")
Back to Journals » International Journal of Nanomedicine » Volume 20
Recent Advances in the Delivery of Bone Morphogenetic Proteins for Targeting Glioma: An Updated Review
Authors Bao H, Chen Y, Zong Y, Jin K , Lan H
Received 18 January 2025
Accepted for publication 24 April 2025
Published 31 May 2025 Volume 2025:20 Pages 7093—7112
DOI https://doi.org/10.2147/IJN.S518340
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Eng San Thian
Huan Bao,1,* Yun Chen,2,* Yonghui Zong,3 Ketao Jin,4 Huanrong Lan5
1Department of Neurosurgery, Jiashan First People’s Hospital, Jiashan First People’s Hospital Luoxing Branch, Jiashan, Zhejiang, 314100, People’s Republic of China; 2Department of Colorectal Surgery, Xinchang People’s Hospital, Affiliated Xinchang Hospital, Wenzhou Medical University, Xinchang, Zhejiang, 312500, People’s Republic of China; 3Center for Clinical Pharmacy, Cancer Center, Department of Pharmacy, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital, Hangzhou Medical College), Hangzhou, Zhejiang, 310014, People’s Republic of China; 4Department of Colorectal and Anal Surgery, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, 310003, People’s Republic of China; 5Department of Surgical Oncology, Hangzhou Cancer Hospital, Hangzhou, Zhejiang, 310002, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ketao Jin, Department of Colorectal and Anal Surgery, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), No. 54, Youdian Road, Hangzhou, Zhejiang, 310003, People’s Republic of China, Email [email protected] Huanrong Lan, Department of Surgical Oncology, Hangzhou Cancer Hospital, No. 34, Yanguan Road, Hangzhou, Zhejiang, 310002, People’s Republic of China, Email [email protected]
Abstract: Bone Morphogenetic Proteins might be the most prospective in glioma treatment because of the facts that they can differentiate glioma cells, inhibit tumor growth and manage glioma stem cells. Its clinical application is hindered by several challenges, including limited permeability across the blood–brain barrier, which impedes effective delivery to the central nervous system; high susceptibility to enzymatic degradation, which compromises stability and therapeutic efficacy; and nonselective binding, which reduces specificity and may result in unintended off-target effects. This review systematically covers the advanced BMP delivery systems such as nanoparticles, smart carriers, gene therapy, and exosome-based system. Hydrogels, scaffolds, and microspheres’ local delivery methods are also discussed as prospective options. The in vitro studies reveal that BMPs are effective and using in vivo glioma models there is also evidence of the effectiveness of BMPs. In addition, new clinical trials reveal concern with safety, tolerability, and therapeutic effects of BMPs, especially their combination with chemotherapy and immunotherapy. BMP specificity and therapeutic performance are further optimized by Personalized medicine and CRISPR/Cas engineering. However, regulatory barriers and product commercialization are challenging issues. This review highlights the need for novel approaches and advanced technologies to address the challenges associated with BMP delivery, aiming to establish BMP-based therapies as an effective treatment strategy for glioma.
