")
Back to Journals » Clinical Ophthalmology » Volume 18
Outcomes of Anti-VEGF Therapy in Eyes with Diabetic Macular Edema, Vein Occlusion-Related Macular Edema, and Neovascular Age-Related Macular Degeneration: A Systematic Review
Authors Aldokhail LS , Alhadlaq AM, Alaradi LM, Alaradi LM , AlShaikh FY
Received 29 July 2024
Accepted for publication 3 December 2024
Published 17 December 2024 Volume 2024:18 Pages 3837—3851
DOI https://doi.org/10.2147/OPTH.S489114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Laila Salah Aldokhail,1 Abdulaziz Mohammad Alhadlaq,2 Lujain Mohamed Alaradi,1 Lamees Mohamed Alaradi,1 Fatimah Yaseen AlShaikh1
1Department of Ophthalmology, College of Medicine, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 2Division of Ophthalmology, Security Forces Hospital, Riyadh, Saudi Arabia, Ophthalmology Department, College of Medicine, Qassim university, Qassim, Saudi Arabia
Correspondence: Laila Salah Aldokhail, Department of Ophthalmology, College of Medicine, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia, Email [email protected]
Background: Anti-vascular endothelial growth factor (anti-VEGF) therapy has revolutionized the management of various ocular conditions, including diabetic macular edema (DME), retinal vein occlusion (RVO)-related macular edema (ME), and neovascular age-related macular degeneration (nAMD). However, there remains a need to systematically assess its effectiveness across these distinct conditions.
Methodology: A systematic review was conducted to identify studies evaluating the efficacy of anti-VEGF therapy in improving ocular outcomes in patients with DME, RVO-related ME, and nAMD. PubMed, Embase, and Cochrane Library databases were searched for relevant articles published up to 2024. Studies meeting the inclusion criteria were critically appraised, and data on the proportion of patients gaining ≥ 15 Early Treatment Diabetic Retinopathy Study (ETDRS) letters in best-corrected visual acuity (BCVA), mean change in BCVA (ETDRS letters), and reduction in central macular thickness (CMT) (μm) were extracted and synthesized.
Results: The systematic review identified 18 studies comprising randomized controlled trials, prospective studies, retrospective analyses, and observational studies. Anti-VEGF therapy demonstrated efficacy across all three conditions, with varying proportions of patients experiencing improvements in BCVA and reductions in CMT. Notably, the proportion of patients gaining ≥ 15 ETDRS letters ranged from 18.1% to 44.8% in DME, while mean changes in BCVA ranged from +4.2 letters to +21.4 letters in RVO-related ME and nAMD. Reductions in CMT ranged from 183.1 μm to 294 μm in DME and RVO-related ME.
Conclusion: Anti-VEGF therapy represents a cornerstone in the management of DME, RVO-related ME, and nAMD, with significant improvements observed in BCVA and reductions in CMT across diverse patient populations. While our findings support the effectiveness of anti-VEGF therapy in improving ocular outcomes, further research is warranted to compare its efficacy with alternative treatment modalities and to elucidate its long-term safety profile.
Keywords: outcomes, anti-VEGF, diabetic macular edema, retinal vein occlusion, neovascular AMD
Introduction
Diabetic macular edema (DME), vein occlusion-related macular edema (VME), and neovascular age-related macular degeneration (nAMD) are prevalent sight-threatening conditions globally, posing significant challenges to patients and healthcare systems alike.1,2 Among the leading causes of visual impairment and blindness, these diseases manifest through complex pathophysiological mechanisms, often resulting in macular edema and neovascularization, ultimately compromising visual function.3
In recent decades, the advent of anti-vascular endothelial growth factor (anti-VEGF) therapy has revolutionized the management of these conditions, offering promising avenues for preserving and, in some cases, improving visual acuity.4,5 By targeting the pathological angiogenic processes underlying DME, VME, and nAMD, anti-VEGF agents have emerged as cornerstone treatments, demonstrating efficacy in reducing macular edema, preventing disease progression, and, in many instances, restoring visual function.5,6
However, despite the widespread adoption of anti-VEGF therapy in clinical practice, the literature remains replete with studies reporting variable outcomes, leading to a need for comprehensive evaluation and synthesis of available evidence. Therefore, this systematic review and meta-analysis aim to critically appraise the outcomes of anti-VEGF therapy in eyes afflicted with DME, VME, and nAMD. By synthesizing data from randomized controlled trials (RCTs) and observational studies, we seek to assess the impact of anti-VEGF agents on key visual and anatomical parameters, including best-corrected visual acuity (BCVA), central macular thickness (CMT), and rates of disease recurrence or progression. Additionally, we aim to explore potential variations in treatment response across different anti-VEGF agents, treatment regimens, and patient subgroups. Through this comprehensive analysis, we endeavor to provide clinicians, researchers, and policymakers with a robust evidence base to inform clinical decision-making, optimize treatment strategies, and enhance patient outcomes in the management of DME, VME, and nAMD.
Materials and Methods
For this systematic review, an extensive search strategy was implemented across multiple databases, including PubMed, Medline, Google Scholar, Embase, and Web of Science. The strategy aimed to identify relevant studies examining the use of anti-vascular endothelial growth factor (anti-VEGF) therapy in the management of various ocular conditions, encompassing diabetic macular edema (DME), branch retinal vein occlusion-related macular edema (BRVO-ME), central retinal vein occlusion-related macular edema (CRVO-ME), and neovascular age-related macular degeneration (nAMD). The search strategy was developed in accordance with established guidelines for systematic reviews and utilized a combination of keywords and Medical Subject Headings (MeSH) terms related to the target conditions and interventions.
The inclusion criteria for study selection were predefined based on the Population, Intervention, Comparator, Outcome, and Study design (PICOS) framework. Only studies involving adult patients (aged 18 and older) diagnosed with DME, BRVO-ME, CRVO-ME, or nAMD who received anti-VEGF therapy (eg, bevacizumab, ranibizumab, aflibercept) as the primary treatment were considered eligible for inclusion. Studies were required to report quantitative data on visual acuity outcomes (eg, best-corrected visual acuity) and/or anatomical changes (eg, central retinal thickness). Additionally, eligible studies had to have a minimum follow-up duration of six months. Studies not meeting these criteria or focusing on unrelated interventions or populations were excluded. In addition, case studies, conference, reviews, and those studies without excess to full text were excluded. The search strategy was tailored to each database’s unique syntax and filters, ensuring comprehensive coverage while minimizing duplication of results.
