent and persistent efficacy of medications on the lesion is essential for managing the course of neurodegenerative disorders. EVs facilitate the gradual release of pharmaceuticals, thereby mitigating the swift distribution and metabolism of drugs in non-lesional tissues. This mechanism prevents the accumulation of substantial drug quantities in undesired regions within a brief timeframe, while concurrently enhancing the effective utilization of drugs in lesional areas.66,76 For instance, certain long-acting neuroprotective agents administered near affected neurons through extracellular vesicles can be released persistently over several days or weeks, ensuring a relatively stable drug concentration that continuously provides neuroprotection, thereby preventing further neuronal damage or decelerating degenerative processes. This obviates the necessity for frequent drug injections or administration, thereby alleviating patient discomfort and medical burden, while also mitigating the potential adverse effects associated with fluctuating blood drug concentrations from frequent dosing. This approach offers patients more stable, enduring, and efficacious therapeutic outcomes, which can enhance symptom management of neurodegenerative diseases, improve patients’ quality of life, and extend their survival duration.60
Involvement in the Clearance of Pathogenic Proteins
Encapsulation and Transport of Pathogenic Proteins
In a typical cellular setting, protein folding and conformation are governed by stringent quality control mechanisms. In neurodegenerative illnesses, proteins misfold or aggregate improperly, resulting in the formation of pathogenic proteins due to genetic abnormalities, environmental influences, and other causes. Extracellular vesicles can identify these anomalous pathogenic proteins via several molecular pathways present on their surface.77 For instance, certain receptor proteins on the surface of extracellular vesicles can selectively identify certain structural domains or aberrant modification sites on pathogenic proteins. In AD, receptors like low-density lipoprotein receptor-related protein 1 (LRP1) on the surface of EVs can identify Aβ,78 while specific phosphorylation sites on tau proteins are recognized by particular protein kinases on EV surfaces, thereby commencing the encapsulation of tau proteins. Besides receptor recognition, intracellular molecular chaperone proteins significantly contribute to the identification and encapsulation of harmful proteins. Molecular chaperone proteins facilitate the proper folding of proteins; upon identifying misfolded pathogenic proteins, they attach to these proteins and direct them toward encapsulation in EVs. Molecular chaperone proteins, including Heat Shock Protein 70 (HSP70), can associate with α-synuclein to promote its encapsulation in EVs, thereby inhibiting the aberrant aggregation of α-synuclein and its deleterious effects within the cell.79 Upon recognition and encapsulation of pathogenic proteins by EVs, these vesicles facilitate the transfer of the proteins to the extracellular milieu via their secretion mechanism. The secretion of EVs is governed by the regulation of many signaling pathways and molecular mechanisms within the cell. Intracellular Rab protein families, among others, regulate the transit and secretion of EVs. Upon the formation of EVs laden with pathogenic proteins, Rab proteins facilitate their transport to the cell membrane by interacting with cytoskeletal proteins and membrane receptors, culminating in their exocytosis.80 The export of pathogenic proteins to the extracellular milieu is crucial for cellular self-defense. The pathological aggregation of α-synuclein in neurons is a primary contributor to neuronal injury and mortality in PD. The extracellular transport of α-synuclein via extracellular vesicles can diminish its accumulation in neurons, hence mitigating neurotoxicity and decelerating disease progression.81
Mediating Cell-to-Cell Delivery and Clearance of Pathogenic Proteins
The intercellular transmission of EVs is a significant mechanism for the dissemination of harmful proteins in neurodegenerative disorders. EVs harboring pathogenic proteins can transmit these proteins to adjacent cells via the extracellular matrix or through direct cellular contact.77 In HD, mutant Huntington’s protein (mHTT) can be encapsulated in EVs and transmitted between neurons. This intercellular transmission can transpire not only between adjacent neurons but also between neurons in disparate brain areas via pathways such as neural circuits, resulting in the progressive decline of the disease.81 The membrane architecture and surface molecules of extracellular vesicles are crucial for intercellular communication. Certain proteins and lipid constituents on the surface of EVs can engage with receptors or ligands on the target cell surface, facilitating the Certain proteins and lipid constituents on the surface of EVs can engage with receptors or ligands on target cells, facilitating the fusion or endocytosis of EVs and thereby enabling the transport of harmful proteins.41 Lipid constituents, such as phosphatidylserine on the surface of EVs, can be identified by receptors on target cells, initiating endocytosis and the internalization of EVs along with their pathogenic proteins into the cells. While EV-mediated transport of pathogenic proteins negatively impacts disease transmission, it also presents a chance for the clearance of these proteins.82 When EVs harboring pathogenic proteins are internalized by recipient cells, these cells may possess more effective clearance systems to manage the pathogenic proteins. For instance, several glial cells, including microglia and astrocytes, possess robust phagocytic and degradative functions, enabling them to destroy pathogenic proteins via their lysosomal system subsequent to the ingestion of extracellular vesicles containing these proteins. Lysosomes house an array of hydrolytic enzymes capable of degrading harmful proteins into smaller molecules, hence facilitating their elimination.83 Furthermore, EVs can augment their capacity to eliminate harmful proteins by modulating signaling pathways within the recipient cells. Certain signaling molecules in extracellular vesicles can activate the autophagy signaling pathway in recipient cells, enhance the creation and fusion of autophagosomes, and thereby augment the autophagic clearance efficiency of cells against harmful proteins.82
Involvement in Immune Regulation and Clearance of Pathogenic Proteins
EVs can serve as an immunological activation signal in neurodegenerative disorders, prompting the immune system to eliminate harmful proteins. When extracellular vesicles transport pathogenic proteins into the extracellular milieu, they can be identified by immune system cells, including macrophages and dendritic cells.84 A diverse array of pattern recognition receptors is present on the surface of these immune cells, enabling them to identify pathogen-associated molecular patterns or damage-associated molecular patterns on the surface of extracellular vesicles. For instance, certain glycoprotein or lipid constituents on the surface of extracellular vesicles can be identified by Toll-like receptors on macrophages, thereby activating them. Activated immune cells secrete various cytokines and chemokines, including interleukin-1β (IL-1β), tumor necrosis factor-α (TNF-α), and chemokine CCL2, which initiate inflammatory reactions. The inflammatory response can recruit additional immune cells, including neutrophils and lymphocytes, to the lesion site, where they collectively engage in the elimination of harmful proteins.85 In AD, EV-activated microglia can eliminate Aβ protein by phagocytosis, while the produced cytokines can modulate the functions of adjacent cells, thereby enhancing the clearance of pathogenic proteins.86 EVs not only stimulate immune responses but also modulate the clearance of pathogenic proteins by influencing immune cell activity. EVs can transport various immune regulatory components, including microRNAs and proteins, which can modulate the function of immune cells. EVs can transport immunomodulatory substances, including microRNAs and proteins, that affect the activity, differentiation, and migration of immune cells. For instance, miRNAs in certain EVs can target and modulate signaling pathways in immune cells, thereby reducing excessive activation of these cells and averting additional damage to neural regions resulting from inflammatory responses. Simultaneously, EVs can modulate the development and functionality of immune cells, enhancing their capacity to eliminate harmful proteins. Certain proteins in extracellular vesicles can facilitate the development of macrophages into phenotypes exhibiting enhanced phagocytic activity, hence improving their ability to phagocytose and eliminate pathogenic proteins. Furthermore, EVs can modulate lymphocyte function, prompting increased cytokine secretion to regulate the immune response and sustain immunological homeostasis, thereby enhancing the clearance of pathogenic proteins.84