Keywords: bone morphogenetic proteins, glioma treatment, blood–brain barrier, nanoparticle-based delivery, gene therapy strategies
Introduction
Gliomas, particularly glioblastomas (GBMs), present significant management challenges due to their high heterogeneity, invasive characteristics, and resistance to treatment.1 Glial tumors encompass various subtypes, including astrocytoma, oligodendroglioma, and ependymoma, classified according to histopathological and molecular characteristics.2 Recent advancements in surgical techniques, radiotherapy, and chemotherapy have resulted in a median survival rate for GBM, the most aggressive variant, of only 15 to 18 months.1 Standard therapy for GBM includes surgical resection, radiation, and the alkylating agent temozolomide (TMZ).3 However, resistance to treatment is common, and recurrence in these patients is nearly inevitable Resistance may arise from mutations in tumor suppressor genes and the overexpression of oncogenes, presenting a significant challenge for effective management.4
The World Health Organization (WHO) classifies gliomas according to their grade (I–IV).5 Lower-grade gliomas (Grades I and II) exhibit slow growth, whereas higher-grade gliomas (Grades III and IV) proliferate rapidly and demonstrate increased malignancy. The most aggressive variant (WHO Grade IV, GBM) is characterized by widespread infiltration of brain tissue, genetic diversity, and significant resistance to treatment.6 For instance, GBM demonstrates heightened amplification of the epidermal growth factor receptor (EGFR) gene, IDH mutations, and loss of heterozygosity on chromosome 10. The methylation status of the O6-methylguanine-DNA methyltransferase (MGMT) gene promoter is a critical factor in predicting response to alkylating agents like TMZ, with methylated tumors showing a more favorable response to treatment.7
Bone Morphogenetic Proteins (BMPs) offer potential for glioma treatment by differentiating glioma cells, inhibiting tumor growth, and regulating glioma stem cells. However, their clinical application is limited by challenges such as poor permeability across the Blood–Brain Barrier (BBB), degradation, and nonselective binding.8 Advanced delivery systems, including nanoparticles, gene therapies, and localized methods like hydrogels and microspheres, aim to enhance BMP targeting and efficacy. Studies confirm the effectiveness of BMPs in preclinical models, and clinical trials are exploring its combinations with chemotherapy and immunotherapy.9 Personalized medicine and CRISPR/Cas technologies are being used to improve BMP delivery, but regulatory and commercialization remains the current challenges. Overcoming these barriers is essential for the successful use of BMPs in glioma treatment.10
Currently, targeted therapies such as EGFR inhibitors have demonstrated limited efficacy, indicating a necessity for additional research to formulate innovative therapeutic strategies. Recent advancements in tumor treating fields (TTF), a non-invasive electrical field therapy, have shown potential in extending survival for GBM patients; however, the treatment remains contentious regarding its standard application.11
This manuscript evaluates the potential of BMPs in glioma treatment, particularly focusing on advancements in delivery systems. The discussion covers the role of BMPs in regulating cancer stem cells, influencing the tumor microenvironment, and interacting with other signaling pathways. The main focus of this review is to highlight the challenges and opportunities in BMP-based therapies, guiding future research toward improving glioma treatment efficacy.
BMPs in Cancer Biology
BMPs, part of the transforming growth factor beta (TGF-β) superfamily, play a crucial role in embryogenesis, bone development, and tissue homeostasis.12 BMP signaling inhibits glioma tumorigenesis by promoting the differentiation of cancer stem cells (CSCs) into non-proliferative astrocyte-like cells. However, certain BMP isoforms may facilitate cancer progression by fostering a microenvironment that supports cancer cell survival and invasion.13 BMP4 has been extensively researched for its anti-tumor effects in glioblastoma and increasing their susceptibility to conventional therapies.14 BMP signaling for glioma treatment is explored through approaches that either use recombinant BMPs or block downstream targets to slow glioma growth.15
The impact of BMPs on the tumor microenvironment and their relationship with these effects must be carefully considered for effective modulation. Ongoing studies aim to optimize BMP signaling to selectively target CSCs while enhancing the efficacy of conventional therapies, such as radiation and chemotherapy, in glioblastoma patients.16 Analysis of BMPs interactions with pathways like Wnt and TGF-β suggests potential applications in gliomas.17
Mechanism of BMP Action in Glioma Regulation
BMPs play significant roles by influencing various complex signaling pathways that regulate cancer cell differentiation, proliferation, and the cancer microenvironment. BMPs interact with heterodimeric receptor complexes composed of type I and type II serine/threonine kinase receptors, which then transmit their signals via intracellular signaling pathways primarily mediated by SMAD proteins. Activated receptor-SMAD complexes translocate to the nucleus to regulate target gene expression, influencing differentiation, apoptosis, and invasion.18
BMPs act as antagonists to pathways like Notch and Wnt, which are crucial for sustaining CSC characteristics. Nonetheless, BMPs play a context-dependent role in gliomas. BMP4 has been shown to reduce the self-renewal capacity of cancer stem cells and their ability to induce tumor recurrence. Conversely, BMP2 and BMP7 may facilitate glioma progression in certain contexts by enhancing glioma cell invasiveness and angiogenesis. Furthermore, BMPs influence immune modulation by regulating macrophage polarization and the recruitment of immune cells to the tumor microenvironment, thereby impacting immune evasion.19 Furthermore, additional oncogenic signaling pathways, including TGF-β, influence BMP signaling via intricate feedback loops, complicating therapeutic targeting significantly (Figure 1).