Following the search strategy implementation, identified articles underwent a two-stage screening process by two independent reviewers. In the initial stage, titles and abstracts were screened based on predefined eligibility criteria. Full-text articles were retrieved for further assessment if they met the initial screening criteria or if there was uncertainty. In the second stage, full-text articles were independently reviewed by the same two reviewers to determine their final eligibility for inclusion in the systematic review. Any discrepancies between reviewers were resolved through discussion or consultation with a third reviewer if necessary.
Data extraction was conducted by one reviewer using a standardized data extraction form and verified by a second reviewer for accuracy. Extracted data included study characteristics, participant demographics, intervention details, outcome measures, and key methodological information. The extracted data were synthesized narratively, focusing on key findings and trends across included studies.
Risk of bias assessments were performed for included studies using established tools such as the Cochrane Risk of Bias tool for randomized controlled trials (RCTs) and the Newcastle-Ottawa Scale for observational studies. Two independent reviewers conducted the assessments, with discrepancies resolved through discussion or consultation with a third reviewer if needed. The synthesis of data involved narrative synthesis of study findings and, if appropriate, meta-analysis to provide pooled effect estimates. Subgroup analyses were conducted to explore potential sources of heterogeneity and assess treatment effects in specific subgroups based on ocular condition, anti-VEGF agent, and study design.
Results
Our search yielded a total of 753 publications, from which duplicate studies were identified and removed by screening the titles, resulting in a reduced pool of 312 articles (Figure 1). Upon further scrutiny of abstracts to eliminate duplicate and irrelevant data not aligned with the scope of our review, an additional 163 articles were excluded. Subsequently, 149 full-length articles underwent thorough evaluation, leading to the exclusion of 131 articles due to overlapping or inconclusive data. Ultimately, 18 pertinent studies meeting our inclusion criteria were included in the final review.
 |
Figure 1 The PRISMA figures showing the steps to choose the studies for systematic review. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLOS Med. 2021;18(3): e1003583.7 |
The systematic review identified a total of 18 studies meeting the inclusion criteria, comprising randomized controlled trials (RCTs),8–11 prospective studies,12–18 retrospective analyses,19–22 and observational studies.20,23,24 These studies investigated the efficacy of anti-vascular endothelial growth factor (anti-VEGF) therapy in the management of various ocular conditions, including diabetic macular edema (DME),8–10,19,20 macular edema secondary to central retinal vein occlusion (CRVO-ME) and branch retinal vein occlusion (BRVO),11–16,21,24 and neovascular age-related macular degeneration (nAMD).17,18,22,23,25
Among the included studies, several Phase III randomized controlled trials (RCTs) evaluated the efficacy of ranibizumab and aflibercept in the treatment of DME. Brown et al8 conducted a Phase III RCT involving 759 adults with DME, comparing ranibizumab at doses of 0.5 mg or 0.3 mg versus sham injection. Similarly, Nguyen et al9 investigated ranibizumab (0.5 mg or 0.3 mg) versus sham injection in 377 adults with DME. Korobelink et al10 conducted a Phase III RCT comparing intravitreal aflibercept injection (IAI) versus macular laser in 872 patients with DME involving the central macula.
In addition to RCTs, retrospective analyses and observational studies provided insights into real-world outcomes of anti-VEGF therapy in diverse patient populations. Ciulla et al4 conducted a retrospective analysis involving 28,568 treatment-naïve patients with diabetic macular edema (DMO), reporting on the mean change in best-corrected visual acuity (BCVA) at 1 year following anti-VEGF injections. Similarly, Gurung et al20 conducted a retrospective observational study assessing improvement in BCVA and central macular thickness (CMT) after 12 months of treatment with various intravitreal anti-VEGF agents for DME.
Studies focusing on macular edema secondary to central retinal vein occlusion (CRVO-ME) also contributed to the evidence base. Heier et al11 conducted a randomized, double-masked, Phase III trial involving 188 patients with CRVO-ME, evaluating the efficacy of intravitreal aflibercept injection (IAI) in improving BCVA, reducing central retinal thickness, and determining the number of pro re nata (PRN) injections required.
Furthermore, studies explored the efficacy of anti-VEGF therapy in diverse settings and patient populations. Brown et al12 conducted a prospective, phase I/II clinical trial assessing the efficacy of monthly intravitreal ranibizumab treatment for eyes at high risk of neovascular complications. Brynskov et al13 conducted a prospective study evaluating the efficacy of intravitreal ranibizumab in patients diagnosed with branch retinal vein occlusion (BRVO) and central retinal vein occlusion (CRVO), reporting on mean change in ETDRS letters and reduction in foveal center point thickness.
Additionally, interventional case series and comparative studies provided insights into novel treatment modalities and comparative effectiveness. Eldeeb et al24 conducted an interventional case series investigating the efficacy of intravitreal Ziv-aflibercept in patients with CRVO-ME, reporting on mean change in log MAR visual acuity and reduction in central macular thickness. Lotfy et al15 conducted a prospective, comparative, randomized, interventional study comparing intravitreal aflibercept versus bevacizumab in patients with macular edema secondary to CRVO, reporting on mean change in central foveal thickness and BCVA.
Moreover, retrospective studies and population-based cohort studies provided real-world insights into treatment outcomes and patterns of care. Khan et al21 conducted a retrospective study comparing intravitreal ranibizumab versus bevacizumab in treatment-naïve patients with macular edema secondary to retinal vein occlusion (RVO), assessing changes in visual acuity and central subfield thickness. Gurung et al25 conducted a real-life population-based cohort study assessing visual outcomes and injection patterns in patients with neovascular AMD receiving intravitreal anti-VEGF drugs.
Finally, multistate modeling studies and prospective studies provided long-term insights into treatment outcomes and disease progression. Finger et al23 conducted a multistate modeling study using real-world cohort data to assess visual acuity in patients with nAMD treated in routine eye clinics, providing insights into visual outcomes over the remaining lifetime. Lukacs et al18 conducted a prospective study evaluating the efficacy of intensive aflibercept and ranibizumab anti-VEGF therapy in patients with exudative AMD, reporting on best-corrected visual acuity, macular atrophy, and disease activity (Table 1).
