")
Back to Journals » International Journal of Nanomedicine » Volume 20
Nanomaterials: Promising Tools for the Diagnosis and Treatment of Myocardial Infarction
Authors Ge Y, Wu L, Mei S, Wu J
Received 10 October 2024
Accepted for publication 24 January 2025
Published 11 February 2025 Volume 2025:20 Pages 1747—1768
DOI https://doi.org/10.2147/IJN.S500146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Jie Huang
Yanmin Ge, Lincong Wu, Shuyang Mei, Junduo Wu
Department of Cardiology, The Second Hospital of Jilin University, Changchun, Jilin, 130000, People’s Republic of China
Correspondence: Junduo Wu, Email [email protected]
Abstract: Myocardial infarction (MI) is the leading cause of mortality from cardiovascular diseases. Rapid diagnosis and effective treatment are critical for improving patient prognosis. Although current diagnostic and therapeutic approaches have made significant progress, they still face challenges such as ischemia-reperfusion injury, microcirculatory disorders, adverse cardiac remodeling, and inflammatory responses. These issues highlight the urgent need for innovative solutions. Nanomaterials, with their diverse types, excellent physicochemical properties, biocompatibility, and targeting capabilities, offer promising potential in addressing these challenges. Advances in nanotechnology have increasingly drawn attention to the application of nanomaterials in both diagnosing and treating myocardial infarction. We summarize the pathophysiological mechanisms and staging of myocardial infarction. We systematically review the applications of nanomaterials in MI diagnosis, including the detection of biomarkers and imaging techniques, as well as in MI treatment, encompassing anti-inflammatory effects, antioxidant stress, inhibition of fibrosis, promotion of angiogenesis, and cardiac conduction repair. We analyze the existing challenges and provide insights into future research directions and potential solutions. Specifically, we discuss the need for rigorous safety assessments, long-term efficacy studies, and the development of robust strategies for translating laboratory findings into clinical practice. In conclusion, nanotechnology holds significant promise as a new strategy for diagnosing and treating myocardial infarction. Its potential to enhance clinical outcomes and revolutionize patient care makes it an exciting area of research with practical applications in real-world clinical settings.
Keywords: myocardial infarction, nanomaterials, nanoparticles, diagnosis and treatment
Introduction
The growing burden of cardiovascular disease (CVD) has become a major public health concern, with CVD-related deaths surpassing cancer fatalities among individuals under 85 years of age. Among CVDs, myocardial infarction (MI) is the primary cause of death.1,2 MI results from the irreversible necrosis of cardiac tissue due to ischemia following coronary artery occlusion. As a dead myocardium cannot regenerate, extensive myocardial damage can lead to cardiac remodeling, ultimately resulting in heart failure, arrhythmias, and even sudden cardiac death. Therefore, early diagnosis and timely therapeutic interventions are crucial for saving lives.3 The current clinical management of vascular diseases includes early diagnosis, reperfusion therapies, and pharmacological treatments such as percutaneous coronary intervention (PCI), thrombolytic therapy, and coronary artery bypass grafting (CABG), all aimed at rapidly restoring myocardial perfusion.4 While reperfusion can salvage myocardial cells, it may also induce further injury, affecting patient prognosis. Additionally, contrast agents and medications can have side effects on other organs, including bleeding caused by antiplatelet drugs and nephrotoxicity from contrast media.5 Given the complex pathophysiology, there are still limitations in current diagnostic and therapeutic methods, necessitating the development of faster and more efficient approaches to diagnose and treat MI.
Nanomaterials, defined as materials with dimensions at the nanoscale (typically 1–100 nm), include various forms such as carbon nanotubes, nanofibers, nanorods, nanoparticles (NPs), and thin films. These materials are widely used in MI treatment and diagnosis due to their unique physical and chemical properties, good biocompatibility, low toxicity, and minimal side effects.6 In diagnostics, nanomaterials, owing to their small size and excellent optical, electrochemical, and magnetic properties, can serve as biosensors and imaging agents, enabling accurate and sensitive detection of serum biomarkers and precise localization of infarcted areas.7,8 For therapeutic purposes, the high surface area-to-volume ratio and porous structure of nanomaterials allow for flexible drug loading and controlled release, facilitating targeted delivery and accumulation in lesion sites, thereby enhancing bioavailability.9,10 Moreover, nanomaterials exhibit anti-inflammatory and antioxidative properties, contributing to vascular regeneration, improved cardiac function, and enhanced cardiac repair.11,12
Despite the significant potential of nanomaterials in treating cardiovascular diseases, translating this potential into clinical applications remains a major challenge. Current comprehensive literature on the specific uses of nanomaterials for diagnosing and treating MI is limited. This review aims to fill this gap by systematically summarizing the latest advancements in nanomedicine for MI. For diagnosis, we explore how nanomaterials are used to detect cardiac biomarkers in blood and imaging techniques, significantly enhancing early detection sensitivity and specificity. For treatment, we categorize the applications of nanomaterials based on their mechanisms of action, including anti-inflammatory effects, antioxidant properties, promotion of angiogenesis, inhibition of fibrosis, and cardiac conduction repair. These approaches offer new avenues to improve patient outcomes in MI. We also analyze current challenges and propose practical solutions to facilitate the clinical application of nanotechnology in MI management (Figure 1).
 |
Figure 1 Nanomaterials play a significant role in the diagnosis and treatment of myocardial infarction (Created in Biorender. Ge, Y. (2025) https://BioRender.com/r52z718). Notes: Nanomaterials have emerged as a promising tool in the diagnosis and treatment of cardiovascular diseases, which are a leading cause of morbidity and mortality worldwide. These materials significantly lower the detection limits of cardiac biomarkers, enhance the sensitivity and resolution of imaging techniques, and enable the early identification of at-risk patients. In therapeutic applications, nanomaterials have been explored for their ability to mitigate inflammatory responses, oxidative stress, and fibrosis, while promoting angiogenesis and cardiac conduction repair. |
The Pathophysiology of Myocardial Infarction
Myocardial infarction (MI) typically occurs based on coronary atherosclerosis, with plaque rupture being a critical event leading to thrombosis and ultimately the occlusion of the coronary artery.13 The mechanisms of plaque formation and rupture involve multiple complex biological processes. Vascular cells are exposed to excessive low-density lipoprotein (LDL). This, along with endothelial activation and/or dysfunction, results in the internalization and accumulation of lipids within the intima. Prolonged exposure to pathogenic factors, including infections, chronic subclinical inflammation, hypertension, diabetes, stress, and smoking, can cause endothelial damage. Such damage leads to the overexpression of adhesion molecules, facilitating the recruitment of circulating immune cells, particularly monocytes. These monocytes adhere to the endothelium and differentiate into macrophages, which then ingest oxidized LDL (ox-LDL) and transform into foam cells, contributing to the development of a fibrous cap and a necrotic core. The progression of the necrotic core creates a hypoxic environment that promotes neovascularization, potentially leading to intraplaque hemorrhage and increased plaque instability. As atherosclerosis progresses, the number of vascular smooth muscle cells (VSMCs) decreases, and the apoptosis of foam cells releases active matrix metalloproteinases (MMPs). MMPs degrade the fibrous cap, increasing the likelihood of plaque rupture and subsequent thrombosis. Intra-arterial thrombosis may also be accompanied by arterial spasm, further contributing to luminal occlusion.14,15 Following an MI, many cardiomyocytes die due to severe impairment of coronary blood flow. Even after reperfusion, the myocardium may experience metabolic disturbances. Additionally, ischemia results in the accumulation of reactive oxygen species (ROS), Ca2+ overload in cardiomyocytes, and a series of inflammatory responses. These factors lead to mitochondrial dysfunction and exacerbate myocardial injury, potentially causing heart failure and arrhythmias.16 In October 2023, the Canadian Cardiovascular Society proposed a new acute staging system for myocardial infarction based on the severity of myocardial tissue injury.17 This staging includes four phases: The first phase involves myocardial edema with or without minor myocyte necrosis. The second phase features myocyte necrosis without microvascular obstruction. The third phase encompasses myocyte necrosis with microvascular obstruction. The fourth phase is characterized by hemorrhagic myocardial infarction. These stages, which are not mutually exclusive, collectively reflect the degree of tissue damage.18
Diagnosis
Cardiac Biomarkers
Serum biomarkers of myocardial injury are specific proteins or enzymes released into the bloodstream following damage to the heart muscle. These markers play a critical role in the diagnosis of myocardial infarction (MI). The evolution of these biomarkers has progressed from aspartate aminotransferase (AST) and lactate dehydrogenase (LDH), through myoglobin (Myo), creatine kinase (CK), and its isoenzyme CK-MB, to cardiac troponin (cTn).16 Currently, CK-MB, cTn, and Myo are collectively referred to as the “troika” for MI, and they are essential for diagnosing MI, assessing re-infarction or the extent of an infarct, and evaluating the severity and risk. Certain microRNAs (miRNAs) found in serum, which are specifically expressed in tissues, hold promise as novel indicators for diagnosing MI.19 The primary methods for detecting these biomarkers include enzyme-linked immunosorbent assay (ELISA) and polymerase chain reaction (PCR). However, these techniques suffer from long processing times, low precision, and high costs. Consequently, various diagnostic methods based on nanomaterials have been developed, enabling rapid and sensitive detection. We have summarized the research on nanomaterials for detecting cardiac biomarkers and listed their advantages (Table 1).
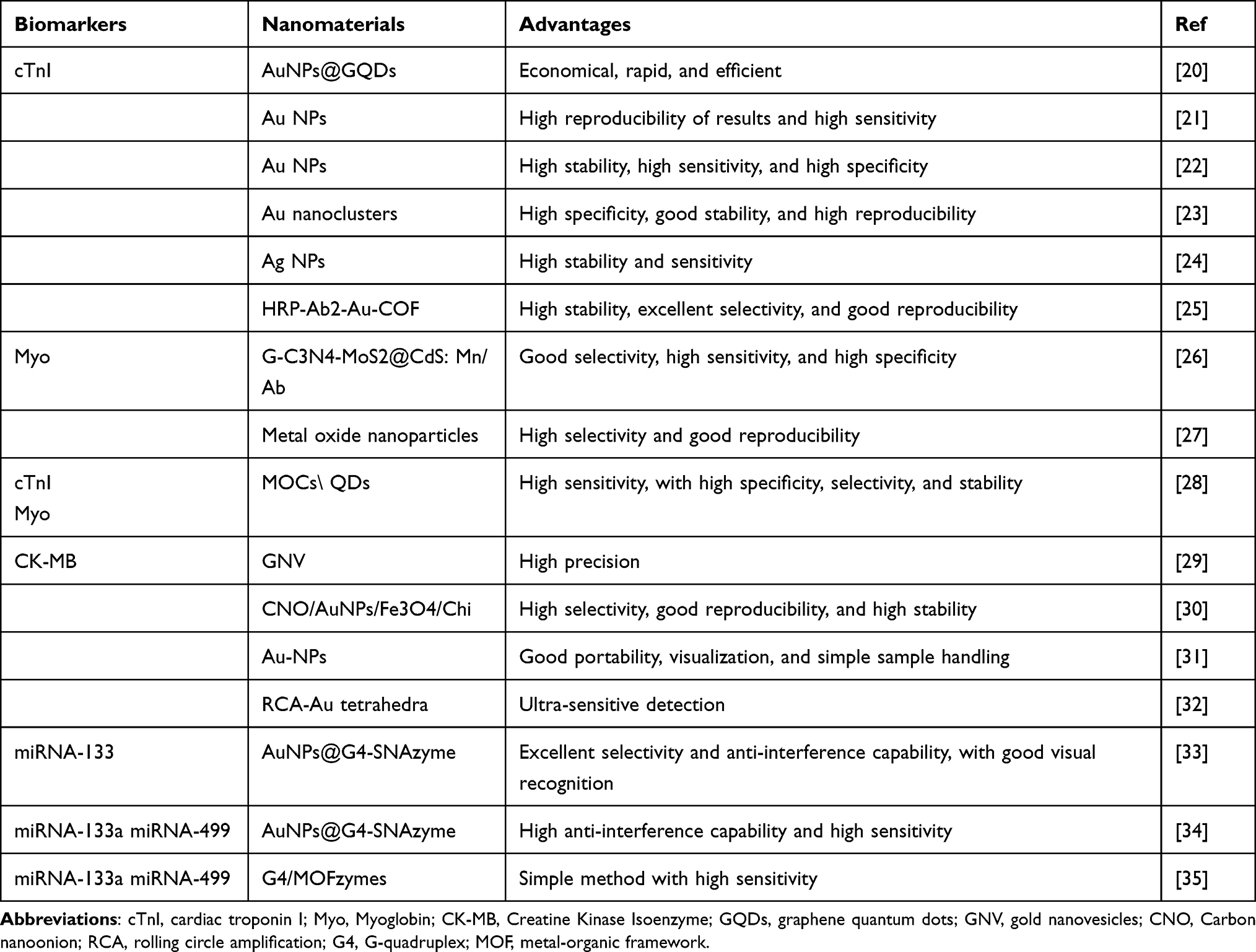 |
Table 1 Researchs on the Application of Nanomaterials in the Detection of MI Biomarkers |
Cardiac Troponin (cTn)
Cardiac troponins (cTns) are crucial for regulating the contraction of the cardiac sarcomere and consist of three subunits: troponin T (TnT), I (TnI), and C (TnC). Among these, cTnI is the most specific and sensitive biomarker for myocardial injury or necrosis and is considered the best indicator for diagnosing MI.36 After myocardial damage, blood levels of cTnI begin to rise within 3–4 hours and return to baseline over 6–8 days. Given that the upper reference limit of cTnI in the serum of healthy individuals is recommended to be as low as 0.03 ng/mL.37 It is crucial to develop biosensors with high sensitivity and specificity. One approach involves using nanomaterials to enhance the capture of cTnI.