 |
Figure 1 GBM has several characteristic features that can or do contribute to its virile phenotype and that can also be viewed as the targets for therapy. Some of the features of infiltrating cells, genomic alterations, abnormal angiogenesis, immune escape and reprogramming of the stroma outside the tumor cells are observed in most of these tumors. Adapted from Cruz JVR, Batista C, Afonso B, et al. Obstacles to glioblastoma treatment two decades after temozolomide. Cancers. 2022;14(13):3203. Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).20 |
The regulation of BMP is influenced by the tumor microenvironment. Hypoxia can alter BMP receptor expression and downstream signaling, shifting BMP activity from tumor suppressive to pro-tumorigenic. The dual roles of BMP biology in gliomas underscore the significance of understanding this relationship for therapeutic potential. Current research is investigating the potential of the BMP pathway to enhance tumor suppression while mitigating negative effects, such as increased invasiveness.21
Role of BMPs in Glioma Biology
BMPs roles in glioma biology are very context-dependent, acting as either tumor suppressors or promoters of invasiveness, contingent upon microenvironmental circumstances or related pathways. The therapeutic potential of BMPs is constrained by an insufficient comprehension of their intricate functions.22,23
BMPs as Tumor Suppressors: Inducing Differentiation and Apoptosis
Specifically, BMPS, including BMP-2, BMP-4, and BMP-7, have been identified as tumor suppressors in gliomas that promote the differentiation of cancer stem cells into non-tumorigenic astrocyte-like cells.24 Glioma stem cells (GSCs) are a subset of cells implicated in tumor recurrence and resistance to standard treatments, with their destruction or differentiation recognized as a possible therapeutic objective.25 Certain BMPs inhibit GSC self-renewal by altering the expression of genes associated with cell fate determination and halting their proliferation.22 BMP-4 induces the production of the astrocytic marker gene GFAP (glial fibrillary acidic protein) and inhibits the tumor’s growth potential consequently.26
Furthermore, BMPs can influence apoptosis via both SMAD-dependent and independent mechanisms, as well as differentiation. BMPs can activate pro-apoptotic genes and downregulate anti-apoptotic genes through SMAD-dependent pathways, including as BIM, while simultaneously downregulating BCL-2.27 Besides its pro-apoptotic action, noncanonical BMP signaling is augmented via p38 MAPK and JNK pathways to eradicate cells with carcinogenic potential. Conversely, IDH wildtype glioblastomas exhibit greater resistance to BMP signaling-induced apoptosis, a finding that is less consistent among different molecular subtypes of glioma.28
Furthermore, BMPs inhibit tumor angiogenesis, so restricting nutritional availability to the tumor. It was demonstrated that BMP-4 downregulates VEGF (vascular endothelial growth factor) to inhibit angiogenesis.29 The existence of this anti-angiogenic action is essential, as gliomas are highly vascular tumors, and the suppression of blood supply negatively impacts their development and spread.30
BMP Signaling Pathways in Glioma Cells
The BMP ligands (BMP 2, 4) bind to type I and type II receptors, initiating the BMP signaling cascade in glioma cells.24 SMAD1/5/8 proteins undergo phosphorylation through this interaction and, in conjunction with SMAD4, translocate to the nucleus to modulate the expression of genes involved in differentiation and apoptosis.31 The modulation of BMP signaling effect is influenced by several intracellular variables and crosstalk signaling, complicating therapeutic targeting.32
BMP-2 and BMP-4 in Glioma Inhibition
