")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Prognostic Analysis of Elderly Patients with Hepatocellular Carcinoma: an Exploration and Machine Learning Model Prediction Based on Age Stratification and Surgical Approach
Authors Cai C, Zhu H, Li B, Tang C, Ren Y, Guo Y, Li J, Wang L, Li D, Li D
Received 27 December 2024
Accepted for publication 27 March 2025
Published 14 April 2025 Volume 2025:12 Pages 747—764
DOI https://doi.org/10.2147/JHC.S512410
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Ahmed Kaseb
Chiyu Cai,1,* Hengli Zhu,1,* Bingyao Li,2,* Changqian Tang,3 Yongnian Ren,1 Yuqi Guo,1 Jizhen Li,1 Liancai Wang,1 Deyu Li,1 Dongxiao Li4
1Department of Hepatobiliary and Pancreatic Surgery, Zhengzhou University People’s Hospital, Zhengzhou, Henan, People’s Republic of China; 2Henan Provincial People’s Hospital, Xinxiang Medical University, Zhengzhou, Henan, People’s Republic of China; 3Department of Hepatobiliary and Pancreatic Surgery, Henan University People’s Hospital, Zhengzhou, Henan, People’s Republic of China; 4Department of Gastroenterology, Zhengzhou University People’s Hospital, Zhengzhou, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Deyu Li, Zhengzhou University People’s Hospital, No. 7, Wei Wu Road, Jinshui District, Zhengzhou, Henan, People’s Republic of China, Email [email protected] Dongxiao Li, Zhengzhou University People’s Hospital, No. 7, Wei Wu Road, Jinshui District, Zhengzhou, Henan, People’s Republic of China, Email [email protected]
Purpose: As the global population ages, precise prognostic tools are needed to optimize postoperative care for elderly hepatocellular carcinoma (HCC) patients. This study established a machine learning-driven predictive model to identify key prognostic determinants and evaluate age/surgical approach impacts, overcoming limitations of traditional statistical methods.
Methods: This retrospective study included 252 postoperative HCC patients aged ≥ 65 years (mean age 69.0± 4.3; 68.25% male). Patients were randomly divided into training (70%, n=177) and validation sets (30%, n=75). We evaluated 147 machine learning models to establish the optimal predictive model. Patients were grouped by age (> 75 vs ≤ 75 years) and surgical approach (laparoscopic vs open).
Results: The LASSO+RSF model showed strong predictive performance with AUC values of 0.869 and 0.818 in the training and validation sets, respectively. Time-dependent AUCs for 1-, 2- and 3-year survival were 0.874, 0.903, and 0.883 in the training set, and 0.878, 0.882, and 0.915 in the validation set. Key predictors included age-adjusted Charlson index (ACCI, LASSO+RSF synergistic weight (LRSW) =0.160), microvascular invasion (0.111), tumor capsule integrity (0.034), and lymphatic invasion (0.023), while three variables (intraoperative blood loss, tumor margin, WBC) were excluded (LRSW< 0.01). A web-based dynamic nomogram (https://cliniometrics.shinyapps.io/LRSF-GeroHCC/) enabled real-time risk stratification. Patients > 75 years had longer length of stay (16 vs 14 days, P=0.033), higher Clavien-Dindo scores (P=0.014), higher ACCI scores (5.5 vs 4.0, P=0.002), and lower PFS (16.5 vs 24 months, P=0.041). Laparoscopic surgery was associated with longer operative time (202.5 vs 159.0min, P< 0.001), shorter length of stay (14 vs 17days, P< 0.001), and lower Clavien-Dindo scores (P=0.038).
Conclusion: The LASSO+RSF model provides validated tools for personalized prognosis management in elderly HCC patients, emphasizing age-adapted surgical strategies and comorbidity-focused perioperative care.
Keywords: hepatocellular carcinoma, geriatric oncology, age-adjusted Charlson comorbidity index, machine learning, survival prediction, minimally invasive surgery
Introduction
Hepatocellular carcinoma (HCC), the most common subtype of liver cancer, accounts for 90% of cases and is the sixth most prevalent malignant tumor worldwide.1 Despite advances in treatment, HCC remains associated with high mortality and poor prognosis, with no sufficiently accurate methods for predicting postoperative comorbidities and tumor recurrence.2–4 This presents a significant public health challenge as the global burden of HCC continues to rise. Furthermore, the aging global population has led to an increasing incidence of HCC among elderly individuals, particularly in China, which has the largest and fastest-growing aging population.5,6
Elderly patients with HCC often experience rapid disease progression, high lethality, and shorter postoperative survival.7 They also exhibit higher in-hospital mortality and comorbidity rates due to a higher prevalence of underlying conditions, such as diabetes, and poorer overall health.7–9 Surgery remains the primary treatment for HCC, with laparoscopic hepatectomy gaining prominence in recent years due to its advantages of less trauma and quicker recovery.10–13 However, the optimal surgical approach for elderly HCC patients whether laparoscopic or open surgery remains a topic of debate.14 Additionally, elderly patients often face higher postoperative complication and mortality rates due to their compromised baseline status and coexisting comorbidities.15
Accurate preoperative assessment of an elderly patient’s baseline status to predict postoperative outcomes is crucial for optimizing treatment strategies. While factors such as body mass index, inflammatory markers, tumor markers, tumor growth characteristics, and cirrhosis have been linked to prognosis,16–20 few studies have addressed the prognostic impact of age stratification within elderly populations. For instance, higher age-adjusted Charlson Comorbidity Index (ACCI) scores have been shown to significantly influence outcomes,21 yet the prognostic differences between patients aged 65–75 years and those over 75 years remain unclear.22–24
This study aimed to address these gaps by analyzing intraoperative factors and prognostic outcomes among elderly HCC patients stratified by age groups (65–75 years and > 75 years) and surgical modalities. We found that patients over 75 years had higher ACCI scores and Clavien-Dindo grade indices, while those undergoing laparoscopic surgery experienced fewer complications and longer overall survival (OS) and progression-free survival (PFS). Furthermore, we developed a preoperative risk prediction model using a machine learning approach, evaluating 147 models to identify the best-performing model: least absolute shrinkage and selection operator + random survival forest (LASSO + RSF). This model, validated by area under the curve (AUC), C-index, sensitivity, and specificity, offers a robust tool for preoperative risk stratification, intervention planning, and improved management of elderly HCC patients, ultimately enhancing patient outcomes and quality of life.
