")
Back to Journals » Clinical Ophthalmology » Volume 19
Faricimab Outcomes in Chorioretinal Disorders: Indian Real-World Analysis (FOCUS Study)
Authors Agrawal V, Gupta A , Agrawal V, Sheth JU
Received 7 February 2025
Accepted for publication 31 May 2025
Published 12 June 2025 Volume 2025:19 Pages 1855—1862
DOI https://doi.org/10.2147/OPTH.S521384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Vishal Agrawal,1 Ayushi Gupta,1 Virendra Agrawal,2 Jay Umed Sheth3
1Department of Retina, Agrawal Hospital, Jaipur, India; 2Department of Retina, Dr. Virendra Laser Phaco Surgery Centre, Jaipur, Rajasthan, India; 3Department of Retina Services, Shantilal Shanghvi Eye Institute, Mumbai, India
Correspondence: Jay Umed Sheth, Department of Retina Services, Shantilal Shanghvi Eye Institute, CS No: 3/207, 4/207, RJ Gaikwad Road, Barkat Ali Dargah Road, Wadala East, Mumbai, 400037, India, Tel +91-9961167200, Email [email protected]
Purpose: To assess the real-world efficacy and safety of intravitreal faricimab in treating Diabetic Macular Edema (DME), neovascular Age-related Macular Degeneration (nAMD), and Central Macular Edema (CME) secondary to retinal vein occlusion (RVO) in an Indian population.
Patients and Methods: This single‑center, retrospective observational study reviewed the records of 49 patients (49 eyes) diagnosed with DME, nAMD, or cystoid macular edema secondary to RVO, who received a total of 150 intravitreal faricimab injections and were followed for at least 24 weeks. Patients received intravitreal faricimab injections, with follow-up at four-week intervals. Outcome measures included changes in best-corrected visual acuity (BCVA) and central macular thickness (CMT), along with resolution of intraretinal (IRF) and subretinal fluid (SRF) in nAMD patients.
Results: Faricimab significantly improved BCVA and reduced CMT across all groups after a mean follow-up period of 33.31 (± 7.41) weeks. DME patients’ BCVA improved from 0.71 (± 0.36) LogMAR to 0.46 (± 0.35) LogMAR (P< 0.0001), nAMD from 1.24 (± 0.73) to 0.43 (± 0.43) LogMAR (P=0.00003), and RVO from 0.78 (± 0.32) to 0.38 (± 24) LogMAR (P=0.02). CMT decreased from 454.43 (± 164.76) μm to 255.3 (± 81.17) μm (P< 0.00001) overall. Significant reductions were also observed in IRF and SRF in nAMD patients, with IRF decreasing from 48% to 16% (P=0.008) and SRF from 100% to 20% (P< 0.00001). No significant adverse events, including intraocular inflammation (IOI), were reported.
Conclusion: Faricimab demonstrated significant visual and anatomical improvements across all diagnostic groups, including off‑label use in RVO‑associated CME during the study period, showing promise as an effective treatment for DME, nAMD, and RVO. These real-world outcomes align with clinical trial data (TENAYA, LUCERNE, YOSEMITE, RHINE), underscoring faricimab’s potential as an effective, dual-action therapy for chorioretinal disorders.
Keywords: faricimab, real-world, age-related macular degeneration, diabetic macular edema, retinal vein occlusion
Introduction
Chorioretinal disorders, particularly Diabetic Macular Edema (DME), Age-Related Macular Degeneration (AMD), and Central Macular Edema (CME) due to retinal vein occlusion (RVO), represent significant causes of vision impairment and blindness globally.1–3 These conditions not only diminish the quality of life but also impose a considerable burden on healthcare systems, particularly in developing nations like India. With the increasing prevalence of diabetes and the aging population, the incidence of DME and AMD is expected to rise, underscoring the urgent need for effective and accessible treatment strategies.4,5
The pathophysiology of these conditions often involves the overproduction of Vascular Endothelial Growth Factor (VEGF), a key mediator for increased vascular permeability and neovascularization.3,6,7 Consequently, anti-VEGF therapy has become the standard of care for managing these disorders. Among the various anti-VEGF agents approved for clinical use, Ranibizumab (Lucentis), Aflibercept (Eylea), and brolucizumab (Pagenax) have demonstrated efficacy in treating DME, neovascular AMD (nAMD), and CME secondary to RVO.6–8 These agents have transformed the management of retinal diseases by effectively reducing retinal edema and improving visual acuity.