BMP-2 and BMP-4 possess unique yet synergistic functions in glioma inhibition, both promoting glioma development, apoptosis, and tumor suppression. Significant emphasis has been directed towards BMP-4 due of its ability to markedly impede GSC self-renewal. This promotes astrocytic differentiation by reducing the quantity of remaining cells capable of initiating new repetitions.33 BMP-2 exhibits a greater capacity for inhibiting angiogenesis, making it suitable for targeting highly vascularized gliomas.34
Nonetheless, these defenses are constrained by the inadequate distribution of BMP-2 and BMP-4 to the brain for therapeutic purposes. The restrictive characteristics of the BBB hinder the infiltration of exogenous BMPs into the tumor site, rendering new delivery strategies, such as nanoparticle-based carriers,35 essential. Moreover, BMPs may paradoxically facilitate invasion in some gliomas at elevated delivery levels, underscoring the necessity of regulating and precisely targeting delivery.22
Crosstalk Between BMPs and Oncogenic Pathways
Glioma blood vessels exhibit resistance to BMP inhibition and simultaneously engage in oncogenic signaling pathways. The pathways (Figure 2) are crucial for sustaining the stemness and viability of glioma cells. BMP-4 suppresses Wnt signaling, thereby decreasing β-catenin mediated transcription of genes essential for GSC maintenance.36 Like Notch signaling, BMPs also inhibit Notch signaling, which is recognized for its protective role in CSCs, thereby restricting glioma proliferation.36
 |
Figure 2 Signaling pathway of BMP4 as well as activators and inhibitors of BMP4 cellular signaling. BMP4 may interact with preformed complexes (PFCs), in which, BMPR Type I and Type II receptors are bound at the cell surface and with Type I receptors that form BMP4 induced signaling complexes (BISC) in association with Type II receptors. RGMs, DRAGON, and BAMBI can increase BMP4 dimer binding of Type I receptors in both PFCs and BISCs. Signal recognition leads to the phosphorylation of receptor associated SMADs (Smad1/5/8). Signaling activated SMADs merge with co-SMAD4 to affect the nucleus and in mutants with p300 or stat, they act as transcription initiationers which broaden neural and astroglial genes. BMP-1 as well as sulfated polysaccharides act as extracellular activator while Noggin, Chordin and Gremlin interact with BMP4, thus inhibiting the activity of this signal pathway. Pathway activity can be blocked using intracellular inhibitors SMAD6/7, Smurf1/2 and dorsomorphin. BMP4 may also use SMAD-independently signalling pathways for instance MAPK/p38, JNK, Erk etc Pseudo-receptors like BAMBI can bind to BMP4 dimers, however these pseudo-receptor complexes do not transduce signals due to absence of kinase domains on them. Adapted from Xi G, Best B, Mania-Farnell B, James CD, Tomita T. Therapeutic potential for bone morphogenetic protein 4 in human malignant glioma. Neoplasia. 2017;19(4):261–270. Creative Commons license (https://creativecommons.org/licenses/by-nc-nd/4.0/).37 |
Second, direct antagonism and myRNA expression caused by BMPs promote proliferation of glioma. Specifically, BMP-2 downregulates the oncomiR, miR-21 associated with glioblastoma invasive and therapy resistance. BMPs regulatory effects widen their therapeutic potential and are promising agents in glioma treatment.22,38 Nevertheless, the introduction of many feedback loops makes the therapeutic landscape difficult. Both BMPs and TGF-β can coopt tumor promoting signals providing resistance to therapeutic intervention. It has been demonstrated that tumors exploit components in the SMAD signaling pathway which share components with BMPs and TGF-β, leading to Bmp and TGFb Immunotherapy to address the dependence of tumors on this pathway for survival and metastasis.39 Furthermore, BMPs act as both tumor suppressors and possible invasion enhancers, and a detailed understanding is crucial before application of any therapeutic.40
BMPs and Glioma Stem Cells: Differentiation Therapy