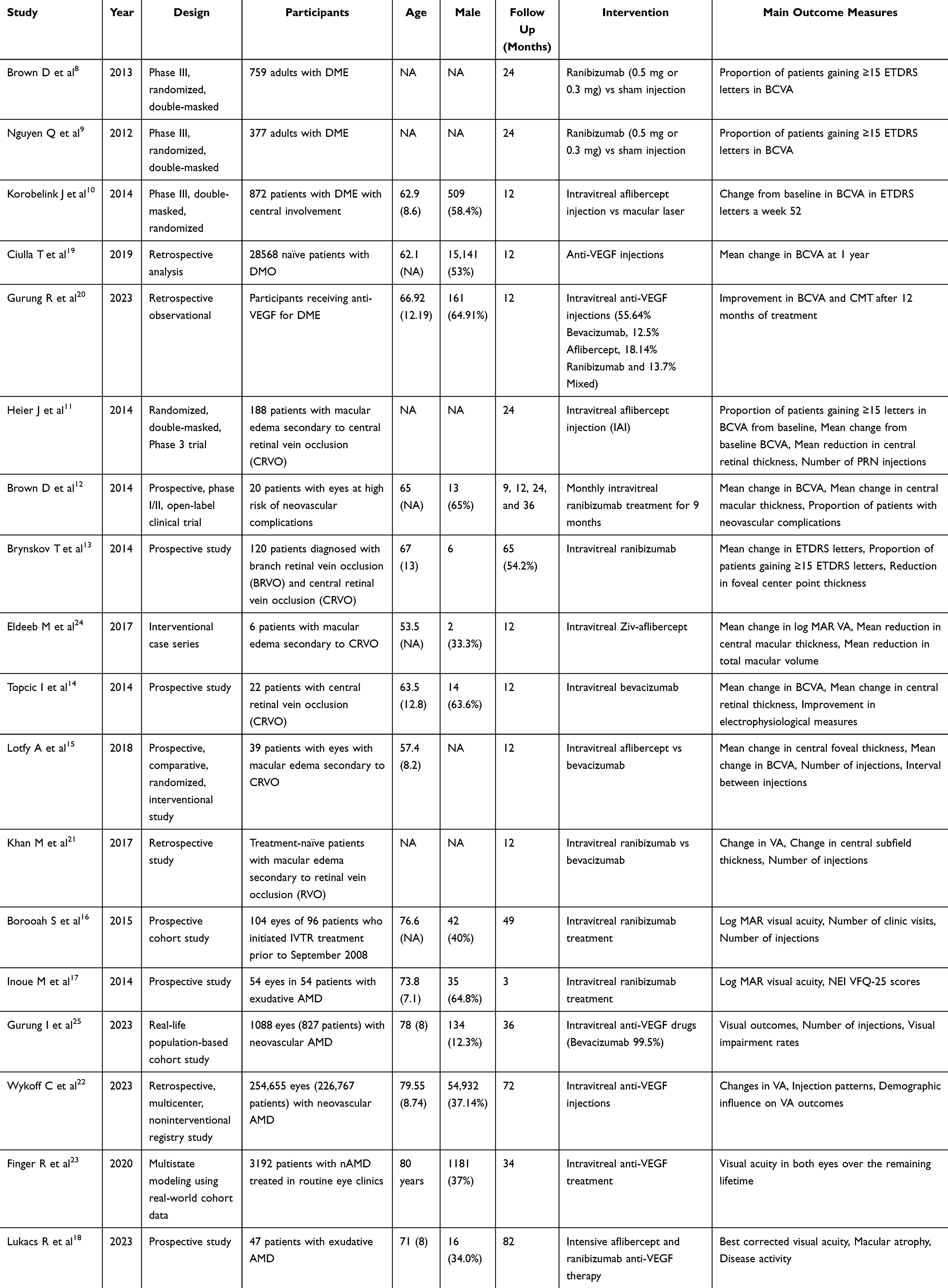 |
Table 1 General Characteristics of the Included Studies |
The results of the studies showed a wide range of outcomes in terms of the proportion of patients gaining ≥15 Early Treatment Diabetic Retinopathy Study (ETDRS) letters in best-corrected visual acuity (BCVA), mean change in BCVA (in ETDRS letters), and reduction in central macular thickness (CMT) in micrometers (μm). In the study by Brown et al, the proportion of patients gaining ≥15 ETDRS letters ranged from 19.2% to 41.6%, with a mean change in BCVA ranging from 2.8 to 11.1 ETDRS letters. They also reported a sustained reduction in CMT.8 Nguyen et al observed a proportion of patients gaining ≥15 ETDRS letters ranging from 18.1% to 44.8%. However, specific values for mean change in BCVA and reduction in CMT were not specified in their study.9 Korobelink et al reported a proportion of patients gaining ≥15 ETDRS letters ranging from 41.6% to 32.4%, with a mean change in BCVA ranging from 10.5 to 12.5 ETDRS letters. They also observed reductions in CMT ranging from 183.1 to 195.0 μm.10 Ciulla et al documented a mean change in BCVA of +4.2 letters, with a linear relationship observed with injections beyond two injections.19 In the study by Gurung et al, specific proportions of patients gaining ≥15 ETDRS letters were not specified. However, they reported a significant improvement of 3.6 ETDRS letters (± 10.99) in BCVA and a significant reduction of 3.6 ETDRS letters (± 10.99) in CMT.20 In general, considering the effectiveness of Anti-VEGF in the treatment of diabetic macular edema, it was found that Anti-VEGF was associated with gaining ≥15 Early ETDRS letters in best-corrected visual acuity (BCVA) in 18.1%-44.8% of all patients, with significant improvement in BCVA and CMT.
The results from studies assessing the effect of treatment on Vein Occlusion-Related Macular Edema (ME) varied across different parameters. Heier et al observed that patients receiving Intravitreal Aflibercept Injection (IAI) 2Q4+PRN had a higher proportion of gaining ≥15 Early Treatment Diabetic Retinopathy Study (ETDRS) letters in best-corrected visual acuity (BCVA) compared to those receiving Sham+IAI PRN. Additionally, they noted significant improvements in mean change in BCVA and reductions in central macular thickness (CMT) over the course of the study.11 Brown et al reported substantial improvements in BCVA at 9 and 36 months, along with reductions in CMT, particularly notable after pro re nata ranibizumab retreatment.12 Brynskov et al found varying proportions of patients gaining ≥15 ETDRS letters between branch retinal vein occlusion (BRVO) and central retinal vein occlusion (CRVO) groups. Both groups experienced improvements in mean change in BCVA, alongside reductions in foveal center point thickness.13 Eldeeb et al documented improvements in log MAR visual acuity and reductions in CMT over a 12-month period. Topcic et al observed significant improvements in BCVA over time, accompanied by a decrease in central retinal thickness following treatment.24 Lotfy et al noted reductions in CMT in both aflibercept and bevacizumab treatment groups, with variations in the number of injections and intervals between injections.15 Khan et al did not find notable differences in outcomes between intravitreal ranibizumab (IVR) and intravitreal bevacizumab (IVB) for ME from retinal vein occlusion (RVO) in routine clinical practice.21 Borooah et al reported a mean loss of letters over the study period without specifying further details regarding changes in BCVA or CMT.16
In studies assessing the impact of interventions on nAMD, Inoue et al found significant improvements in the postoperative NEI VFQ-25 mean composite score, indicating better visual function following treatment. However, specific data regarding the proportion of patients gaining ≥15 Early Treatment Diabetic Retinopathy Study (ETDRS) letters in best-corrected visual acuity (BCVA) or reductions in central macular thickness (CMT) were not specified.17 Gurung et al did not provide details on the mean change in BCVA or reductions in CMT, but they reported that 35% of patients experienced an improvement in BCVA.20 Wykoff et al reported a mean increase of 3.0 ETDRS letters in BCVA at year 1 but noted a net loss of 4.6 letters from baseline after 6 years. They also investigated factors such as injection frequency, treatment discontinuations, and demographic influences on visual acuity (VA).22 Finger et al focused on the long-term visual acuity outcomes in both eyes over the remaining lifetime without specifying details on specific visual acuity changes or anatomical improvements.23 Lukacs et al reported that 55% of patients had stable or improved BCVA (with ≤ 10 letters lost). However, they did not provide further information regarding mean changes in BCVA, macular atrophy, or disease activity18 (Table 2).