Potential of MSCs in Treating Neurodegenerative Diseases
MSCs possess significant potential in the management of neurodegenerative disorders. It can assume a neuroprotective function by releasing antioxidant enzymes and molecules to neutralize reactive oxygen species in neurons, so alleviating damage from oxidative stress, including the reduction of Aβ-induced oxidative injury in neurons in AD.87 Additionally, it can mitigate neuronal death by modulating apoptotic signaling pathways, including the PI3K/Akt/mTOR protein family,88 employing secreted heat shock proteins to engage with apoptotic proteins in neurons, and releasing small RNA to suppress apoptotic protein expression, thereby decreasing apoptosis of dopaminergic neurons in the PD model. In the promotion of neuroregeneration, MSCs secrete brain-derived neurotrophic factor (BDNF), nerve growth factor, and other neurotrophic factors, which are essential for the proliferation and differentiation of neural stem cells.89 These factors can stimulate the proliferation of neural stem cells in the spinal cord and direct their differentiation into neurons, thereby aiding in the repair of damaged neural pathways in spinal cord injury research. It also supplies extracellular matrix components such as laminin and fibronectin that promote the development of neural synapses, offering physical support for their extension, directing their growth, and positively contributing to the repair of peripheral nerve injuries. The immunomodulatory role of MSCs is very significant. It can modulate the inflammatory response, suppress the secretion of pro-inflammatory cytokines such as IL-1β and TNF-α, and enhance the synthesis of anti-inflammatory cytokines such as IL-10.90 In conditions like AD and PD, it facilitates the transition of over-activated microglia from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype, thereby mitigating inflammatory damage to neurons.91 It can regulate T cells and B cells, decrease T cell proliferation and activation, and diminish autoimmune reactions, which aids in managing neurodegenerative illnesses with autoimmune components. Furthermore, MSCs or their produced extracellular vesicles possess the capability to traverse the blood-brain barrier. The blood-brain barrier typically obstructs the entry of most substances into the brain; nevertheless, MSCs can traverse it by secreting molecules that modulate its permeability or by engaging with the endothelial cells of the barrier.92,93 In animal investigations, labeled MSCs successfully traversed the blood-brain barrier into the brain parenchyma. Furthermore, MSCs can serve as targeted therapeutic vectors; following genetic modification, they can specifically recognize and address lesions associated with neurodegenerative diseases. This is accomplished by expressing receptors on their surface that bind to the targets of these diseases, thereby directing themselves and the therapeutic substances they secrete to precisely interact with the affected neurons, resulting in more effective treatment outcomes.92
Therapeutic Advantages of MSC-sEVs
Safety
MSC-EVs typically exhibit immunomodulatory characteristics, encompassing both immunosuppression and immunopromotion, alongside minimal immunogenicity.94–96 They are deficient in the major histocompatibility complex.97 This indicates that they are less prone to recognition and assault by the immune system when utilized allogeneically, and when transplanted among individuals, MSC-EVs are considerably less likely to provoke immune rejection than intact cells, thereby diminishing the risk of inflammation, tissue damage, and other consequences of immune responses.98 MSCs - extracellular vesicles can also execute immunomodulatory actions. They regulate the function of immune cells, including T cells, B cells, and macrophages.99 In an inflammatory milieu, they can suppress the hyperactive immune response and diminish the secretion of pro-inflammatory cytokines by transporting anti-inflammatory agents or modulating immune cell signaling pathways, thereby averting excessive immune attacks on self-tissues and mitigating the risk of immune-related disorders.95,100 Furthermore, MSC-derived extracellular vesicles are not whole cells and do not pose the risk of unregulated cell proliferation and tumorigenesis associated with cell transplantation. In contrast to stem cell therapy, stem cells may, under specific conditions, undergo malignant transformation and develop tumors due to their self-renewal and multidirectional differentiation capabilities. MSC-derived EVs are cell-secreted vesicles primarily involved in signaling and conveying bioactive chemicals. They lack the ability for cell division and malignant transformation, rendering them safer for therapeutic applications. Furthermore, the constituents of MSC-derived EVs mostly include proteins, nucleic acids (such as mRNA and miRNA), and lipids, which closely resemble the natural components found in live organisms.87 They can effectively interact with host cells and assimilate into cellular physiological processes. During tissue repair, the bioactive substances released by MSC-EVs can be absorbed by adjacent cells, facilitating normal metabolism and functional recovery without inducing toxicity or adverse reactions, unlike certain exogenous chemical drugs, due to the significant disparity between their chemical structure and in vivo components, thereby demonstrating excellent biocompatibility. Various quality control measures are employed during the preparation of MSC-EVs to assure their safety. Vesicles can be isolated and purified by ultracentrifugation, ultrafiltration, affinity chromatography, and other methods to eliminate impurities, cellular debris, and potential pathogens. These approaches can guarantee the integrity and quality of vesicle formulations while mitigating safety concerns, including allergic and inflammatory reactions due to contaminants.(Figure 2)
 |
Figure 2 Therapeutic advantages of MSC-EVs. |
Targeted
MSC-EVs can encapsulate several physiologically active molecules, including messenger RNA (mRNA), micro RNA (miRNA), and proteins.87 The contents of these packages can be sent to designated cells based on the vesicles’ targeting.101 In the process of tissue repair, vesicles can transport mRNAs and miRNAs that facilitate cell proliferation and differentiation, directing them to cells within the injured tissues. In inflammatory contexts, MSC-derived extracellular vesicles can be drawn by inflammatory signals and induce chemotaxis, facilitating targeted therapy. Inflammatory areas secrete several chemokines, including interleukin-8 (IL-8) and monocyte chemotactic protein-1 (MCP-1). Vesicles can detect the concentration gradient of chemokines and navigate towards the site of inflammation. Various membrane proteins and glycoproteins on the surface of MSC-derived EVs facilitate interactions with specific receptors on target cells, while integrins present on certain vesicles can identify receptors on the target cell surface. Integrins present on the surface of specific vesicles can identify extracellular matrix components or similar receptors on target cells.102 In the tumor microenvironment, some integrins can facilitate the aggregation of vesicles towards tumor cells. This targeting method, grounded in molecular recognition, facilitates the exact delivery of MSC-EVs to certain cell types, hence enabling targeted therapy. Ligand-receptor interactions on the vesicle surface are significant, as growth factors or cytokines present on the vesicle surface function as ligands that bind to the respective receptors on the target cell surface. The physicochemical characteristics of MSC-EVs, including size and charge, influence their targeting capabilities. The diminutive size of vesicles (often 30–1000nm) facilitates their penetration into biological tissues and enables targeted aggregation in certain tissue microenvironments, adhering to physicochemical principles.103 (Figure 2)