Mansuriya et al coated graphene quantum dots (GQDs) and gold nanoparticles (AuNPs) onto a gold electrode via a droplet coating method, followed by immobilizing cTnI antibodies onto the GQD-AuNP composite, to fabricate an electrochemical (EC) immunosensor with a sensitivity of up to 6.81 μA cm−2 pg−1. However, this functionalized sensing system, which uses both antigens and antibodies, has some limitations, including low recovery rates, multi-step processing, extended research cycles, high antibody loading and manufacturing costs, and poor stability and performance at extreme temperatures.20 Recent studies have demonstrated that liquid crystals (LCs) offer precise, sensitive, and rapid detection with low interference, and their unique electro-optical properties can be utilized for molecular detection. Zapp et al developed an electrochemical immunosensor featuring columnar liquid crystal (LCol) and poly(allylamine hydrochloride) (PAH)-stabilized gold nanoparticles (AuNPs-PAH), characterized by enhanced cTnI capture through immobilized cTnI antibodies. The interaction between cTnI and the immunosensor showed a linear response from 0.01 to 0.3 ng/mL, with good reproducibility and high sensitivity.21 Additionally, Lopa et al deposited AuNPs conjugated with oligonucleotide aptamers onto titanium foil. Upon binding to cTnI, the negatively charged aptamer folds, inducing charge disturbance and redox reactions of potassium ferricyanide/ferrocyanide (K4[Fe(CN)6]/K3[Fe(CN)6]) in solution, with the potential change being inversely related to the cTnI concentration.22 This represents an improvement over traditional electroanalytical methods.
NPs can be conjugated with biomolecules that possess specific physical properties, such as through the hybridization chain reaction (HCR), to amplify signals and enhance sensitivity. Zhu et al developed a method for cTnI detection using gold nanoclusters (Au NCs) in conjunction with HCR for signal amplification. The Ab2-AuNP-T1 smart probe is constructed by conjugating a DNA initiator strand (T1) and antibody 2 (Ab2) to AuNPs. in the presence of cTnI, a sandwich immunocomplex forms, comprising cTnI, antibody 1 (Ab1), and the Ab2-AuNP-T1 probe. The initiator strand T1 from the Ab2-AuNP-T1 then triggers the opening of the hairpin DNA structures (H1 and H2) that are duplex-labeled on the Au NCs. This process initiates a series of hybridization events, resulting in the modification of a large number of Au NCs on the electrode surface. Finally, a strong electrochemiluminescence (ECL) signal is generated due to the reaction between the modified Au NCs and potassium persulfate (K2S2O8). Under optimal conditions, this method achieved a detection limit as low as 1.01 fg/mL, with high specificity, stability, and reproducibility.23 Signal enhancement can also be achieved by employing organic frameworks, which facilitate substrate and product diffusion, significantly improving reaction efficiency. Luminol is one of the most critical signal enhancers in ECL. Wang et al designed a metal-organic framework (MOF)-based nanoprobe composed of silver nanoparticles (AgNPs) and luminol, which increased the ECL efficiency of the luminol system by approximately 115 times. This nanoprobe exhibited an ultra-sensitive detection limit (LOD) for cTnI of 0.58 fg/mL.24 Additionally, Feng et al prepared a covalent organic framework (COF)--based probe for cTnI determination. The HRP-Ab2-Au-COF electrochemical signaling probe integrates target recognition and signal function amplification. The high porosity of the COF allows it to encapsulate a significant amount of horseradish peroxidase (HRP), thereby significantly amplifying the electrochemical reduction signal. Moreover, the COF demonstrates excellent biocompatibility, effectively maintaining enzyme activity and stability.25
Myoglobin (Myo)
Myo is present in both cardiac and skeletal muscles. Following a myocardial infarction (MI), Myo levels begin to rise within approximately 1–2 hours. When cardiomyocytes are damaged, Myo is released into the bloodstream, making it one of the earliest biomarkers for MI.38 Although the detection of Myo has some early warning value in MI, other non-cardiac-related traumas can also increase blood Myo levels, resulting in lower specificity.39 Ma et al used a photoelectrochemical (PEC) method to detect Myo. They prepared Mn-doped CdS nanocrystals sensitized 2D/2D heterostructure g-C3N4-MoS2, which served as the photoactive matrix for a PEC sensing platform. By using anti-myoglobin-labeled CuO conjugates for binding, this method could detect Myo in the range of 1 pg/mL to 50 ng/mL.26 Additionally, label-free manganese-doped titanium dioxide (TiO2) nanoparticle electrochemical sensors have shown the capability for quantitative Myo detection, with a limit of detection (LOD) of 0.22 ng/mL.27 Some studies have indicated that a dual-biomarker approach, such as simultaneously detecting Myo and cTnI, can enhance diagnostic value. In 2022, He et al constructed a dual-probe sensor. One probe consisted of mesoporous carbon nanospheres (MOC) combined with the luminescent material Ru(bpy)32+ and loaded with Myo aptamers on the surface. The other probe, composed of MoS2, generated an ECL signal in a single potential scan, enabling the simultaneous detection of Myo and cTnI. The intensity of the ECL signal reflected the concentrations of cTnI and Myo.28
Creatine Kinase Isoenzyme (CK-MB)
Creatine kinase (CK) is distributed throughout various organs and tissues and is an important enzyme in human energy metabolism. CK consists of M and B subunits and exists in four forms: CK-BB, CK-MB, CK-MM, and CK-MiMi. These isoenzymes are primarily found in skeletal muscle (MM), cardiac muscle (MB), brain (BB), and mitochondria (MiMi). After the onset of MI, CK-MB begins to rise within 2–4 hours, reaching its peak within 24 hours, and returns to normal levels within 48–72 hours. The degree of elevation is generally consistent with the size of the infarcted area.40 Pu et al improved the enzyme-free immunoassay (EFISA) by encapsulating three chromogenic reagents (phenolphthalein, methyl red, and bromothymol blue) in 3D gold nanovesicles (GNVs) as multiplexing nanoprobes. The loading and release of these reagents can be controlled by temperature, with a detection limit for CK-MB of 910 pg/mL.29 Adhikari et al developed a highly sensitive ECL immunosensor based on a series of nanocomposite-modified single-walled carbon nanotube (SWCNT) screen-printed electrodes. This sensor can detect CK-MB in the range of 10 ng/mL to 50 fg/mL.30 Chen et al designed a DNA hydrogel microfluidic chip-mediated point-of-care testing (POCT) platform for CK-MB detection. In the presence of CK-MB, the aptamer binds to CK-MB, leading to the dissociation of the hydrogel and the subsequent release of pre-captured AuNPs. The number of released AuNPs is proportional to the concentration of CK-MB, with a LOD as low as 0.027 nM.31 Zhang et al proposed a dual-sensitized smartphone colorimetric strategy for CK-MB detection, combining rolling circle amplification (RCA) coils and Au tetrahedra. This platform has a detection limit as low as 0.8 pM and performs well in spiked human serum samples.32
miRNAs
Currently, smartphone-based strategies are being more widely reported for the detection of clinical serum samples. Certain miRNAs have emerged as potential biomarkers for myocardial infarction (MI). For example, Sun et al developed a novel chemiluminescence (CL)-based G-quadruplex/hemin spherical nucleic acid enzyme (SNAzyme) sensing platform. The target miR-133 triggers catalytic hairpin assembly (CHA) amplification. The CHA products are captured on a 96-well plate, and the chemiluminescent signals are recorded and analyzed using a smartphone. This approach achieved the visualization of AMI-related miRNAs in patient serum for the first time.33 Lin et al also reported that the SNAzyme platform, when used with a smartphone, can detect CL-based AMI-related miRNA-133a and miRNA-499. By targeting miRNA-triggered DNAzyme cleavage on Au-NPs, they generated G-quadruplex/hemin-mimicking HRP-like SNAzymes. This enabled the detection of miRNAs at concentrations as low as 10 fM in human serum.34 In another recent development, Lan et al synthesized a hemin-bridged MOF as a functional interface to enhance the payload and catalysis of G4-DNAzymes. Compared to previous smartphone-based counterparts, this new and simple method improved the sensitivity of CL imaging by six orders of magnitude and extended the duration by approximately 50 times.35 This biosensor provides a faster and more efficient solution to meet the growing demand for AMI diagnosis.
Recent studies demonstrate that nanomaterials significantly enhance traditional detection methods. Specifically, they increase the capture efficiency of cardiac biomarkers and exhibit a signal amplification effect, resulting in ultra-low detection limits. These improvements offer advantages such as high efficiency, accuracy, sensitivity, and specificity. As nanotechnology advances, future research can focus on developing multiplexed biosensors for rapid and convenient detection of multiple biomarkers.
Imaging
Magnetic resonance imaging (MRI), computed tomography (CT), ultrasound (US) imaging, and photoacoustic (PA) imaging are commonly used diagnostic techniques in clinical practice. However, these techniques still have certain limitations. Nanoparticles (NPs) exhibit excellent contrast and optical properties, which can significantly enhance imaging sensitivity and resolution, facilitating the early and rapid localization of infarcted areas. For this, we have summarized the research on nanomaterials in myocardial infarction imaging (Table 2).
 |
Table 2 Researchs on the Application of Nanomaterials in MI Imaging |
MRI
MRI is characterized by its non-radiative, multi-parametric, multi-planar, and multi-sequence imaging capabilities, along with high soft tissue resolution. It can accurately identify at-risk and viable myocardium, assess the reversibility of myocardial injury, and precisely measure the extent and size of infarction, making it the gold standard for non-invasive imaging of MI.49 Li et al developed gadolinium-doped carbon dots (Gd-CDs) as MRI contrast agents. Gd-CDs possess strong fluorescence, good stability, and high biocompatibility. Additionally, Gd-CDs preferentially accumulate in ischemic cardiac tissue through leaky endothelium, without entering normal myocardial cells. This enables targeted imaging of infarcted regions during the acute phase of MI.41 Recently, a research team prepared PEG-QK-modified gadolinium-doped carbon dots (GCD-PEG-QK). Vascular endothelial growth factor (VEGF) receptors are overexpressed in infarcted hearts and specifically bind to the VEGF-mimicking peptide QK. In an I/R mouse model, mice injected with GCD-PEG-QK showed significant signal enhancement in the infarcted area. This study was the first to use QK peptide-conjugated nanoprobes as MRI contrast agents for diagnosing myocardial infarction. Furthermore, in vivo studies demonstrated that GCD-PEG-QK enhanced angiogenic repair and the protective effects of the QK peptide on I/R-induced myocardial injury by targeting infarcted myocardium and delivering the QK peptide.42 PH-responsive MnO nanocomposites (MnO2@BSA) have also been used for MRI in MI. It was found that MnO2@BSA highly accumulates in the MI region and is rapidly metabolized from the body after systemic injection. With high-contrast enhancement, it accurately imaged MI in a rabbit model, demonstrating excellent diagnostic performance.43
CT
CT provides rapid image acquisition, high-resolution details, and the ability to visualize both bone and soft tissues. It can display coronary artery imaging and is valuable for diagnosing MI.50 Ruptured plaques are characterized by the presence of numerous macrophages. N1177, composed of iodinated nanoparticles, is selectively engulfed by macrophages. The density of ruptured atherosclerotic plaques significantly increases 2 hours after intravenous injection of N1177, making it useful for early detection in MI patients.44 Compared to currently used iodine compounds, AuNPs provide better CT contrast and extended circulation time, allowing for longer imaging durations. This is beneficial for vascular and microvascular system imaging, where AuNPs can clearly delineate blood vessels.51 Kee et al developed AuNPs integrated with collagen-binding adhesion protein 35 (CNA35), functionalized to target collagen within myocardial infarct scars in rodents. These AuNPs enable expanded blood pool enhancement for coronary vascular imaging. Six hours after intravenous administration, AuNP signals were still detectable in the blood, significantly higher than the half-life of iodine-based drugs.45
Ultrasound and Photoacoustic Imaging
US is a medical imaging technique that provides real-time images and is considered safe and convenient. US is particularly suitable for integration with nanoscale platforms due to its unique imaging capabilities.52 Li et al designed hollow nano-silica structures (HNSS) with an internal core made of perfluorocarbon to generate ultrasound contrast. Additionally, they were conjugated with antibodies targeting hs-cTnI, a well-known marker of myocardial injury, allowing for the detection of MI in rats via US after intravenous injection of HNSS.46 PA is an emerging biomedical imaging method that can display lesion locations through the photoacoustic effect, offering non-invasive, high optical contrast, and other advantages.53 Zhang used non-invasive fibrin-targeting nanoparticles, which accumulated in the injured area in an I/R model. The PA signals from the infarcted area could then be detected using the ultrasonic transducer of a photoacoustic imaging system.47 Zhao’s team synthesized ultra-small Bi2S3-NPs using self-assembled single-stranded DNA as a template and used them as imaging probes in myocardial infarction. They successfully imaged myocardial infarction, demonstrating excellent biocompatibility, stability, and high photoacoustic imaging performance.48
Our review highlights the application of nanomaterials in non-invasive imaging. Nanomaterials enhance signal intensity and detection sensitivity, offering excellent targeting and spatial resolution. Each imaging modality has its unique advantages and plays a crucial role in MI screening and diagnosis. Future research will focus on multimodal imaging, integrating multiple imaging modalities to provide comprehensive diagnostic information.