 |
Table 2 Outcomes of Using Anti-VEGF in Different Ocular Condition |
Bias Risk Assessment
The risk of bias assessment for the included studies revealed varying levels of methodological rigor. Among the randomized controlled trials (RCTs), such as those by Brown et al,8 Nguyen et al,9 and Korobelink et al,10 the overall risk of bias was low across most domains. These studies demonstrated adequate randomization procedures, allocation concealment, and blinding, thereby reducing the risks of selection, performance, and detection biases. Additionally, their complete reporting of outcomes and low attrition rates supported the reliability of their findings.
Conversely, the retrospective and observational studies exhibited higher risks of bias, particularly due to their study designs. Studies like Ciulla et al,19 Gurung et al,20 and Wykoff et al22 were rated as high risk due to potential selection bias, performance bias, and the presence of uncontrolled confounding factors. Retrospective studies inherently lack randomization, increasing the likelihood of baseline differences between treatment groups influencing outcomes. Furthermore, the absence of blinding in these studies could lead to performance and detection biases, where subjective outcomes like visual acuity may be inadvertently influenced by patient or investigator expectations.
In terms of confounding factors, prospective cohort studies such as those by Borooah et al16 and Inoue et al17 showed moderate risks, primarily due to the possibility of unmeasured confounding variables affecting the results. Moreover, real-world cohort studies and registry-based analyses, such as Finger et al23 and Gurung et al,25 were susceptible to biases related to the representativeness of the included population and the accuracy of recorded outcomes (Table 3).
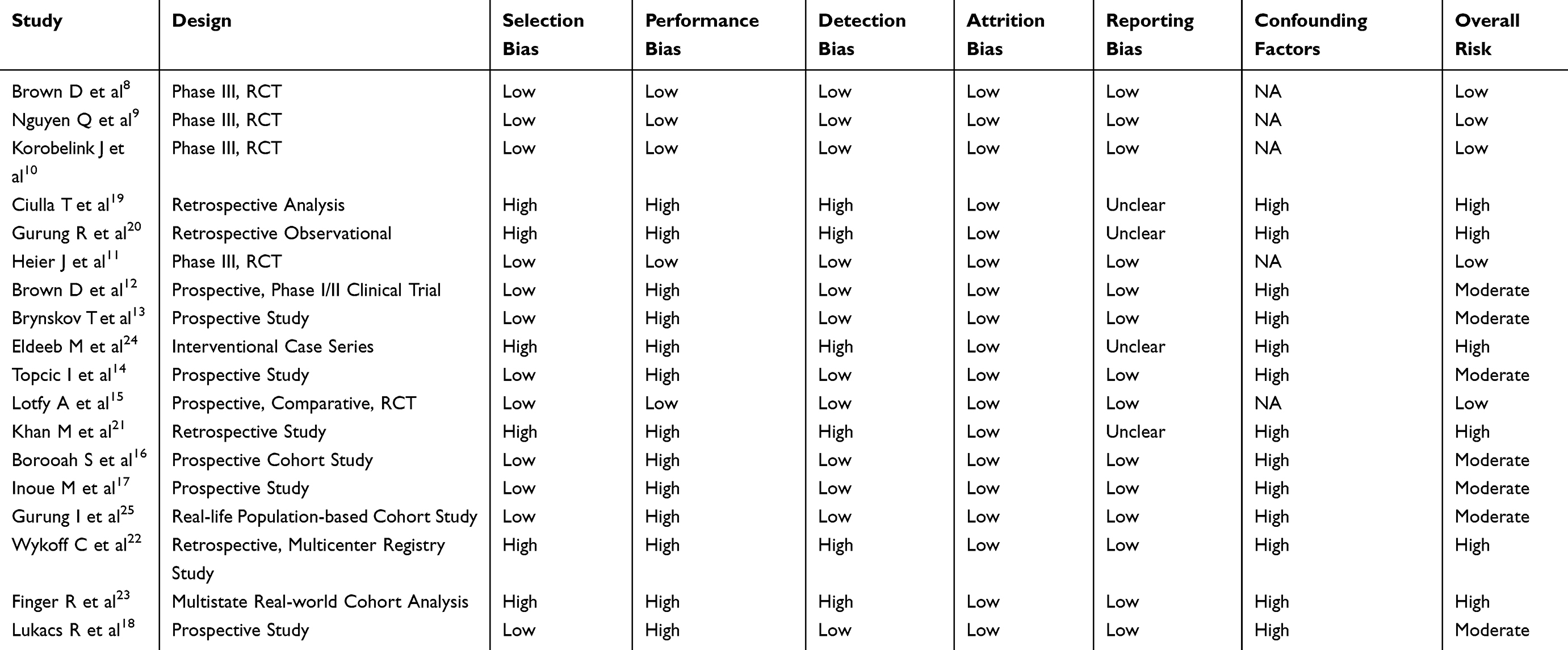 |
Table 3 Bias Risk Assessment Using Cochrane Risk of Bias Tool |
Discussion
The treatment landscape for various ocular conditions, including diabetic macular edema (DME), macular edema secondary to retinal vein occlusion (RVO), and neovascular age-related macular degeneration (nAMD), has evolved significantly with the advent of anti-vascular endothelial growth factor (anti-VEGF) therapy. We aim to provide insights into the role of anti-VEGF therapy in optimizing visual outcomes and improving quality of life for patients with DME, RVO, and nAMD.