However, despite the success of existing anti-VEGF treatments, there remains a need for novel therapeutic options that can enhance patient outcomes. This is particularly relevant in the Indian context, where factors such as treatment adherence, accessibility, and the burden of comorbidities may impact the effectiveness of existing therapies. Faricimab, a newly introduced bispecific antibody, has emerged as a promising candidate for treating chorioretinal disorders.9 Unlike traditional anti-VEGF therapies, Faricimab simultaneously targets VEGF-A and Angiopoietin-2 (Ang-2), a novel approach that addresses two critical pathways involved in retinal pathologies.9,10 The dual mechanism of action of Faricimab holds the potential to improve clinical outcomes, as it not only inhibits abnormal blood vessel growth but also stabilizes the existing vasculature by counteracting the effects of Ang-2.9,10 This innovative approach aims to provide a more comprehensive treatment strategy for patients suffering from DME, nAMD, and CME due to RVO.
The TENAYA and LUCERNE trials, pivotal Phase 3 studies, evaluated faricimab in patients with nAMD, while the YOSEMITE and RHINE trials assessed its efficacy in DME.9–11 These studies showed that faricimab provided non-inferior visual and anatomical outcomes compared to aflibercept, with up to 60% of patients achieving 16‑week dosing intervals—an advantage over ranibizumab’s typical 4‑ to 8‑week schedule and aflibercept’s 8‑ to 12‑week label intervals.9–11 This extended durability could be particularly impactful in developing nations such as India, where patients often default on monthly visits. Faricimab received regulatory approval in India in January 2024 for DME and nAMD. However, its application in macular edema secondary to retinal vein occlusion remains off‑label. Early-phase data from the BALATON and COMINO trials demonstrate favorable anatomical and visual outcomes in RVO patients, supporting its broader utility in clinical practice.12
Despite the impressive outcomes of the randomized clinical trials (RCT’s), their tightly controlled environments—where patients are carefully screened, treatments are provided at no cost, follow-up visits and imaging are rigidly scheduled, and non-adherent subjects are often excluded—rarely mirror the realities of real-world practice. In low- and middle-income settings such as India, clinicians face a very different array of challenges: clinics may lack manpower and/or imaging facilities, patients frequently travel long distances and juggle treatment visits with work or family obligations, and comorbidities such as uncontrolled diabetes, hypertension, or even infectious disease exposures can complicate both safety and efficacy assessments. Moreover, the financial burden of therapies, and variability in clinician training further erode the consistency of dosing and monitoring seen in RCTs. Cultural factors like health literacy, local beliefs about injections, and reliance on traditional medicine, add another layer of complexity that trials seldom capture.
While clinical trials provide robust data on the efficacy and safety of new treatments, real-world data are essential for understanding how these therapies perform outside the controlled environment of trials, especially in diverse populations like those in India.13–15 Real-world studies capture a broader spectrum of patient characteristics, including those with multiple comorbidities or who may not meet the strict inclusion criteria of clinical trials.13–15 They also provide insights into the practical challenges of administering treatment, such as patient adherence to follow-up and the impact of resource limitations in the healthcare system.13–15 Given the significant healthcare challenges in India, such as patient access to treatment and adherence to frequent injections, faricimab’s ability to provide longer-lasting effects may offer meaningful benefits in the real-world setting.
In the initial real‑world CLEAR‑DME cohort under routine clinical conditions, faricimab yielded clinically meaningful visual gains, sustained macular thickness reduction, and high rates of fluid resolution, accompanied by reduced hyperreflective foci and a favorable safety profile.16 Benefits were particularly pronounced in treatment‑naïve eyes, supporting further investigation in broader patient populations.16 The primary objective of this study is to evaluate the real-world efficacy (visual and anatomical outcomes) and safety of intravitreal Faricimab in patients diagnosed with DME, nAMD, and CME due to RVO in India, and to assess its potential to guide cost‑effective treatment strategies in resource‑limited settings.