Glioma stem cells (GSCs) impede effective glioma treatment due to their ability to promote tumor recurrence and high resistance to conventional therapies, such as radiotherapy and chemotherapy, owing to their stemness. One current approach is to differentiate GSCs into non-tumorigenic, differentiated cells, rather than target malignant cells. BMPs are known to be major regulators of GSC differentiation (Figure 3) and although not conclusively proven, BMP2, BMP4, and BMP7, are a promising approach to reduce tumor malignancy.34 GSC differentiation by BMPs into cell types resembling astrocytes or neurons mitigates their tumorigenic characteristics. GFAP (glial fibrillary acidic protein) can be activated by BMP-4 and decrease GSC proliferation and block GSCs forming neurospheres.41 Associated to gene differentiation is the loss of expression of stemness transcription factors including SOX2 and OLIG2 which are required for the maintenance of GSC identity.42
 |
Figure 3 BMP Signalling Pathways in Glioma Cells. |
The SMAD dependent signaling pathways regulate the impact of BMPs in differentiation therapy. BMPs bind to their receptors on the surface of GSCs leading to activation of SMAD1/5/8 proteins which form complexes with SMAD4, translocate nuclear and recruit DNA and RNA polymerases.43,44 ID1 (inhibitor of differentiation 1) is regulated by them during differentiation, when it inhibits cell cycle and contributes to lineage-specific development.45,46 Furthermore, BMPs activate non-canonical signaling pathways including p38 MAPK and PI3K/AKT pathways which help improve differentiation and decrease cell survival under stress conditions.24,44
This therapeutic approach has the potential to enhance glioma sensitivity to standard treatments by exploiting BMP-induced differentiation therapy. More specifically, differentiated cells are less sensitive to chemotherapy and radiotherapy than their undifferentiated, stem-like counterparts.15 Previous studies show that preculating glioma cells with BMP4 sensitizes these cells to the first-line chemotherapy for glioblastoma, TMZ, by inhibiting MGMT (O6 methylguanine DNA methyltransferase).47 This combinatorial strategy improves therapeutic outcome and minimizes the chance of tumor relapse.
Although there have been some small developments, most of them have been impeded by various challenges in the use of BMP-based differentiation treatment.48 In some gliomas, resistance BMP signaling is also associated with Smad4 mutations or overactivation of Wnt/β-catenin pathways that maintain stem cell characteristics in the presence of BMPs.49,50
While BMP-induced differentiation holds promise, its effects may not be permanent due to the plasticity of differentiated cells, which can revert to a stem-like state under certain conditions. As such, the long-term efficacy of differentiation therapy requires further investigation. Research is focusing on identifying effective combination therapies that maintain a differentiated state of GSCs while enhancing therapeutic efficacy. A promising approach is the combined inhibition of BMP signaling with oncogenic pathways such as Notch and TGF-β. Blocking BMP signaling can prevent GSCs from reverting to a stem-like state, while inhibiting Notch and TGF-β, which are involved in maintaining GSCs’ stemness and survival, further diminishes the tumor’s regenerative potential. Additionally, combining BMPs with molecular compounds or chemotherapeutic agents may offer a synergistic effect, improving treatment outcomes by promoting differentiation and enhancing the response to radiation and chemotherapy.17
Despite the promising therapeutic potential of BMPs in glioma, their clinical application is hindered by challenges in delivery and stability. The following section examines these challenges, specifically the short half-life, rapid degradation, limited blood–brain barrier penetration, non-specific distribution, off-target effects, and immune response to exogenous BMPs.