Treatment
The complexity of cardiac repair, involving multiple processes such as inflammatory infiltration, oxidative stress, angiogenesis, and fibrosis, has led to the emergence of nanomaterials as novel therapeutic strategies for MI. These strategies aim to inhibit inflammation, reduce reactive oxygen species (ROS), suppress fibrosis, promote angiogenesis, and restore electrical conduction. The following section summarizes representative studies on the use of nanomaterials in MI treatment. We have listed the roles that nanomaterials play in the treatment of MI, along with their advantages (Table 3).
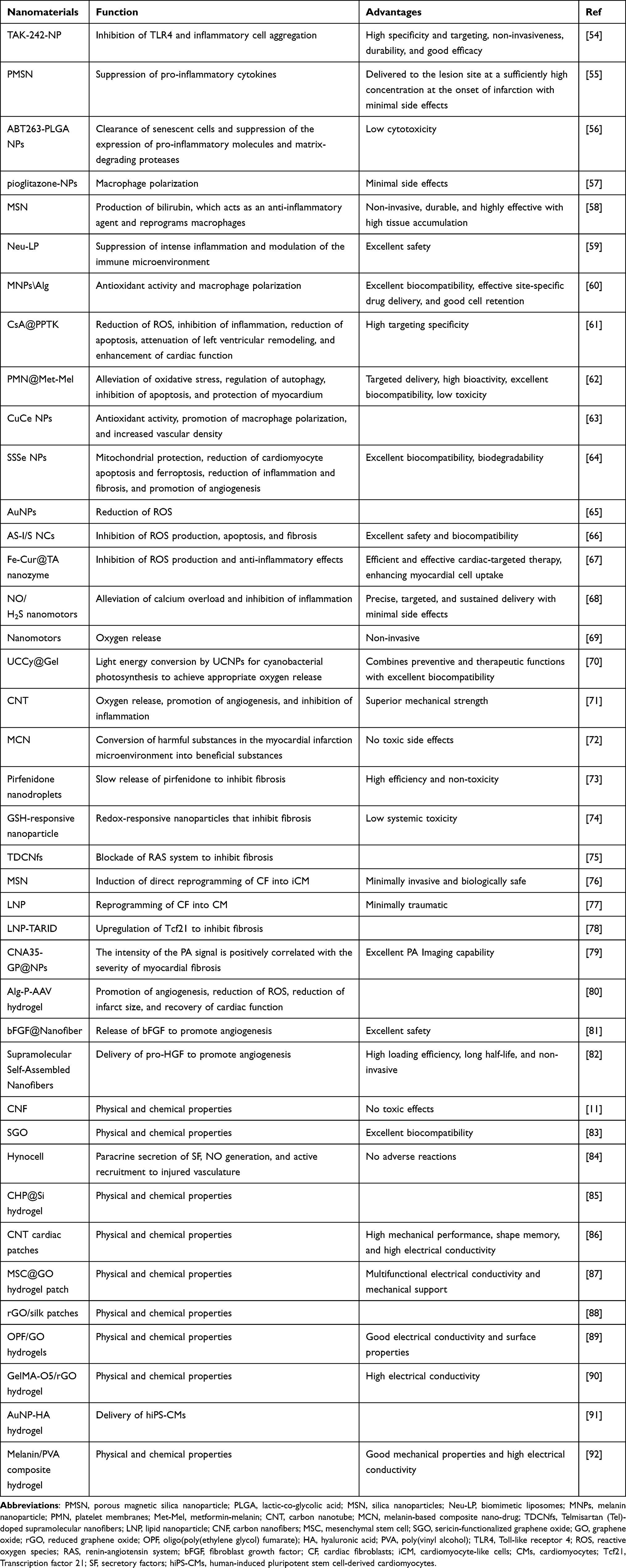 |
Table 3 Researchs on the Application of Nanomaterials in the Treatment of MI |
Anti-Inflammatory Effects
Macrophages play a crucial role in regulating immune responses during different stages of MI, including the inflammatory, proliferative (anti-inflammatory), and stabilization phases. In the early stages of MI, macrophages are rapidly recruited to the infarcted area, where pro-inflammatory M1 macrophages secrete pro-inflammatory cytokines and proteases, effectively clearing damaged cells from the infarcted region. Subsequently, anti-inflammatory M2 macrophages become more prevalent in the later stages of MI, secreting anti-inflammatory cytokines that promote healing and remodeling of cardiac tissue.93
However, excessive activation of M1 macrophages can lead to cardiomyocyte death, inhibit myocardial regeneration, and enhance scar formation, resulting in an expanded infarct area.94 Fujiwara et al investigated TAK-242-loaded poly-(lactic-co-glycolic acid) (PLGA) NPs. TAK-242, a chemical inhibitor of Toll-like receptor 4 (TLR4), was administered intravenously in a rat model of MI with reperfusion. This treatment inhibited the recruitment of Ly-6 high monocytes to the heart, reduced circulating HMGB1, NF-κB activation, and the expression of inflammatory factors, thereby decreasing the infarct size.54 Sulforaphane (SFN) is widely used in the treatment of MI due to its cardioprotective effects and low toxicity. Zhang et al synthesized porous magnetic silica nanoparticles (PMSNs) and loaded them with SFN. PMSNs delivered SFN to the infarcted area, where the drug upregulated HSP70 via the Nrf2/HSF1 pathway, exerting a cardioprotective effect against myocardial injury. This reduced the levels of IL-1β, IL-6, and TNF-α, improving cardiac function and cell survival without adverse effects.55 Li et al demonstrated that biodegradable PLGA NPs delivering an anti-senescence drug (ABT263-PLGA) successfully eliminated senescent cells in the hearts of ischemia/reperfusion injury(IRI) rats. This treatment significantly reduced the activation of JNK and NF-κB signaling pathways associated with M1 polarization, promoting the transition from the inflammatory phase to the reparative phase and mitigating adverse remodeling.56
M2 macrophages possess anti-inflammatory properties, suppressing fibrosis, inducing cell proliferation, and promoting angiogenesis.95 Therefore, promoting the conversion to M2 macrophages can also inhibit inflammation. Tokutome et al designed pioglitazone-loaded poly(lactic-co-glycolic acid) NPs. In a mouse model of MI, intravenous injection of pioglitazone-NPs reduced macrophage recruitment and polarized macrophages toward the healing M2 phenotype, significantly lowering mortality after MI.57 Neutrophil apoptotic body membranes combined with 5-aminolevulinic acid hexyl ester (HAL)-loaded mesoporous silica nanoparticles (MSN) were used to prepare neutrophil apoptotic bodies (eNABs). eNABs actively target macrophages, and the encapsulated HAL initiates the heme biosynthesis pathway, releasing anti-inflammatory bilirubin upon intracellular release. This further promotes macrophage reprogramming and enhances the anti-inflammatory effect. In a rat model of MI, intravenous injection of these nanoparticles promoted M2 macrophage conversion and improved cardiac function.58 Chen et al prepared biomimetic liposomes (Neu-LPs) by fusing liposomes (LPs) with neutrophil membranes. Due to their abundant chemokine and cytokine membrane receptors, Neu-LPs targeted the infarcted heart, neutralizing pro-inflammatory cytokines, inhibiting M1 macrophage activity, and promoting the transition of macrophages to the M2 phenotype, thereby promoting angiogenesis through immunomodulation.59 Zhou et al constructed melanin nanoparticle (MNP)/alginate (Alg) hydrogels using Ca2+ crosslinking. The hydrogels promoted the conversion of M1 macrophages to M2 macrophages, reducing CD86 signaling in mononuclear macrophages and increasing CD206 signaling. In a rat model of MI, the hydrogels cleared ROS, and the oxygen produced by the reaction with ROS promoted macrophage polarization toward the M2 phenotype, significantly enhancing cardiomyocyte survival.60
Studies have shown that nanomaterials target macrophages, inhibiting the accumulation of M1 macrophages and promoting their conversion to M2 macrophages. This shift reduces the production of pro-inflammatory factors and mitigates myocardial cell damage. Future research can explore key regulatory nodes to promote the M1-to-M2 transition, balance the populations of these macrophage subtypes, and enhance myocardial cell repair.
Anti-ROS
Early coronary reperfusion is one of the most effective strategies for treating myocardial infarction (MI). Although reperfusion therapy can restore blood flow and oxygen supply, it may also result in myocardial ischemia/reperfusion injury (IRI) during the treatment process. It is well established that ROS is a central factor in IRI.96 Excessive production of ROS is the primary cause of tissue damage mediated by myocardial IRI. During reperfusion, cardiomyocytes experience a burst release of ROS and Ca2+ overload, leading to excessive opening of the mitochondrial permeability transition pore (mPTP). The over-opening of mPTP further induces the release of more ROS from mitochondria and promotes cardiomyocyte apoptosis.97 Therefore, anti-ROS therapy can effectively protect hypoxic and ischemic cells and reduce the infarct size of the myocardium.98 The application of nanomaterials in anti-ROS therapy for IRI mainly involves two aspects: scavenging excess ROS and inhibiting ROS generation.