Diabetic macular edema (DME) is a common complication of diabetes mellitus and a leading cause of vision loss in diabetic patients.26,27 It occurs due to the accumulation of fluid in the macula, the central part of the retina responsible for detailed vision.1,28 This accumulation of fluid leads to retinal thickening and impairment of vision.1 Patients with DME often experience symptoms such as blurred vision, difficulty reading, and distortion of straight lines.29
Our findings from the included studies demonstrate the effectiveness of anti-vascular endothelial growth factor (anti-VEGF) therapy in improving ocular symptoms in patients with DME. Phase III randomized controlled trials (RCTs) comparing anti-VEGF agents such as ranibizumab and aflibercept with sham injection or laser treatment consistently showed significant improvements in best-corrected visual acuity (BCVA) and reductions in central macular thickness (CMT). For example, Brown et al and Nguyen et al reported significant increases in the proportion of patients gaining ≥15 Early Treatment Diabetic Retinopathy Study (ETDRS) letters in BCVA and reductions in CMT following anti-VEGF treatment compared to sham injection or laser treatment.8,9
Comparative studies have also suggested that anti-VEGF therapy may be superior to other treatment modalities, such as laser therapy, in improving visual outcomes in patients with DME.6,20,30 In a previous systematic and meta-analysis, Li G et al, 2023 showed that Faricimab showed no significant difference considering adverse events with a significant difference for CST (MD = −22.41, 95% CI [−29.95 to −14.86], P < 0.00001) and the number of injections (MD = −0.93, 95% CI [−1.33 to −0.54], P < 0.00001).31 While laser therapy has been a traditional treatment option for DME, it is associated with potential complications such as scarring and visual field loss.32–34 In contrast, anti-VEGF therapy targets the underlying pathophysiology of DME by inhibiting vascular endothelial growth factor, leading to improvements in macular edema and visual function.6 This is similar to what reported in a recent meta-analysis conducted by Chen J et al who reported that anti-VEGF therapy had better improvement in BCVA than laser photocoagulation or combination therapy, with no difference considering CMT at 6 months.35
The observed improvements in ocular symptoms with anti-VEGF therapy can be attributed to its ability to reduce vascular permeability and inhibit the growth of abnormal blood vessels in the retina.36,37 By targeting the underlying angiogenic and inflammatory processes involved in DME, anti-VEGF agents help restore the integrity of the blood-retinal barrier and reduce fluid leakage into the macula.6 Additionally, anti-VEGF therapy may have neuroprotective effects, preserving retinal function and preventing further vision loss in patients with DME.38
Central retinal vein occlusion-macular edema (CRVO-ME) and branch retinal vein occlusion-macular edema (BRVO-ME) are retinal vascular disorders characterized by impaired venous outflow and macular edema.39,40 These conditions result in decreased retinal perfusion, ischemia, and the release of pro-inflammatory cytokines, leading to the accumulation of fluid in the macula and visual impairment.41 Patients with CRVO-ME and BRVO-ME often present with symptoms such as decreased visual acuity, metamorphopsia, and central scotomas.42
Our findings indicate that anti-VEGF therapy is effective in improving ocular symptoms in patients with CRVO-ME and BRVO-ME. Phase III randomized controlled trials (RCTs) evaluating the efficacy of intravitreal aflibercept injection (IAI) in patients with CRVO-ME consistently demonstrated significant improvements in visual acuity and reductions in central retinal thickness compared to sham injection or laser treatment.11 Similarly, Brynskov et al reported improvements in visual acuity and reductions in foveal center point thickness following intravitreal ranibizumab treatment in patients with BRVO-ME.13
Comparative studies have suggested that anti-VEGF therapy may be superior to other treatment modalities, such as macular laser therapy or corticosteroids, in improving visual outcomes in patients with CRVO-ME and BRVO-ME.43–45 While laser therapy and corticosteroids have been used in the management of these conditions, they are associated with limited efficacy and potential side effects. In contrast, anti-VEGF therapy targets the underlying angiogenic and inflammatory processes involved in CRVO-ME and BRVO-ME, leading to reductions in macular edema and improvements in visual function.46
The observed improvements in ocular symptoms with anti-VEGF therapy may be attributed to its ability to reduce vascular permeability, inhibit neovascularization, and improve retinal perfusion in patients with CRVO-ME and BRVO-ME.44,47 By blocking the activity of vascular endothelial growth factor (VEGF), anti-VEGF agents help restore the integrity of the blood-retinal barrier and reduce fluid leakage into the macula.48,49 Additionally, anti-VEGF therapy may have anti-inflammatory effects, reducing the release of inflammatory mediators and cytokines that contribute to macular edema and retinal damage.50
Neovascular age-related macular degeneration (nAMD) is a progressive retinal disorder characterized by the growth of abnormal blood vessels beneath the macula, leading to retinal damage and vision loss.51,52 Patients with nAMD often experience symptoms such as central vision distortion, visual field defects, and difficulty reading or recognizing faces.53
Our findings suggest that anti-VEGF therapy is effective in improving ocular symptoms in patients with nAMD. Phase III randomized controlled trials (RCTs) evaluating the efficacy of anti-VEGF agents such as ranibizumab and aflibercept in patients with nAMD consistently demonstrated significant improvements in visual acuity and reductions in macular thickness compared to placebo or photodynamic therapy (PDT).17,22 Additionally, Lukacs et al reported that a majority of patients with nAMD receiving intensive aflibercept and ranibizumab anti-VEGF therapy had stable or improved visual acuity over the study period.18
Comparative studies have indicated that anti-VEGF therapy may be superior to other treatment modalities, such as PDT or corticosteroids, in improving visual outcomes in patients with nAMD.54,55 While PDT and corticosteroids have been used in the management of nAMD, they are associated with limited efficacy and potential side effects.56,57 In contrast, anti-VEGF therapy targets the underlying angiogenic and inflammatory processes involved in nAMD, leading to reductions in abnormal vessel growth and improvements in visual function.58
The observed improvements in ocular symptoms with anti-VEGF therapy may be attributed to its ability to inhibit neovascularization, reduce vascular leakage, and improve retinal perfusion in patients with nAMD.5 By blocking the activity of vascular endothelial growth factor (VEGF), anti-VEGF agents help normalize retinal vasculature and reduce the risk of choroidal neovascularization.59 Additionally, anti-VEGF therapy may have anti-inflammatory effects, reducing retinal inflammation and preserving retinal function in patients with nAMD.59
Despite the comprehensive nature of our review, several limitations should be acknowledged. Firstly, the limited number of included studies (18 in total) constrains the breadth of evidence available, which may restrict the robustness of our conclusions. This relatively small sample of studies also raises concerns about the generalizability of the findings to broader patient populations. In addition, the heterogeneity among the included studies presents a significant challenge in synthesizing the evidence. The studies varied widely in terms of study design (randomized controlled trials, observational studies, and retrospective analyses), patient characteristics (age, baseline visual acuity, comorbidities), treatment protocols (dosing frequency, anti-VEGF agents used), and follow-up durations. Such variability not only limits the comparability of outcomes but may also obscure true treatment effects, thereby impacting the overall validity of the pooled findings. For instance, differences in dosing regimens and follow-up durations across studies could lead to inconsistencies in reported visual and anatomical outcomes, making it challenging to draw definitive conclusions on optimal treatment strategies. Additionally, the majority of studies included in our review were observational or retrospective in nature, which inherently carry a risk of bias and confounding factors that may impact the validity of the results. Potential biases, such as selection bias in non-randomized studies and performance bias due to inconsistent administration of interventions, could distort the true effect of anti-VEGF therapy. Furthermore, confounding factors related to patients’ demographic and clinical profiles, such as the presence of comorbid conditions or prior treatments, may influence the reported outcomes. Moreover, the reliance on published literature introduces the possibility of publication bias, where studies reporting positive outcomes are more likely to be published than those with null or negative findings. This bias can lead to an overestimation of the benefits of anti-VEGF therapy and limit the comprehensiveness of our analysis.