Materials and Methods
The FOCUS (Faricimab Outcomes in Chorioretinal Disorders: Indian Real-World Analysis) study was designed as an exploratory, single-center, retrospective observational study at Agrawal Hospital, Jaipur, India. The study was performed between January and December 2024 and adhered to the principles outlined in the Declaration of Helsinki. Approval was obtained from the Institutional Ethics Committee of Agrawal Hospital, and written informed consent was secured from all patients for treatment, data collection, and publication.
Patient Selection and Eligibility
We conducted a systematic review of medical records to identify patients diagnosed with DME, nAMD, or CME secondary to RVO who received intravitreal faricimab during the study period. Inclusion criteria encompassed patients aged 18 years or older who were either treatment-naive or had received previous anti-VEGF therapy (≥ 4 weeks ago) with a minimum follow-up period of 24 weeks. Exclusion criteria included patients with a history of intravitreal corticosteroid therapy, significant media opacities that would interfere with examination, concurrent significant ocular pathologies, history of prior retinal surgery, or history of prior anti-VEGF therapy within the past 4 weeks.
All eligible patients received intravitreal faricimab injections (6 mg in 0.05 mL) under sterile conditions following standard operating protocols. The injections were administered by trained retinal specialists in an operating room. A comprehensive discussion on the risks, benefits, and alternatives to faricimab treatment was conducted with each patient prior to the initiation of therapy. All patients were advised re-injection based on pro-re-nata (PRN) regimen from the baseline. The PRN criteria included presence of any fluid for nAMD eyes, or a CMT of ≥350 µm for DME and RVO eyes.
Clinical Assessments
Comprehensive clinical evaluations were performed at baseline and during follow-up visits, which occurred at four weeks and then every four weeks thereafter. The following assessments were conducted: Best Corrected Visual Acuity (BCVA): using the Snellen visual acuity chart, Intraocular Pressure (IOP) using the Goldmann applanation tonometer, dilated fundus evaluation, Central Macular Thickness (CMT using the spectral-domain optical coherence tomography (SD-OCT) [Cirrus Carl Zeiss Meditec, Dublin, CA], and intraretinal Fluid (IRF) and subretinal Fluid (SRF) evaluation in patients with nAMD.
Outcome Measures
The primary outcome measures included changes in BCVA (LogMAR BCVA) and CMT at the final visit post-injection. Secondary outcomes comprised the resolution of IRF and SRF in wet ARMD patients, as well as a detailed safety profile of the treatment.
Statistical Analysis
All data were analyzed using SPSS version 23.0. Continuous variables, such as BCVA and CMT, were expressed as mean ± standard deviation (SD) for normally distributed data and as median (interquartile range) for non-normally distributed data. Categorical variables, such as the presence of IRF and SRF, were expressed as percentages. The Shapiro–Wilk test was used to assess the normality of the data. For normally distributed data, changes from baseline were analyzed using the paired t-test, while for non-normally distributed data, the Wilcoxon signed-rank test was used. Categorical variables, such as the resolution of IRF and SRF, were compared using the McNemar’s test. A P-value of <0.05 was considered statistically significant.
Results
Demographic Characteristics and Baseline Variables
A total of 49 eyes from 49 patients were included in the FOCUS study. The mean age of the study population was 62.69 (± 12.34) years, with males accounting for 59.18% (n = 29) and females representing 40.82% (n = 20). Of the study eyes, 32.65% (n=16) were treatment-naïve, while 67.35% (n = 33) had received prior anti-VEGF therapy. Among the previously treated eyes, the mean number of prior injections was 3.49 (± 2.37). The most common diagnosis amongst the study eyes was nAMD (25 eyes; 51.02%), followed by DME (17 eyes; 34.69%) and RVO (7 eyes; 14.29%).
A total of 150 faricimab injections were administered during the study period with a mean of 3.06 (± 1.28) injections. The most common diagnosis for which the injections were administered was nAMD, accounting for 48.67% (n = 73 injections), followed by DME in 34% (n = 51 injections), and RVO in 17.33% (n = 26 injections). The mean follow-up period of the study eyes was 33.31 (± 7.41) weeks. The distribution of eyes based on the number of injections received showed that 6 eyes (12.24%) received one injection, 12 eyes (24.49%) received two injections, 12 eyes (24.49%) received three injections, 11 eyes (22.45%) received four injections, and 8 eyes (16.33%) received five injections during the study period (Table 1).