Timely elimination of ROS can effectively alleviate inflammation, tissue damage, and cardiomyocyte death. A team developed regulatory T cell (Treg) biomimetic nanoparticles (CsA@PPTK) that release CsA in a ROS-responsive manner. This strongly blocks the over-opening of mPTP, clears ROS, and, through the reprogramming of Treg generation, increases the ratio of M2 macrophages to M1 macrophages and the oxidative microenvironment, thereby reducing myocardial fibrosis and left ventricular remodeling.61 Melanin plays a crucial role in eliminating ROS and alleviating oxidative stress. Sun et al developed biomimetic nanoparticles (PMN@Met-Mel) that target damaged myocardium. In a mouse model of MI, this complex reduced oxidative stress, activated the AMP-activated protein kinase (AMPK) signaling pathway, and regulated the expression of downstream autophagic proteins LC3B and p62. This enhanced cellular autophagy, maintained mitochondrial homeostasis and function, and protected cardiomyocytes from ischemic injury.62 Copper-deposited cerium oxide nanoparticles (CuCe NPs) have been found to release copper, which buffers glutathione depletion and upregulates superoxide dismutase 1 (SOD1). This promotes anti-inflammatory and M2 polarization of macrophages by modulating the signal transducer and activator of transcription 1 and 6 (STAT1 and STAT6). Additionally, the therapeutic effects of CuCe NPs were confirmed in ischemic vascular diseases, such as hindlimb ischemia and MI in mouse models. Copper deposition increased perfusion and reduced tissue damage.63 Sun et al embedded self-sustaining selenium into nanoparticles. These nanoparticles effectively cleared the burst of ROS in the early stages of MI in mice and converted to glutathione peroxidase 4 (GPx4) for continuous on-demand clearance during inflammation and fibrosis. This promoted the repair of the endogenous antioxidant system, protected mitochondria, reduced myocardial apoptosis and ferroptosis, inhibited inflammation and fibrosis, and ultimately promoted angiogenesis in MI tissues.64 Shilo et al incorporated AuNPs into hydrogels containing extracellular matrix (ECM) as a scaffold material for cardiac cells. The particles on collagen fibers within the hydrogel promote rapid intercellular electrical signal transmission, enabling functional assembly of cardiac implants. In a mouse ischemia/reperfusion model, the composite hydrogel showed ROS absorption both in vitro and in vivo. The reduction in ROS levels maintained the morphology and integrity of cardiac tissue and vasculature, reduced scar size and inflammatory response, and significantly prevented the deterioration of cardiac function.65
Mitochondria, as the core organelles for ROS production, are key targets for inhibiting ROS generation.66 Mitochondrial-targeted selenium-gold nanocomposites used for photoacoustic (PA) imaging-guided IRI therapy can inhibit ROS-mediated oxidative damage and regulate mitogen-activated protein kinases (MAPKs) and phosphatidylinositol 3-kinase (PI3K)/AKT pathways by suppressing the depletion of mitochondrial membrane potential and restoring ATP synthase activity. This attenuates IRI in rats.99 Natural polyphenols, such as curcumin, play a role in inhibiting ROS production. Nanozymes, which combine the advantages of biological enzymes and nanomaterials, including higher catalytic activity and stability than natural enzymes, have shown promise. Liu et al utilized the strong coordination between Fe3+ and the anti-inflammatory drug curcumin (Cur) and modified the nanozyme with tannic acid (TA) to synthesize a novel drug-based metal nanozyme, Fe-Cur@TA. This nanozyme directly targets the inflammatory radical cycle, blocking the vicious cycle of inflammatory radicals, reducing the infiltration of acute immune cells into the infarct site, promoting M2-like phenotype polarization of macrophages, inhibiting the secretion of inflammatory cytokines, and enhancing the anti-inflammatory ability of Cur. In mouse and preclinical beagle dog MI models, Fe-Cur@TA provided effective cardioprotection, improved cardiac function, and mitigated adverse cardiac remodeling.67 Inhibiting calcium overload provides another approach to suppress ROS generation. Recombinant granulocyte colony-stimulating factor (G-CSF) has a direct reparative effect on injured cardiomyocytes, but its efficacy is limited due to poor cardiac targeting. Li et al recently proposed the concept of “nano-motors”, where the production of nitric oxide (NO) is considered the driving force for enhancing the targeting, retention, and penetration of nanoparticles into IRI. NO/H2S nano-motors can highly express ROS/inducible nitric oxide synthase (iNOS) at the IRI site, effectively delivering G-CSF to the IRI site. Superoxide dismutase, covalently bound to the outermost layer, reduces ROS at the IRI site. The synergistic effect of NO and H2S effectively regulates the IRI microenvironment, avoiding the toxicity caused by high concentrations of a single gas while inhibiting inflammation and relieving calcium overload, thus promoting the cardioprotective effects of G-CSF.68
Rapid and sustained oxygen delivery after MI can rescue cardiac cells and restore heart function. Guan et al designed oxygen-releasing nanoparticles that, when injected either before or after MI, promote oxygen delivery. Exogenous oxygen enhances the survival of hypoxic myocardial cells by increasing intracellular oxygen levels and promoting ATP synthesis. Additionally, these nanoparticles stimulated endothelial tube formation, promoted angiogenesis, and inhibited cardiac fibrosis. The released oxygen reduced tissue inflammation by lowering the density of pro-inflammatory macrophages and oxidative stress without generating excessive ROS that could damage the tissue.69 Liu et al developed a nanocarrier loaded with cyanobacteria and encapsulated it in a hydrogel. In a mouse model of MI, the nanocarrier released photosynthetic oxygen under 980 nm near-infrared (NIR) irradiation, thereby inhibiting M1 polarization of macrophages and downregulating the expression of pro-inflammatory cytokines such as IL-6 and TNF-α. When the hydrogel was implanted into the apex of healthy mice and kept in the dark for 2 to 4 hours, the engineered cyanobacterial system consumed oxygen through respiration, creating a controlled local hypoxic microenvironment. This upregulated heat shock protein 70 (HSP70) and inhibited the expression of the apoptotic protein caspase-3, thereby preventing myocardial infarction.70 The integration of nanomaterials with 3D printing platforms to enhance the acceptability of implants and reconstruct infarcted hearts is a promising research direction. Mehrotra et al used conductive bioink containing carbon nanotubes (CNTs) to bioprint functional 3D vascularized anisotropic cardiac structures. The study found that, in addition to releasing oxygen and modulating macrophage phenotypes, these structures have other potential advantages.71 Liu et al designed a melanin-based composite nano-drug (MCN) to reprogram the microenvironment in a mouse model of MI. The MCN effectively converts harmful substances (such as H+ and ROS) into beneficial states (O2 and H2O). This conversion reduces mitochondrial ROS levels, protects mitochondrial integrity and function, significantly inhibits cardiomyocyte apoptosis, and greatly reduces inflammation and fibrosis in the infarcted myocardial tissue.72
Studies have shown that nanomaterials can mitigate oxidative stress through multiple mechanisms, such as scavenging ROS and inhibiting ROS generation pathways. By promoting oxygen generation, nanomaterials improve the cardiac microenvironment, providing an effective strategy for treating IRI. ROS is known to play a critical role in the development of hypertension, diabetes, and hypercholesterolemia. Future approaches using nanomaterials loaded with drugs targeting specific antioxidant pathways may offer additive or synergistic protective effects, further enhancing cardioprotection.100
Inhibition of Fibrosis
Following MI, a series of growth factors and cytokines activate cardiac fibroblasts(CFs), leading to their transformation into myofibroblasts and the development of pathological myocardial fibrosis. Pathological myocardial fibrosis results in ECM deposition, decreased ventricular compliance, and contractile and diastolic dysfunction, which are risk factors for sudden death and chronic heart failure. Transforming growth factor-β (TGF-β) induces the transcription of alpha-smooth muscle actin (α-SMA) by activating the Smad3 signaling pathway. Inhibiting the TGF-β pathway can effectively alleviate fibrosis.101–103 Copper inhibits fibroblasts, thereby inhibiting fibrosis and promoting recovery of cardiac function.104 The antifibrotic drug pirfenidone (PFD) is a TGF-β1 inhibitor. Using acellular peritoneal matrix-loaded PFD nanodroplets extends the total release duration of PFD, thereby reducing cardiac fibrosis. Additionally, PFD inhibits the transformation of CFs into myofibroblasts and reduces the synthesis and secretion of type I and III collagen by these cells.73 Ji et al developed a glutathione (GSH)--responsive nanoparticle platform for the specific delivery of highly effective antifibrotic drugs to activated CFs in the infarcted region after MI. This targeted delivery system enhances the therapeutic efficacy of antifibrotic drugs while minimizing systemic toxicity, providing a promising approach for the intervention of cardiac fibrosis.74 After MI, cardiac overload leads to chamber dilation and increased wall stress, subsequently activating the renin-angiotensin-aldosterone system (RAAS) and inflammatory responses, which promote the formation and excessive fibrosis of myofibroblasts.105 Targeting renin-angiotensin system(RAS) represents a promising therapeutic approach against fibrosis. Telmisartan (Tel)-doped supramolecular nanofibers (TDCNfs) have good targeting and downstream pathway mediation, providing significant protection to damaged myocardium. By reducing apoptosis and inflammation, enhancing antifibrotic potential, and limiting toxicity, TDCNfs show superior potential in combating adverse cardiac outcomes following MI.75
Nanoparticle-mediated non-coding RNAs also show considerable potential in treating fibrosis. MicroRNA-mediated cardiac reprogramming can directly convert fibroblasts into induced cardiomyocytes, showing promise in cardiac therapy.106 Researchers have developed FH peptide-labeled mesoporous silica nanoparticles (MSNs) that target damaged myocardial tissue. These nanoparticles are then encapsulated with neutrophil-mimicking membranes, creating a virus-mimicking system that carries microRNAs. This system can directly convert fibroblasts into induced cardiomyocytes, reducing fibrosis.76 Intravenous injection of lipid nanoparticles (LNPs) containing modified mRNA (modRNA) delivered to damaged myocardium can induce the direct conversion of fibroblasts into cardiomyocytes and reduce myocardial fibrosis.77 Transcription factor 21 (Tcf21) is recognized as a marker of CFs because it is crucial for fibroblast development during cardiac development.107 Long non-coding RNA-TARID (Tcf21 antisense RNA-induced demethylation LncRNA) activates Tcf21 expression by inducing demethylation of its promoter.108 Zhu et al demonstrated that lncRNA-TARID-loaded LNPs upregulated Tcf21 and inhibited its profibrotic differentiation in mouse and pig models of myocardial infarction.78 Recently, a team developed a collagen-targeted multimodal imaging nanoplatform, CNA35-GP@NPs, which includes LNPs, encapsulated gold nanorods (GNRs), and perfluoropentane (PFP). In a rat model of myocardial infarction, CNA35-GNR/PFP@NPs achieved PA, US, and enhanced CT imaging of fibrotic myocardium. The PA signal intensity was positively correlated with the severity of myocardial fibrosis, making this a promising method for detecting and treating post-MI fibrosis.79
In summary, nanomaterials enhance drug efficacy by loading antifibrotic agents, improving bioavailability, and offering precise targeting and biosafety, leading to increased therapeutic effectiveness. Nanomaterials loaded with non-coding RNAs not only inhibit fibrosis but also promote myocardial cell regeneration and repair, offering promising new avenues for the treatment of fibrosis. Future developments aim to integrate diagnostic and therapeutic functionalities, enabling early detection and personalized treatment strategies.
Promotion of Angiogenesis
Angiogenesis at the infarct border following MI is a critical tissue repair process. Therapeutic angiogenesis can restore blood flow in the early stages of MI, salvage ischemic myocardial tissue, reduce infarct size, and improve patient prognosis.109 Currently, nanotechnology is being utilized to enhance therapeutic angiogenesis through the development of nano-drug delivery systems. Some nanomaterials can also directly promote angiogenesis or be used for the fabrication of artificial blood vessels.
VEGF and fibroblast growth factors (FGFs) play crucial roles in neovascularization. VEGF has a short half-life, and its direct injection into the myocardium results in rapid enzymatic inactivation, significantly reducing its pharmacological effect. Therefore, the use of nanomaterials can more effectively target the release of angiogenic factors in the myocardial infarction area. Wu et al designed an injectable conductive hydrogel (Alg-P-AAV hydrogel) with angiogenic capabilities by incorporating lignosulfonate-doped polyaniline (PAN/LS) nanorods, adeno-associated virus encoding VEGF (AAV9-VEGF), and calcium-crosslinked alginate hydrogel as the basic scaffold. After injecting Alg-P-AAV hydrogel around the infarcted area in rats, it activated the angiogenic pathways involving VEGFR2 and PI3K.80 Basic fibroblast growth factor (bFGF) has been shown to promote angiogenesis, but its clinical efficacy is limited due to its short biological half-life and low plasma stability. Wang et al co-assembled bFGF with biocompatible precursor peptide K2 to form bFGF@K2 micelles, which, upon interaction with MMP9, converted into bFGF@Nanofiber. The nanofibers slowly released bFGF in MI rats, significantly increasing bFGF retention and promoting neovascularization.81 Recently, hepatocyte growth factor (HGF) has been found to promote angiogenesis by activating the Met receptor. Guo et al used self-assembling peptide nanofibers to load pro-hepatocyte growth factor (pro-HGF) activators. These nanofibers interact with the β-chain of pro-HGF in MI, achieving allosteric activation. The nanofibers extended the release time of the activator in MI mice and significantly promoted neovascularization at the infarct border zone.82
Certain nanomaterials can directly promote angiogenesis, such as CNT, carbon nanofibers (CNF), and graphene oxide (GO).110,111 Tashakori-Miyanroudi et al synthesized collagen scaffolds with CNF, promoting the formation of vascular networks in the rat myocardial infarction area.11 GO specifically induces angiogenesis by regulating the physiological levels of ROS and the activation of endothelial inducible nitric oxide synthase (iNOS).112 The chick embryo angiogenesis assay supports the angiogenic capacity of sericin-functionalized graphene oxide (SGO), demonstrating its ability to promote vascular development and maturation.83 Additionally, certain metal nanoparticles promote angiogenesis, such as cobalt,113 cerium,114 strontium,115 magnesium,116 and copper.117 For example, copper regulates the activity of several proteins and factors involved in angiogenesis, such as VEGF, fibronectin, angiopoietins, ceruloplasmin, and FGF.118 Copper-induced angiogenesis mechanisms include hypoxia-induced HIF-1 pathway.119 Copper can also activate the MAPK signaling pathway, leading to increased NO production, thereby promoting angiogenesis.118 Recently, a team designed artificial hybrid nanoparticles containing copper proteins. These nanoparticles mimic the secretory factors (SF) released by hypoxic stem cells and catalyze the conversion of NO precursors in plasma, thus promoting NO production and angiogenesis. In a mouse model of myocardial infarction, the nanoparticles synergistically promoted vascular regeneration through the combined release of SF and NO.84 Copper-loaded milk protein-derived microgels can maintain homeostasis in the internal environment after MI.120 Moreover, mesoporous silica nanoparticles (MSNs) have shown great potential in angiogenesis in recent years. Feng et al designed a novel injectable hydrogel to deliver mesoporous silica (CHP@Si) for myocardial repair. The hydrogel-released CHP@Si promotes the expression of angiogenic factors eNOS and FGF-2.85
Promoting endogenous angiogenesis through the direct or indirect delivery of growth factors or cytokines requires time. Artificial blood vessels can guide blood flow to the infarcted area, similar to CABG. Organic nanofibers, including PLGA NPs, gelatin shell nanofibers, and polycaprolactone, are used to produce artificial blood vessels, providing a new approach to artificial angiogenesis.119 However, artificial vascular grafts still have many limitations, such as thrombosis, vessel rupture, and blood extravasation. There is a need to develop artificial blood vessels with good mechanical properties, biocompatibility, and antithrombotic capabilities. Further, in vivo experiments are required to demonstrate the feasibility of tissue-engineered vascular grafts.121
In summary, nanomaterials can deliver proteins or drugs that promote angiogenesis to the desired location, exhibiting excellent stability and targeting. Some nanomaterials can directly stimulate angiogenesis with high efficiency and minimal toxicity. Additionally, research on using nanomaterials in the fabrication of artificial blood vessels is growing. Future efforts should focus on optimizing production techniques to minimize the risk of transplant failure.
