")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Predictors of Clinical Stability and Mortality in COPD: A Longitudinal Study
Authors Loo WTW , Chew SY , Tan JHY, Soh RY, Koh MS , Lapperre TS, Tiew PY
Received 31 March 2025
Accepted for publication 30 June 2025
Published 7 July 2025 Volume 2025:20 Pages 2311—2324
DOI https://doi.org/10.2147/COPD.S531435
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vanesa Bellou
Wesley Teck Wee Loo,1 Si Yuan Chew,1 Jessica Han Ying Tan,2 Rui Ya Soh,2 Mariko Siyue Koh,1,3 Therese S Lapperre,4,5 Pei Yee Tiew1,3,6
1Department of Respiratory and Critical Care Medicine, Singapore General Hospital, Singapore; 2Department of Respiratory Medicine, Sengkang General Hospital, Singapore; 3Duke-NUS Medical School, Singapore; 4Department of Pulmonology, University Hospital of Antwerp, Edegem, Belgium; 5Laboratory of Experimental Medicine and Pediatrics, Division of Respiratory Medicine, University of Antwerp, Wilrijk, Belgium; 6Lee Kong Chian, School of Medicine, Nanyang Technological University, Singapore
Correspondence: Wesley Teck Wee Loo, Department of Respiratory and Critical Care Medicine, Singapore General Hospital, 20 College Road Singapore, Singapore, 169856, Email [email protected]
Background: There is no consensus on the definition of clinical stability in chronic obstructive pulmonary disease (COPD), and it is less frequently used as a treatment target compared to severe asthma. The factors that determine clinical stability and their effects on mortality are less well-studied in patients with COPD.
Methods: To address this gap, we conducted a prospective longitudinal cohort study to identify predictors of two-year clinical stability, defined as no exacerbations and stable symptoms (< 2 point change in CAT score from baseline), and the impact of comorbid cardiovascular disease (CVD) on clinical stability and mortality in COPD patients.
Results: A total of 463 patients (mean age 71 ± 9 years) were enrolled in this study. The cohort was predominantly Chinese (81.7%) and 45.6% of participants were current smokers. The majority (55.7%) had a history of CVD. Approximately 36% of the cohort achieved clinical stability at one year, and one-third achieved stability at two years. Predictors of 2-year clinical stability included higher body mass index (BMI) (p< 0.001), higher post-bronchodilator FEV1/FVC ratio (p=0.0132), fewer baseline exacerbations (p=0.007), absence of bronchiectasis (p=0.045), preserved hemoglobin levels (p=0.019), and successful smoking cessation (p=0.039). Notably, while 2-year clinical stability did not predict subsequent mortality, the presence of CVD was a significant predictor of 5-years mortality (HR 1.48, 95% CI 0.99– 2.22; p=0.05).
Conclusion: Our study identified several predictors of 2-year clinical stability in patients with COPD. However, clinical stability at 2 years did not predict subsequent mortality. These findings suggest that clinical stability and mortality are distinct outcomes that are driven by different sets of predictive variables. This underscores the need for a comprehensive approach to COPD management that not only addresses exacerbations and symptoms, but also considers a broader range of factors influencing survival, particularly the management of comorbidities such as cardiovascular disease.
Keywords: stability, mortality, cardiovascular disease, South East Asia, multi-ethnic, comorbidities
Introduction
Chronic obstructive pulmonary disease (COPD) remains a major global health concern, with an, estimated prevalence of 6.2% in Asia and 5.9% in Singapore.1,2 It is the fourth leading cause of death worldwide and ranks eighth in the disability-adjusted life years lost.3 The disease burden is more substantial in Asia, with the highest prevalence and mortality of COPD in the Asia-Pacific region.4,5
Mortality and exacerbations are pivotal clinical outcomes in COPD and frequently serve as important endpoints in clinical studies.6,7 Composite endpoints have been introduced to capture a more comprehensive assessment of disease progression and treatment efficacy. One such measure is clinically important deterioration (CID), which integrates multiple indicators of worsening health status, including declines in lung function, exacerbations, and deterioration in patient-reported outcomes such as St. George’s Respiratory Questionnaire (SGRQ) or COPD Assessment Test (CAT) scores.8 Pharmacological therapy has been shown to reduce the risk of CID, triple therapy more so than dual therapy,8,9 while older age and lower Forced Expiratory Volume in 1 second (FEV1) increase the risk of CID.10 While markers of clinical deterioration are essential for evaluating disease progression, and the concept of clinical stability is less frequently utilized in COPD. Recognizing and quantifying clinical stability is crucial as it reflects effective disease management and may inform therapeutic decisions. Efforts have been made in recent years to better understand disease stability in COPD, defined variably as the absence of exacerbation, as well as the absence of significant clinical deterioration or the presence of improvement over a period of time.11–15 This has led to calls for the pursuit of clinical stability in the management of COPD patients.12 However, there remains a lack of consensus on a defined duration for clinical stability. With the emergence of biologics in treatment of airway diseases, including the recent approval of biologics for COPD,16 it is essential to explore and refine the concept of disease stability, drawing parallels to advancements made in the field of severe asthma.17
Cardiovascular comorbidities are increasingly recognized as a significant contributor to the morbidity and mortality of COPD,18 with the prevalence of cardiovascular disease (CVD) among COPD patients estimated to be between 20% to 60%.19,20 A meta-analysis showed a more than two-fold increase in the risk of CVD in patients with COPD compared to patients without COPD.19 Such an association arises from shared risk factors and increased systemic inflammation from chronic and intermittent hypoxia.21,22 Although ethnic disparities in susceptibility to cardiovascular disease and mortality have been reported, their impact on individuals with both COPD and CVD in multi-ethnic Asian cohorts remains underexplored. The REGARDS COPD cohort from the United States found no significant difference in all-cause mortality between Black and White individuals.23 However, there was a 40% higher risk of cardiovascular mortality among Black women compared to White women.23 Data from the Asia-Pacific region indicate an increased mortality risk in COPD patients with concomitant atrial fibrillation.24 Additionally, analyses of COPD patients of Chinese ethnicity in South East Asia showed that patients with cardiovascular disease are at higher risk of mortality.25 An older study examining cardiovascular disease in a multi-ethnic Singaporean cohort reported higher ischemic heart disease related mortality in Indian individuals compared to Malay and Chinese ethnic groups.26 However, the prevalence and impact of comorbid CVD on clinical stability and mortality in a multi-ethnic South East Asian COPD cohort remains underexplored.