Challenges in Delivering BMPs to Glioma
Short Half-Life and Rapid Degradation of BMPs
BMPs are a promising approach to treating glioma but have a short half-life, which substantially limits their use. A significant presence of matrix metalloproteinases in the tumor microenvironment contributes to the rapid degradation of BMPs, limiting their therapeutic efficacy. Moreover, upon systemic circulation, BMPs can be drawn from their reservoirs, reducing their availability at sites of inflammation and hindering their capacity to exert therapeutic effects until they are released. This rapid degradation requires high or frequent dosing to maintain therapeutic levels and prevent unwanted side effects such as ectopic bone formation, inflammation, and immune responses. In certain conditions, BMPs might promote tumor growth, particularly in environments where they can activate pro-tumorigenic pathways. For example, BMPs can stimulate cancer cell survival and invasion by enhancing the expression of genes involved in cellular migration and epithelial–mesenchymal transition (EMT). Additionally, BMPs may contribute to tumor progression by inducing angiogenesis or immune suppression in the tumor microenvironment. The effect of BMPs is highly context-dependent and varies across different microenvironments, where they can either suppress tumor growth by inducing differentiation and apoptosis or, conversely, drive tumor progression by activating pathways that promote cell proliferation, invasion, and immune evasion.51,52
Given the dual roles BMPs can play in tumor progression or suppression, addressing their delivery challenges is crucial for optimizing their therapeutic potential. To overcome these problems, researchers have developed advanced drug delivery systems, such as encapsulating BMPs inside biodegradable hydrogels, polymeric microspheres, or nanoparticles.53,54 These carriers release the BMPs at the target site with sustained release enabling elimination of repeated dosing. It has been demonstrated that the BMP is released in a gradual manner, protected from enzymatic degradation within internal hydrogels such as alginate and chitosan.55 To increase BMP stability and facilitate localized delivery to glioma cells, polymer-based carriers such as poly (lactic-co-glycolic acid) (PLGA) nanoparticles have been studied.55,56 The stabilization of engineered BMP analogs or fusion proteins represents a promising strategy. These issues inhibit the retention and degradation of BMPs. More recently, studies indicate that BMPs conjugated to heparin-based carriers increased half life and provided protection from enzymatic degradation and are more efficacious for glioma treatment.57,58
Limited Blood–Brain Barrier (BBB) Penetration
A major barrier to the delivery of therapeutic agents, such as bone morphogenetic proteins, to gliomas is the blood–brain barrier. Factors such as size, charge and hydrophilicity of proteins limit their transport across the BBB, thus requiring other strategies.48,55 Systemic delivery methods do not achieve therapeutic concentrations of BMPs within the brain, limiting the efficacy of BMPs in the treatment of gliomas.15,37
A delivery strategy currently being formulated to alleviate these limitations is innovative. The first strategy is to encapsulate BMPs within nanoparticles that can cross the blood–brain barrier. Receptor-mediated transport across blood–brain barrier is achieved by ligand-functionalized liposomes and polymeric nanoparticles. Nanoparticles covered by peptides targeting low-density lipoprotein receptors (LDLr) enable brain uptake of BMPs.59 Additionally, gold nanoparticles functionalized with cell-penetrating peptides can deliver therapeutic proteins across the blood–brain barrier and to glioma tissues.60,61 Ultrasound combined with microbubbles is an innovative approach that can transiently disrupt the BBB.62 Delivery of BMPs, into the brain parenchyma was improved using this technique. Localized, non-invasive delivery is a key feature of focused ultrasound (FUS), though it poses risks of tissue damage and inflammation.63,64 Therefore, their safety and efficacy for clinical application need to be optimized.