Cardiac Conduction Repair
When designing biomaterials for the in vivo treatment of myocardial infarction (MI), conductivity is often overlooked. Conductive biomaterials are used in MI treatment because they can enhance the propagation of electrical signals through non-conductive scar tissue.122 AuNPs and carbon-based nanomaterials, such as CNTs and GO, exhibit effective conductivity and play a crucial role in improving intercellular communication, electrical signal transmission, and anti-arrhythmic effects.123,124 Cardiac patch transplantation and intramyocardial injection of biomaterials can alleviate adverse effects following MI. These treatments improve the function of infarcted hearts by bridging infarcted and non-infarcted myocardium and restoring myocardial electrical integrity.125–127
Conductive cardiac patches use their conductivity to connect healthy myocardium with the infarcted area, thereby reconstructing damaged cardiac tissue.128 CNTs are one-dimensional cylindrical nanostructured carbon materials with high anisotropy and extremely high aspect ratios. Wang et al designed a conductive cardiac patch using elastin, gelatin, and CNTs, which exhibited high mechanical performance, shape memory, and conductivity. In both rat and mini-pig models of MI, this patch demonstrated improved electrical conduction and cardiac function.86 Mei et al GO with mesenchymal stem cells (MSCs) to create a conductive (MSC@GO) hydrogel patch. This patch adheres to the epicardium, providing strong electrical integration with the infarcted heart and offering mechanical and regenerative support to the infarcted area. It upregulates the expression of connexin 43 (Cx43) and effectively repairs myocardial infarction in vivo. In a mouse model of MI, the MSC@GO hydrogel patch reduced apoptosis, promoted Cx43 expression, and enhanced cardiac function, supporting cardiac repair.87 Anisotropic conductive reduced graphene oxide (rGO)/silk patches can repair infarcted myocardium by reconstructing the anisotropic electrical microenvironment in the infarcted heart. These patches improve cardiac function, resist ventricular fibrillation, and increase angiogenesis in the capillary network, thereby alleviating post-infarction myocardial remodeling.88
Intramyocardial injection of hydrogels incorporating nanomaterials can restore electrical conduction at the site of MI, maintaining cardiac function and enhancing repair.129 Zhou et al designed a conductive injectable hydrogel by incorporating GO nanoparticles into oligo(poly(ethylene glycol) fumarate) (OPF) hydrogels. In vitro, the combination of GO and OPF hydrogels enhanced cell attachment. In a rat model of MI, the injection of conductive OPF/GO hydrogels into the infarcted area not only provided mechanical support but also improved Ca2+ signal propagation, upregulated Cx43 expression, reduced infarct size, and enhanced neovascularization compared to OPF and PBS groups.89 Zhu et al prepared an injective hydrogel composed of GelMA, oxidized dextran, and rGO. The UCMSCs were encapsulated within this GelMA/oxidized dextran/rGO hydrogel and then injected into the infarcted myocardium of rats. They observed that the use of GelMA/oxidized dextran/rGO significantly improved ejection fraction, reduced infarct size, and enhanced Cx43 expression levels compared to the control group (rGO-free hydrogel).90 In a study by Hekai Li, a hydrogel composed of AuNPs and hyaluronic acid (HA) was fabricated. The AuNP-HA hydrogel encapsulated human-induced pluripotent stem cell-derived cardiomyocytes (hiPS-CMs). After permanent ligation of the left anterior descending coronary artery in mice, the hydrogel was injected into the infarcted myocardium. The AuNP-HA hydrogel improved the contractile function and electrophysiological activity of hiPS-CMs by promoting the formation of gap junction protein Cx43 through the integrin/ILK1/p-AKT pathway. Additionally, hiPS-CMs promoted vascular regeneration in the infarcted area via paracrine effects, exerting a protective effect on the heart.91 A functional conductive hydrogel was prepared by combining hydrophilic and biocompatible poly(vinyl alcohol) (PVA) with conductive melanin nanoparticles. The composite hydrogel, prepared through a simple manufacturing process involving five freeze-thaw cycles, exhibited satisfactory mechanical properties and conductivity, approaching the mechanical and electrical properties of native heart tissue. In vitro experiments evaluated its physical properties and biocompatibility, indicating that the introduction of melanin particles successfully improved the elasticity, conductivity, and cell adhesion of PVA hydrogels. In vivo, the composite hydrogel enhanced cardiac repair in a rat model of MI by reducing infarct size, slowing ventricular wall thinning, and promoting angiogenesis.92
In summary, nanomaterials hold significant potential in enhancing electrical conduction, ensuring effective myocardial cell contraction after MI, reducing the incidence of arrhythmias, and promoting heart repair. While cardiac patches and intramyocardial injection are simple and effective, they are invasive procedures with associated risks. Future research should explore minimally invasive or non-invasive approaches to improve treatment efficacy further and reduce patient morbidity.
Current Issues
Nanomedicine shows significant potential in treating cardiovascular diseases, and efficient NPs drug delivery systems are being developed. However, several challenges remain. As a relatively new field, nanotechnology requires specialized regulatory guidelines to ensure consistency in the size, shape, chemical composition, and surface charge of NPs.130 Compared to conventional chemicals, NPs exhibit higher biotoxicity and more complex toxicological mechanisms, with cardiotoxicity being a major concern.131 NPs can affect the normal contraction and relaxation of the myocardium, alter cardiac hemodynamics, and induce oxidative stress, apoptosis, and inflammatory responses in myocardial cells. These effects can also disrupt mitochondrial membrane integrity, potentially leading to various serious heart conditions.132 For example, zinc oxide (ZnO) NPs produce cytotoxic effects in a concentration- and time-dependent manner, inducing apoptosis and mitochondrial dysfunction in rat myocardial cells, which affects their normal function.133 Additionally, NPs have been reported to influence the progression of AS. Polymer NPs, silica (Si) NPs, TiO2 NPs, and CNTs have been found to cause dyslipidemia, foam cell formation, and the expansion of atherosclerotic plaques in vivo.134 To mitigate nanoparticle toxicity, we have developed a series of strategies that focus on selecting appropriate raw materials and optimizing the nanoparticles’ size, shape, and surface charge. NPs can be synthesized using biocompatible materials such as plants, fungi, bacteria, and microalgae. These materials are non-toxic, biodegradable, and renewable, offering significant advantages. The synthesis of metal NPs using plant parts or their extracts has been demonstrated to be both effective and environmentally friendly. Various plant metabolites, including terpenoids, flavonoids, sugars, and proteins, can actively reduce metal ions to form nanoparticles.135 For example, Saifuddin et al found that extracts from roots, stems, leaves, flowers, fruits, and seeds of green plants can reduce Ag+ to stable nano-forms of Ag+0.136 Polyphenols, a class of naturally occurring secondary metabolites found in fruits, vegetables, and herbs, exhibit a range of pharmacological activities, including immunomodulation, intrinsic antioxidant properties, anti-inflammatory effects, and anti-angiogenic properties. Yu et al utilized phenolic compounds to synthesize nanoparticles for the treatment of MI injury.137 Alternatively, biodegradable materials, such as PLGA, are also suitable for NP synthesis. When NPs reach target cells, cellular uptake occurs, releasing the drug while the NPs are degraded.138 Adjusting the size, shape, and surface charge of NPs can enhance their safety and efficacy. Nanoparticle size is a critical determinant of cellular uptake efficiency, as it influences the enthalpy and entropy characteristics that govern adhesion between NPs and cell receptors.139 Smaller NPs have been shown to exhibit higher cellular uptake efficiency. NPs with diameters less than 10 nm are typically cleared rapidly by the kidneys, making them suitable for short-term therapy or diagnostics and avoiding long-term retention in the cardiovascular system.140,141 The shape of NPs, such as spherical, cubic, or rod-like, also impacts cellular uptake. Spherical NPs are reported to be more readily taken up by cells compared to other shapes with the same composition, and they are relatively safer.142 Positively charged NPs are highly associated with cytotoxicity, and reducing positive charge can minimize damage to cardiovascular endothelial cells.143 Optimizing the surface modification of NPs is crucial. Various coating materials and techniques are available for different types of NPs, including polymer-based, lipid-based, and inorganic NPs. Coating materials include polyethylene glycol (PEG), polyvinylpyrrolidone (PVP,) PVA, phosphocholine-based copolymers, and polysaccharides such as dextran and chitosan.144,145 Recently, Vukoje et al demonstrated that dextran-coated AgNPs exhibit lower cytotoxicity compared to uncoated AgNPs.146
Moreover, the stability of nanodrugs within the body is crucial. NPs interact with proteins, glucose, and lipids in vivo, potentially altering their metabolic pathways or affecting their targeting efficiency. One of the most studied interactions is between NPs and proteins. Upon entering the body, NPs are rapidly coated by surrounding proteins, forming a “protein corona” on their surface. This protein corona can significantly alter the surface properties of NPs, influencing their behavior.147 For example, when covered by proteins, the ligands on the NP surface may become blocked, rendering targeted ligands ineffective, or the NP-protein complex may be cleared by macrophages.148 In circulation, these drugs must resist biological factors such as protein adsorption, immune responses, and enzymatic degradation to maintain their structure and function. Hemodynamic forces can cause disintegration, leading to microvascular embolism and altering the uniform distribution of active components, thus impacting the efficacy of nanomedical treatments. Therefore, precise control of drug release kinetics is essential to ensure that therapeutic molecules are delivered at the right time, place, and in the appropriate dose.
Lastly, current research primarily relies on animal models, with limited analysis of clinical cases. Disease progression and pathology in animals often differ significantly from those in humans, making the direct application of animal study results to human patients challenging. Therefore, translating NP-based therapies into clinical practice remains a significant challenge.
Conclusion
Nanomaterials offer a promising approach for the diagnosis and treatment of myocardial infarction, including the detection of biomarkers, imaging, modulation of macrophage inflammation, anti-ROS activity, inhibition of fibrosis, promotion of angiogenesis, and cardiac repair. These materials can enhance imaging and biosensing capabilities, using advanced contrast agents and high-resolution imaging technologies for early detection of coronary artery disease. Furthermore, they enable targeted drug delivery, tissue engineering, and the regulation of inflammation and oxidative stress, addressing multiple aspects of myocardial infarction pathophysiology. Despite these advances, challenges and opportunities persist in the delivery, design, and personalized application of NPs for myocardial infarction. Ongoing innovation and collaboration among researchers, clinicians, and industry partners hold the potential to revolutionize the management of myocardial infarction and improve patient outcomes.
Data Sharing Statement
There are no supplemental data with this paper. All information is available in the manuscript.