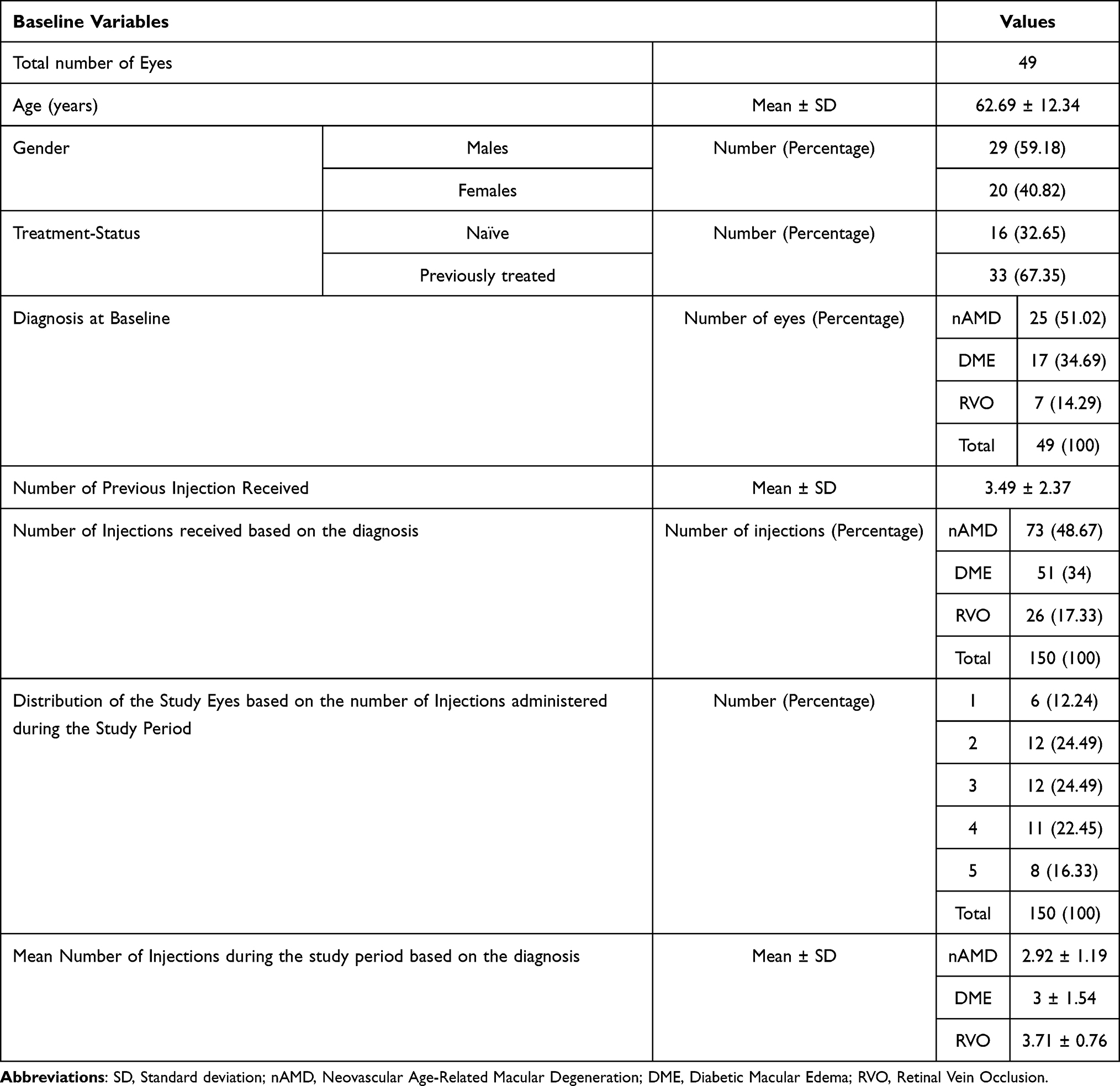 |
Table 1 Demographic Characteristics of the Study Population |
Best-Corrected Visual Acuity
The changes in BCVA across the different diagnostic categories were significant following treatment with faricimab at 24 weeks. In DME patients, mean baseline BCVA improved from 0.71 (±0.36) LogMAR to 0.46 (±0.35) LogMAR (P<0.0001). Similarly, in the nAMD cohort, the baseline BCVA of 1.24 (±0.73) LogMAR improved to 0.43 (±0.43) LogMAR (P=0.00003). For patients with CME due to RVO, BCVA improved from a baseline of 0.78 (±0.32) LogMAR to 0.38 (±0.24) LogMAR (P=0.02). Overall, across all eyes in the study, mean BCVA improved significantly from 1.24 (±0.73) LogMAR at baseline to 0.53 (±0.4) LogMAR post-injection (P<0.00001). Table 2 demonstrates the BCVA changes across the study population.