Therefore, our objective was to identify the predictors of two-year clinical stability of COPD and the impact of comorbid CVD on clinical stability and five-year mortality, by conducting a prospective longitudinal observational study.
Methods
Patients with COPD aged 40 years and above attending a multidisciplinary COPD clinic consisting of pulmonologists, COPD nurses, physiotherapists, pharmacists, and smoking cessation counselors at Singapore General Hospital were prospectively recruited from 2013 to 2024. Patient with confirmed COPD who were able to provide written informed consent were included in the study. Those who did not provide consent were excluded. COPD was defined according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2013 as the presence of respiratory symptoms and/or risk factor exposure and post-bronchodilator FEV1/FVC<0.7.27,28 Patient demographics, smoking history, clinical data including symptom score (CAT score), exacerbations, and hospitalization in the previous year, comorbidities, spirometry, year of COPD diagnosis, CT thorax, blood eosinophil count, hemoglobin level, and baseline treatment were obtained from patient histories and supplemented by verification from medical records at recruitment. During annual follow-up visits, smoking history, CAT score, number of exacerbations, spirometry results, and COPD treatment were obtained and recorded. The duration of COPD at study entry was determined on the basis of the year of the first recorded spirometry. Exacerbation was defined as acute worsening of symptoms requiring corticosteroids and/or antibiotics. Frequent exacerbators were defined as having two or more exacerbations in the year preceding study recruitment as well as moderate exacerbations, which refer to COPD exacerbations necessitating emergency visits or hospital admission. Cardiovascular disease was defined as the presence of coronary artery disease, heart failure, atrial fibrillation and flutter, cerebrovascular disease, hypertensive heart disease, peripheral arterial disease, pulmonary arterial hypertension, cardiomyopathy, and valvular heart disease.29,30 All deaths in Singapore were automatically updated in our national electronic health record and the date of death was recorded. We defined COPD stability at 1- and 2-years as having met both the following criteria: (1) no exacerbations requiring oral corticosteroids, antibiotics, and/or hospitalization and (2) a stable CAT score (<2 points change from baseline) over 1 and 2 years. For the evaluation of 2-year stability, patients who died before the 2-year assessment or who were lost to follow-up were excluded because the cause of death was not available. Patients who were included in the evaluation of 2-year stability were subsequently included in the analysis of 5-year mortality. Study data were collected and managed using REDCap electronic data capture tools hosted at Singapore General Hospital.31,32
This study was approved by the SingHealth Centralized Institutional Review Board under CIRB 2018/2186 (2013/184/C) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants at recruitment.
Statistical Analysis
Data were analyzed using the R software (version 3.6.1, R Foundation for Statistical Computing, Vienna, Austria). Normality was assessed using the Shapiro–Wilk test. Continuous variables with a normal distribution were presented as mean ± standard deviation, whereas non-normally distributed variables were reported as medians with interquartile ranges. The Mann–Whitney U-test was used to compare non-normally distributed continuous variables between the two groups. Categorical variables were compared using the chi-square test, and the Kruskal–Wallis test followed by Dunn’s test with false discovery rate correction was used for multiple group comparisons. Additionally, multivariate logistic regression for CVD were performed by including variables that were significant in the univariate analysis and clinically relevant. The Hosmer–Lemeshow test was used to evaluate goodness of fit, with a p-value > 0.05 indicating acceptable calibration. Multicollinearity was assessed using variance inflation factors (VIFs), and no variables exceeded the conventional threshold (VIF > 5). Missing data were present in fewer than 20% of all the variables except for education level and were handled by complete-case analysis whereby cases with missing values were excluded from the relevant analyses. Mortality analysis was performed using Kaplan-Meier survival curves and the Cox proportional hazard ratio. Variables with a p-value <0.05, in the univariate Cox proportional hazard analysis for mortality, were included in the multivariate model. Proportional hazards assumption was tested using Schoenfeld residuals and the global test was not statistically significant indicating that the assumption was adequately met.