Multifunctionality
MSC-EVs can transport an array of growth factors and signaling molecules, including vascular endothelial growth factor (VEGF) and fibroblast growth factor (FGF). These chemicals can induce the growth of target cells.90 Simultaneously, certain micro RNAs (miRNAs) within vesicles can modulate the expression of genes associated with cell differentiation, directing the differentiation of stem cells into specific cell types, such as facilitating the conversion of neural stem cells into neurons, thereby aiding in the repair of neural tissues. MSCs - extracellular vesicles also significantly contribute to the development of angiogenesis. Angiogenic substances, including VEGF, can stimulate endothelial cells to promote cell migration and lumen development.104 In an inflammatory milieu, MSC-EVs can modulate the function of immune cells. They can suppress the secretion of pro-inflammatory cytokines, including IL-6 and TNF-α, while enhancing the synthesis of anti-inflammatory cytokines, such as IL-10. MSCs have regulatory influences on T cells and B cells. They can impede the growth and activation of T cells and diminish autoimmune reactions.105 MSCs - extracellular vesicles can also influence the fibrotic process. In fibrotic illnesses including liver fibrosis and pulmonary fibrosis, the deposition of extracellular matrix components, such as collagen, can be diminished by reducing the activation and proliferation of myofibroblasts.106 Certain miRNAs within vesicles can suppress the expression of fibrosis-associated genes, for instance, by suppressing the transforming growth factor-β (TGF-β) signaling pathway, thereby obstructing the conversion of normal cells into myofibroblasts and mitigating tissue fibrosis. MSCs can offer nutritional support to neuronal cells and safeguard them against oxidative stress, excitotoxicity, and other insults.106 They transport neurotrophic factors, including BDNF, which can promote the survival of neuronal cells.107 In models of neurodegenerative diseases, including Alzheimer’s and Parkinson’s, MSC-derived extracellular vesicles can diminish neuronal cell mortality. MSC-EVs can enhance neurite development and regeneration by transporting miRNAs and proteins associated with neural regeneration.108 (Figure 2)
Therapeutic Role of MSC-sEVs in Neurodegenerative Diseases
Neuroprotective Effect
Neurodegenerative diseases are typically associated with increased oxidative stress, resulting in heightened amounts of reactive oxygen species (ROS) in neuronal cells, which can subsequently impair cellular structure and function. MSC-sEVs are abundant in antioxidant enzymes and compounds, including superoxide dismutase (SOD) and glutathione peroxidase (GSH-Px). These components can be discharged into the extracellular environment or introduce antioxidants into the cell by fusing with nerve cells, thereby scavenging reactive oxygen species and mitigating oxidative stress damage to nerve cells. In an AD model, MSC-sEVs effectively diminished oxidative stress in neurons and safeguarded them from amyloid-beta (Aβ)-induced oxidative injury.109 MSC-sEVs can suppress neuronal death via various routes. They can control intracellular apoptosis-related signaling pathways, including the PI3K-Akt and Bcl-2 family proteins pathways. sEVs encompass certain proteins, including members of the heat shock protein (HSP) family, which engage with apoptotic proteins in neuronal cells and impede the activation of these apoptotic proteins. Conversely, miRNAs transported by MSC- sEVs significantly contribute to the anti-apoptotic mechanism. For instance, miR-21 is a prevalent anti-apoptotic miRNA that diminishes neuronal cell death by suppressing the expression of apoptotic proteins. In the PD model, anti-apoptotic agents like miR-21, conveyed by MSC-derived small extracellular vesicles, can markedly diminish apoptosis in dopaminergic neurons.110
Neurorestorative Effects
Mesenchymal stem cell-derived small extracellular vesicles (MSC-sEVs) encompass a range of neurotrophic substances, including brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF).111 These neurotrophic substances can enhance the proliferation and development of neural stem cells (NSC) and stimulate their differentiation into neurons. In spinal cord injury research, MSC-sEVs can enhance the proliferation of neural stem cells within the spinal cord and facilitate their differentiation into mature neurons, thereby aiding in the repair of damaged neural circuits.112 Additionally, certain extracellular matrix constituents in sEVs, like laminin and fibronectin, can offer structural support for neuronal synapse development and direct their extension pathways. Neuroinflammation is pivotal in the initiation and advancement of neurodegenerative diseases, and MSC- sEVs can influence neuroinflammatory responses to mitigate neuroinflammation by suppressing the secretion of pro-inflammatory cytokines, such as IL-1β and TNF-α, while simultaneously enhancing the production of anti-inflammatory cytokines, such as IL-10. In conditions like AD and PD, excessive microglial activation results in neuroinflammation, while MSC-sEVs can alter microglial phenotype from pro-inflammatory M1 to anti-inflammatory M2, thereby mitigating inflammatory damage to neuronal cells.113
Improvement of Neural Microenvironment
Neurodegenerative illnesses are associated with many neurotoxins, including Aβ deposition in AD and α-synuclein aggregation in PD. MSC-sEVs can eliminate neurotoxins from the neuronal milieu through phagocytosis or by binding to them. Certain receptors on the surface of MSC-sEVs can identify and attach to amyloid-beta (Aβ), which is subsequently internalized into sEVs through endocytosis and either degraded or transported to other extracellular locations for processing, thereby diminishing the accumulation of neurotoxins surrounding neuronal cells and enhancing their living environment.114 MSC-sEVs encompass vascular endothelial growth factors (VEGF) and additional angiogenic molecules that facilitate angiogenesis in tissues.115 Enhancing angiogenesis in the therapy of neurodegenerative illnesses might augment blood circulation in neural tissues, supplying essential nutrients and oxygen to neurons, thereby promoting their survival and functional recovery. In a model of neurodegenerative disease linked to ischemic brain injury, MSC- sEVs augmented the reparative potential of neural tissue by facilitating angiogenesis.116
Existing Clinical Applications of MSC-sEVs in Neurodegenerative Diseases
Clinical trials are underway utilizing MSC-sEVs to enhance cognitive performance in patients with AD within the context of neurodegenerative disorders. The method may involve diminishing neuroinflammation in the brain, eliminating Aβ deposits, and facilitating neuroregeneration.117 For example, a small preclinical trial observed a slowing of cognitive decline in AD model mice after administration of MSC-sEVs. This may be due to the fact that the route of administration allows MSC-sEVs to enter the brain directly and exert their neuroprotective and reparative effects.118 In Parkinson’s treatment, MSC-derived small extracellular vesicles can mitigate PD symptoms by safeguarding dopaminergic neurons from oxidative stress and death. Numerous preclinical investigations have shown that MSC- sEVs can transport neurotrophic substances, including brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF), to the substantia nigra region, thereby enhancing the survival of dopaminergic neurons and facilitating functional recovery.111 While extensive clinical applications remain constrained, these investigations offer innovative concepts for the future management of PD and are anticipated to enhance motor function in affected patients.