In addition, there has been strong interest in localized delivery methods including intracranial injection and implantation of BMP loaded scaffolds. Due to the fact that BMPs are administered at the tumor site with these methods, they act as an alternate to the blood–brain barrier.65 However, surgery, infection and potential damage to tissues introduced with these invasive techniques pose a risk. Existing challenges with local delivery of BMP do not preclude local delivery as a viable glioma treatment option based on advancements in scaffold design with biocompatible polymers.55
Non-Specific Distribution and Off-Target Effects
The main restriction on the application of BMPs in glioma therapy is their nonselective dispersion in the whole body. The systemic delivery of BMPs can induce excess BMPs accumulation in non-targeted tissues (ectopic bone formation or inflammation in healthy tissues), and systemic delivery can result in selective BMP delivery to targeted sites.66 There are significant challenges in cancer therapeutics, where precise targeting is needed, and normal physiological functions disrupted should be minimized, but specificity is absent. In addition, the leakage of BMPs into healthy brain regions disrupts normal differentiation of the neural cell process and can become neurotoxic.67
To overcome these issues, methods for targeted delivery have been developed. In vivo, BMP delivery becomes more specific with nanoparticles functionalized with tumor homing peptides or antibodies. While selective ligand nanoparticles toward glioma-specific receptors, such as integrins or epidermal growth factor receptor (EGFR), have shown modest improvements in preclinical models, selectivity for glioma has not been achieved yet.68,69 Through the guided accumulation of magnetic nanoparticles under an external magnetic field, the accumulation of BMPs in tumor tissues was shown to be effective.55,70 Additional innovation in the delivery of BMPs limits off target effects and increases the therapeutic potential of BMPs.37,71
Immune Response to Exogenous BMPs
Another challenge in the practical therapeutic application of exogenous BMPs is the immune response they elicit. In the absence of these proteins within the tumor microenvironment, immunity is notably activated, particularly following systemic administration. Abnormalities in the anti-BMP immunities which put forward the scenario where immune system recognizes BMPs as antigens and this creates an immune response including generation of the inhibitory antibodies and pro-inflammatory signals which causes the ineffectiveness of BMPs.72,73 Exacerbating tumor associated inflammation may further complicate glioma treatment.74
There are several ways researchers can overcome immune-related challenges. The stealth nanoparticles of interest are those coated with polyethylene glycol (PEG), which have been used to encapsulate BMPs. TEGylation (or protein masking via PEGylation) of protein prolongs its circulation time and increases its bioavailability.75 Further, engineering BMP analogs with reduced immunogenicity, or fusing BMPs with immunosuppressive molecules, may further reduce immunogenicity while retaining the ability to mediate therapeutic efficacy.55,76 Localization of delivery is explored by preclinical studies in various forms, such as intracranial implants, in order to minimize systemic exposure and reduce the likelihood of an immune reaction.77
Strategies for BMP Delivery Across the Blood–Brain Barrier
Regulation of BBB permeability is highly restricted and influenced by various tissue characteristics, making the systemic delivery of therapeutic molecules particularly challenging.78,79 To address this issue, the objective is to explore advanced nanoparticle-based strategies, where BMPs can be encapsulated within nanoparticles. This encapsulation not only protects BMPs from degradation but also facilitates their passive or active transport across the BBB, thereby enhancing their therapeutic efficacy.55
Nanoparticle-Based Delivery Systems
Due to the capacity of nanoparticles to penetrate through the blood–brain barrier and deliver to the gliomas, its use in systemic delivery of therapeutic medication has gained popularity. Lipid nanoparticles (LNPs) are an efficient delivery system with benign biocompatibility and the ability to cross biological membranes.80 In these particles, BMPs are centered in a lipid bilayer to protect them from enzymatic breakdown and immune clearance. Lipid nanoparticles can be functionalized with specific ligands or peptides to facilitate transcytosis through the BBB mediated by receptor processes.81 Receptor interactions of LNPs with brain endothelial cells enhance the transport of LNPs with transferrin or apolipoprotein ligands.82 Endosomal escape of completed LNPs containing BMPs allows them to reach their target cells in glioma, where they are essential, facilitating BMP delivery. Lipid nanoparticles associated with polyethylene glycol (PEG) stabilizers suppress immune clearance and increase the concentration of BMPs at the tumor site resulting in enhanced circulation time. As demonstrated by liposome application in approved mRNA vaccines, lipid-based nanoparticles also hold great promise for clinical translation.83