Results
Baseline Characteristics of the Study Cohort
In total, 463 patients were recruited between 2013–2024 (Figure 1). The baseline characteristics of the study cohort are summarized in Table 1. The mean age of the patients was 71 (standard deviation [SD], 9), with male accounting for 96.3% of the cohort. The majority of the cohort was of Chinese ethnicity (81.7%), followed by Malay (10.8%), closely mirroring Singapore’s demographic composition. Current smokers represented 45.6% of the cohort, with median pack years of 50.0 (interquartile range [IQR] 40–68). The median duration of COPD at time of study recruitment was 2 years (IQR 1–5), 113 (24%) were newly diagnosed with COPD at initial assessment. The median COPD assessment test (CAT) score was 13.0 (IQR 7–20) and the median modified medical research council (mMRC) dyspnea score was 2.00 (IQR 1–3), indicating moderate symptom burden among the study cohort. Most patients were receiving either dual bronchodilator therapy (37.8%, n=175) or triple therapy (37.4%, n=173) at baseline.
 |
Table 1 Baseline Characteristics of the Overall Cohort and with and Without Cardiovascular Disease (CVD) |
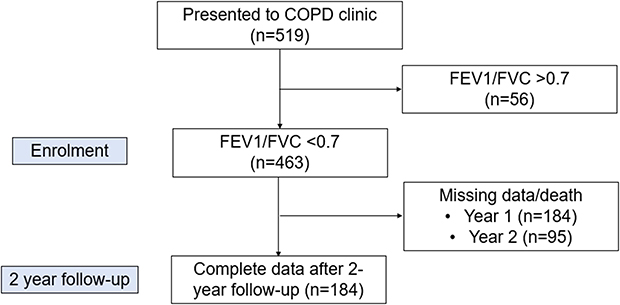 |
Figure 1 STROBE flowchart of study. |
Characteristics of COPD Patients with and Without Cardiovascular Disease
A large proportion of our cohort (55.7%; n=258) had a history of CVD (Table 1). COPD patients with CVD were generally older (mean 73 vs 69 years; p<0.001) and had a longer duration of COPD (median 2 vs 1 year; p=0.008), higher smoking pack years (median 50 vs 47 years; p=0.025), and higher body mass index (BMI) (median 22.1 vs 20.6; p<0.001). There was no significant difference in the prevalence of CVD among different ethnic groups. Patients with CVD were also more likely to have other comorbidities, including hyperlipidemia (69.8% vs 19.0%; p<0.001), diabetes mellitus (21.7% vs 8.3%; p<0.001), chronic kidney disease (CKD) (14.7% vs 2.0%; p<0.001), and depression (3.9% vs 0.5%; p=0.038). Multivariate logistic regression identified several factors significantly associated with the presence of CVD (Supplementary Table 1). Older age (OR 1.05, 95% CI 1.02–1.08; p = 0.003) and higher BMI (OR 1.07, 95% CI 1.01–1.14; p = 0.028) were associated with moderate but clinically relevant incremental risks. Greater smoking pack years showed a trend towards significance (OR 1.01 per pack-year, 95% CI 1.00–1.01; p = 0.060). Importantly, hyperlipidaemia was associated with a substantial increase in risk, more than eightfold (OR 8.44, 95% CI 4.93–14.44; p < 0.001) highlighting a major clinical impact. Similarly, CKD increased the odds of CVD by approximately fourfold (OR 4.00, 95% CI 1.08–14.76; p = 0.037), underscoring its clinical relevance. In contrast, other variables including gender, diabetes, and depression were not significantly associated with CVD and showed effect sizes of limited clinical importance in this cohort. The logistic regression model demonstrated good fit (Hosmer–Lemeshow test, p = 0.303). No significant multicollinearity was detected (all VIFs < 2).
COPD Duration and Disease Severity
A longer COPD duration at the time of recruitment was associated with several indicators of disease severity, including lower lung function (Figure 2A), higher symptom burden, and an increased frequency of exacerbations (Figure 2B). Additionally, patients with a longer COPD duration were more likely to have cardiovascular disease (Figure 2C), a higher prevalence of concomitant bronchiectasis (Figure 2D), a lower blood eosinophil count, quit smoking, and more frequent triple therapy. Longer COPD duration was also associated with increased exacerbations and higher baseline symptom (CAT) scores.