Methods
Patients
A step-by-step diagram of the process of this study is shown (Figure 1). A total of 835 patients diagnosed with HCC at Zhengzhou University People’s Hospital from January 2018 to June 2024 were initially identified for this study; and 252 elderly patients with HCC were ultimately included after applying the inclusion and exclusion criteria. The patient’s medical record data was collected by retrospective analysis. This study was approved by the Ethical Review Committee of Zhengzhou University People’s Hospital (Approval No. (2023) Ethic Review No. (12)). Informed consent was waived because this study was retrospective. All patient data were anonymized and handled in strict compliance with confidentiality regulations. The study was conducted in accordance with the Declaration of Helsinki.
 |
Figure 1 Flowchart of study design and patient selection. Abbreviations: HCC, hepatocellular carcinoma; C-index, concordance index; AUC, area under the ROC curve; KM curve, Kaplan-Meier curve; RSF, random survival forests. |
Inclusion Criteria
(1) Age ≥ 65 years, (2) Tolerable to surgical treatment, (3) No history of malignant tumor and surgery, (4) No anti-tumor treatment before operation, (5) Pathological diagnosis was confirmed as HCC.
Exclusion Criteria
(1) Age < 65 years. (n = 414), (2) History of other malignancies. (n = 35), (3) Conversion to open surgery or palliative resection during the operation. (n = 63), (4) Preoperative Antitumor Therapy. (n = 41), (5) Incomplete clinical medical records. (n = 30).
Surgery Procedure
The study included patients undergoing radical hepatectomy for HCC, which included both laparoscopic and open surgical procedures. Each patient was placed supine and intubated for general anesthesia administration. In the laparoscopic group, an incision of about 10 mm was made at the lower edge of the umbilicus. Carbon dioxide pneumoperitoneum was established, and the intra-abdominal pressure was maintained at 12–14 mmHg (1 mmHg = 0.133 kPa). 10 mm Trocar was used as the lens hole, and a laparoscope was placed to explore the feasibility of the operation, and other Trocars were inserted under laparoscopic guidance, with 12 mm Trocar and 5 mm Trocar being placed into each of the left and right upper abdomens, respectively. A 12 mm Trocar and a 5 mm Trocar were placed in the left and right upper abdomen, respectively, as the primary and secondary operating holes. The position of the operation holes was adjusted according to the hepatic resection site. The perihepatic ligament was freed and the liver segment where the lesion was located was exposed. Depending on the location of the lesion, the surgical approach, and the degree of cirrhosis, the method of hepatic flow blockade is determined. Selective hemihepatic flow obstruction was used for anatomical hemihepatectomy, for lesions located in the left outer lobe, right posterior lobe, or right anterior lobe, intermittent Pringle’s method was used if necessary (strictly 15 min of blockade and 5 min of opening) or dissection of the corresponding hepatic pedicle for selective local blockade. An ultrasonic knife was used to transect the hepatic parenchyma, combined with a linear cutting stapler (EC60) to separate the hepatic parenchyma from the Glisson system. During liver resection, small ducts and liver parenchyma distant from the hepatic pedicle and main trunk of the hepatic vein can be coagulated and divided using an ultrasonic scalpel or Ligasure, thicker ducts could be clamped with absorbable clips, peptide clips, or Hem-o-lock vascular clips and then dissected, bleeding on the liver wound surface is controlled using high-frequency electrocoagulation and spray coagulation modes, while bleeding caused by vascular retraction on the liver wound surface is managed with laparoscopic suturing for hemostasis. After achieving precise hemostasis under the laparoscope, an abdominal drainage tube is placed.
In the open surgery group, an oblique incision of about 25 cm was made under the right costal arch, and the abdomen was entered layer by layer, and the hepatic falciform ligament, hepatic colonic ligament, hepatic-kidney ligament, right deltoid ligament, and right coronary ligament were successively cut open. After freeing the liver, the mass was revealed, and according to the location of the tumor, the blood flow into the liver was blocked by selecting the whole liver or half of the liver, and the blocking method was similar to that of the laparoscopic resection (LR) group. After intraoperative ultrasonography, parenchymal transection was performed with ring clamps, and major vascular structures could be ligated or sutured. Definitive hemostasis was achieved, and an abdominal drain was placed.
Data Collection
After confirming the diagnosis of HCC by postoperative histological pathology, data were collected from the electronic medical record system. General clinical information included age, gender, hepatitis B virus (HBV), cirrhosis, Child-Pugh, BCLC stage, albumin (ALB), aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (TBil), white blood cell(WBC), red blood cell(RBC), platelet(PLT), prothrombin time(PT), carcinoembryonic antigen (CEA), alpha-fetoprotein (AFP), operative time, intraoperative blood loss, length of stay, hospital costs, surgical approach, and preoperative imaging information including intratumor necrosis, intratumor hemorrhage, satellite nodule, tumor number, tumor diameter, tumor capsule, tumor margin, exophytic growth, imaging information was reviewed by two hepatobiliary surgeons with 10 years of experience and in case of disputes decision making was sought from hepatobiliary surgeons with more than 30 years of experience. Postoperative histopathological information included Edmondson grade, microvascular invasion, perineural invasion, lymphatic invasion.
OS was defined as the time from the date of surgery to the endpoint of follow-up, including the date of the patient’s death or the date of the last effective follow-up. PFS was defined as the time from the start of randomization to tumor progression or death from any cause. Operative time was defined as the time from skin incision to completion of suturing, and intraoperative bleeding was assessed by measuring the weight of gauze and changes in blood volume in the suction device.
Follow-up included PFS and OS. Follow-up was in the form of outpatient follow-up or telephone follow-up. Tumor markers such as AFP, CEA, and imaging tests were performed regularly during the follow-up period. Follow-up continues until June 2024 to record patients’ OS and PFS at 1, 2, and 3 years.
Preoperative Comorbidity and ACCI
The ACCI scoring system assigns points based on preoperative comorbidities and age. The scoring criteria are as follows: 1 point is assigned to patients with the following comorbidities: myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic pulmonary disease, connective tissue disease, ulcer disease, mild liver disease, hypertension, and diabetes. 2 points are assigned for the combination of the following diseases: moderate or severe renal disease, diabetes with end-organ damage, solid tumor, hemiplegia, leukemia, and malignant lymphoma. 3 points are given for moderate or severe liver disease. 6 points are given for a combination of metastatic solid tumor or acquired immunodeficiency syndrome (AIDS). Additionally, patients are scored based on age: The risk increases by 1 point for every 10 years above 40 years (50–59 years: 1 point; 60–69 years: 2 points; 70–79 years: 3 points; >80 years: 4 points). Total ACCI score is the sum of comorbidity points and age points.25,26 The distribution of preoperative comorbidities and the ACCI scoring criteria are shown (Table S1).