Future Prospects and Challenges
MSC-sEVs predominantly consist of a lipid bilayer encasing an interior bioactive material that resembles the makeup of human cells. This enables effective interaction with host cells upon entry into the human body, minimizing the risk of significant immunological rejection. The blood-brain barrier is a highly selective, semi-permeable membrane that obstructs the majority of external substances from accessing the brain. Nonetheless, MSC-derived sEVs can exploit their diminutive size to traverse the blood-brain barrier and access the brain via mechanisms such as cell-to-cell tight junctions or endocytosis. This property allows MSC-sEVs to directly target neurodegenerative lesions in the brain, offering an effective treatment for neurodegenerative illnesses such as Alzheimer’s and PD. MSC-sEVs can be engineered to function as a natural medicine delivery system. Pharmaceuticals, genetic material, or other bioactive agents for the management of neurodegenerative disorders can be encapsulated in sEVs for precise delivery and gradual release. For instance, specific neuroprotective genes or pharmaceuticals can be incorporated into MSC-derived small extracellular vesicles via genetic engineering methods, allowing for targeted delivery of these therapeutic agents to affected nerve cells, thereby enhancing treatment efficacy and minimizing adverse effects on healthy tissues.
The extraction and purification of sEVs presents a technical difficulty. In cell culture, sEVs are combined with many biological constituents (eg, cellular debris, protein aggregates, lipoprotein particles, etc.) and require separation by advanced procedures. Widely employed separation techniques including ultracentrifugation, ultrafiltration, and size exclusion chromatography; nevertheless, each technique possesses inherent limits. Divergences in the cellular origins of MSCs, the tissues of derivation, the culture conditions, and additional variables might result in significant variations in the composition and functionality of sEVs. There is an absence of standardized quality control measures and production specifications. While it is shown that MSC- sEVs possess many possible modes of action in the treatment of neurodegenerative disorders, these processes are intricate and numerous aspects remain unclear. The interaction between sEVs and neuronal cells is a complex process that encompasses various factors, including the recognition of receptors on sEVs by ligands on neuronal cells, the uptake mechanism of sEVs, the release of internal bioactivities, and the underlying mechanism of action. Furthermore, there may be synergistic or antagonistic interactions among the many bioactive compounds present in sEVs (eg, distinct miRNAs, proteins, etc)., and these interactions may vary across different neurodegenerative disease contexts. This intricacy hinders the precise modulation and optimization of therapeutic techniques for MSC- sEVs and restricts the accurate prediction of their therapeutic effects. While current studies indicate that MSC- sEVs possess a favorable short-term safety profile, the evaluation of their long-term safety remains insufficient. In the prolonged management of neurodegenerative illnesses, it is essential to evaluate whether sEVs elicit an immunological response, induce aberrant cell proliferation (eg, tumorigenesis), and pose potential detrimental consequences on other organ systems.
Discussion
MSC-EVs have demonstrated beneficial effects in the management of various prevalent neurodegenerative disorders. In AD, they can transport substances like nerve growth factor to facilitate neuronal regeneration, modulate the brain’s inflammatory response, and enhance cognitive function; in PD, they can assist in the repair and regeneration of dopaminergic neurons, regulate neuroinflammation, and ameliorate the patient’s motor symptoms; in HD, they can modulate neurotransmitter levels and inhibit neuroinflammation to mitigate associated symptoms; and in ALS, it can modulate the immune system and offer nutritional support to decelerate motor neuron degeneration and enhance the quality of patient survival. This comprehensively illustrates the therapeutic potential of MSC-EVs across several disease pathways, offering optimism for enhancing patients’ conditions and quality of life. Secondly, the method via which MSC-EVs exert a therapeutic effect is complex. It can serve as a drug delivery system to facilitate accurate medication administration and lesion treatment due to its excellent biocompatibility, inherent targeting capabilities, capacity to traverse the blood-brain barrier, and ability to modify its contents to improve delivery efficacy. Conversely, in the elimination of pathogenic proteins, it may function as a “transport carrier” for pertinent degradation enzymes or regulatory molecules, while also modulating the process of cellular autophagy. Additionally, it indirectly aids in the clearance of pathogenic proteins by regulating neuroinflammatory responses, thereby preserving the internal stability of the nervous system and decelerating disease progression. Simultaneously, its immunomodulatory mechanism can regulate immune cell equilibrium, suppress the neuroinflammatory response, and demonstrate efficacy in promoting neuronal growth and differentiation, as well as enhancing autophagy, collectively underpinning its role in the treatment of neurodegenerative diseases. Moreover, regarding the present state of application, while MSC-EVs have demonstrated efficacy in preclinical research and certain clinical trials, they continue to encounter numerous hurdles. The production process lacks standardized procedures, resulting in significant variability in the quality and activity of MSC-EVs from diverse sources and batches. Quality control is hindered by the absence of comprehensive and widely accepted testing and evaluation standards, complicating the accurate assessment of their quality, activity, and safety. Clinical trials are limited by small sample sizes, brief study durations, and restricted observational indices, which impede the precise evaluation of their efficacy and safety. Furthermore, ethical and regulatory considerations necessitate strict adherence to requirements regarding cell sourcing, patient informed consent, and procedural norms; any mismanagement in these areas may obstruct the advancement of their clinical application. Moreover, regarding ethics and laws, the origin of cells, patient informed permission, and the standardization of each process must adhere rigorously to the pertinent criteria; any inappropriate management may significantly impede the advancement of clinical application. MSC-EVs possess significant potential in the therapy of neurodegenerative illnesses, offering innovative strategies to address these challenging conditions. To attain widespread, safe, and effective clinical applications, comprehensive research is essential to address current challenges and enhance production, quality control, and clinical trials, thereby maximizing their therapeutic potential and benefiting patients with neurodegenerative diseases globally.