 |
Table 2 Changes in the Best-Corrected Visual Acuity (BCVA) and Central Macular Thickness (CMT) in the Study Population Post Faricimab Injection |
Central Macular Thickness (CMT)
Significant reductions in CMT were observed across all diagnostic groups following faricimab treatment. For the entire cohort, the mean CMT decreased from 454.43 (± 164.76) µm at baseline to 255.3 (± 81.17) µm at four weeks post-injection (P<0.00001). Among patients with DME, mean CMT significantly reduced from 524.35 (± 156.92) µm at baseline to 296.23 (± 78.4) µm post-injection (P=0.00001). In the nAMD group, CMT decreased from 396.72 (± 143.3) µm to 221.88 (± 45.69) µm (P<0.00001). Similarly, for patients with RVO, the mean CMT decreased from 490.71 (± 200.26) µm to 304.33 (± 145.22) µm post-injection (P=0.03) (Table 2).
Changes in Intraretinal Fluid (IRF) and Subretinal Fluid (SRF) in nAMD Patients
In eyes with nAMD, the presence of SRF and IRF was significantly reduced following faricimab injections. At baseline, all nAMD eyes (n = 25; 100%) had detectable SRF, which decreased to 5 eyes (20%) at the final visit post-injection (P<0.00001). Similarly, the proportion of eyes with IRF decreased from 48% (n = 12) at baseline to 16% (n = 4) post-injection (P=0.008) (Table 3).
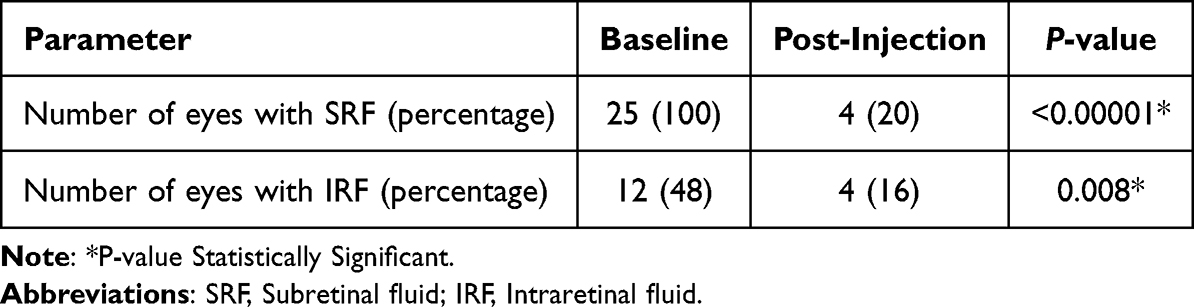 |
Table 3 Changes in the Proportion of Eyes with Intraretinal Fluid (IRF) and Subretinal Fluid (SRF) in the Neovascular Age-Related Macular Degeneration (nAMD) Group Post Faricimab Injection |
Safety Outcomes
Faricimab was well-tolerated across all patient groups, with no significant ocular or systemic adverse events, including intraocular inflammation (IOI), reported during the study period. No treatment discontinuity were noted.
Discussion
The FOCUS study evaluated the real-world efficacy and safety of intravitreal faricimab in patients with DME, nAMD, and CME secondary to RVO in an Indian population. The study findings demonstrated significant improvements in visual acuity and CMT across all diagnostic groups, with a notable reduction in IRF and SRF in nAMD eyes. Faricimab was also well-tolerated, with no significant ocular or systemic adverse events reported. These results align with previous clinical trial data and highlight faricimab’s potential as a dual-action treatment for chorioretinal disorders in real-world settings.