Clavien-Dindo Grade
The specific grading criteria are as follows: Grade I: Mild symptoms such as slight nausea or low-grade fever, usually self-limiting, without the need for medication. Grade II: Complications that require drug treatment, including blood transfusions and parenteral nutrition. Grade III: Complications requiring surgical intervention, interventional procedures, or endoscopic treatment. Grade IIIb involves the need for general anesthesia, while Grade IIIa does not. Grade IV: Life-threatening complications requiring intensive care unit (ICU) management. Grade IVa refers to single organ failure (including dialysis), and Grade IVb refers to multiple organ failure. Grade V: Death.27,28 The types and numbers of postoperative complications for all patients are shown (Table S2).
Machine Model Construction
In this study, we systematically evaluated 147 machine learning models encompassing 14 algorithms (LASSO, RSF, obliqueRSF, survival-SVM, GBM, CoxBoost, StepCox, ElasticNet, Ridge, XGBoost, SuperPC, plsRcox, CForest, CTree) and their hybrid combinations. All models underwent stratified 10-fold cross-validation on the training cohort, with folds stratified by event status and time-to-event quantiles to preserve survival data dynamics. Hyperparameters were tuned via grid search: LASSO/Ridge/ElasticNet regularization strength λ spanned 100 log-spaced values (10−5 to 102), with ElasticNet’s α parameter iterated from 0 to 1 in 0.1 increments; RSF employed a fixed node size of 5 (validated through sensitivity analyses) and randomly subsampled ⌈√p⌉ features per split (p = total features); XGBoost optimized learning rate (0.01–0.3), maximum depth (5–10), and subsampling ratio (0.6–1). To mitigate overfitting, the optimal LASSO+RSF model integrated dual regularization: LASSO’s 1-standard-error rule selected λ_min, retaining 8 predictors, while RSF utilized bootstrap aggregation (1000 trees, 63.2% case sampling per tree) with √p feature randomization. Model performance was rigorously validated on an independent hold-out set (30%, n=76) using survival-specific metrics: time-dependent AUC (1/2/3-year), C-index, DCA, PR curve, Brier score and Integrated Brier Score (IBS). Reproducibility was ensured through fixed random seeding (seed=123) applied to all stochastic processes.
Based on the final prediction model, we developed an interactive web-based nomogram using the shiny package (version 1.7.5) in R (version 4.3.2). This dynamic tool allows clinicians to adjust predictors through slider bars or numeric input interfaces, generating real-time individualized survival probability predictions with 95% confidence intervals. The backend system integrates model parameters seamlessly via the plumbr package, presenting results through synchronized visualizations (simulated Kaplan-Meier curves) and numerical reports (1-, 3-, 5-year survival rates). The application is accessible via standard web browsers (URL: https://cliniometrics.shinyapps.io/LRSF-GeroHCC/).
Data Processing and Analysis
SPSS (version 26.0) and R software (version 4.3.2) were used for data analysis. Missing data were handled as follows: For samples with 1–2 missing values, median imputation was applied to quantitative variables, and mode imputation was used for categorical variables. Normally distributed continuous variables were expressed as mean ± standard deviation (‘x ± s), and a t-test was used for difference analysis; skewed continuous variables were expressed as median (Q1, Q3), and a Mann–Whitney U-test was used for difference analysis. Categorical variables were expressed as absolute numbers, the chi-square test was used for difference analysis, and the Fisher test was used when 1 ≤ n < 5. Univariate and multivariate analyses were performed using Cox proportional risk models for patients with 3-year OS and PFS. Survival was estimated by the Kaplan-Meier method and the corresponding survival curves were plotted. The predictive performance of the machine learning models was assessed by AUC, C-index, Brier score and IBS. P < 0.05 were considered statistically significant.
Results
Patient Characteristics
A total of 252 patients were included in this study. The clinical features of the entire data set are shown (Table 1). Among them, 43 patients (17.06%) were > 75 years, and 209 patients (82.94%) were 65–75 years. Among these patients, 172 were male (68.25%) and 80 were female (31.75%). The average age was 69.0±4.3 years. ACCI scores, a key predictor for comorbidities, had a median of 4.0 (3.0, 6.0), which did not show a significant increase with age. The most frequent comorbidities included mild liver disease (89 cases, 35.32%), ulcer disease (72 cases, 28.57%), hypertension (65 cases, 25.79%), chronic pulmonary disease (45 cases, 17.86%), and moderate/severe liver disease (44 cases, 17.46%) (Table S1), highlighting the need for perioperative focus on gastrointestinal, respiratory, and circulatory systems in geriatric care. In addition, 113 patients (44.84%) underwent laparoscopic surgery, and 139 patients (55.16%) underwent open surgery. The median operation time was 185.5 (146.0, 239.3) minutes, and the median intraoperative blood loss was 200.0 (100.0, 276.3) mL. Clavien-Dindo classification: There were 160 cases (63.49%) in the low Clavien-Dindo group (Clavien-Dindo < 3) and 92 cases (36.51%) in the high Clavien-Dindo group (Clavien-Dindo ≥ 3). The most frequent complications included electrolyte disturbances (85 cases, 33.73%), malnutrition (81 cases, 32.14%), infections (62 cases, 24.60%), anemia (46 cases, 18.25%), and ascites (38 cases, 15.08%), emphasizing the high prevalence of nutrition-related challenges in elderly surgical populations (Table S2).