 |
Figure 2 Scatter boxplot of illustrating the association of COPD duration with (A) GOLD spirometry grade, (B) GOLD ABE group, (C) presence (Yes) or absence (No) of cardiovascular disease and (D) presence (Yes) or absence (No) of bronchiectasis. Box plots indicate the median and interquartile range and the largest and smallest values above or below the 75th and 25th percentile, respectively. ***p<0.001,. ns: not significant **p<0.01, *p<0.05, ns: not significant. Abbreviation: GOLD, Global Initiative for Chronic Obstructive Lung Disease. |
Predictors of Clinical Stability in COPD at Two years
We next assessed longitudinal two-year clinical stability based on symptoms (CAT score) and exacerbations. Fifty-seven patients died before the two-year assessment and were excluded; and complete two-year longitudinal data were available for 184 patients. The baseline characteristics of the patients with and without 2-year longitudinal data are summarized in Supplementary Table 2. Overall, the number of exacerbations significantly decreased from baseline to year 1 and 2. The proportion of patients with frequent exacerbations at baseline was 46.0% (n=85), compared to 31.0% (n=57) at year 1 and 36.4% (n=67) at year 2 (p=0.009, Kruskal Wallis test) (Figure 3A). In contrast, there was no significant change in the proportion of patients with CAT scores <10 over the 2-year follow-up period (baseline: 34.8% (n=64); year 1: n= 37.0% (n=68); year 2: 29.3% (n=54); p=0.282, Kruskal Wallis test) (Figure 3B). The proportion of patients who remained clinically stable was similar between years 1 (34.6%, n=64) and year 2 (32.6%, n=60) (p=0.741, Kruskal Wallis test) (Figure 3C).
 |
Figure 3 Sankey plots illustrating the changes in the proportion of patients with (A) frequent exacerbation (FE), (B) CAT score of less than 10, and (C) clinical stability from baseline to 2 years of follow-up. Abbreviation: CAT, COPD Assessment test. |
Predictors of clinical stability in COPD at two years include higher BMI (p<0.001), higher post-bronchodilator FEV1/FVC ratio (p=0.0132), fewer exacerbations at baseline (p=0.007), absence of concomitant bronchiectasis (p=0.045), and higher hemoglobin levels (p=0.019) (Table 2). Additionally, the presence of hyperlipidemia (p=0.019) and treatment with lipid-lowering agents (p=0.035) were associated with clinical stability at 2-years. Notably, a greater proportion of patients who achieved stability had quit smoking (67% vs 33%; p=0.039) during the 2-year period. Patients with clinical stability were less likely to be on triple therapy (36.7% vs 57.3%; p=0.033).
 |
Table 2 Characteristics of Patients with and Without Clinical Stability After 2 years |
Impact of Clinical Stability and Cardiovascular Disease on Mortality
Having determined clinical stability, we next evaluated the 5 years-mortality in patients with and without 2-year stability. The median follow-up period was 1780 (IQR 1100–2780) days. Interestingly, clinical stability at two years was not associated with subsequent mortality. The Kaplan-Meier survival curve demonstrated no significant difference in all-cause mortality between patients who achieved clinical stability at 2 years and those who did not (p=0.73) (Figure 4A). In contrast, patients with CVD had significantly higher mortality rates than those without (p=0.017) (Figure 4B). This association persisted (hazard ratio for CVD 1.48, 95% CI 0.99–2.22; p=0.05) even after adjusting for potential confounders, including age, gender, smoking pack years, FEV1% predicted and duration of COPD (Supplementary Table 3). The model was stratified by BMI category to account for its non-proportional effect over time. The global test for the proportional hazards assumption was not significant (p=0.075), and no individual covariates showed evidence of non-proportionality, suggesting that the final model adequately satisfies the proportional hazard assumption. Other factors associated with 5-years mortality include older age, higher baseline dyspnea (mMRC) scores, and history of pulmonary tuberculosis (Supplementary Tables 4 and 5).
 |
Figure 4 Kaplan-Meier curves illustrating the survival differences between (A) patients with (Y) and without (N) 2-year clinical stability and (B) cardiovascular disease (CVD). stable_2: 2-year clinical. |
Discussion
In our study, clinical stability, defined by the absence of exacerbations and having stable symptom control, was achieved in 34.6% of patients at year one and 32.6% at year two following optimization of COPD management in a multidisciplinary clinic setting. The factors associated with attaining clinical stability at two years included a higher body mass index (BMI), better lung function, preserved hemoglobin levels, fewer baseline exacerbations, successful smoking cessation, hyperlipidemia treated with lipid-lowering agents, and the absence of concomitant bronchiectasis. These findings underscore the value of a multidisciplinary approach to COPD management that emphasizes personalized treatment and targeting of treatable traits to mitigate disease progression and prevent complications. Notably, achieving clinical stability at two years did not correlate with subsequent mortality, suggesting that factors beyond short-term clinical stability, such as comorbid CVD, significantly influenced long-term survival outcomes. More than half of the patients with COPD in our cohort had comorbid CVD, which was associated with older age, higher cumulative smoking exposure, increased BMI, longer COPD duration, and a higher prevalence of metabolic comorbidities. Key predictors of mortality included older age, higher dyspnea score, presence of CVD, and history of pulmonary tuberculosis. Additionally, longer COPD duration was linked to worse lung function, greater symptom burden, more frequent exacerbations, and the presence of comorbid CVD and bronchiectasis at study entry. This suggests that COPD worsens over time, leading to increased disease burden and complications, highlighting the importance of early diagnosis in preventing disease progression. Despite these associations, the duration of COPD did not affect the clinical stability at two years. These findings highlight the complex interplay between factors influencing disease progression and outcomes in patients with COPD, emphasizing the need for comprehensive and individualized management strategies.