Anti-VEGF therapy has revolutionized the management of retinal vascular diseases, such as DME, nAMD, and CME secondary to RVO.6–8 The introduction of agents like ranibizumab, aflibercept, and brolucizumab has transformed the prognosis for patients with these conditions, significantly improving visual outcomes and preventing further vision loss. By inhibiting VEGF, these therapies reduce vascular permeability and neovascularization, leading to a decrease in retinal edema and improved visual acuity.3,8 However, despite these advancements, there are limitations to existing anti-VEGF therapies, including the need for frequent injections and the potential for incomplete response in some patients. Additionally, the burden of repeated treatments can be a significant challenge, particularly in low- and middle-income countries (LMICs) like India, where access to treatment and adherence to regular follow-ups may be hindered by socioeconomic factors.14,15
Faricimab offers a unique therapeutic advantage by targeting both VEGF-A and Angiopoietin-2 (Ang-2), addressing two key pathways involved in the pathophysiology of retinal diseases.9,10 VEGF-A promotes abnormal blood vessel growth and increased vascular permeability, while Ang-2 destabilizes blood vessels, making them more susceptible to VEGF-induced leakage and neovascularization.9,10 Faricimab’s bispecific approach enables not only the inhibition of new vessel formation but also the stabilization of existing vasculature, potentially providing longer-lasting effects and improved clinical outcomes.9,10 This dual mechanism of action may offer benefits, especially in populations where treatment adherence is a challenge, as faricimab has the potential to extend treatment intervals compared to traditional anti-VEGF agents.9,10
The pivotal phase 3 clinical trials—YOSEMITE and RHINE for DME, and TENAYA and LUCERNE for nAMD—have demonstrated the efficacy and safety of faricimab.9–11 These trials showed that faricimab was non-inferior to aflibercept in terms of visual and anatomical outcomes, with the added benefit of extended dosing intervals.9–11 In the YOSEMITE and RHINE trials, approximately 60% of DME patients were able to achieve 16-week dosing intervals, while similar results were observed in the TENAYA and LUCERNE trials for nAMD.9–11 The ability to extend dosing intervals without compromising efficacy represents a significant advancement in the treatment of chorioretinal disorders, particularly in resource-limited settings where frequent clinic visits may not be feasible. Notably, in the real‑world CLEAR‑DME cohort, faricimab achieved significant visual improvement, durable and sustained macular edema reduction, and marked fluid resolution, with decreased hyperreflective foci and an overall favorable safety profile, particularly in treatment‑naïve patients.16
When comparing the results of the FOCUS study with these clinical trials and real-world data, similar trends are observed. In our real-world cohort, faricimab significantly improved BCVA and reduced CMT in patients with DME, nAMD, and RVO. In addition, the FOCUS study showed that the presence of IRF and SRF was significantly reduced in nAMD patients following faricimab treatment. These findings mirror the results of the clinical trials, where faricimab demonstrated robust efficacy in resolving fluid accumulation in the retina, a key marker of disease activity. Interestingly, the BCVA gains observed in our real-world nAMD population appear slightly more pronounced than those reported in clinical trials. This may be attributed to several factors, including differences in baseline visual acuity, the inclusion of treatment-naïve patients who typically show more pronounced improvements, and the potential influence of regression to the mean. These factors highlight the importance of interpreting real-world outcomes in the context of broader clinical variability. Notably, our study reinforces the efficacy of Faricimab in a real-world setting, emphasizing its potential to address treatment gaps and improve patient outcomes in diverse populations.
In the FOCUS study, faricimab was used off-label for the treatment of chorioretinal disorders, specifically in cases of CME due to RVO, despite its approval being limited to DME and nAMD at the time. Our decision to use faricimab was based on its unique bispecific mechanism targeting both VEGF-A and Ang-2, which we hypothesized could offer enhanced benefits in these conditions. Notably, after the completion of our study, the BALATON and COMINO trials were published, confirming the efficacy of faricimab in RVO.12 These trials demonstrated non-inferior visual improvements and macular thickness reductions compared to aflibercept, alongside a greater reduction in macular leakage in the faricimab-treated groups.12 Our findings align closely with these trial outcomes, supporting the potential for faricimab to receive regulatory approval for RVO in the future. This suggests that faricimab could become a valuable therapeutic option for CME in RVO, further expanding its clinical utility.