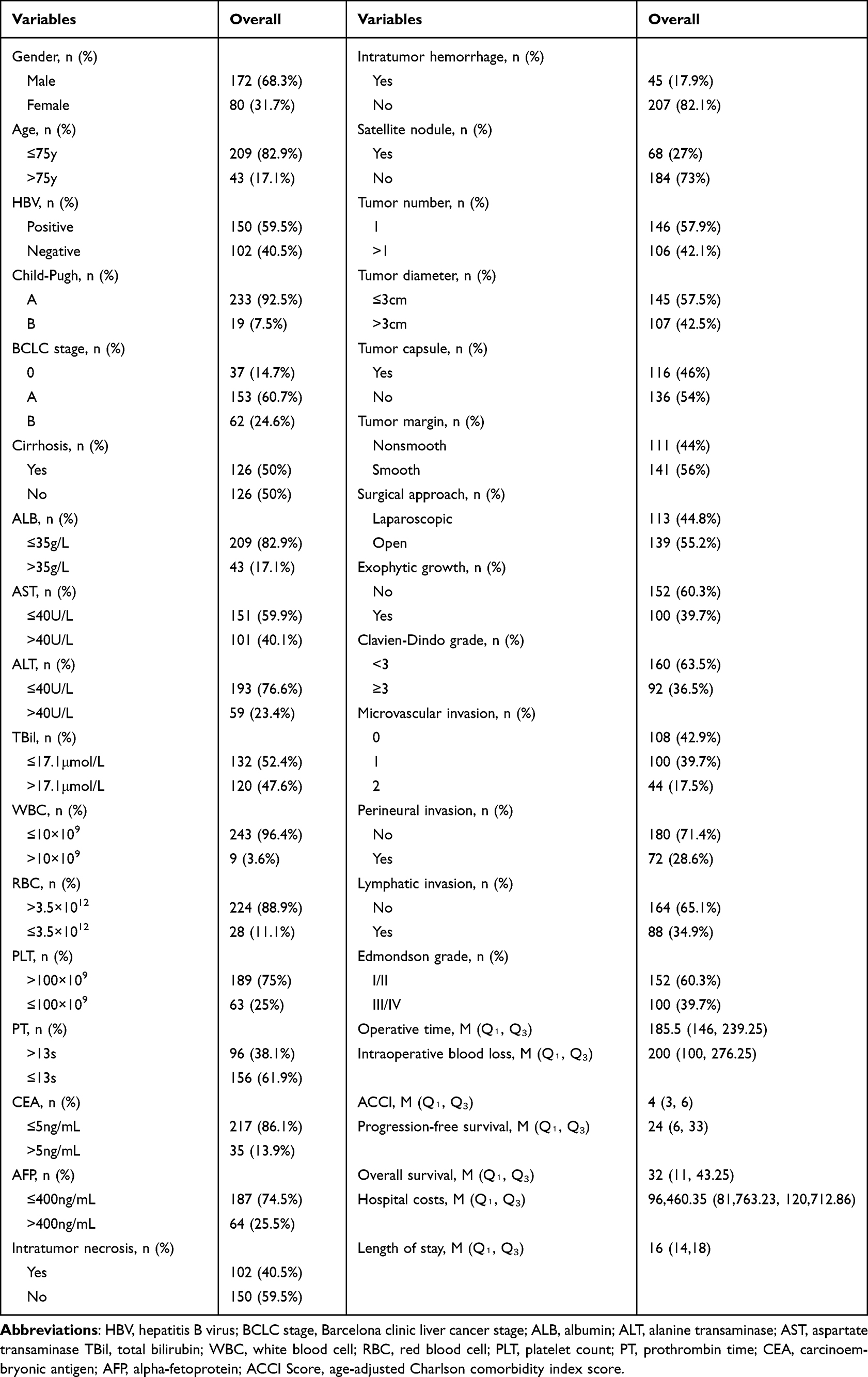 |
Table 1 Patient Characteristics |
In terms of follow-up, 252 patients were followed up in this study, and the median OS was 32.0 (11.0, 43.3) months. The median PFS was 24.0 (6.0, 33.0) months.
Comparison of Prediction Efficiency of Different Models
The data were randomly divided into a training set (70%, n = 177) and a validation set (30%, n = 75). There was no significant difference between the two sets (Table 2).
 |
Table 2 Dataset Partition Table |
A total of 147 combinations of machine learning models were constructed. We calculated the average C-index of each model in both cohorts to assess the models’ predictive performance (Figure 2A). The models were ranked and compared visually, showing that the LASSO + RSF model achieved the highest accuracy, with a combined AUC of 0.843, demonstrating strong predictive power. The prediction efficacy for 1-year, 2-year, and 3-year survival in the training set was 0.874, 0.903, and 0.883, respectively, and in the validation set was 0.878, 0.882, and 0.915, respectively (Figure 2B and C). Calibration curves further confirmed excellent agreement between predicted and observed outcomes in both cohorts (Figure 2D and E).
 |
Figure 2 Performance comparison of prediction models. (A) ROC curves of different models (LASSO+RSF, RSF, RSF+obliqueRSF, RSF+GBM, CoxBoost+RSF) in the training cohort; (B) ROC curves in the validation cohort; (C) Decision curve analysis (DCA) in the training cohort; (D) DCA in the validation cohort; (E) Precision-recall (PR) curves in the training cohort; (F) PR curves in the validation cohort. |
To validate LASSO+RSF’s optimality, we conducted head-to-head comparisons of the top 5 models by C-index (LASSO+RSF, RSF, RSF+obliqueRSF, RSF+GBM, CoxBoost+RSF). Comprehensive performance evaluation incorporating AUC analysis, decision curve analysis (DCA), and precision-recall (PR) curves demonstrated LASSO+RSF’s consistent superiority in both training and validation sets, with significantly higher AUC values in both training (0.883 vs comparator range 0.839–0.881) and validation cohorts (0.915 vs 0.863–0.906). DCA indicated enhanced clinical net benefit, while PR curves revealed higher precision and true positive rates (Figure 3). Additional validation through Brier scores and integrated Brier scores (IBS) at 1–3 years confirmed LASSO+RSF’s stability advantage (Table S3).
 |
Figure 3 Screening and validation of machine learning models. (A) C-index values of 147 combined models in the training (blue) and validation (Orange) groups, ranked by mean C-index. (B and C) Time-dependent ROC curves at 1-, 2-, and 3-year overall survival (OS) for the LASSO+RSF model in training and validation groups. (D and E) Calibration curves comparing predicted vs observed survival probabilities (dashed line: ideal fit). (F and G) Kaplan-Meier curves for OS stratified by LASSO+RSF risk groups (log-rank P<0.001). (H and I) Kaplan-Meier curves for progression-free survival (PFS) in risk groups (log-rank P<0.001). |
Variable importance weighting via LASSO+RSF identified key prognostic determinants: ACCI (0.160), MVI (0.111), tumor capsule (0.034), lymphatic invasion (0.023), intraoperative blood loss (0.008), tumor margin (0.002), and white blood cell count (0.0003) (Figure 4 and Table 3). Three variables (intraoperative blood loss, tumor margin, white blood cell) were excluded based on their synergistic weight scores (LRSW <0.01), indicating minimal combined contribution from both regularization and survival importance metrics. For clinical translation, we developed an interactive web-based dynamic nomogram (https://cliniometrics.shinyapps.io/LRSF-GeroHCC/) enabling real-time prognostic assessment through intuitive parameter input (Figure 5).