Efforts made to phenotype COPD patients may have led to more personalized treatment, but does not account for the variability that may occur over time.14,33 Concepts of clinical control and stability have thus emerged to account for these temporal variations, but predictors of such an endpoint have remained elusive.34 Our study suggests that easily obtainable clinical data such BMI, lung function tests, haemoglobin levels and number of exacerbations may help to predict clinical stability of COPD and further refine treatment targets. Indeed, this highlights the benefit and importance of early recognition and multidisciplinary management of COPD encouraged by the GOLD guidelines.27 This include a personalized treatment approach targeting treatable traits in COPD management, such as preservation of lung function with pharmacotherapy, nutritional support to optimize BMI, and smoking cessation to help achieve stability.35,36 The introduction and optimization of pharmacological therapy is also important in reducing CID and exacerbations in COPD,8,10 although its effect may be attenuated by older age, particularly as the mean age of our cohort is higher than that of many other studies.10 Nonetheless, these remain fundamental in preventing exacerbations and reducing mortality.
Despite efforts to achieve clinical stability, the absence of a difference in mortality between clinically stable and unstable patients reflects the complexity of COPD. Moreover, our results indicate that while a longer duration of COPD is associated with more severe disease and increased exacerbations, it does not influence 2-year stability in our cohort. This suggests that achieving 2-year stability is possible even in severe diseases with a multidisciplinary team (MDT) approach and personalized treatment strategies. An MDT approach that incorporates guideline-directed therapy and comprehensive COPD management plays a crucial role in optimizing patient outcomes.37 By leveraging the expertise of various healthcare professionals, the MDT ensures a holistic and individualized care plan that addresses the diverse needs of COPD patients.37 The team typically includes physicians, nurses, and allied health professionals such as physiotherapists, dietitians, and social workers, each contributing to patient education, symptom management, and tailored interventions.35,37 Through coordinated efforts, the MDT with treatable trait approach improves quality of life in patients with chronic airway disease.35,38
Although clinical stability may serve as a useful short-term treatment endpoint, it fails to capture the full extent of the factors driving mortality in COPD. Other important predictors of COPD mortality include cardiovascular disease, older age, dyspnea score, previous exacerbations, male sex, hypoxemia, use of long-term oxygen therapy, body mass index, prior pulmonary tuberculosis, and lower FEV1.25,39–43 This is consistent with our findings; however, in multivariate analysis, neither lung function nor BMI remained significant predictors of mortality. Overall, this finding suggests that clinical stability and mortality are distinct outcomes, each driven by different sets of predictive variables, underscoring the need for a comprehensive approach to COPD management that addresses both clinical stability (exacerbations and symptoms) and a broad range of factors that influence long-term survival.
While studies have identified ethnic differences in COPD comorbidities and CVD, our findings did not show significant differences in CVD between ethnic groups.26,44 A cross-sectional study in the US (1999–2018) found variation in CVD risk between Hispanic white and black populations, but these differences were largely explained by social determinants of health.45 Similarly, a prospective cohort study from the UK reported adiposity as an important risk factor for CVD irrespective of ethnicity.46 These findings suggest that factors beyond ethnicity, such as socioeconomic status, healthcare access, and risk factor exposure, may play a more substantial role in determining CVD risk. Additionally, the small number of Malay and Indian patients with COPD in our cohort may have limited our ability to detect ethnic differences because these ethnic groups have been shown to have a higher incidence of cardiovascular comorbidities.47
Nonetheless, our study contributes to a growing body of evidence highlighting the importance of early identification and management of CVD in COPD, irrespective of ethnicity.19,25,39,41 This is especially crucial in patients with a history of heavy smoking (>40 pack-years), given its deleterious effects on both the cardiovascular and respiratory systems.21,48 Furthermore, evidence of manifestations of metabolic comorbidities, such as hyperlipidemia and diabetes mellitus, suggests chronicity of the underlying inflammatory milieu, reinforcing the need to screen these patients for CVD.49,50 Early multidisciplinary management of CVD in COPD is essential to improve outcomes.
Although our study provides valuable insights as a longitudinal prospective analysis with 2 years of follow-up data on clinical stability and 5 years of mortality outcomes in an Asian population, it has several limitations. First, it was conducted at a single tertiary center, which limits its generalizability. However, this limitation is mitigated by Singapore’s small geographical size, and our hospital is a tertiary referral center that receives referrals from various regions of Singapore.51 Second, the cohort was predominantly male, consistent with other Asian COPD studies52 where male patients with lower BMI are commonly observed compared to Western cohorts.53,54 Third, the absence of detailed cause of death data precluded differentiation between respiratory and non-respiratory causes of mortality. Additionally, follow-up spirometry data were unavailable for all patients; therefore, they were not included in the definition of clinical stability. We did not perform sensitivity analyses to test the robustness of our findings against alternative definitions or assumptions. This may limit the generalizability of our results. Future studies could incorporate validated criteria and sensitivity analyses on predictor of COPD stability and mortality. Finally, longitudinal data on the development of cardiovascular disease and its association with acute exacerbations are unavailable and fall beyond the scope of this study.