The FOCUS study confirmed the favorable safety profile of faricimab, with no significant ocular or systemic adverse events reported during the study period. This is consistent with the safety data from the YOSEMITE, RHINE, TENAYA, and LUCERNE trials, where faricimab was well-tolerated with a low incidence of adverse events.9–11 In particular, no cases of intraocular inflammation, a concern with some other anti-VEGF therapies, were observed in the FOCUS study. This further supports the use of faricimab as a safe and effective treatment option for chorioretinal disorders in a real-world setting.
While most of the existing data on faricimab originates from controlled clinical trials, there remains a relative scarcity of published real-world post-approval data, especially from regions outside the US and Europe. This highlights the relevance and originality of our findings, particularly in a diverse, real-world population.
Despite the promising results, the FOCUS study has several limitations. Firstly, it is a retrospective, single-center study, which may limit the generalizability of the findings. Additionally, the follow-up period of 24 weeks is relatively short, and may not capture the long-term efficacy and safety of faricimab. While early improvements in vision and retinal anatomy suggest that faricimab provides meaningful benefits in real-world settings even within this limited timeframe, the full scope of its durability and impact remains to be established. Importantly, the lack of randomization introduces potential selection bias. The decision to initiate faricimab treatment was based on clinician judgment and may have been influenced by patient-specific factors such as disease severity, prior treatment history, or socioeconomic considerations. This could have led to preferential treatment of patients deemed more likely to benefit from the drug, thereby influencing the observed outcomes. At the same time, despite the shorter follow-up period of the FOCUS study compared to the clinical trials, the early improvements in vision and retinal anatomy suggest that faricimab provides meaningful benefits in real-world settings, even within a short timeframe. Moreover, faricimab’s longer duration of action could lead to even greater long-term benefits, particularly in LMICs, where maintaining frequent follow-up visits is often challenging. Future studies with longer follow-up periods and larger, multi-center cohorts are needed to confirm these findings. Another limitation is the lack of a direct comparator group, as patients were not randomized to receive faricimab or another anti-VEGF agent. Consequently, while the results are encouraging, they should be interpreted with caution, particularly when comparing the outcomes to those of randomized controlled trials.
One of the key strengths of the FOCUS study is its contribution to real-world data, particularly in the context of LMICs like India. While clinical trials provide valuable insights into the efficacy and safety of new treatments, they are conducted in controlled environments with strict inclusion and exclusion criteria. In contrast, real-world studies capture a broader spectrum of patient characteristics, including those with multiple comorbidities or who may not meet the stringent criteria of clinical trials. The study included both treatment-naïve and previously treated eyes, offering a comprehensive assessment of faricimab’s efficacy across different patient groups. Additionally, the inclusion of patients with various chorioretinal disorders and a range of prior treatments adds to the generalizability of the findings. As a natural extension of this work, future directions could include prospective, head-to-head comparisons of faricimab with other anti-VEGF agents such as aflibercept in Indian cohorts. Additionally, a multicenter real-world registry could provide valuable long-term safety data, particularly focusing on rare adverse events such as IOI.
Conclusion
In conclusion, the FOCUS study demonstrates that intravitreal Faricimab is a safe and effective treatment for patients with DME, nAMD, and CME due to RVO in India. The significant improvements in BCVA and CMT, along with the favorable safety profile, highlight its potential as a valuable addition to the therapeutic arsenal for chorioretinal disorders. However, given the study’s observational design and limited follow-up duration, the findings—particularly in the RVO subgroup—should be interpreted as preliminary. These results underscore the need for larger, controlled studies with longer follow-up to validate the therapeutic role of Faricimab across diverse chorioretinal conditions. As real-world evidence from low- and middle-income countries becomes increasingly important, future research should aim to assess long-term outcomes, durability of response, and cost-effectiveness in broader, more heterogeneous populations.
Disclosure
J.S reports affiliation with Shantilal Shanghvi Foundation, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234.
2. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045 [published correction appears in Diabetes Res Clin Pract. 2022;183:109119]. Diabet Res Clin Pract. 2023;204:110945. doi:10.1016/j.diabres.2023.110945
3. Gupta N, Mansoor S, Sharma A, et al. Diabetic retinopathy and VEGF. Open Ophthalmol J. 2013;7:4–10.
4. Maiti S, Akhtar S, Upadhyay AK, et al. Socioeconomic inequality in awareness, treatment and control of diabetes among adults in India: evidence from National Family Health Survey of India (NFHS), 2019–2021. Sci Rep. 2023;13:2971.