Data Sharing Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
We thank everyone who contributed to this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Municipal level scientific research plan project of Ganzhou Municipal Health Commission (2022-2-62), Science and Technology Plan of Jiangxi Provincial Administration of Traditional Chinese Medicine (2022B495).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Scheltens P, De Strooper B, Kivipelto M, et al. Alzheimer’s disease. Lancet. 2021;397(10284):1577–1590. doi:10.1016/S0140-6736(20)32205-4
2. Samii A, Nutt JG, Ransom BR. Parkinson’s disease. Lancet. 2004;363(9423):1783–1793. doi:10.1016/S0140-6736(04)16305-8
3. Walker FO. Huntington’s disease. Lancet. 2007;369(9557):218–228. doi:10.1016/S0140-6736(07)60111-1
4. Taylor JP, Brown RH, Cleveland DW. Decoding ALS: from genes to mechanism. Nature. 2016;539(7628):197–206. doi:10.1038/nature20413
5. Temple S. Advancing cell therapy for neurodegenerative diseases. Cell Stem Cell. 2023;30(5):512–529. doi:10.1016/j.stem.2023.03.017
6. Margiana R, Markov A, Zekiy AO, et al. Clinical application of mesenchymal stem cell in regenerative medicine: a narrative review. Stem Cell Res Ther. 2022;13(1):366. doi:10.1186/s13287-022-03054-0
7. Wang Y, Fang J, Liu B, Shao C, Shi Y. Reciprocal regulation of mesenchymal stem cells and immune responses. Cell Stem Cell. 2022;29(11):1515–1530. doi:10.1016/j.stem.2022.10.001
8. Fan XL, Zhang Y, Li X, Fu QL. Mechanisms underlying the protective effects of mesenchymal stem cell-based therapy. Cell Mol Life Sci. 2020;77(14):2771–2794. doi:10.1007/s00018-020-03454-6
9. Welsh JA, Goberdhan DCI, O’Driscoll L, et al. Minimal information for studies of extracellular vesicles (MISEV2023): from basic to advanced approaches. J of Extracellular Vesicle. 2024;13(2):e12404. doi:10.1002/jev2.12404
10. Dixson AC, Dawson TR, Di Vizio D, Weaver AM. Context-specific regulation of extracellular vesicle biogenesis and cargo selection. Nat Rev Mol Cell Biol. 2023;24(7):454–476. doi:10.1038/s41580-023-00576-0
11. Van Niel G, Carter DRF, Clayton A, Lambert DW, Raposo G, Vader P. Challenges and directions in studying cell–cell communication by extracellular vesicles. Nat Rev Mol Cell Biol. 2022;23(5):369–382. doi:10.1038/s41580-022-00460-3
12. Upadhya R, Zingg W, Shetty S, AK S. Astrocyte-derived extracellular vesicles: neuroreparative properties and role in the pathogenesis of neurodegenerative disorders. J Control Release. 2020;323:225–239. doi:10.1016/j.jconrel.2020.04.017
13. Gurunathan S, Kang MH, Qasim M, Khan K, Biogenesis KJH. Membrane trafficking, functions, and next generation nanotherapeutics medicine of extracellular vesicles. IJN. 2021;Volume 16:3357–3383. doi:10.2147/IJN.S310357
14. Iraci N, Leonardi T, Gessler F, Vega B, Pluchino S. Focus on extracellular vesicles: physiological role and signalling properties of extracellular membrane vesicles. IJMS. 2016;17(2):171. doi:10.3390/ijms17020171
15. Leidal AM, Debnath J. Unraveling the mechanisms that specify molecules for secretion in extracellular vesicles. Methods. 2020;177:15–26. doi:10.1016/j.ymeth.2020.01.008
16. Colombo M, Raposo G, Biogenesis TC. Secretion, and intercellular interactions of exosomes and other extracellular vesicles. Annu Rev Cell Dev Biol. 2014;30(1):255–289. doi:10.1146/annurev-cellbio-101512-122326
17. Raposo G, Stoorvogel W. Extracellular vesicles: exosomes, microvesicles, and friends. J Cell Biol. 2013;200(4):373–383. doi:10.1083/jcb.201211138
18. Li Y, Xia X, Wang Y, Zheng JC. Mitochondrial dysfunction in microglia: a novel perspective for pathogenesis of alzheimer’s disease. J Neuroinflammation. 2022;19(1):248. doi:10.1186/s12974-022-02613-9
19. Khan S, Barve KH, Kumar MS. Recent advancements in pathogenesis, diagnostics and treatment of alzheimer’s disease. CN. 2020;18(11):1106–1125. doi:10.2174/1570159X18666200528142429
20. Swerdlow RH, Burns JM, Khan SM. The Alzheimer’s disease mitochondrial cascade hypothesis: progress and perspectives. BBA. 2014;1842(8):1219–1231. doi:10.1016/j.bbadis.2013.09.010
21. Zenaro E, Piacentino G, Constantin G. The blood-brain barrier in alzheimer’s disease. Neurobiol Dis. 2017;107:41–56. doi:10.1016/j.nbd.2016.07.007
22. Yamazaki Y, Kanekiyo T. Blood-brain barrier dysfunction and the pathogenesis of alzheimer’s disease. IJMS. 2017;18(9):1965. doi:10.3390/ijms18091965
23. Hardy J, Selkoe DJ. The amyloid hypothesis of alzheimer’s disease: progress and problems on the road to therapeutics. Science. 2002;297(5580):353–356. doi:10.1126/science.1072994
24. Morris HR, Spillantini MG, Sue CM, Williams-Gray CH. The pathogenesis of Parkinson’s disease. Lancet. 2024;403(10423):293–304. doi:10.1016/S0140-6736(23)01478-2
25. Subramaniam SR, Chesselet MF. Mitochondrial dysfunction and oxidative stress in parkinson’s disease. Prog Neurobiol. 2013;106-107:17–32. doi:10.1016/j.pneurobio.2013.04.004
26. Spillantini MG, Schmidt ML, Lee VMY, Trojanowski JQ, Jakes R, Goedert M. α-synuclein in Lewy bodies. Nature. 1997;388(6645):839–840. doi:10.1038/42166
27. Tong H, Yang T, Xu S, et al. Huntington’s disease: complex pathogenesis and therapeutic strategies. IJMS. 2024;25(7):3845. doi:10.3390/ijms25073845
28. Ross CA, Tabrizi SJ. Huntington’s disease: from molecular pathogenesis to clinical treatment. Lancet Neurol. 2011;10(1):83–98. doi:10.1016/S1474-4422(10)70245-3
29. Jimenez-Sanchez M, Licitra F, Underwood BR, Rubinsztein DC. Huntington’s disease: mechanisms of pathogenesis and therapeutic strategies. Cold Spring Harb Perspect Med. 2017;7(7):a024240. doi:10.1101/cshperspect.a024240
30. Joshi DC, Chavan MB, Gurow K, Gupta M, Dhaliwal JS, Ming LC. The role of mitochondrial dysfunction in Huntington’s disease: implications for therapeutic targeting. Biomed Pharmacother. 2025;183:117827. doi:10.1016/j.biopha.2025.117827
31. Zaman M, Khan AN, Wahiduzzaman ZSM, Khan RH, Khan RH. Protein misfolding, aggregation and mechanism of amyloid cytotoxicity: an overview and therapeutic strategies to inhibit aggregation. Int J Biol Macromol. 2019;134:1022–1037. doi:10.1016/j.ijbiomac.2019.05.109
32. Feldman EL, Goutman SA, Petri S, et al. Amyotrophic lateral sclerosis. Lancet. 2022;400(10360):1363–1380. doi:10.1016/S0140-6736(22)01272-7