Conclusion
In this prospective longitudinal study, we identified several clinical and modifiable factors including higher BMI, better lung function, preserved haemoglobin levels, fewer baseline exacerbations, successful smoking cessation, and absence of concomitant bronchiectasis as significant predictors of two-year clinical stability in patients with COPD. However, achieving clinical stability did not predict long-term survival. Instead, key predictors of five-year mortality were comorbid cardiovascular disease, prior pulmonary tuberculosis, older age, and higher dyspnea scores. These findings highlight the complex and multifactorial nature of COPD progression and outcomes, underscoring the importance of a comprehensive, individualized approach to COPD management that addresses both respiratory and systemic comorbidities to improve short- and long-term outcomes.
Data Sharing Statement
The datasets generated and analyzed during the current study are not available in public domains but can be requested from the corresponding author.
Funding
This research was supported by the Singapore Ministry of Health’s National Medical Research Council under its Transition Award Grant (MOH-001275-00)(P.Y.T) and the National Research Foundation Singapore under its Open Fund-Large Collaborative Grant (MOH-001636), and administered by the Singapore Ministry of Health’s National Medical Research Council.
Disclosure
P.Y.T was on advisory boards for AstraZeneca and Sanofi outside the submitted work. M. S. K has received research grants from AstraZeneca and honorarium paid to her employer (Singapore General Hospital) from GSK, AstraZeneca, Sanofi, Novartis and Boehringer Ingelheim outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Netw Open. 2023;6(12):e2346598–e2346598. doi:10.1001/jamanetworkopen.2023.46598
2. Lim S, Lam DC-L, Muttalif AR, et al. Impact of chronic obstructive pulmonary disease (COPD) in the Asia-Pacific region: the EPIC Asia population-based survey. Asia Pacific Family Med. 2015;14(1):4. doi:10.1186/s12930-015-0020-9
3. World Health Organisation. Chronic obstructive pulmonary disease. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
4. Adeloye D, Song P, Zhu Y, et al. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
5. Soriano JB, Kendrick PJ, Paulson KR, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
6. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
7. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
8. Singh D, Maleki-Yazdi MR, Tombs L, Iqbal A, Fahy WA, Naya I. Prevention of clinically important deteriorations in COPD with umeclidinium/vilanterol. Int J Chron Obstruct Pulmon Dis. 2016;11:1413–1424. doi:10.2147/copd.S101612
9. Han MK, Criner GJ, Dransfield MT, et al. Prognostic value of clinically important deterioration in COPD: IMPACT trial analysis. ERJ Open Res. 2021;7(1):00663–2020. doi:10.1183/23120541.00663-2020
10. Manzetti GM, Ora J, Sepiacci A, Cazzola M, Rogliani P, Calzetta L. Clinically Important Deterioration (CID) and Ageing in COPD: a systematic review and meta-regression analysis according to PRISMA statement. Int J Chron Obstruct Pulmon Dis. 2023;18:2225–2243. doi:10.2147/COPD.S396945
11. Soler-Cataluña J J, Alcázar-Navarrete B, Miravitlles M. The concept of control in COPD: a new proposal for optimising therapy. Eur Respir J. 2014;44(4):1072–1075. doi:10.1183/09031936.00064414
12. Singh D, Han MK, Bhatt SP, et al. Is disease stability an attainable COPD treatment goal? Am J Respir Crit Care Med. 2024. doi:10.1164/rccm.202406-1254CI
13. Miravitlles M, Sliwinski P, Rhee CK, et al. Predictive value of control of COPD for risk of exacerbations: an international, prospective study. Respirology. 2020;25(11):1136–1143. doi:10.1111/resp.13811
14. Miravitlles M, Sliwinski P, Rhee CK, et al. Changes in control status of COPD over time and their consequences: a prospective international study. Arch Bronconeumol. 2021;57(2):122–129. doi:10.1016/j.arbres.2020.06.003
15. Miravitlles M, Sliwinski P, Rhee CK, et al. Evaluation of criteria for clinical control in a prospective, international, multicenter study of patients with COPD. Respir Med. 2018;136:8–14. doi:10.1016/j.rmed.2018.01.019
16. Bhatt SP, Rabe KF, Hanania NA, et al. Dupilumab for COPD with Type 2 inflammation indicated by eosinophil counts. N Engl J Med. 2023;389(3):205–214. doi:10.1056/NEJMoa2303951