Furthermore, while anti-VEGF therapy emerged as a promising treatment modality across DME, RVO, and nAMD, our review did not directly compare its efficacy with alternative treatment modalities such as corticosteroids or laser therapy. Therefore, we cannot definitively conclude the superiority of anti-VEGF therapy over other interventions based on the included studies. Additionally, the long-term safety profile and potential adverse effects of anti-VEGF therapy were not comprehensively addressed in this review, warranting further investigation. Lastly, the scope of our review was limited to studies published up to the date of our search, and new evidence may have emerged since then that could impact the conclusions drawn from our review. Despite these limitations, our study provides valuable insights into the effectiveness of anti-VEGF therapy in improving ocular outcomes across a range of retinal conditions, highlighting its role as a cornerstone in contemporary ophthalmic practice.
Despite these limitations, our study provides valuable insights into the effectiveness of anti-VEGF therapy in improving ocular outcomes across a range of retinal conditions, reinforcing its role as a cornerstone in contemporary ophthalmic practice. For future research, we recommend a focus on large-scale, multicenter randomized controlled trials to establish more definitive conclusions regarding the optimal dosing regimens, comparative effectiveness of different anti-VEGF agents, and the long-term safety profile of these therapies. From a clinical practice perspective, adopting individualized treatment protocols based on patient characteristics and response to therapy may enhance visual and anatomical outcomes. Additionally, integrating real-world data from diverse patient populations would provide a more comprehensive understanding of treatment efficacy and safety, ultimately guiding evidence-based clinical decision-making.
Conclusion
In conclusion, our comprehensive review of studies evaluating the efficacy of anti-VEGF therapy across diabetic macular edema (DME), macular edema secondary to retinal vein occlusion (RVO), and neovascular age-related macular degeneration (nAMD) emphasizes the significant strides made in improving visual outcomes for patients with these sight-threatening conditions. Across the spectrum of diseases, anti-VEGF therapy demonstrated notable efficacy in improving best-corrected visual acuity (BCVA) and reducing central macular thickness (CMT), thereby addressing key markers of disease severity and progression. Moreover, our findings suggest that anti-VEGF therapy represents a cornerstone in the management of these conditions, offering a robust therapeutic option for patients where conventional treatments may have fallen short. Importantly, the real-world data presented in our review align with findings from randomized controlled trials, affirming the broader applicability and effectiveness of anti-VEGF therapy in routine clinical practice.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang J, Zhang J, Zhang C, et al. Diabetic macular edema: current understanding, molecular mechanisms and therapeutic implications. Cells. 2022;11(21):3362. doi:10.3390/cells11213362
2. Kim JE. Exploring neovascular age-related macular degeneration and diabetic macular edema and advances in treatment. Am J Manag Care. 2022;28(Suppl 3):S35–S43. doi:10.37765/ajmc.2022.88853
3. Li Y, Liu Y, Liu S, et al. Diabetic vascular diseases: molecular mechanisms and therapeutic strategies. Signal Transduct Target Ther. 2023;8(1):152. doi:10.1038/s41392-023-01400-z
4. Hang A, Feldman S, Amin AP, Ochoa JAR, Park SS. intravitreal anti-vascular endothelial growth factor therapies for retinal disorders. Pharmaceuticals. 2023;16(8):1140. doi:10.3390/ph16081140
5. Khachigian LM, Liew G, Teo KYC, Wong TY, Mitchell P. Emerging therapeutic strategies for unmet need in neovascular age-related macular degeneration. J Transl Med. 2023;21(1):133. doi:10.1186/s12967-023-03937-7
6. Cheema AA, Cheema HR. Diabetic macular edema management: a review of anti-Vascular Endothelial Growth Factor (VEGF) therapies. Cureus. 2024. doi:10.7759/cureus.52676
7. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. PLoS Medicine. 2021;18(3):e1003583. doi:10.1371/journal.pmed.1003583
8. Brown DM, Nguyen QD, Marcus DM, et al. Long-term outcomes of ranibizumab therapy for diabetic macular edema: the 36-month results from two phase iii trials. Ophthalmology. 2013;120(10):2013–2022. doi:10.1016/j.ophtha.2013.02.034
9. Nguyen QD, Brown DM, Marcus DM, et al. Ranibizumab for diabetic macular edema. Ophthalmology. 2012;119(4):789–801. doi:10.1016/j.ophtha.2011.12.039
10. Korobelnik J-F, Do D V, Schmidt-Erfurth U, et al. Intravitreal aflibercept for diabetic macular edema. Ophthalmology. 2014;121(11):2247–2254. doi:10.1016/j.ophtha.2014.05.006
11. Heier JS, Clark WL, Boyer DS, et al. Intravitreal aflibercept injection for macular edema due to central retinal vein occlusion. Ophthalmology. 2014;121(7):1414–1420.e1. doi:10.1016/j.ophtha.2014.01.027
12. Brown DM, Wykoff CC, Wong TP, Mariani AF, Croft DE, Schuetzle KL. Ranibizumab in preproliferative (Ischemic) central retinal vein occlusion. Retina. 2014;34(9):1728–1735. doi:10.1097/IAE.0000000000000191
13. Brynskov T, Kemp H, Sørensen TL. Intravitreal ranibizumab for retinal vein occlusion through 1 year in clinical practice. Retina. 2014;34(8):1637–1643. doi:10.1097/IAE.0000000000000111