Ethical Approval Statement
Ethics approval is not applicable as this is a review paper and does not involve direct research on animals or humans.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Martin SS, Aday AW, Almarzooq ZI, et al. 2024 heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation. 2024;149(8):e347–e913. doi:10.1161/CIR.0000000000001209
2. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153–e639. doi:10.1161/CIR.0000000000001052
3. Bhatt DL, Lopes RD, Harrington RA. Diagnosis and treatment of acute coronary syndromes: a review. JAMA. 2022;327(7):662–675. doi:10.1001/jama.2022.0358
4. Saito Y, Oyama K, Tsujita K, Yasuda S, Kobayashi Y. Treatment strategies of acute myocardial infarction: updates on revascularization, pharmacological therapy, and beyond. J Cardiol. 2023;81(2):168–178. doi:10.1016/j.jjcc.2022.07.003
5. Yandrapalli S, Andries G, Gupta S, Dajani AR, Aronow WS. Investigational drugs for the treatment of acute myocardial infarction: focus on antiplatelet and anticoagulant agents. Expert Opin Investig Drugs. 2019;28(3):223–234. doi:10.1080/13543784.2019.1559814
6. Pan Q, Xu J, Wen CJ, Xiong YY, Gong ZT, Yang YJ. Nanoparticles: promising tools for the treatment and prevention of myocardial infarction. Int J Nanomed. 2021;16:6719–6747. doi:10.2147/IJN.S328723
7. Yu Z, Gong H, Li M, Tang D. Hollow Prussian blue nanozyme-richened liposome for artificial neural network-assisted multimodal colorimetric-photothermal immunoassay on smartphone. Biosens Bioelectron. 2022;218:114751. doi:10.1016/j.bios.2022.114751
8. Tang C, Zhou K, Wu D, Zhu H. Nanoparticles as a novel platform for cardiovascular disease diagnosis and therapy. Int J Nanomed. 2024;19:8831–8846. doi:10.2147/IJN.S474888
9. Li H, Zhu J, Xu YW, et al. Notoginsenoside R1-loaded mesoporous silica nanoparticles targeting the site of injury through inflammatory cells improves heart repair after myocardial infarction. Redox Biol. 2022;54:102384. doi:10.1016/j.redox.2022.102384
10. Song L, Jia K, Yang F, Wang J. Advanced nanomedicine approaches for myocardial infarction treatment. Int J Nanomed. 2024;19:6399–6425. doi:10.2147/IJN.S467219
11. Tashakori-Miyanroudi M, Rakhshan K, Ramez M, et al. Conductive carbon nanofibers incorporated into collagen bio-scaffold assists myocardial injury repair. Int J Biol Macromol. 2020;163:1136–1146. doi:10.1016/j.ijbiomac.2020.06.259
12. Jain A, Behera M, Mahapatra C, Sundaresan NR, Chatterjee K. Nanostructured polymer scaffold decorated with cerium oxide nanoparticles toward engineering an antioxidant and anti-hypertrophic cardiac patch. Mater Sci Eng C Mater Biol Appl. 2021;118:111416. doi:10.1016/j.msec.2020.111416
13. Falk E, Nakano M, Bentzon JF, Finn AV, Virmani R. Update on acute coronary syndromes: the pathologists’ view. Eur Heart J. 2013;34(10):719–728. doi:10.1093/eurheartj/ehs411
14. Wang Y, Li Y, Lu Y, Li J. Biomimetic nanoparticles for the diagnosis and therapy of atherosclerosis. Chem Rec. 2024;24:e202400087. doi:10.1002/tcr.202400087
15. Badimon L, Vilahur G. Thrombosis formation on atherosclerotic lesions and plaque rupture. J Intern Med. 2014;276(6):618–632. doi:10.1111/joim.12296
16. Zhang Y, Yu W, Zhang L, Li P. Nanozyme-based visual diagnosis and therapeutics for myocardial infarction: the application and strategy. J Adv Res. 2024.
17. Kumar A, Vora K, Bhatt DL, Dharmakumar R. The Canadian Cardiovascular Society Classification of acute atherothrombotic myocardial infarction provides a novel staging scheme based on tissue injury severity. Eur Heart J. 2024;45(12):976–979. doi:10.1093/eurheartj/ehad821
18. Kumar A, Connelly K, Vora K, et al. The Canadian Cardiovascular Society Classification of acute atherothrombotic myocardial infarction based on stages of tissue injury severity: an expert consensus statement. Can J Cardiol. 2024;40(1):1–14. doi:10.1016/j.cjca.2023.09.020
19. Almaghrbi H, Giordo R, Pintus G, Zayed H. Non-coding RNAs as biomarkers of myocardial infarction. Clin Chim Acta. 2023;540:117222. doi:10.1016/j.cca.2023.117222
20. Mansuriya BD, Altintas Z. Enzyme-free electrochemical nano-immunosensor based on graphene quantum dots and gold nanoparticles for cardiac biomarker determination. Nanomaterials. 2021;11(3):578. doi:10.3390/nano11030578
21. Zapp E, Brondani D, Silva TR, Girotto E, Gallardo H, Vieira IC. Label-free immunosensor based on liquid crystal and gold nanoparticles for cardiac troponin I detection. Biosensors. 2022;12(12):1113. doi:10.3390/bios12121113
22. Lopa NS, Rahman MM, Ahmed F, et al. Simple, low-cost, sensitive and label-free aptasensor for the detection of cardiac troponin I based on a gold nanoparticles modified titanium foil. Biosens Bioelectron. 2019;126:381–388. doi:10.1016/j.bios.2018.11.012
23. Zhu L, Ye J, Yan M, et al. Electrochemiluminescence immunosensor based on Au nanocluster and hybridization chain reaction signal amplification for ultrasensitive detection of cardiac troponin I. ACS Sens. 2019;4(10):2778–2785. doi:10.1021/acssensors.9b01369
24. Wang S, Zhao Y, Wang M, et al. Enhancing luminol electrochemiluminescence by combined use of cobalt-based metal organic frameworks and silver nanoparticles and its application in ultrasensitive detection of cardiac troponin I. Anal Chem. 2019;91(4):3048–3054. doi:10.1021/acs.analchem.8b05443
25. Feng S, Yan M, Xue Y, Huang J, Yang X. Electrochemical immunosensor for cardiac troponin I detection based on covalent organic framework and enzyme-catalyzed signal amplification. Anal Chem. 2021;93(40):13572–13579. doi:10.1021/acs.analchem.1c02636
26. Ma Y, Dong YX, Wang B, Ren SW, Cao JT, Liu YM. CdS:Mn-sensitized 2D/2D heterostructured g-C(3)N(4)-MoS(2) with excellent photoelectrochemical performance for ultrasensitive immunosensing platform. Talanta. 2020;207:120288. doi:10.1016/j.talanta.2019.120288
27. Al Fatease A, Haque M, Umar A, et al. Label-free electrochemical sensor based on manganese doped titanium dioxide nanoparticles for myoglobin detection: biomarker for acute myocardial infarction. Molecules. 2021;26(14):4252. doi:10.3390/molecules26144252
28. He S, Zhang P, Sun J, Ji Y, Huang C, Jia N. Integrating potential-resolved electrochemiluminescence with molecularly imprinting immunoassay for simultaneous detection of dual acute myocardial infarction markers. Biosens Bioelectron. 2022;201:113962. doi:10.1016/j.bios.2022.113962
29. Pu Q, Yang X, Guo Y, et al. Simultaneous colorimetric determination of acute myocardial infarction biomarkers by integrating self-assembled 3D gold nanovesicles into a multiple immunosorbent assay. Mikrochim Acta. 2019;186(3):138. doi:10.1007/s00604-019-3242-y
30. Adhikari J, Keasberry NA, Mahadi AH, Yoshikawa H, Tamiya E, Ahmed MU. An ultra-sensitive label-free electrochemiluminescence CKMB immunosensor using a novel nanocomposite-modified printed electrode. RSC Adv. 2019;9(59):34283–34292. doi:10.1039/C9RA05016G
31. Chen M, Wang Y, Zhao X, et al. Target-responsive DNA hydrogel with microfluidic chip smart readout for quantitative point-of-care testing of creatine kinase MB. Talanta. 2022;243:123338. doi:10.1016/j.talanta.2022.123338
32. Zhang J, Wang Y, Zhao X, et al. Dual sensitization smartphone colorimetric strategy based on RCA coils gathering Au tetrahedra and its application in the detection of CK-MB. Anal Chem. 2021;93(50):16922–16931. doi:10.1021/acs.analchem.1c04139
33. Sun Y, Shi L, Wang Q, Mi L, Li T. Spherical Nucleic Acid Enzyme (SNAzyme) boosted chemiluminescence miRNA imaging using a smartphone. Anal Chem. 2019;91(5):3652–3658. doi:10.1021/acs.analchem.8b05696
34. Shi L, Sun Y, Mi L, Li T. Target-Catalyzed Self-Growing Spherical Nucleic Acid Enzyme (SNAzyme) as a double amplifier for ultrasensitive chemiluminescence MicroRNA detection. ACS Sens. 2019;4(12):3219–3226. doi:10.1021/acssensors.9b01655
35. Mi L, Sun Y, Shi L, Li T. Hemin-bridged MOF interface with double amplification of G-quadruplex payload and DNAzyme catalysis: ultrasensitive lasting chemiluminescence MicroRNA imaging. ACS Appl Mater Interfaces. 2020;12(7):7879–7887. doi:10.1021/acsami.9b18053
36. Chapman AR, Adamson PD, Shah ASV, et al. High-sensitivity cardiac troponin and the universal definition of myocardial infarction. Circulation. 2020;141(3):161–171. doi:10.1161/CIRCULATIONAHA.119.042960
37. Yuan Z, Wang L, Chen J, et al. Electrochemical strategies for the detection of cTnI. Analyst. 2021;146(18):5474–5495. doi:10.1039/D1AN00808K
38. Rabbani G, Ahmad E, Khan ME, et al. Synthesis of carbon nanotubes-chitosan nanocomposite and immunosensor fabrication for myoglobin detection: an acute myocardial infarction biomarker. Int J Biol Macromol. 2024;265(Pt 1):130616.
39. Sun JH, Liu XK, Xing XW, Yang Y, Xuan HH, Fu BB. Value of cardiac troponin, myoglobin combined with heart-type fatty acid-binding protein detection in diagnosis of early acute myocardial infarction. Pak J Med Sci. 2023;39(6):1690–1694. doi:10.12669/pjms.39.6.7101
40. Aydin S, Ugur K, Aydin S, Sahin İ, Yardim M. Biomarkers in acute myocardial infarction: current perspectives. Vasc Health Risk Manag. 2019;15:1–10. doi:10.2147/VHRM.S166157
41. Li Y, Li B, Wang X, Meng Y, Bai L, Zheng Y. Safe and efficient magnetic resonance imaging of acute myocardial infarction with gadolinium-doped carbon dots. Nanomedicine. 2020;15(24):2385–2398. doi:10.2217/nnm-2020-0160
42. Li B, Li Y, Chen S, Wang Y, Zheng Y. VEGF mimetic peptide-conjugated nanoparticles for magnetic resonance imaging and therapy of myocardial infarction. J Control Release. 2023;360:44–56. doi:10.1016/j.jconrel.2023.06.017
43. Wang F, Wen L, Liu J, et al. Albumin nanocomposites with MnO(2)/Gd(2)O(3) motifs for precise MR imaging of acute myocardial infarction in rabbit models. Biomaterials. 2020;230:119614. doi:10.1016/j.biomaterials.2019.119614
44. Van Herck JL, De meyer GR, Martinet W, et al. Multi-slice computed tomography with N1177 identifies ruptured atherosclerotic plaques in rabbits. Basic Res Cardiol. 2010;105(1):51–59. doi:10.1007/s00395-009-0052-0
45. Kee PH, Danila D. CT imaging of myocardial scar burden with CNA35-conjugated gold nanoparticles. Nanomedicine. 2018;14(6):1941–1947. doi:10.1016/j.nano.2018.06.003
46. Guo M, Du W, Lyu N, et al. Ultra-early diagnosis of acute myocardial infarction in rats using ultrasound imaging of hollow double-layer silica nanospheres. Adv Healthc Mater. 2020;9(3):e1901155. doi:10.1002/adhm.201901155
47. Zhang Y, Chen X, Liu L, Tian J, Hao L, Ran HT. Photoacoustic imaging of myocardial infarction region using non-invasive fibrin-targeted nanoparticles in a rat myocardial ischemia-reperfusion model. Int J Nanomed. 2021;16:1331–1344. doi:10.2147/IJN.S293736
48. Zhao P, Li B, Li Y, Chen L, Wang H, Ye L. DNA-Templated ultrasmall bismuth sulfide nanoparticles for photoacoustic imaging of myocardial infarction. J Colloid Interface Sci. 2022;615:475–484. doi:10.1016/j.jcis.2022.01.194
49. Wang X, Pu J. Recent advances in cardiac magnetic resonance for imaging of acute myocardial infarction. Small Methods. 2024;8(3):e2301170. doi:10.1002/smtd.202301170
50. Assen MV, Vonder M, Pelgrim GJ, Von Knebel Doeberitz PL, Vliegenthart R. Computed tomography for myocardial characterization in ischemic heart disease: a state-of-the-art review. Eur Radiol Exp. 2020;4(1):36. doi:10.1186/s41747-020-00158-1
51. Meir R, Popovtzer R. Cell tracking using gold nanoparticles and computed tomography imaging. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2018;10(2). doi:10.1002/wnan.1480
52. Setia A, Mehata AK, Priya V, et al. Current advances in nanotheranostics for molecular imaging and therapy of cardiovascular disorders. Mol Pharmaceut. 2023;20(10):4922–4941. doi:10.1021/acs.molpharmaceut.3c00582
53. Lin Y, Qiu T, Lan Y, et al. Multi-modal optical imaging and combined phototherapy of nasopharyngeal carcinoma based on a nanoplatform. Int J Nanomed. 2022;17:2435–2446. doi:10.2147/IJN.S357493
54. Fujiwara M, Matoba T, Koga J-I, et al. Nanoparticle incorporating Toll-like receptor 4 inhibitor attenuates myocardial ischaemia–reperfusion injury by inhibiting monocyte-mediated inflammation in mice. Cardiovasc Res. 2019;115(7):1244–1255. doi:10.1093/cvr/cvz066
55. Zhang J, Dong Y, Liu X, et al. Effective myocardial infarction treatment by targeted accumulation of Sulforaphane using porous magnetic silica nanoparticles. Int J Pharm. 2023;645:123389. doi:10.1016/j.ijpharm.2023.123389
56. Lee J-R, Park B-W, Park J-H, et al. Local delivery of a senolytic drug in ischemia and reperfusion-injured heart attenuates cardiac remodeling and restores impaired cardiac function. Acta Biomater. 2021;135:520–533. doi:10.1016/j.actbio.2021.08.028
57. Tokutome M, Matoba T, Nakano Y, et al. Peroxisome proliferator-activated receptor-gamma targeting nanomedicine promotes cardiac healing after acute myocardial infarction by skewing monocyte/macrophage polarization in preclinical animal models. Cardiovasc Res. 2019;115(2):419–431. doi:10.1093/cvr/cvy200
58. Bao L, Dou G, Tian R, et al. Engineered neutrophil apoptotic bodies ameliorate myocardial infarction by promoting macrophage efferocytosis and inflammation resolution. Bioact Mater. 2022;9:183–197. doi:10.1016/j.bioactmat.2021.08.008
59. Chen J, Song Y, Wang Q, et al. Targeted neutrophil-mimetic liposomes promote cardiac repair by adsorbing proinflammatory cytokines and regulating the immune microenvironment. J Nanobiotechnology. 2022;20(1):218. doi:10.1186/s12951-022-01433-6
60. Zhou J, Liu W, Zhao X, et al. Natural melanin/alginate hydrogels achieve cardiac repair through ROS scavenging and macrophage polarization. Adv Sci. 2021;8(20). doi:10.1002/advs.202100505
61. Li F, Liu D, Liu M, et al. Tregs biomimetic nanoparticle to reprogram inflammatory and redox microenvironment in infarct tissue to treat myocardial ischemia reperfusion injury in mice. J Nanobiotechnol. 2022;20(1). doi:10.1186/s12951-022-01445-2
62. Sun M, Hu N, Gao Y, et al. Platelet membrane‐encapsulated nanocomplexes based on profundity scavenging ros strategy for myocardial infarction therapy. Adv Healthcare Mater. 2024.