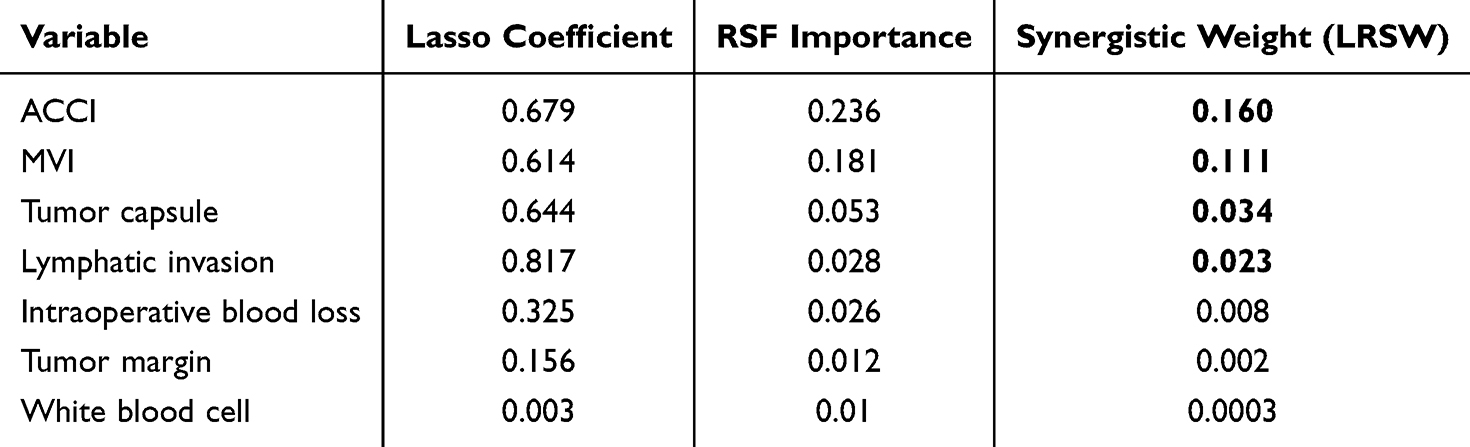 |
Table 3 Comparative Feature Significance Assessment |
 |
Figure 4 Top 7 variables ranked by importance scores in the LASSO+RSF model. Synergistic weight matrix showing combined effects of LASSO-selected features and RSF survival analysis. |
 |
Figure 5 Web-based dynamic nomogram for survival prediction. Interactive nomogram integrating clinical variables to estimate 1-, 2-, and 3-year survival probabilities (URL: https://cliniometrics.shinyapps.io/LRSF-GeroHCC/). |
Additionally, the recurrence risk score was calculated using the model, and patients were divided into low-risk and high-risk groups according to the median score. Kaplan-Meier curves related to OS and PFS in the training and validation sets were plotted to compare the prognostic differences. The results show a statistical difference (P < 0.001) in both the training set and validation set (Figure 2F–I).
Age Grouping Analysis of Influencing Factors
The patients in the training set were divided into two groups, > 75 years (n = 30) and 65–75 years (n = 147), and the distribution circles of the relevant variables for patients in the age subgroups are shown (Figure 6). The screened variables were put together with the latent variables and statistically compared between the age subgroups. The results showed statistical differences between Length of Stay (LOS) (age≤75 vs >75:16.0days vs 14.0days, P = 0.033), PFS (16.5months vs 14.0moths, P = 0.041), ACCI (5.5 vs 4.4, P = 0.002), Clavien-Dindo grade≥3 (53.3% vs 29.9%, P = 0.014) (Table 4) and in the validation set, PFS (8.0months vs 24.0months, P = 0.044), ACCI (6.0 vs 4.0, P < 0.001), Clavien- Dindo grade≥3 (69.23% vs 37.10%P = 0.033) were statistically different from each other (Table S4).
 |
Table 4 Feature Distribution by Age Groups in the Training Group |
 |
Figure 6 Radar plots of surgical group characteristics. (A) Training group. (B) Validation group. Abbreviations: LOS, length of stay; HC, hospital costs; PFS, Progression-free survival; OS, overall survival; OT, operative time; IBL, intraoperative blood loss; CD grade, Clavien-Dindo grade. |
Surgical Approach Grouping Analysis of Influencing Factors
The patients in the training set were divided into open surgery group (n = 105) and laparoscopic surgery group (n = 72). The circle plots of the distribution of the relevant variables of the patients grouped by surgical modality were shown (Figure 7). The results showed statistically significant differences between operative time (OT) (laparoscopic vs open: 202.5min vs 159.0min, P < 0.001), LOS (14.0days vs 17.0days, P < 0.001), and Clavien-Dindo grade≥3 (25% vs 40%, P = 0.038) (Table 5). In the validation set, the difference between OT (220min vs 180min, P = 0.011), LOS (14.5days vs 16.0days, P = 0.011), Clavien-Dindo≥3 grade (25% vs 53.19%, P = 0.017) was statistically significant (Table S5).
 |
Table 5 Feature Distribution by Surgical Approaches in the Training Group |
 |
Figure 7 Radar plots of age-stratified group characteristics. Patients were stratified by age groups (≤75, >75 years). (A) Training group. (B) Validation group. Abbreviations: LOS, length of stay; HC, hospital costs; PFS, progression-free survival; OS, overall survival; ACCI, age-adjusted Charlson comorbidity index; OT, operative time; IBL, intraoperative blood loss; CD grade, Clavien-Dindo grade; LI, lymphatic invasion; MVI, microvascular invasion. |
Discussion
HCC is a solid tumor with rapid clinical progression and a high degree of malignancy, which poses a serious threat to patients due to its high morbidity, mortality, recurrence, and invisibility.1,3 Despite the continuous expansion of clinical treatment options for tumors, surgical resection remains the primary treatment for primary liver cancer.10 However, for elderly patients, whether they can benefit from surgical treatment and the impact of such treatment on their quality of life remains controversial. Particularly in older patients, it is still necessary to gather more clinical data to determine whether surgery can significantly improve survival outcomes. Additionally, while laparoscopic liver cancer resection has been widely applied, its suitability in elderly patients, especially those over 75 years old, requires further investigation.