5. Bloom DE, Sekher TV, Lee J. Longitudinal Aging Study in India (LASI): new data resources for addressing aging in India. Nat Aging. 2021;1:1070–1072. doi:10.1038/s43587-021-00155-y
6. Chakraborty D, Sheth JU, Boral S, Sinha TK. Off-label intravitreal brolucizumab for recalcitrant diabetic macular edema: a real-world case series. Am J Ophthalmol Case Rep. 2021;24:101197.
7. Chakraborty D, Sharma A, Mondal S, et al. Brolucizumab versus aflibercept for recalcitrant diabetic macular edema in Indian real-world scenario - The BRADIR Study. Am J Ophthalmol Case Rep. 2024;36:102152.
8. Sheth JU, Stewart MW, Narayanan R, et al. Macular neovascularization. Surv Ophthalmol. 2024;2024:1.
9. Wong TY, Haskova Z, Asik K, et al. Faricimab treat-and-extend for diabetic macular edema: two-year results from the randomized phase 3 YOSEMITE and RHINE Trials. Ophthalmology. 2024;131(6):708–723.
10. Wykoff CC, Abreu F, Adamis AP, et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, phase 3 trials. Lancet. 2022;399(10326):741–755.
11. Khanani AM, Kotecha A, Chang A, et al. TENAYA and LUCERNE: two-year results from the phase 3 neovascular age-related macular degeneration trials of faricimab with treat-and-extend dosing in year 2. Ophthalmology. 2024;131(8):914–926.
12. Tadayoni R, Paris LP, Danzig CJ, et al. Efficacy and safety of faricimab for macular edema due to retinal vein occlusion: 24-week results from the BALATON and COMINO Trials. Ophthalmology. 2024;131(8):950–960.
13. Sheldrick RC. Randomized trials vs real-world evidence: how can both inform decision-making? JAMA. 2023;329(16):1352–1353. doi:10.1001/jama.2023.4855
14. Chakraborty D, Maiti A, Sheth JU, et al. Brolucizumab in neovascular age-related macular degeneration - Indian real-world experience: the BRAILLE Study - fifty-two-week outcomes. Clin Ophthalmol. 2022;16:4303–4313. doi:10.2147/OPTH.S395577
15. Chakraborty D, Maiti A, Sheth JU, et al. Brolucizumab in neovascular age-related macular degeneration - Indian real-world experience: the BRAILLE Study. Clin Ophthalmol. 2021;15:3787–3795. doi:10.2147/OPTH.S328160
16. Chakraborty D, Das S, Maiti A, et al. Clinical evaluation of faricimab in real-world diabetic macular edema in India- A multicenter observational study. Clin Ophthalmol. 2025;19:269–277. doi:10.2147/OPTH.S502033
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Faricimab for Treatment-Resistant Diabetic Macular Edema
Rush RB, Rush SW
Clinical Ophthalmology 2022, 16:2797-2801
Published Date: 24 August 2022
One Year Results of Faricimab for Aflibercept-Resistant Diabetic Macular Edema
Rush RB
Clinical Ophthalmology 2023, 17:2397-2403
Published Date: 16 August 2023
Outcomes of Anti-VEGF Therapy in Eyes with Diabetic Macular Edema, Vein Occlusion-Related Macular Edema, and Neovascular Age-Related Macular Degeneration: A Systematic Review
Aldokhail LS, Alhadlaq AM, Alaradi LM, Alaradi LM, AlShaikh FY
Clinical Ophthalmology 2024, 18:3837-3851
Published Date: 17 December 2024
Clinical Evaluation of Faricimab in Real-World Diabetic Macular Edema in India- A Multicenter Observational Study
Chakraborty D, Das S, Maiti A, Sinha TK, Das A, Sheth J, Boral SK, Mondal S, Nandi K
Clinical Ophthalmology 2025, 19:269-277
Published Date: 25 January 2025
Intravitreal Plungerless Injector Device (IPLID): An Innovative Intravitreal Injector Device
Yepez JB, Murati FA, Petitto M, Kozak I, Arevalo JF
Clinical Ophthalmology 2025, 19:535-541
Published Date: 14 February 2025