63. Im GB, Kim YG, Yoo TY, et al. Ceria nanoparticles as copper chaperones that activate SOD1 for synergistic antioxidant therapy to treat ischemic vascular diseases. Adv Mater. 2023;35(16):e2208989. doi:10.1002/adma.202208989
64. Sun Q, Ma H, Zhang J, et al. A self-sustaining antioxidant strategy for effective treatment of myocardial infarction. Adv Sci. 2023;10(5):e2204999. doi:10.1002/advs.202204999
65. Shilo M, Oved H, Wertheim L, et al. Injectable nanocomposite implants reduce ROS accumulation and improve heart function after infarction. Adv Sci. 2021;8(24):e2102919. doi:10.1002/advs.202102919
66. Song Y, Xing H, He Y, et al. Inhibition of mitochondrial reactive oxygen species improves coronary endothelial function after cardioplegic hypoxia/reoxygenation. J Thorac Cardiovasc Surg. 2022;164(5):e207–e226. doi:10.1016/j.jtcvs.2021.06.029
67. Liu X, Chen B, Chen J, et al. A cardiac‐targeted nanozyme interrupts the inflammation‐free radical cycle in myocardial infarction. Adv Mater. 2023;36(2).
68. Li N, Huang C, Zhang J, et al. Chemotactic NO/H2S nanomotors realizing cardiac targeting of G-CSF against myocardial ischemia-reperfusion injury. ACS Nano. 2023;17(13):12573–12593. doi:10.1021/acsnano.3c02781
69. Guan Y, Niu H, Wen J, Dang Y, Zayed M, Guan J. Rescuing cardiac cells and improving cardiac function by targeted delivery of oxygen-releasing nanoparticles after or even before acute myocardial infarction. ACS Nano. 2022;16(11):19551–19566. doi:10.1021/acsnano.2c10043
70. Liu Y, Zhong D, He Y, et al. Photoresponsive hydrogel-coated upconversion cyanobacteria nanocapsules for myocardial infarction prevention and treatment. Adv Sci. 2022;9(30):e2202920. doi:10.1002/advs.202202920
71. Mehrotra S, Singh RD, Bandyopadhyay A, Janani G, Dey S, Mandal BB. Engineering microsphere-loaded non-mulberry silk-based 3D bioprinted vascularized cardiac patches with oxygen-releasing and immunomodulatory potential. ACS Appl Mater Interfaces. 2021;13(43):50744–50759. doi:10.1021/acsami.1c14118
72. Liu Y, Wang S, Zhang J, et al. Reprogramming the myocardial infarction microenvironment with melanin-based composite nanomedicines in mice. Nat Commun. 2024;15(1):6651. doi:10.1038/s41467-024-50854-4
73. Fu Y, Shi J, Qian H, et al. Alleviation of cardiac fibrosis using acellular peritoneal matrix-loaded pirfenidone nanodroplets after myocardial infarction in rats. Eur J Pharmacol. 2022;933:175238. doi:10.1016/j.ejphar.2022.175238
74. Ji X, Meng Y, Wang Q, et al. Cysteine-based redox-responsive nanoparticles for fibroblast-targeted drug delivery in the treatment of myocardial infarction. ACS Nano. 2023;17(6):5421–5434. doi:10.1021/acsnano.2c10042
75. Wen Z, Zhan J, Li H, et al. Dual-ligand supramolecular nanofibers inspired by the renin-angiotensin system for the targeting and synergistic therapy of myocardial infarction. Theranostics. 2021;11(8):3725–3741. doi:10.7150/thno.53644
76. Wang Q, Song Y, Chen J, et al. Direct in vivo reprogramming with non-viral sequential targeting nanoparticles promotes cardiac regeneration. Biomaterials. 2021;276:121028. doi:10.1016/j.biomaterials.2021.121028
77. Evers MJW, Du W, Yang Q, et al. Delivery of modified mRNA to damaged myocardium by systemic administration of lipid nanoparticles. J Control Release. 2022;343:207–216. doi:10.1016/j.jconrel.2022.01.027
78. Zhu D, Liu S, Huang K, et al. Intrapericardial long non-coding RNA-Tcf21 antisense RNA inducing demethylation administration promotes cardiac repair. Eur Heart J. 2023;44(19):1748–1760. doi:10.1093/eurheartj/ehad114
79. Li F, Chen L, Zhong S, et al. Collagen-targeting self-assembled nanoprobes for multimodal molecular imaging and quantification of myocardial fibrosis in a rat model of myocardial infarction. ACS Nano. 2024;18(6):4886–4902. doi:10.1021/acsnano.3c09801
80. Wu C, Zhang Y, Xu Y, et al. Injectable polyaniline nanorods/alginate hydrogel with AAV9-mediated VEGF overexpression for myocardial infarction treatment. Biomaterials. 2023;296:122088. doi:10.1016/j.biomaterials.2023.122088
81. Wang Y, Wang D, Wu C, et al. MMP 9-instructed assembly of bFGF nanofibers in ischemic myocardium to promote heart repair. Theranostics. 2022;12(17):7237–7249. doi:10.7150/thno.77345
82. Guo W, Feng W, Huang J, et al. Supramolecular self-assembled nanofibers efficiently activate the precursor of hepatocyte growth factor for angiogenesis in myocardial infarction therapy. ACS Appl Mater Interfaces. 2021;13(19):22131–22141. doi:10.1021/acsami.0c23153
83. Vedakumari SW, Veda Jancy SJ, Pravin YR, et al. Facile synthesis of sericin modified graphene oxide nanocomposites for treating ischemic diseases. Environ Res. 2022;209:112925. doi:10.1016/j.envres.2022.112925
84. Zhang X, Zhang Y, Zhang R, et al. Biomimetic design of artificial hybrid nanocells for boosted vascular regeneration in ischemic tissues. Adv Mater. 2022;34(14).
85. Feng J, Xing M, Qian W, Qiu J, Liu X. An injectable hydrogel combining medicine and matrix with anti-inflammatory and pro-angiogenic properties for potential treatment of myocardial infarction. Regen Biomater. 2023;10. doi:10.1093/rb/rbad036
86. Wang L, Liu Y, Ye G, et al. Injectable and conductive cardiac patches repair infarcted myocardium in rats and minipigs. Nat Biomed Eng. 2021;5(10):1157–1173. doi:10.1038/s41551-021-00796-9
87. Mei T, Cao H, Zhang L, et al. 3D printed conductive hydrogel patch incorporated with MSC@GO for efficient myocardial infarction repair. ACS Biomater Sci Eng. 2024;10(4):2451–2462. doi:10.1021/acsbiomaterials.3c01837
88. Zhao G, Feng Y, Xue L, et al. Anisotropic conductive reduced graphene oxide/silk matrices promote post-infarction myocardial function by restoring electrical integrity. Acta Biomater. 2022;139:190–203. doi:10.1016/j.actbio.2021.03.073
89. Zhou J, Yang X, Liu W, et al. Injectable OPF/graphene oxide hydrogels provide mechanical support and enhance cell electrical signaling after implantation into myocardial infarct. Theranostics. 2018;8(12):3317–3330. doi:10.7150/thno.25504
90. Zhu S, Yu C, Liu N, et al. Injectable conductive gelatin methacrylate / oxidized dextran hydrogel encapsulating umbilical cord mesenchymal stem cells for myocardial infarction treatment. Bioact Mater. 2022;13:119–134. doi:10.1016/j.bioactmat.2021.11.011
91. Li H, Yu B, Yang P, et al. Injectable AuNP-HA matrix with localized stiffness enhances the formation of gap junction in engrafted human induced pluripotent stem cell-derived cardiomyocytes and promotes cardiac repair. Biomaterials. 2021;279:121231. doi:10.1016/j.biomaterials.2021.121231
92. Guan H, Liu J, Liu D, et al. Elastic and conductive Melanin/Poly(Vinyl Alcohol) composite hydrogel for enhancing repair effect on myocardial infarction. Macromol Biosci. 2022;22(12):e2200223. doi:10.1002/mabi.202200223
93. Hu D, Li R, Li Y, et al. Inflammation-targeted nanomedicines alleviate oxidative stress and reprogram macrophages polarization for myocardial infarction treatment. Adv Sci. 2024;11(21):e2308910. doi:10.1002/advs.202308910
94. Matter MA, Paneni F, Libby P, et al. Inflammation in acute myocardial infarction: the good, the bad and the ugly. Eur Heart J. 2024;45(2):89–103. doi:10.1093/eurheartj/ehad486
95. Kologrivova I, Shtatolkina M, Suslova T, Ryabov V. Cells of the immune system in cardiac remodeling: main players in resolution of inflammation and repair after myocardial infarction. Front Immunol. 2021;12:664457. doi:10.3389/fimmu.2021.664457
96. Hao T, Qian M, Zhang Y, et al. An injectable dual-function hydrogel protects against myocardial ischemia/reperfusion injury by modulating ROS/NO disequilibrium. Adv Sci. 2022;9(15):e2105408. doi:10.1002/advs.202105408
97. Bugger H, Pfeil K. Mitochondrial ROS in myocardial ischemia reperfusion and remodeling. Biochim Biophys Acta Mol Basis Dis. 2020;1866(7):165768. doi:10.1016/j.bbadis.2020.165768
98. Teixeira RB, Pfeiffer M, Zhang P, et al. Reduction in mitochondrial ROS improves oxidative phosphorylation and provides resilience to coronary endothelium in non-reperfused myocardial infarction. Basic Res Cardiol. 2023;118(1):3. doi:10.1007/s00395-022-00976-x
99. Sun Y, Zhang P, Li Y, et al. Light-activated gold-selenium core-shell nanocomposites with NIR-II photoacoustic imaging performances for heart-targeted repair. ACS Nano. 2022;16(11):18667–18681. doi:10.1021/acsnano.2c07311
100. Zhang Z, Dalan R, Hu Z, et al. Reactive oxygen species scavenging nanomedicine for the treatment of ischemic heart disease. Adv Mater. 2022;34(35):e2202169. doi:10.1002/adma.202202169
101. Shen J, Liang J, Rejiepu M, et al. Analysis of immunoinfiltration and EndoMT based on TGF-β signaling pathway-related genes in acute myocardial infarction. Sci Rep. 2024;14(1):5183. doi:10.1038/s41598-024-55613-5
102. Liang B, Zhang XX, Li R, Zhu YC, Tian XJ, Gu N. Guanxin V alleviates acute myocardial infarction by restraining oxidative stress damage, apoptosis, and fibrosis through the TGF-β1 signalling pathway. Phytomedicine. 2022;100:154077. doi:10.1016/j.phymed.2022.154077
103. Zeng Z, Wang Q, Yang X, et al. Qishen granule attenuates cardiac fibrosis by regulating TGF-β /Smad3 and GSK-3β pathway. Phytomedicine. 2019;62:152949. doi:10.1016/j.phymed.2019.152949
104. Xiao Y, Feng Q, Huang L, et al. Copper promotes cardiac functional recovery via suppressing the transformation of fibroblasts to myofibroblasts in ischemia-infarcted monkey hearts. J Nutr Biochem. 2023;111:109180. doi:10.1016/j.jnutbio.2022.109180
105. Yin X, Yin X, Pan X, et al. Post-myocardial infarction fibrosis: pathophysiology, examination, and intervention. Front Pharmacol. 2023;14:1070973. doi:10.3389/fphar.2023.1070973