14. Gardašević Topčić I, Šuštar M, Brecelj J, Hawlina M, Jaki Mekjavić P. Morphological and electrophysiological outcome in prospective intravitreal bevacizumab treatment of macular edema secondary to central retinal vein occlusion. Doc Ophthalmol. 2014;129(1):27–38. doi:10.1007/s10633-014-9445-y
15. Lotfy A, Solaiman KAM, Abdelrahman A, Samir A. Efficacy and frequency of intravitreal aflibercept versus bevacizumab for macular edema secondary to central retinal vein occlusion. Retina. 2018;38(9):1795–1800. doi:10.1097/IAE.0000000000001782
16. Borooah S, Jeganathan VS, Ambrecht A-M, et al. Long-term visual outcomes of intravitreal ranibizumab treatment for wet age-related macular degeneration and effect on blindness rates in south-east Scotland. Eye. 2015;29(9):1156–1161. doi:10.1038/eye.2015.83
17. Inoue M, Arakawa A, Yamane S, Kadonosono K. Intravitreal injection of ranibizumab using a pro re nata regimen for age-related macular degeneration and vision-related quality of life. Clin Ophthalmol. 2014;8:1711. doi:10.2147/OPTH.S68293
18. Lukacs R, Schneider M, Nagy ZZ, et al. Seven-year outcomes following intensive anti-vascular endothelial growth factor therapy in patients with exudative age-related macular degeneration. BMC Ophthalmol. 2023;23(1):110. doi:10.1186/s12886-023-02843-2
19. Ciulla TA, Pollack JS, Williams DF. Visual acuity outcomes and anti-VEGF therapy intensity in diabetic macular oedema: a real-world analysis of 28 658 patient eyes. Br J Ophthalmol. 2021;105(2):216–221. doi:10.1136/bjophthalmol-2020-315933
20. Gurung RL, FitzGerald LM, Liu E, et al. Predictive factors for treatment outcomes with intravitreal anti-vascular endothelial growth factor injections in diabetic macular edema in clinical practice. Int J Retin Vitr. 2023;9(1):23. doi:10.1186/s40942-023-00453-0
21. Khan M, Wai KM, Silva FQ, et al. Comparison of ranibizumab and bevacizumab for macular edema secondary to retinal vein occlusions in routine clinical practice. Ophthalmic Surg Lasers Imaging Retina. 2017;48(6):465–472. doi:10.3928/23258160-20170601-04
22. Wykoff CC, Garmo V, Tabano D, et al. Impact of anti-VEGF treatment and patient characteristics on vision outcomes in neovascular age-related macular degeneration. Ophthalmol Sci. 2024;4(2):100421. doi:10.1016/j.xops.2023.100421
23. Finger RP, Puth M-T, Schmid M, Barthelmes D, Guymer RH, Gillies M. Lifetime outcomes of anti–vascular endothelial growth factor treatment for neovascular age-related macular degeneration. JAMA Ophthalmol. 2020;138(12):1234. doi:10.1001/jamaophthalmol.2020.3989
24. Eldeeb M, Chan EW, Dedhia CJ, Mansour A, Chhablani J. One-year outcomes of ziv-aflibercept for macular edema in central retinal vein occlusion. Am J Ophthalmol Case Rep. 2017;8:58–61. doi:10.1016/j.ajoc.2017.10.011
25. Korva-Gurung I, Kubin A-M, Ohtonen P, Hautala N. Visual outcomes of anti-VEGF treatment on neovascular age-related macular degeneration: a Real-World Population-Based Cohort Study. Pharmaceuticals. 2023;16(7):927. doi:10.3390/ph16070927
26. Romero-Aroca P. Managing diabetic macular edema: the leading cause of diabetes blindness. World J Diabetes. 2011;2(6):98. doi:10.4239/wjd.v2.i6.98
27. Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis. 2015;2(1):17. doi:10.1186/s40662-015-0026-2
28. Musat O, Cernat C, Labib M, et al. Diabetic macular edema. Rom J Ophthalmol. 2015;59(3):133–136.
29. Yoshizumi H, Ejima T, Nagao T, Wakisaka M. Recovery from diabetic macular edema in a diabetic patient after minimal dose of a sodium glucose co-transporter 2 inhibitor. Am J Case Rep. 2018;19:462–466. doi:10.12659/AJCR.909708
30. Chi S-C, Kang Y-N, Huang Y-M. Efficacy and safety profile of intravitreal dexamethasone implant versus antivascular endothelial growth factor treatment in diabetic macular edema: a systematic review and meta-analysis. Sci Rep. 2023;13(1):7428. doi:10.1038/s41598-023-34673-z
31. Li G, Zhu N, Ji A. Comparative efficacy and safety of faricimab and other anti-VEGF therapy for age-related macular degeneration and diabetic macular edema: a systematic review and meta-analysis of randomized clinical trials. Medicine. 2023;102(50):e36370. doi:10.1097/MD.0000000000036370
32. Romero-Aroca P, Reyes-Torres J, Baget-Bernaldiz M, Blasco-Sune C. Laser treatment for diabetic macular edema in the 21st century. Curr Diabetes Rev. 2014;10(2):100–112. doi:10.2174/1573399810666140402123026
33. Park YG, Kim EY, Roh YJ. Laser-based strategies to treat diabetic macular edema: history and new promising therapies. J Ophthalmol. 2014;2014:1–9. doi:10.1155/2014/769213
34. Everett LA, Paulus YM. Laser therapy in the treatment of diabetic retinopathy and diabetic macular edema. Curr Diab Rep. 2021;21(9):35. doi:10.1007/s11892-021-01403-6
35. Chen J, Wang H, Qiu W. Intravitreal anti-vascular endothelial growth factor, laser photocoagulation, or combined therapy for diabetic macular edema: a systematic review and network meta-analysis. Front Endocrinol. 2023;14. doi:10.3389/fendo.2023.1096105
36. Simó R, Sundstrom JM, Antonetti DA. Ocular anti-VEGF therapy for diabetic retinopathy: the role of VEGF in the pathogenesis of diabetic retinopathy. Diabetes Care. 2014;37(4):893–899. doi:10.2337/dc13-2002