33. Hardiman O, Al-Chalabi A, Chio A, et al. Amyotrophic lateral sclerosis. Nat Rev Dis Primers. 2017;3(1):17071. doi:10.1038/nrdp.2017.71
34. Beers DR, Appel SH. Immune dysregulation in amyotrophic lateral sclerosis: mechanisms and emerging therapies. Lancet Neurol. 2019;18(2):211–220. doi:10.1016/S1474-4422(18)30394-6
35. Schou AS, Nielsen JE, Askeland A, Jørgensen MM. Extracellular vesicle-associated proteins as potential biomarkers. In: Advances in Clinical Chemistry. Vol. 99. Elsevier;2020:1–48. doi:10.1016/bs.acc.2020.02.011
36. Sjögren M, Andreasen N, Blennow K. Advances in the detection of alzheimer’s disease—use of cerebrospinal fluid biomarkers. Clin Chim Acta. 2003;332(1–2):1–10. doi:10.1016/S0009-8981(03)00121-9
37. Bravo-Miana RDC, Arizaga-Echebarria JK, Otaegui D. Central nervous system-derived extracellular vesicles: the next generation of neural circulating biomarkers? Transl Neurodegener. 2024;13(1):32. doi:10.1186/s40035-024-00418-9
38. Olsson B, Lautner R, Andreasson U, et al. CSF and blood biomarkers for the diagnosis of Alzheimer’s disease: a systematic review and meta-analysis. Lancet Neurol. 2016;15(7):673–684. doi:10.1016/S1474-4422(16)00070-3
39. Lim CZJ, Natalia A, Sundah NR, Shao H. Biomarker organization in circulating extracellular vesicles: new applications in detecting neurodegenerative diseases. Adv Biosys. 2020;4(12):1900309. doi:10.1002/adbi.201900309
40. Fiandaca MS, Kapogiannis D, Mapstone M, et al. Identification of preclinical alzheimer’s disease by a profile of pathogenic proteins in neurally derived blood exosomes: a case‐control study. Alzheimer’s Dementia. 2015;11(6):600. doi:10.1016/j.jalz.2014.06.008
41. You Y, Ikezu T. Emerging roles of extracellular vesicles in neurodegenerative disorders. Neurobiol Dis. 2019;130:104512. doi:10.1016/j.nbd.2019.104512
42. Parnetti L, Paciotti S, Farotti L, Bellomo G, Sepe FN, Eusebi P. Parkinson’s and Lewy body dementia CSF biomarkers. Clin Chim Acta. 2019;495:318–325. doi:10.1016/j.cca.2019.04.078
43. Mollenhauer B, Parnetti L, Rektorova I, et al. Biological confounders for the values of cerebrospinal fluid proteins in Parkinson’s disease and related disorders. J Neurochem. 2016;139(S1):290–317. doi:10.1111/jnc.13390
44. Atik A, Stewart T, Zhang J. Alpha‐synuclein as a biomarker for parkinson’s disease. Brain Pathol. 2016;26(3):410–418. doi:10.1111/bpa.12370
45. Simonsen AH, Kuiperij B, El-Agnaf OMA, et al. The utility of α-synuclein as biofluid marker in neurodegenerative diseases: a systematic review of the literature. Biomarkers Med. 2016;10(1):19–34. doi:10.2217/BMM.14.105
46. Chia SJ, Tan EK, Chao YX. Historical perspective: models of parkinson’s disease. IJMS. 2020;21(7):2464. doi:10.3390/ijms21072464
47. Shi M, Liu C, Cook TJ, et al. Plasma exosomal α-synuclein is likely CNS-derived and increased in parkinson’s disease. Acta Neuropathol. 2014;128(5):639–650. doi:10.1007/s00401-014-1314-y
48. Rani K, Mukherjee R, Singh E, et al. Neuronal exosomes in saliva of parkinson’s disease patients: a pilot study. Parkinsonism Relat Disord. 2019;67:21–23. doi:10.1016/j.parkreldis.2019.09.008
49. Reed ER, Latourelle JC, Bockholt JH, et al. MicroRNAs in CSF as prodromal biomarkers for Huntington disease in the PREDICT-HD study. Neurology. 2018;90(4). doi:10.1212/WNL.0000000000004844
50. Zsindely N, Nagy G, Siági F, Farkas A, Bodai L. Dysregulated miRNA and mRNA expression affect overlapping pathways in a Huntington’s disease model. IJMS. 2023;24(15):11942. doi:10.3390/ijms241511942
51. Didiot MC, Hall LM, Coles AH, et al. Exosome-mediated delivery of hydrophobically modified siRNA for huntingtin mRNA silencing. Mol Ther. 2016;24(10):1836–1847. doi:10.1038/mt.2016.126
52. Chatterjee M, Özdemir S, Fritz C, et al. Plasma extracellular vesicle tau and TDP-43 as diagnostic biomarkers in FTD and ALS. Nat Med. 2024;30(6):1771–1783. doi:10.1038/s41591-024-02937-4
53. Halliday GM, Kiernan MC, Kril JJ, et al. TDP-43 in the hypoglossal nucleus identifies amyotrophic lateral sclerosis in behavioral variant frontotemporal dementia. J Neurol Sci. 2016;366:197–201. doi:10.1016/j.jns.2016.05.005
54. Riku Y, Iwasaki Y, Ishigaki S, et al. Motor neuron TDP-43 proteinopathy in progressive supranuclear palsy and corticobasal degeneration. Brain. 2022;145(8):2769–2784. doi:10.1093/brain/awac091
55. Hornung S, Dutta S, Bitan G. CNS-derived blood exosomes as a promising source of biomarkers: opportunities and challenges. Front Mol Neurosci. 2020;13:38. doi:10.3389/fnmol.2020.00038
56. Raghunathan R, Turajane K, Wong LC. Biomarkers in neurodegenerative diseases: proteomics spotlight on ALS and parkinson’s disease. IJMS. 2022;23(16):9299. doi:10.3390/ijms23169299
57. Thompson AG, Gray E, Heman-Ackah SM, et al. Extracellular vesicles in neurodegenerative disease — pathogenesis to biomarkers. Nat Rev Neurol. 2016;12(6):346–357. doi:10.1038/nrneurol.2016.68
58. Mackenzie IR, Rademakers R, Neumann M. TDP-43 and FUS in amyotrophic lateral sclerosis and frontotemporal dementia. Lancet Neurol. 2010;9(10):995–1007. doi:10.1016/S1474-4422(10)70195-2
59. Nieland L, Mahjoum S, Grandell E, Breyne K, Breakefield XO. Engineered EVs designed to target diseases of the CNS. J Control Release. 2023;356:493–506. doi:10.1016/j.jconrel.2023.03.009
60. Vader P, Mol EA, Pasterkamp G, Schiffelers RM. Extracellular vesicles for drug delivery. Adv Drug Delivery Rev. 2016;106:148–156. doi:10.1016/j.addr.2016.02.006
61. Rufino-Ramos D, Albuquerque PR, Carmona V, Perfeito R, Nobre RJ, Pereira De Almeida L. Extracellular vesicles: novel promising delivery systems for therapy of brain diseases. J Control Release. 2017;262:247–258. doi:10.1016/j.jconrel.2017.07.001
62. Elsharkasy OM, Nordin JZ, Hagey DW, et al. Extracellular vesicles as drug delivery systems: why and how? Adv Drug Delivery Rev. 2020;159:332–343. doi:10.1016/j.addr.2020.04.004
63. Shahjin F, Chand S, Yelamanchili SV. Extracellular vesicles as drug delivery vehicles to the central nervous system. J Neuroimmune Pharmacol. 2020;15(3):443–458. doi:10.1007/s11481-019-09875-w
64. Pan R, Chen D, Hou L, Hu R, Jiao Z. Small extracellular vesicles: a novel drug delivery system for neurodegenerative disorders. Front Aging Neurosci. 2023;15:1184435. doi:10.3389/fnagi.2023.1184435