17. Canonica GW, Blasi F, Carpagnano GE, et al. Severe asthma network Italy definition of clinical remission in severe asthma: a delphi consensus. J Allergy Clin Immunol Pract. 2023;11(12):3629–3637. doi:10.1016/j.jaip.2023.07.041
18. Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28(6):1245–1257. doi:10.1183/09031936.00133805
19. Chen W, Thomas J, Sadatsafavi M, FitzGerald JM. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Lancet Respir Med. 2015;3(8):631–639. doi:10.1016/S2213-2600(15)00241-6
20. Morgan AD, Zakeri R, Quint JK. Defining the relationship between COPD and CVD: what are the implications for clinical practice? Ther Adv Respir Dis. 2018;12:1753465817750524. doi:10.1177/1753465817750524
21. Rabe KF, Hurst JR, Suissa S. Cardiovascular disease and COPD: dangerous liaisons? Eur Respir Rev. 2018;27(149):180057. doi:10.1183/16000617.0057-2018
22. Polman R, Hurst JR, Uysal OF, Mandal S, Linz D, Simons S. Cardiovascular disease and risk in COPD: a state of the art review. Expert Rev Cardiovasc Ther. 2024;22(4–5):177–191. doi:10.1080/14779072.2024.2333786
23. Krishnan JK, Rajan M, Banerjee S, et al. Race and sex differences in mortality in individuals with chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2022;19(10):1661–1668. doi:10.1513/AnnalsATS.202112-1346OC
24. Bucci T, Romiti GF, Shantsila A, et al. Risk of death and cardiovascular events in asian patients with atrial fibrillation and chronic obstructive pulmonary disease: a report from the Prospective APHRS registry. J Am Heart Assoc. 2024;13(7):e032785. doi:10.1161/JAHA.123.032785
25. Tiew PY, Fws K, Narayana JK, et al. “High-Risk” clinical and inflammatory clusters in COPD of Chinese Descent. Chest. 2020;158(1):145–156. doi:10.1016/j.chest.2020.01.043
26. Hughes K, Lun KC, Yeo PP. Cardiovascular diseases in Chinese, Malays, and Indians in Singapore. I. Differences in mortality. J Epidemiol Community Health. 1990;44(1):24–28. doi:10.1136/jech.44.1.24
27. From the Global Strategy for the Diagnosis, Management and Prevention of COPD, global initiative for chronic obstructive lung disease (GOLD) 2021. Available from: http://goldcopd.org/.
28. West JB. GOLD Executive Summary. Am J Respir Crit Care Med. 2013;188(11):1366–1367. doi:10.1164/rccm.201304-0743LE
29. Vaduganathan M, Mensah GA, Turco JV, Fuster V, Roth GA. the global burden of cardiovascular diseases and risk: a compass for future health. J Am Coll Cardiol. 2022;80(25):2361–2371. doi:10.1016/j.jacc.2022.11.005
30. Nordon C, Rhodes K, Quint JK, et al. EXAcerbations of COPD and their OutcomeS on CardioVascular diseases (EXACOS-CV) Programme: protocol of multicountry observational cohort studies. BMJ Open. 2023;13(4):e070022. doi:10.1136/bmjopen-2022-070022
31. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
32. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
33. Han MK, Agusti A, Calverley PM, et al. Chronic obstructive pulmonary disease phenotypes. Am J Respir Crit Care Med. 2010;182(5):598–604. doi:10.1164/rccm.200912-1843CC
34. Soler-Cataluña JJ, Alcázar-Navarrete B, Miravitlles M. The concept of control of COPD in clinical practice. Int J Chron Obstruct Pulmon Dis. 2014;9:1397–1405. doi:10.2147/copd.S71370
35. McDonald VM, Harrington J, Clark VL, Gibson PG. Multidisciplinary care in chronic airway diseases: the Newcastle model. ERJ Open Res. 2022;8(3):00215–2022. doi:10.1183/23120541.00215-2022
36. Agusti A, Bel E, Thomas M, et al. Treatable traits: toward precision medicine of chronic airway diseases. Eur Respir J. 2016;47(2):410–419. doi:10.1183/13993003.01359-2015
37. Kuzma AM, Meli Y, Meldrum C, et al. Multidisciplinary care of the patient with chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(4):567–571. doi:10.1513/pats.200708-125ET
38. McDonald VM, Clark VL, Cordova-Rivera L, Wark PAB, Baines KJ, Gibson PG. Targeting treatable traits in severe asthma: a randomised controlled trial. Eur Respir J. 2020;55(3):1901509. doi:10.1183/13993003.01509-2019
39. Owusuaa C, Dijkland SA, Nieboer D, van der Rijt CCD, van der Heide A, van der Rijt CCD. Predictors of mortality in chronic obstructive pulmonary disease: a systematic review and meta-analysis. BMC Pulm Med. 2022;22(1):125. doi:10.1186/s12890-022-01911-5
40. Tsimogianni AM, Papiris SA, Stathopoulos GT, Manali ED, Roussos C, Kotanidou A. Predictors of outcome after exacerbation of chronic obstructive pulmonary disease. J Gen Intern Med. 2009;24(9):1043–1048. doi:10.1007/s11606-009-1061-2