37. Toohey TP, Shortt J, John N, Al-Qureshi S, Wickremasinghe SS. Intravitreal anti-vascular endothelial growth factor therapy in the treatment of vision loss associated with hematologic malignancy. Am J Ophthalmol Case Rep. 2024;36:102095. doi:10.1016/j.ajoc.2024.102095
38. Yadav M, Grezenko H, Kanukollu VMR, et al. A systematic review of the neuroprotective effects of Vascular Endothelial Growth Factor (VEGF) in diabetic retinopathy and diabetic macular edema: unraveling the molecular mechanisms and clinical implications. Cureus. 2023. doi:10.7759/cureus.51351
39. Sadda S. Retinal vein occlusion and macular edema critical evaluation of the clinical value of ranibizumab. Clin Ophthalmol. 2011;771. doi:10.2147/OPTH.S13774
40. Zhao X, Zhao Q, Wang C, et al. Central and peripheral changes in retinal vein occlusion and fellow eyes in ultra-widefield optical coherence tomography angiography. Invest Opthalmol Vis Sci. 2024;65(2):6. doi:10.1167/iovs.65.2.6
41. Rhoades W, Dickson D, Nguyen Q, Do D. Management of macular edema due to central retinal vein occlusion – the role of aflibercept. Taiwan J Ophthalmol. 2017;7(2):70. doi:10.4103/tjo.tjo_9_17
42. Manabe K, Osaka R, Nakano Y, et al. Metamorphopsia associated with central retinal vein occlusion. PLoS One. 2017;12(10):e0186737. doi:10.1371/journal.pone.0186737
43. Qian T, Zhao M, Xu X. Comparison between anti-VEGF therapy and corticosteroid or laser therapy for macular oedema secondary to retinal vein occlusion: a meta-analysis. J Clin Pharm Ther. 2017;42(5):519–529. doi:10.1111/jcpt.12551
44. Shalchi Z, Mahroo O, Bunce C, Mitry D. Anti-vascular endothelial growth factor for macular oedema secondary to branch retinal vein occlusion. Cochrane Database Syst Rev. 2020;2020(7). doi:10.1002/14651858.CD009510.pub3
45. Xing Q, Huang X-B, Peng L. Comparison of efficacy of conbercept, aflibercept, and ranibizumab ophthalmic injection in the treatment of macular edema caused by retinal vein occlusion: a meta-analysis. Int J Ophthalmol. 2023;16(7):1145–1154. doi:10.18240/ijo.2023.07.21
46. Qin H-F, Zhang C-Y, Luo D-W, et al. Anti-VEGF reduces inflammatory features in macular edema secondary to retinal vein occlusion. Int J Ophthalmol. 2022;15(8):1296–1304. doi:10.18240/ijo.2022.08.11
47. Kimoto K, Kubota T. Anti-VEGF agents for ocular angiogenesis and vascular permeability. J Ophthalmol. 2012;2012:1–11. doi:10.1155/2012/852183
48. Li Y-F, Ren Q, Sun C-H, et al. Efficacy and mechanism of anti-vascular endothelial growth factor drugs for diabetic macular edema patients. World J Diabetes. 2022;13(7):532–542. doi:10.4239/wjd.v13.i7.532
49. Stewart MW. The expanding role of vascular endothelial growth factor inhibitors in ophthalmology. Mayo Clin Proc. 2012;87(1):77–88. doi:10.1016/j.mayocp.2011.10.001
50. Imazeki M, Noma H, Yasuda K, Motohashi R, Goto H, Shimura M. Anti-VEGF therapy reduces inflammation in diabetic macular edema. Ophthalmic Res. 2021;64(1):43–49. doi:10.1159/000508953
51. Wong JHC, Jyw M, Jobling AI, et al. Exploring the pathogenesis of age-related macular degeneration: a review of the interplay between retinal pigment epithelium dysfunction and the innate immune system. Front Neurosci. 2022;16:1009599. doi:10.3389/fnins.2022.1009599
52. Vyawahare H, Shinde P. Age-related macular degeneration: epidemiology, pathophysiology, diagnosis, and treatment. Cureus. 2022;14(9). doi:10.7759/cureus.29583
53. Pitrelli Vazquez N, Knox PC. Assessment of visual distortions in age-related macular degeneration: emergence of new approaches. Br Ir Orthopt J. 2015;12:9–15.
54. Wallsh JO, Gallemore RP. Anti-VEGF-resistant retinal diseases: a review of the latest treatment options. Cells. 2021;10(5):1049. doi:10.3390/cells10051049
55. Li E, Donati S, Lindsley KB, Krzystolik MG, Virgili G. Treatment regimens for administration of anti-vascular endothelial growth factor agents for neovascular age-related macular degeneration. Cochrane Database Syst Rev. 2020;2020(5). doi:10.1002/14651858.CD012208.pub2
56. Nagi R, Muthukrishnan A, Rakesh N. Effectiveness of photodynamic therapy (PDT) in the management of symptomatic oral lichen planus -a systematic review. J Oral Biol Craniofac Res. 2023;13(2):353–359. doi:10.1016/j.jobcr.2023.03.003
57. Zborowski J, Kida D, Szarwaryn A, et al. A comparison of clinical efficiency of photodynamic therapy and topical corticosteroid in treatment of oral lichen planus: a Split-Mouth Randomised Controlled Study. J Clin Med. 2021;10(16):3673. doi:10.3390/jcm10163673
58. Xu M, Fan R, Fan X, Shao Y, Li X. Progress and challenges of anti-VEGF agents and their sustained-release strategies for retinal angiogenesis. Drug Des Devel Ther. 2022;16:3241–3262. doi:10.2147/DDDT.S383101
59. Levine ES, Custo Greig E, Mendonça LSM, et al. The long-term effects of anti-vascular endothelial growth factor therapy on the optical coherence tomography angiographic appearance of neovascularization in age-related macular degeneration. Int J Retin Vitr. 2020;6(1):39. doi:10.1186/s40942-020-00242-z
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Brolucizumab versus Aflibercept in Patients with Diabetic Macular Edema: A Meta-Analysis of Randomized Controlled Trials
Justino LB, Justino GB, Graffunder FP, Binotti WW, Khodor A, Caranfa JT
Clinical Ophthalmology 2024, 18:3679-3690
Published Date: 10 December 2024
Faricimab Outcomes in Chorioretinal Disorders: Indian Real-World Analysis (FOCUS Study)
Agrawal V, Gupta A, Agrawal V, Sheth JU
Clinical Ophthalmology 2025, 19:1855-1862
Published Date: 12 June 2025