65. Banks WA, Sharma P, Bullock KM, KM H, Ludwig N, Whiteside TL. Transport of extracellular vesicles across the blood-brain barrier: brain pharmacokinetics and effects of inflammation. IJMS. 2020;21(12):4407. doi:10.3390/ijms21124407
66. Sil S, Dagur RS, Liao K, et al. Strategies for the use of extracellular vesicles for the delivery of therapeutics. J Neuroimmune Pharmacol. 2020;15(3):422–442. doi:10.1007/s11481-019-09873-y
67. Lu M, Xing H, Yang Z, et al. Recent advances on extracellular vesicles in therapeutic delivery: challenges, solutions, and opportunities. Eur J Pharm Biopharm. 2017;119:381–395. doi:10.1016/j.ejpb.2017.07.010
68. Huyan T, Li H, Peng H, et al. Extracellular vesicles – advanced nanocarriers in cancer therapy: progress and achievements. IJN. 2020;Volume 15:6485–6502. doi:10.2147/IJN.S238099
69. Yang X, Ma Y, Xie H, et al. Extracellular vesicles in the treatment of parkinson’s disease: a review. CMC. 2021;28(31):6375–6394. doi:10.2174/0929867328666210113170941
70. Liang Y, Iqbal Z, Lu J, et al. Cell-derived nanovesicle-mediated drug delivery to the brain: principles and strategies for vesicle engineering. Mol Ther. 2023;31(5):1207–1224. doi:10.1016/j.ymthe.2022.10.008
71. Muhammad SA. Are extracellular vesicles new hope in clinical drug delivery for neurological disorders? Neurochem Int. 2021;144:104955. doi:10.1016/j.neuint.2021.104955
72. Zhang L, Wu T, Shan Y, et al. Therapeutic reversal of Huntington’s disease by in vivo self-assembled siRNAs. Brain. 2021;144(11):3421–3435. doi:10.1093/brain/awab354
73. Das CK, Jena BC, Banerjee I, et al. Exosome as a novel shuttle for delivery of therapeutics across biological barriers. Mol Pharm. 2019;16(1):24–40. doi:10.1021/acs.molpharmaceut.8b00901
74. Gaurav I, Thakur A, Iyaswamy A, Wang X, Chen X, Yang Z. Factors affecting extracellular vesicles based drug delivery systems. Molecules. 2021;26(6):1544. doi:10.3390/molecules26061544
75. Wang L, Wang D, Ye Z, Xu J. Engineering extracellular vesicles as delivery systems in therapeutic applications. Adv Sci. 2023;10(17):2300552. doi:10.1002/advs.202300552
76. Nasiri Kenari A, Cheng L, Hill AF. Methods for loading therapeutics into extracellular vesicles and generating extracellular vesicles mimetic-nanovesicles. Methods. 2020;177:103–113. doi:10.1016/j.ymeth.2020.01.001
77. Quek C, Hill AF. The role of extracellular vesicles in neurodegenerative diseases. Biochem Biophys Res Commun. 2017;483(4):1178–1186. doi:10.1016/j.bbrc.2016.09.090
78. Shinohara M, Tachibana M, Kanekiyo T, Bu G. Role of LRP1 in the pathogenesis of Alzheimer’s disease: evidence from clinical and preclinical studies. J Lipid Res. 2017;58(7):1267–1281. doi:10.1194/jlr.R075796
79. Aprile FA, Källstig E, Limorenko G, Vendruscolo M, Ron D, Hansen C. The molecular chaperones DNAJB6 and Hsp70 cooperate to suppress α-synuclein aggregation. Sci Rep. 2017;7(1):9039. doi:10.1038/s41598-017-08324-z
80. Hurwitz SN, Conlon MM, Rider MA, Brownstein NC, Meckes DG. Nanoparticle analysis sheds budding insights into genetic drivers of extracellular vesicle biogenesis. J of Extracellular Vesicle. 2016;5(1):31295. doi:10.3402/jev.v5.31295
81. Vella LJ, Sharples RA, Nisbet RM, Cappai R, Hill AF. The role of exosomes in the processing of proteins associated with neurodegenerative diseases. Eur Biophys J. 2008;37(3):323–332. doi:10.1007/s00249-007-0246-z
82. Takeuchi T, Nagai Y. Emerging roles of extracellular vesicles in polyglutamine diseases: mutant protein transmission, therapeutic potential, and diagnostics. Neurochem Int. 2022;157:105357. doi:10.1016/j.neuint.2022.105357
83. Takeuchi T. Pathogenic and protective roles of extracellular vesicles in neurodegenerative diseases. J Biochem. 2021;169(2):181–186. doi:10.1093/jb/mvaa131
84. Mahmoudi F, Hanachi P, Montaseri A. Extracellular vesicles of immune cells; immunomodulatory impacts and therapeutic potentials. Clin Immunol. 2023;248:109237. doi:10.1016/j.clim.2023.109237
85. Kalluri R. The biology and function of extracellular vesicles in immune response and immunity. Immunity. 2024;57(8):1752–1768. doi:10.1016/j.immuni.2024.07.009
86. Gao C, Jiang J, Tan Y, Chen S. Microglia in neurodegenerative diseases: mechanism and potential therapeutic targets. Sig Transduct Target Ther. 2023;8(1):359. doi:10.1038/s41392-023-01588-0
87. Keshtkar S, Azarpira N, Ghahremani MH. Mesenchymal stem cell-derived extracellular vesicles: novel frontiers in regenerative medicine. Stem Cell Res Ther. 2018;9(1):63. doi:10.1186/s13287-018-0791-7
88. Ebrahim N, Al Saihati HA, Alali Z, et al. Exploring the molecular mechanisms of MSC-derived exosomes in alzheimer’s disease: autophagy, insulin and the PI3K/Akt/mTOR signaling pathway. Biomed Pharmacother. 2024;176:116836. doi:10.1016/j.biopha.2024.116836
89. Deng P, Anderson JD, Yu AS, Annett G, Fink KD, Nolta JA. Engineered BDNF producing cells as a potential treatment for neurologic disease. Expert opin biol ther. 2016;16(8):1025–1033. doi:10.1080/14712598.2016.1183641
90. Harrell CR, Volarevic A, Djonov V, Volarevic V. Mesenchymal stem cell-derived exosomes as new remedy for the treatment of neurocognitive disorders. IJMS. 2021;22(3):1433. doi:10.3390/ijms22031433
91. Ding M, Shen Y, Wang P, et al. Exosomes isolated from human umbilical cord mesenchymal stem cells alleviate neuroinflammation and reduce amyloid-beta deposition by modulating microglial activation in alzheimer’s disease. Neurochem Res. 2018;43(11):2165–2177. doi:10.1007/s11064-018-2641-5
92. Tashima T. Mesenchymal Stem Cell (MSC)-based drug delivery into the brain across the blood–brain barrier. Pharmaceutics. 2024;16(2):289. doi:10.3390/pharmaceutics16020289
93. Conaty P, Sherman LS, Naaldijk Y, Ulrich H, Stolzing A, Rameshwar P. Methods of mesenchymal stem cell homing to the blood–brain barrier. In: Singh SR, Rameshwar P, editors. Somatic Stem Cells. Vol 1842. Methods in Molecular Biology. New York: Springer; 2018:81–91. doi:10.1007/978-1-4939-8697-2_6
94. Zhang ZG, Buller B, Chopp M. Exosomes — beyond stem cells for restorative therapy in stroke and neurological injury. Nat Rev Neurol. 2019;15(4):193–203. doi:10.1038/s41582-018-0126-4