41. Murakami Y, Yasui H, Sato J, et al. Predictors of poor clinical outcomes including in-hospital death and low ability to perform activities of daily living at discharge in hospitalized patients with chronic obstructive pulmonary disease exacerbation. Ther Adv Respir Dis. 2023;17:17534666231172924. doi:10.1177/17534666231172924
42. Brat K, Plutinsky M, Hejduk K, et al. Respiratory parameters predict poor outcome in COPD patients, category GOLD 2017 B. Int J Chron Obstruct Pulmon Dis. 2018;13:1037–1052. doi:10.2147/copd.S147262
43. Alzaabi O, Guerot E, Planquette B, Diehl J-L, Soumagne T. Predicting outcomes in patients with exacerbation of COPD requiring mechanical ventilation. Ann Intens Care. 2024;14(1):159. doi:10.1186/s13613-024-01394-z
44. Lee H, Shin SH, Gu S, et al. Racial differences in comorbidity profile among patients with chronic obstructive pulmonary disease. BMC Med. 2018;16(1):178. doi:10.1186/s12916-018-1159-7
45. He J, Zhu Z, Bundy JD, Dorans KS, Chen J, Hamm LL. Trends in cardiovascular risk factors in US adults by race and ethnicity and socioeconomic status, 1999-2018. JAMA. 2021;326(13):1286–1298. doi:10.1001/jama.2021.15187
46. Ho FK, Gray SR, Welsh P, et al. Ethnic differences in cardiovascular risk: examining differential exposure and susceptibility to risk factors. BMC Med. 2022;20(1):149. doi:10.1186/s12916-022-02337-w
47. Vanitha DOP, Yeli W, Ngiap Chuan T, Tazeen HJ. Socioeconomic status and ethnic variation associated with type 2 diabetes mellitus in patients with uncontrolled hypertension in Singapore. BMJ Open Diabetes Res Care. 2021;9(1):e002064. doi:10.1136/bmjdrc-2020-002064
48. Lee YH, Shin MH, Kweon SS, et al. Cumulative smoking exposure, duration of smoking cessation, and peripheral arterial disease in middle-aged and older Korean men. BMC Public Health. 2011;11:94. doi:10.1186/1471-2458-11-94
49. Chen G, Mu Q, Meng ZJ. Cigarette smoking contributes to th1/th2 cell dysfunction via the cytokine milieu in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2023;18:2027–2038. doi:10.2147/copd.S426215
50. Maddatu J, Anderson-Baucum E, Evans-Molina C. Smoking and the risk of type 2 diabetes. Transl Res. 2017;184:101–107. doi:10.1016/j.trsl.2017.02.004
51. Goh KJ, Chai HZ, Ng LS, et al. Outcomes of second-tier rapid response activations in a tertiary referral hospital: a prospective observational study. Ann Acad Med Singap. 2021;50(11):838–847. doi:10.47102/annals-acadmedsg.2021238
52. Zhong N, Moon HS, Lee KH, et al. TIOtropium safety and performance in respimat® (TIOSPIRTM): analysis of Asian cohort of COPD patients. Respirology. 2016;21(8):1397–1403. doi:10.1111/resp.12856
53. Loh L-C, Oh Y-M, Lee S-D. Researchers oBoA. The Asian Network for Obstructive Lung Disease (ANOLD)-COPD from an Asian perspective. QJM. 2015;108(12):921–922. doi:10.1093/qjmed/hcv109
54. Nishimura M. Similarities and differences between East and West in COPD. Respirology. 2016;21(8):1340–1341. doi:10.1111/resp.12914
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Elevated Thyroid Stimulating Hormone with Atherosclerotic Cardiovascular Disease and Its Mortality in Elderly Community-Dwelling Chinese
Wang Y, Liu C, Liu L, Chen X, Wei L, Liu J, Peng S, Pi J, Zhang Q, Tomlinson B, Chan P, Zhang L, Fan H, Zheng L, Liu Z, Zhang Y
Clinical Interventions in Aging 2022, 17:1139-1150
Published Date: 2 August 2022
The Relationship Between the Neutrophil Percentage-to-Albumin Ratio and Rates of 28-Day Mortality in Atrial Fibrillation Patients 80 Years of Age or Older
Cai J, Li M, Wang W, Luo R, Zhang Z, Liu H
Journal of Inflammation Research 2023, 16:1629-1638
Published Date: 17 April 2023
The Relationship Between Fracture and Mortality in a Chinese Maintenance Hemodialysis Patients Cohort
Liu X, Liu Z, Niu Y, Zhang K, Zhang X, Yu C
Journal of Multidisciplinary Healthcare 2024, 17:2031-2038
Published Date: 1 May 2024
Prevalence and Risk Factors of Cardiovascular Disease in Rheumatoid Arthritis Patients: A Comparative Analysis of Real-World Data
Tekeoglu S
International Journal of General Medicine 2024, 17:5859-5868
Published Date: 6 December 2024
Extremely High Systemic Immune Inflammation Levels Increase the Risk of All-Cause and Cardiovascular Mortality in Postmenopausal Women
Wu F, Yang J, Liu Y, Zhang Y
International Journal of Women's Health 2025, 17:1457-1468
Published Date: 20 May 2025