Machine learning is increasingly applied in clinical decision-making, disease diagnosis, and predicting patient prognosis.29,30 Our study is the first to apply machine learning models to predict postoperative prognosis in elderly patients with HCC. We utilized 147 ensemble models and ultimately selected the best model, LASSO+RSF, which helped overcome the limitations of individual algorithms. Through the analysis of influencing factors using the LASSO+RSF model, we identified the most important factors affecting patient prognosis: ACCI score, MVI, tumor capsule, lymphatic invasion. The ACCI score is positively correlated with age, reflecting the patient’s preoperative baseline health status. A higher ACCI score (≥4) indicates that older patients with multiple comorbidities may have a poorer prognosis after surgical treatment. Among the comorbidities observed in this study, mild liver disease was the most common (89 cases), followed by peptic ulcer, hypertension, and chronic obstructive pulmonary disease, with 72, 65, and 45 cases, respectively (Table S1). These comorbidities should be addressed with preoperative interventions and postoperative education to control disease progression. Previous studies have shown that the ACCI score significantly affects postoperative prognosis in HCC and other malignancies.31–33However, since the severity of patients varies across different centers, specific standards should be based on each center’s previous experience. Therefore, strict adherence to surgical indications is crucial for these patients. Furthermore, preoperative clinical interventions and active control of comorbidities can improve patients’ quality of life and long-term survival outcomes.
MVI was also a key factor influencing patients’ postoperative prognosis. Previous studies have shown that higher MVI grade or MVI positivity was significantly associated with poor prognosis in patients with HCC.34–36 Moreover, studies have shown that age was a clinical variable that was significantly associated with MVI.37,38 Hu et al15 found that both greater than 75 years of age and MVI positivity were independent risk factors affecting the postoperative prognosis of HCC, a finding further confirmed in our study. In addition, the tumor capsule, composed of fibrous tissue, partially isolates the tumor from the surrounding liver tissue, limiting further tumor expansion. Multiple studies have indicated that tumor capsule rupture or the absence of a capsule in liver cancer is closely associated with higher MVI and early recurrence39,40 Lymphatic invasion is another important prognostic indicator in HCC, often linked to tumor invasiveness, reflecting the extent of tumor spread from the primary site to distant organs, directly impacting patient prognosis. To facilitate clinical application of the model, we developed a web-based dynamic nomogram based on the model. Clinicians can input patients’ risk assessment scores to obtain survival and prognostic probabilities. When a patient’s predicted postoperative survival probability is low, physicians should actively communicate with the patient, fully disclose surgical risks, and if surgery is pursued, optimize preoperative evaluations and aggressively manage preexisting comorbidities.
Additionally, a study from an international multicenter database emphasized that advanced age alone should not be the determinant for surgical eligibility. They stratified age groups and developed validated models to support this conclusion. Our approach differs in that we did not use traditional logistic regression or Cox survival analysis during data analysis. Instead, we constructed and selected the optimal model through different modeling approaches, which may result in higher predictive accuracy compared to their methods.41 In this study, elderly HCC patients of different age groups (age ≤ 75 versus age > 75) were compared for relevant risk factors and found that PFS, ACCI, and Clavien-Dindo grades were statistically different in both the training and validation groups and that patients over 75 years of age had a shorter PFS as well as a higher ACCI and Clavien-Dindo grade scores, suggesting that patients over 75 years of age have poorer short-term prognosis and long-term prognosis, a trend that was also demonstrated in a study by Hatanaka et al.24 Therefore, when the age of HCC patients over 75 years, the choice of surgical treatment should be made with greater caution. A detailed preoperative assessment of the patient’s overall health status is necessary to determine whether they can truly benefit from surgical intervention.
This study confirms that laparoscopic surgery demonstrates clear perioperative advantages in elderly HCC patients: compared to open surgery, it significantly shortens hospital stays (mean reduction of 3.0 days), decreases the incidence of postoperative complications (particularly a 15% risk reduction in Clavien-Dindo grade ≥III severe complications), thereby improving short-term patient outcomes. These findings align closely with those of Xiang et al,42 who reported a 15.5% reduction in postoperative complications in the laparoscopic group compared to the open group (P = 0.003). Similarly, Amato’s cohort further validated these benefits, with laparoscopic cases demonstrating 33% fewer minor complications (P = 0.02) and 112 mL less blood loss, albeit with comparable operative times (P = 0.73).12 Despite the superior perioperative outcomes of laparoscopic surgery, the average operative time is prolonged by approximately 43.5 minutes (P < 0.001), which may relate to the learning curve for instrumentation and the selection of complex cases. Besides, while no significant cost difference was observed in this study (P = 0.132), regional economic disparities and healthcare resource allocation must be considered. A recent meta-analysis incorporating seven cohort studies43 similarly highlights the cross-study consistency in reduced hospital stays and complications for laparoscopic groups, though the extent of prolonged operative time showed significant heterogeneity across centers, suggesting that technical proficiency may critically influence this metric. Regarding oncological outcomes, our study found no significant differences in overall survival (P = 0.243) or progression-free survival (P = 0.104) between laparoscopic and open surgery, consistent with the findings of Chen K et al.44 Based on current evidence, we recommend prioritizing laparoscopic surgery for elderly HCC patients, with individualized decision-making guided by: (1) the technical capacity of the medical center; (2) regional socioeconomic considerations (cost-effectiveness evaluations are essential in areas with limited insurance coverage).
This study has several limitations. It is a single-center, retrospective study, and although the predictive performance was high, multi-center external validation is needed. Additionally, the predominance of hepatitis B-related HCC and the higher proportion of male patients in China may introduce selection bias. Despite employing 10-fold cross-validation, potential bias and overfitting risks remain, necessitating caution regarding the model’s generalizability due to sample size constraints. In the future, we plan to conduct external validation using data from hospitals in regions with low HBV prevalence, focusing on monitoring predictive performance deviation in non-HBV populations, presetting an acceptable AUC difference threshold of ≤0.10. Furthermore, we will implement prospective cohort studies at centers with expertise in laparoscopic surgery to integrate the model predictions with surgical decision trees and validate its predictive capability.
Despite these limitations, we successfully developed Web-based Dynamic Nomogram based on the LASSO+RSF model. Key factors influencing the prognosis of elderly HCC patients included ACCI score, MVI, tumor capsule and lymphatic invasion. Patients over 75 years old had poorer short- and long-term outcomes. Laparoscopic surgery, while increasing surgical time, reduced postoperative complications, offering valuable insights for clinical treatment decisions in elderly HCC patients.
Conclusion
A predictive model was successfully established to forecast postoperative prognosis in elderly HCC patients, and by comparing different age groups and surgical approaches, valuable insights for clinical treatment decisions were provided.