95. Ahad Mir P, Hussain MS, Ahmad Khanday M, Mohi-ud-din R, Pottoo FH, Hasssan Mir R. Immunomodulatory roles of mesenchymal stem cell-derived extracellular vesicles: a promising therapeutic approach for autoimmune diseases. CSCR. 2024;20. doi:10.2174/011574888X341781241216044130
96. Salami F, Tavassoli A, Mehrzad J, Parham A. Immunomodulatory effects of mesenchymal stem cells on leukocytes with emphasis on neutrophils. Immunobiology. 2018;223(12):786–791. doi:10.1016/j.imbio.2018.08.002
97. Harrell CR, Jankovic MG, Fellabaum C, et al. Molecular mechanisms responsible for anti-inflammatory and immunosuppressive effects of mesenchymal stem cell-derived factors. In: Pham PV, editor. Tissue Engineering and Regenerative Medicine. Vol 1084. Advances in Experimental Medicine and Biology. Springer International Publishing; 2018:187–206. doi:10.1007/5584_2018_306
98. Pan W, Li S, Li K, Zhou P. Mesenchymal stem cells and extracellular vesicles: therapeutic potential in organ transplantation. Stem Cells International. 2024;2024(1):2043550. doi:10.1155/2024/2043550
99. Tsuji K, Kitamura S, Wada J. Immunomodulatory and regenerative effects of mesenchymal stem cell-derived extracellular vesicles in renal diseases. IJMS. 2020;21(3):756. doi:10.3390/ijms21030756
100. Lai P, Weng J, Guo L, Chen X, Du X. Novel insights into MSC-EVs therapy for immune diseases. Biomark Res. 2019;7(1):6. doi:10.1186/s40364-019-0156-0
101. Harrell C, Fellabaum C, Jovicic N, Djonov V, Arsenijevic N, Volarevic V. Molecular mechanisms responsible for therapeutic potential of mesenchymal stem cell-derived secretome. Cells. 2019;8(5):467. doi:10.3390/cells8050467
102. Harrell CR, Jovicic N, Djonov V, Arsenijevic N, Volarevic V. Mesenchymal stem cell-derived exosomes and other extracellular vesicles as new remedies in the therapy of inflammatory diseases. Cells. 2019;8(12):1605. doi:10.3390/cells8121605
103. Matsuzaka Y, Yashiro R. Therapeutic strategy of mesenchymal-stem-cell-derived extracellular vesicles as regenerative medicine. IJMS. 2022;23(12):6480. doi:10.3390/ijms23126480
104. Gangadaran P, Rajendran RL, Lee HW, et al. Extracellular vesicles from mesenchymal stem cells activates VEGF receptors and accelerates recovery of hindlimb ischemia. J Control Release. 2017;264:112–126. doi:10.1016/j.jconrel.2017.08.022
105. Qian X, An N, Ren Y, Yang C, Zhang X, Li L. Immunosuppressive effects of mesenchymal stem cells-derived exosomes. Stem Cell Rev and Rep. 2021;17(2):411–427. doi:10.1007/s12015-020-10040-7
106. Xu Y, Li J, Qiu Y, et al. USC-derived small extracellular vesicles-functionalized scaffolds promote scarless vaginal defect repair via delivery of decorin and DUSP3 proteins. IJN. 2025;Volume 20:1615–1634. doi:10.2147/IJN.S499856
107. Zhou X, Deng X, Liu M, et al. Intranasal delivery of BDNF-loaded small extracellular vesicles for cerebral ischemia therapy. J Control Release. 2023;357:1–19. doi:10.1016/j.jconrel.2023.03.033
108. Palanisamy CP, Pei J, Alugoju P, et al. New strategies of neurodegenerative disease treatment with extracellular vesicles (EVs) derived from mesenchymal stem cells (MSCs). Theranostics. 2023;13(12):4138–4165. doi:10.7150/thno.83066
109. De Godoy MA, Saraiva LM, De Carvalho LRP, et al. Mesenchymal stem cells and cell-derived extracellular vesicles protect hippocampal neurons from oxidative stress and synapse damage induced by amyloid-β oligomers. J Biol Chem. 2018;293(6):1957–1975. doi:10.1074/jbc.M117.807180
110. Vilaça-Faria H, Salgado AJ, Teixeira FG. Mesenchymal stem cells-derived exosomes: a new possible therapeutic strategy for parkinson’s disease? Cells. 2019;8(2):118. doi:10.3390/cells8020118
111. Turano E, Scambi I, Virla F, Bonetti B, Mariotti R. Extracellular vesicles from mesenchymal stem cells: towards novel therapeutic strategies for neurodegenerative diseases. IJMS. 2023;24(3):2917. doi:10.3390/ijms24032917
112. Li K, Liu Z, Wu P, et al. Micro electrical fields induced MSC-sEVs attenuate neuronal cell apoptosis by activating autophagy via lncRNA MALAT1/miR-22-3p/SIRT1/AMPK axis in spinal cord injury. J Nanobiotechnol. 2023;21(1):451. doi:10.1186/s12951-023-02217-2
113. Liang Z, Yang Z, Xie H, et al. Small extracellular vesicles from hypoxia-preconditioned bone marrow mesenchymal stem cells attenuate spinal cord injury via miR-146a-5p-mediated regulation of macrophage polarization. Neural Regen Res. 2024;19(10):2259–2269. doi:10.4103/1673-5374.391194
114. Tan TT, Lai RC, Sim WK, Zhang B, Lim SK. Enhancing EV-cell communication through “External Modulation of Cell by EV” (EMCEV). Cytotherapy. 2025;27(1):1–6. doi:10.1016/j.jcyt.2024.07.014
115. Wang T, Li T, Niu X, et al. ADSC-derived exosomes attenuate myocardial infarction injury by promoting miR-205-mediated cardiac angiogenesis. Biol Direct. 2023;18(1):6. doi:10.1186/s13062-023-00361-1
116. Lu X, Lv C, Zhao Y, et al. TSG-6 released from adipose stem cells-derived small extracellular vesicle protects against spinal cord ischemia reperfusion injury by inhibiting endoplasmic reticulum stress. Stem Cell Res Ther. 2022;13(1):291. doi:10.1186/s13287-022-02963-4
117. Lin L, Huang L, Huang S, et al. MSC-derived extracellular vesicles alleviate NLRP3/GSDMD-mediated neuroinflammation in mouse model of sporadic alzheimer’s disease. Mol Neurobiol. 2024;61(8):5494–5509. doi:10.1007/s12035-024-03914-1
118. Cone AS, Yuan X, Sun L, et al. Mesenchymal stem cell-derived extracellular vesicles ameliorate Alzheimer’s disease-like phenotypes in a preclinical mouse model. Theranostics. 2021;11(17):8129–8142. doi:10.7150/thno.62069
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
VPS35-Retromer: Multifunctional Roles in Various Biological Processes – A Focus on Neurodegenerative Diseases and Cancer
Fan X, Xie Y, Cao S, Zhu L, Wang X
Journal of Inflammation Research 2025, 18:4665-4680
Published Date: 3 April 2025
Proteomic Characterization of Extracellular Vesicles from Human Neural Precursor Cells: A Promising Advanced Therapy for Neurodegenerative Diseases

Stricker PEF, de Oliveira NB, Mogharbel BF, Irioda AC, da Rosa NN, Lührs L, Saçaki CS, Munhoz da Rocha I, Alves LR, Poubel SB, Cardoso da Silva J, Carvalho PC, Fischer JSG, de Carvalho KAT
International Journal of Nanomedicine 2025, 20:6675-6699
Published Date: 25 May 2025