106. Yang L, Xue S, Du M, Lian F. Highly efficient MicroRNA delivery using functionalized carbon dots for enhanced conversion of fibroblasts to cardiomyocytes. Int J Nanomed. 2021;16:3741–3754. doi:10.2147/IJN.S304873
107. Acharya A, Baek ST, Huang G, et al. The bHLH transcription factor Tcf21 is required for lineage-specific EMT of cardiac fibroblast progenitors. Development. 2012;139(12):2139–2149. doi:10.1242/dev.079970
108. Gil N, Ulitsky I. Regulation of gene expression by cis-acting long non-coding RNAs. Nat Rev Genet. 2020;21(2):102–117. doi:10.1038/s41576-019-0184-5
109. Bestepe F, Fritsche C, Lakhotiya K, et al. Deficiency of miR-409-3p improves myocardial neovascularization and function through modulation of DNAJB9/p38 MAPK signaling. Mol Ther Nucleic Acids. 2023;32:995–1009. doi:10.1016/j.omtn.2023.05.021
110. Tashakori-Miyanroudi M, Janzadeh A, Seifalian A, Aboutaleb N, Azizi Y, Ramezani F. Will carbon nanotube/nanofiber bring new hope for the treatment of heart damage? A systematic review. Nanomedicine. 2022;17(29):2189–2205. doi:10.2217/nnm-2022-0113
111. D’Amora U, Dacrory S, Hasanin MS, et al. Advances in the physico-chemical, antimicrobial and angiogenic properties of graphene-oxide/cellulose nanocomposites for wound healing. Pharmaceutics. 2023;15(2):338. doi:10.3390/pharmaceutics15020338
112. Mukherjee S, Sriram P, Barui AK, et al. Graphene oxides show angiogenic properties. Adv Healthc Mater. 2015;4(11):1722–1732. doi:10.1002/adhm.201500155
113. Zhang H, Zhao Y, Zhang Y, Hang R, Yao X, Hang R. Exosomes derived from macrophages upon cobalt ion stimulation promote angiogenesis. Colloids Surf B Biointerfaces. 2021;203:111742. doi:10.1016/j.colsurfb.2021.111742
114. Fu L, Li R, Whitelock JM, Lord MS. Tuning the intentional Corona of cerium oxide nanoparticles to promote angiogenesis via fibroblast growth factor 2 signalling. Regen Biomater. 2022;9:rbac081. doi:10.1093/rb/rbac081
115. Lu W, Zhou C, Ma Y, et al. Improved osseointegration of strontium-modified titanium implants by regulating angiogenesis and macrophage polarization. Biomater Sci. 2022;10(9):2198–2214. doi:10.1039/D1BM01488A
116. Hong X, Tian G, Zhu Y, Ren T. Exogeneous metal ions as therapeutic agents in cardiovascular disease and their delivery strategies. Regen Biomater. 2024;11:rbad103. doi:10.1093/rb/rbad103
117. Zhu S, Zhao B, Li M, et al. Microenvironment responsive nanocomposite hydrogel with NIR photothermal therapy, vascularization and anti-inflammation for diabetic infected wound healing. Bioact Mater. 2023;26:306–320. doi:10.1016/j.bioactmat.2023.03.005
118. Kargozar S, Baino F, Hamzehlou S, Hamblin MR, Mozafari M. Nanotechnology for angiogenesis: opportunities and challenges. Chem Soc Rev. 2020;49(14):5008–5057. doi:10.1039/c8cs01021h
119. Shi HT, Huang ZH, Xu TZ, Sun AJ, Ge JB. New diagnostic and therapeutic strategies for myocardial infarction via nanomaterials. EBioMedicine. 2022;78:103968. doi:10.1016/j.ebiom.2022.103968
120. Hong X, Tian G, Dai B, et al. Copper-loaded milk-protein derived microgel preserves cardiac metabolic homeostasis after myocardial infarction. Adv Sci. 2024;11(35):e2401527. doi:10.1002/advs.202401527
121. Joseph J, Domenico Bruno V, Sulaiman N, et al. A novel small diameter nanotextile arterial graft is associated with surgical feasibility and safety and increased transmural endothelial ingrowth in pig. J Nanobiotechnology. 2022;20(1):71. doi:10.1186/s12951-022-01268-1
122. Li Y, Wei L, Lan L, et al. Conductive biomaterials for cardiac repair: a review. Acta Biomater. 2022;139:157–178. doi:10.1016/j.actbio.2021.04.018
123. Ashtari K, Nazari H, Ko H, et al. Electrically conductive nanomaterials for cardiac tissue engineering. Adv Drug Deliv Rev. 2019;144:162–179. doi:10.1016/j.addr.2019.06.001
124. Edrisi F, Baheiraei N, Razavi M, Roshanbinfar K, Imani R, Jalilinejad N. Potential of graphene-based nanomaterials for cardiac tissue engineering. J Mater Chem B. 2023;11(31):7280–7299. doi:10.1039/D3TB00654A
125. Yin Q, Zhu P, Liu W, et al. A conductive bioengineered cardiac patch for myocardial infarction treatment by improving tissue electrical integrity. Adv Healthc Mater. 2023;12(1):e2201856. doi:10.1002/adhm.202201856
126. Shi T, Wang P, Ren Y, et al. Conductive hydrogel patches with high elasticity and fatigue resistance for cardiac microenvironment remodeling. ACS Appl Mater Interfaces. 2023.
127. Zhang L, Bei Z, Li T, Qian Z. An injectable conductive hydrogel with dual responsive release of rosmarinic acid improves cardiac function and promotes repair after myocardial infarction. Bioact Mater. 2023;29:132–150. doi:10.1016/j.bioactmat.2023.07.007
128. Li Y, Qiu X. Bioelectricity-coupling patches for repairing impaired myocardium. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2022;14(4):e1787. doi:10.1002/wnan.1787
129. Lee M, Kim MC, Lee JY. Nanomaterial-based electrically conductive hydrogels for cardiac tissue repair. Int J Nanomed. 2022;17:6181–6200. doi:10.2147/IJN.S386763
130. Zhou Y, Yue T, Ding Y, et al. Nanotechnology translation in vascular diseases: from design to the bench. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2024;16(1):e1919. doi:10.1002/wnan.1919
131. Guo C, Liu Y, Li Y. Adverse effects of amorphous silica nanoparticles: focus on human cardiovascular health. J Hazard Mater. 2021;406:124626. doi:10.1016/j.jhazmat.2020.124626
132. Cheng Y, Chen Z, Yang S, et al. Nanomaterials-induced toxicity on cardiac myocytes and tissues, and emerging toxicity assessment techniques. Sci Total Environ. 2021;800:149584. doi:10.1016/j.scitotenv.2021.149584
133. Herrera-Rodríguez MA, Del Pilar Ramos-Godinez M, Cano-Martínez A, et al. Food-grade titanium dioxide and zinc oxide nanoparticles induce toxicity and cardiac damage after oral exposure in rats. Part Fibre Toxicol. 2023;20(1):43. doi:10.1186/s12989-023-00553-7
134. Chen S, Su Y, Zhang M, et al. Insights into the toxicological effects of nanomaterials on atherosclerosis: mechanisms involved and influence factors. J Nanobiotechnology. 2023;21(1):140. doi:10.1186/s12951-023-01899-y
135. Niżnik Ł, Noga M, Kobylarz D, et al. Gold nanoparticles (AuNPs)-Toxicity, safety and green synthesis: a critical review. Int J Mol Sci. 2024;25(7):4057. doi:10.3390/ijms25074057
136. Saifuddin NN, Matussin SN, Fariduddin Q, Khan MM. Potentials of roots, stems, leaves, flowers, fruits, and seeds extract for the synthesis of silver nanoparticles. Bioprocess Biosyst Eng. 2024;47(8):1119–1137. doi:10.1007/s00449-024-03044-x
137. Yu X, Wang J, Wang T, et al. Ellagic acid-enhanced biocompatibility and bioactivity in multilayer core-shell gold nanoparticles for ameliorating myocardial infarction injury. J Nanobiotechnology. 2024;22(1):554. doi:10.1186/s12951-024-02796-8
138. Ryu S, Park S, Lee HY, Lee H, Cho CW, Baek JS. Biodegradable nanoparticles-loaded PLGA microcapsule for the enhanced encapsulation efficiency and controlled release of hydrophilic drug. Int J Mol Sci. 2021;22(6):2792. doi:10.3390/ijms22062792
139. Hoshyar N, Gray S, Han H, Bao G. The effect of nanoparticle size on in vivo pharmacokinetics and cellular interaction. Nanomedicine. 2016;11(6):673–692. doi:10.2217/nnm.16.5
140. Wang Y, Sun SK, Liu Y, Zhang Z. Advanced hitchhiking nanomaterials for biomedical applications. Theranostics. 2023;13(14):4781–4801. doi:10.7150/thno.88002
141. Mitchell MJ, Billingsley MM, Haley RM, Wechsler ME, Peppas NA, Langer R. Engineering precision nanoparticles for drug delivery. Nat Rev Drug Discov. 2021;20(2):101–124. doi:10.1038/s41573-020-0090-8
142. Sharma N, Kurmi BD, Singh D, et al. Nanoparticles toxicity: an overview of its mechanism and plausible mitigation strategies. J Drug Targeting. 2024;32(5):457–469. doi:10.1080/1061186X.2024.2316785
143. You G, Hou J, Xu Y, Miao L, Ao Y, Xing B. Surface properties and environmental transformations controlling the bioaccumulation and toxicity of cerium oxide nanoparticles: a critical review. Rev Environ Contam Toxicol. 2021;253:155–206. doi:10.1007/398_2020_42
144. Biba R, Košpić K, Komazec B, et al. Surface coating-modulated phytotoxic responses of silver nanoparticles in plants and freshwater green algae. Nanomaterials. 2021;12(1):24. doi:10.3390/nano12010024
145. Sun L, Wang J, Li L, Xu ZP. Dynamic nano-assemblies based on two-dimensional inorganic nanoparticles: construction and preclinical demonstration. Adv Drug Deliv Rev. 2022;180:114031. doi:10.1016/j.addr.2021.114031
146. Vukoje I, Lazić V, Sredojević D, et al. Influence of glucose, sucrose, and dextran coatings on the stability and toxicity of silver nanoparticles. Int J Biol Macromol. 2022;194:461–469. doi:10.1016/j.ijbiomac.2021.11.089
147. Kopac T. Protein Corona, understanding the nanoparticle-protein interactions and future perspectives: a critical review. Int J Biol Macromol. 2021;169:290–301. doi:10.1016/j.ijbiomac.2020.12.108
148. Liu N, Tang M, Ding J. The interaction between nanoparticles-protein Corona complex and cells and its toxic effect on cells. Chemosphere. 2020;245:125624. doi:10.1016/j.chemosphere.2019.125624
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Caries Management with Non-Metallic Nanomaterials: A Systematic Review
Xu VW, Nizami MZI, Yin IX, Lung CYK, Yu OY, Chu CH
International Journal of Nanomedicine 2022, 17:5809-5824
Published Date: 30 November 2022
How Advanced are Conductive Nanocomposite Hydrogels for Repairing and Monitoring Myocardial Infarction?
Liu Y, Liu D, Xue Y, Sun H, Zhan X, Sun L, Kang K
International Journal of Nanomedicine 2025, 20:6777-6812
Published Date: 28 May 2025