Ethical Approval
This study was conducted in strict adherence to the ethical guidelines and principles of the Declaration of Helsinki and was approved by the Ethics Committee of Zhengzhou University People’s Hospital ((2023) Ethic Review No. (12)). This research is a retrospective study that only collected patient data from medical records. Informed consent from the participants was waived by the Ethics Committee of Zhengzhou University People’s Hospital.
Acknowledgments
We would like to express our gratitude to Dr. Haibo Yu for his valuable assistance in drafting and reviewing the ethical statement of this manuscript.
Funding
National Natural Science Foundation of China (Grant No. 82103617 and 82103618); Scientific and technological project of Henan Province (Grant No. 232102311024 and 232301420056); Henan Provincial Young and Middle-aged Health Science and Technology Innovation Talent (Grant No. YXKC2021049 and YXKC2021048).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
3. Rahib L, Wehner MR, Matrisian LM, Nead KT. Estimated projection of US cancer incidence and death to 2040. JAMA Network Open. 2021;4(4):e214708. doi:10.1001/jamanetworkopen.2021.4708
4. Qi J, Li M, Wang L, et al. National and subnational trends in cancer burden in China, 2005-20: an analysis of national mortality surveillance data. Lancet Public Health. 2023;8(12):e943–e955. doi:10.1016/s2468-2667(23)00211-6
5. Lu LG, Zhou ZL, Wang XY, et al. PD-L1 blockade liberates intrinsic antitumourigenic properties of glycolytic macrophages in hepatocellular carcinoma. Gut. 2022;71(12):2551–2560. doi:10.1136/gutjnl-2021-326350
6. Xia C, Dong X, Li H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chinese Med J. 2022;135(5):584–590. doi:10.1097/cm9.0000000000002108
7. Lee JS, Park DA, Ryoo S, Park J, Choi GH, Yoo JJ. Efficacy and safety of surgical resection in elderly patients with hepatocellular carcinoma: a systematic review and meta-analysis. Gut Liver. 2024;18(4):695–708. doi:10.5009/gnl230485
8. Zhao LY, Huo RR, Xiang X, et al. Hepatic resection for elderly patients with hepatocellular carcinoma: a systematic review of more than 17,000 patients. Expert rev gastroenterol hepatol. 2018;12(10):1059–1068. doi:10.1080/17474124.2018.1517045
9. Guo H, Wu T, Lu Q, et al. Hepatocellular carcinoma in elderly: clinical characteristics, treatments and outcomes compared with younger adults. PLoS One. 2017;12(9):e0184160. doi:10.1371/journal.pone.0184160
10. Benson AB, D’Angelica MI, Abbott DE, et al. Hepatobiliary cancers, version 2.2021, NCCN clinical practice guidelines in oncology. J Nat Comprehensive Cancer Network. 2021;19(5):541–565. doi:10.6004/jnccn.2021.0022
11. Wen N, Cai Y, Li F, et al. The clinical management of hepatocellular carcinoma worldwide: a concise review and comparison of current guidelines: 2022 update. Biosci Trends. 2022;16(1):20–30. doi:10.5582/bst.2022.01061
12. Amato B, Aprea G, De Rosa D, et al. Laparoscopic hepatectomy for HCC in elderly patients: risks and feasibility. Aging Clin Exp Res. 2017;29(Suppl 1):179–183. doi:10.1007/s40520-016-0675-6
13. Di Sandro S, Danieli M, Ferla F, et al. The current role of laparoscopic resection for HCC: a systematic review of past ten years. Translat Gastroenterol Hepatol. 2018;3:68. doi:10.21037/tgh.2018.08.05
14. Shimada S, Kamiyama T, Orimo T, et al. Prognoses, outcomes, and clinicopathological characteristics of very elderly patients with hepatocellular carcinoma who underwent hepatectomy. World j Surg Oncol. 2020;18(1):122. doi:10.1186/s12957-020-01899-4
15. Hu Y, Cai Y, Ma W, et al. The prognostic nutritional index and tumor pathological characteristics predict the prognosis of elderly patients with early-stage hepatocellular carcinoma after surgery. Biosci Trends. 2023;17(5):369–380. doi:10.5582/bst.2023.01212
16. He Y, Liang T, Mo S, et al. Effect of timing of surgical resection of primary hepatocellular carcinoma on survival outcomes in elderly patients and prediction of clinical models. BMC Gastroenterol. 2021;21(1):230. doi:10.1186/s12876-021-01815-4
17. Yasukawa K, Shimizu A, Kubota K, et al. Impact of liver fibrosis severity on oncological prognosis in hepatocellular carcinoma. Liver Cancer. 2024;13(2):150–160. doi:10.1159/000533857
18. Cui S, Cao S, Chen Q, He Q, Lang R. Preoperative systemic inflammatory response index predicts the prognosis of patients with hepatocellular carcinoma after liver transplantation. Front Immunol. 2023;14:1118053. doi:10.3389/fimmu.2023.1118053
19. Moazzam Z, Alaimo L, Endo Y, et al. A prognostic model to predict survival after recurrence among patients with recurrent hepatocellular carcinoma. Ann Surg. 2024;279(3):471–478. doi:10.1097/sla.0000000000006056
20. Xu L, Xu Y, Li G, Yang B. Perioperative factors related to the prognosis of elderly patients with hepatocellular carcinoma. Eur J Med Res. 2022;27(1):280. doi:10.1186/s40001-022-00896-5
21. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251. doi:10.1016/0895-4356(94)90129-5
22. Faber W, Stockmann M, Schirmer C, et al. Significant impact of patient age on outcome after liver resection for HCC in cirrhosis. Eur J Surg Oncol. 2014;40(2):208–213. doi:10.1016/j.ejso.2013.10.018
23. Harada M, Aramaki O, Midorikawa Y, et al. Impact of patient age on outcome after resection for hepatocellular carcinoma. Biosci Trends. 2021;15(1):33–40. doi:10.5582/bst.2020.03437
24. Hatanaka T, Kakizaki S, Hiraoka A, et al. The prognosis of elderly patients with hepatocellular carcinoma: a multi-center 19-year experience in Japan. Cancer Med. 2023;12(1):345–357. doi:10.1002/cam4.4850
25. Takada Y, Kawashima H, Ohno E, et al. The impact of the age-adjusted Charlson comorbidity index as a prognostic factor for endoscopic papillectomy in ampullary tumors. J Gastroenterol. 2022;57(3):199–207. doi:10.1007/s00535-022-01853-z
26. Koppie TM, Serio AM, Vickers AJ, et al. Age-adjusted Charlson comorbidity score is associated with treatment decisions and clinical outcomes for patients undergoing radical cystectomy for bladder cancer. Cancer. 2008;112(11):2384–2392. doi:10.1002/cncr.23462
27. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
28. Clavien PA, Sanabria JR, Strasberg SM. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery. 1992;111(5):518–526.
29. Levine AB, Schlosser C, Grewal J, Coope R, Jones SJM, Yip S. Rise of the machines: advances in deep learning for cancer diagnosis. Trends Cancer. 2019;5(3):157–169. doi:10.1016/j.trecan.2019.02.002
30. Swanson K, Wu E, Zhang A, Alizadeh AA, Zou J. From patterns to patients: advances in clinical machine learning for cancer diagnosis, prognosis, and treatment. Cell. 2023;186(8):1772–1791. doi:10.1016/j.cell.2023.01.035
31. Shinkawa H, Tanaka S, Takemura S, et al. Predictive value of the age-adjusted charlson comorbidity index for outcomes after hepatic resection of hepatocellular carcinoma. World j Surg. 2020;44(11):3901–3914. doi:10.1007/s00268-020-05686-w
32. Suidan RS, Leitao MM Jr, Zivanovic O, et al. Predictive value of the age-adjusted Charlson Comorbidity index on perioperative complications and survival in patients undergoing primary debulking surgery for advanced epithelial ovarian cancer. Gynecologic Oncol. 2015;138(2):246–251. doi:10.1016/j.ygyno.2015.05.034
33. Liu J, Li J, He J, Zhang H, Liu M, Rong J. The age-adjusted Charlson Comorbidity index predicts post-operative delirium in the elderly following thoracic and abdominal surgery: a prospective observational cohort study. Front Aging Neurosci. 2022;14:979119. doi:10.3389/fnagi.2022.979119
34. Lee S, Kang TW, Song KD, et al. Effect of microvascular invasion risk on early recurrence of hepatocellular carcinoma after surgery and radiofrequency ablation. Ann Surg. 2021;273(3):564–571. doi:10.1097/sla.0000000000003268
35. Wang X, Chai X, Zhang J, Tang R, Chen Q. Nomograms established for predicting microvascular invasion and early recurrence in patients with small hepatocellular carcinoma. BMC Cancer. 2024;24(1):929. doi:10.1186/s12885-024-12655-2
36. Schlichtemeier SM, Pang TC, Williams NE, et al. A pre-operative clinical model to predict microvascular invasion and long-term outcome after resection of hepatocellular cancer: the Australian experience. Eur j Surg Oncol. 2016;42(10):1576–1583. doi:10.1016/j.ejso.2016.05.032
37. Dong Y, Zuo D, Qiu YJ, et al. Preoperative prediction of microvascular invasion (MVI) in hepatocellular carcinoma based on kupffer phase radiomics features of sonazoid contrast-enhanced ultrasound (SCEUS): a prospective study. Clin Hemorheol Microcirc. 2022;81(1):97–107. doi:10.3233/ch-211363
38. Ma X, Wei J, Gu D, et al. Preoperative radiomics nomogram for microvascular invasion prediction in hepatocellular carcinoma using contrast-enhanced CT. Eur Radiol. 2019;29(7):3595–3605. doi:10.1007/s00330-018-5985-y
39. Xu X, Zhang HL, Liu QP, et al. Radiomic analysis of contrast-enhanced CT predicts microvascular invasion and outcome in hepatocellular carcinoma. J Hepatol. 2019;70(6):1133–1144. doi:10.1016/j.jhep.2019.02.023
40. Mo ZY, Chen PY, Lin J, Liao JY. Pre-operative MRI features predict early post-operative recurrence of hepatocellular carcinoma with different degrees of pathological differentiation. Radiol Med. 2023;128(3):261–273. doi:10.1007/s11547-023-01601-0
41. Chen ZX, Schwartz M, Gu LH, et al. Development and validation of safety and efficacy-associated risk calculator for hepatocellular carcinoma in the elderly after resection (SEARCHER): a multi-institutional observational study. Int J Surg. 2022;106:106842. doi:10.1016/j.ijsu.2022.106842
42. Xiang L, Li J, Chen J, et al. Prospective cohort study of laparoscopic and open hepatectomy for hepatocellular carcinoma. Br J Surg. 2016;103(13):1895–1901. doi:10.1002/bjs.10294
43. Wang Q, Li HJ, Dai XM, et al. Laparoscopic versus open liver resection for hepatocellular carcinoma in elderly patients: systematic review and meta-analysis of propensity-score matched studies. Int J Surg. 2022;105:106821. doi:10.1016/j.ijsu.2022.106821
44. Chen K, Pan Y, Maher H, Zhang B, Zheng XY. Laparoscopic hepatectomy for elderly patients: major findings based on a systematic review and meta-analysis. Medicine. 2018;97(30):e11703. doi:10.1097/md.0000000000011703
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
RuleFit-Based Nomogram Using Inflammatory Indicators for Predicting Survival in Nasopharyngeal Carcinoma, a Bi-Center Study
Luo C, Li S, Zhao Q, Ou Q, Huang W, Ruan G, Liang S, Liu L, Zhang Y, Li H
Journal of Inflammation Research 2022, 15:4803-4815
Published Date: 24 August 2022
Prognosis and Personalized Treatment Prediction in Different Mutation-Signature Hepatocellular Carcinoma
Zhang Y, Liu Z, Li J, Li X, Duo M, Weng S, Lv P, Jiang G, Wang C, Li Y, Liu S, Li Z
Journal of Hepatocellular Carcinoma 2023, 10:241-255
Published Date: 15 February 2023
Identification of High-Risk Patients for Postoperative Myocardial Injury After CME Using Machine Learning: A 10-Year Multicenter Retrospective Study
Liu Y, Song C, Tian Z, Shen W
International Journal of General Medicine 2023, 16:1251-1264
Published Date: 7 April 2023
Identification and Validation of Anoikis-Related Signatures for Predicting Prognosis in Lung Adenocarcinoma with Machine Learning
Wang Q, Sun N, Zhang M
International Journal of General Medicine 2023, 16:1833-1844
Published Date: 16 May 2023
The Prognostic Value of the Age-Adjusted Charlson Comorbidity Index Among the Elderly with Breast Cancer
Wang Z, Zhong Y, Zhou Y, Mao F, Zhang X, Wang C, Sun Q
Clinical Interventions in Aging 2023, 18:1163-1174
Published Date: 26 July 2023