Advantages of polymeric nanoparticles include adjustable size; customizable surface properties; and ability to facilitate sustained release of BMPs over an extended period. They are biodegradable polymers-based nanoparticles such as poly (lactic-co-glycolic acid) or chitosan, releasing their cargo during degradation progressively.84 To optimize efficacy, BMPs are administered by sustained release, which both deliver therapeutic concentrations at the tumor site and minimize systemic exposure. Ligands, for example folic acid or antibodies targeting glioma markers, can be surface modified with polymeric nanoparticles to allow selective uptake by tumor cells.85 We design polymeric nanoparticles which can selectively release BMPs within the tumor microenvironment in response to specific environmental stimuli, such as pH or enzymatic activity. Dual drug-BMP delivery systems in the form of polymeric nanoparticles are used to deliver chemotherapeutic agents and BMP to inhibit glioma growth.86 Finally, these systems can successfully traverse the blood–brain barrier and concentrate within the glioma tissue; thus, they hold great promise for future clinical applications.87
The use of inorganic nanoparticles, including gold nanoparticles, silica nanoparticles, and magnetic nanoparticles, for BMP delivery is gaining significant attention. These systems can respond to external stimuli, including electromagnetic fields, and generate imaging signals, making them suitable for theranostic applications. They hold promise not only for targeted therapy but also for monitoring treatment efficacy in real-time.88 Gold nanoparticles with adjustable size and surface characteristics may diffuse or be taken up by their surface by receptor mediated uptake in active transport across the blood–brain barrier.61 Through photoacoustic techniques, this conjugation enables delivery of therapeutic proteins to gliomas.64 The high surface area of silica nanoparticles for BMP loading are functionalized for increased targeting efficiency. Remote control movement of magnetic nanoparticles, especially those of iron oxide, can be performed by external magnetic field. These BMPs can be incorporated into nanoparticles and delivered across the BBB to reach glioma locations, to bypass off target effects.37
Carrier-Mediated Transport Techniques
Carrier-mediated transport techniques utilize biological carriers to enhance BMP delivery across the blood–brain barrier, aiming to improve the specificity and efficacy of glioma treatment.89
Transferrin-Modified Delivery Systems
Iron transport in the bloodstream is primarily facilitated by transferrin, a glycoprotein known for its role in transporting therapeutic agents across the BBB. However, the selectivity of the BBB poses a challenge for transporting large molecules such as BMPs. The transferrin receptor (TfR), which transferrin uses to bind, is abundantly expressed on the endothelial cells of the BBB, making it a potential target for enhancing the delivery of therapeutic agents.90,91
There are now numerous data which show that the transport efficiency of BMPs can be greatly enhanced through modifications of BMP delivery systems with transferrin.68 BMPs loaded into transferrin-coated nanoparticles exhibit enhanced cellular uptake in glioma cells that enhances anti-tumor efficacy. For example, it has been shown that delivery and retention of BMP-2 linked to transferrin modified liposomes is superior compared to free BMP-2 and reduces tumor size in preclinical models to an impressive extent.92
In addition, these systems possess dual role of delivering both BMPs and chemotherapeutic agents, which may work in synergistic fashion to overcome treatment resistance in typically chemoresistant gliomas.4,93 With targeted delivery, this approach not only improves the efficacy of BMPs, but reduces side effects due to the systemic exposure minimizing with traditional chemotherapeutics. In addition, transferrin carriers maintain high versatility, allowing for the cosmetic special of different BMPs as well as therapeutic agents into the same delivery platform.94
However, stability and release kinetics issues continue for transferrin modified systems. Implicit to achieving optimal therapeutic outcomes is ensuring the sustained release of BMPs while maintaining their bioactivity.95 There is ongoing research to refine the formulation and mechanism of targeting of transferrin modified delivery systems to further improve the performance of these systems in glioma therapy.61,78
Peptide-Based BBB Targeting
Therefore, peptide-based strategies have become a new approach to augment delivery of BMPs across BBB. Specific peptides able to bind receptors on the BBB are used for these techniques that utilize transcytosis of the BMPs. For example, T7 peptides which have shown potential to increase permeability of therapeutic agents across the BBB by modulating receptor mediated endocytosis.96
We have shown that T7 peptide-modified nanoparticles incorporating BMPs can effectively take up in glioma cells and substantially augment anti-tumor activity. BMPs are thus allowed to “target” their intended site of action by the peptide’s ability to target specific receptors of the BBB. Zhu et al (2023) research indicated that T7 modified BMP delivery systems induced significant glioma cell proliferation suppression in vitro, indicating the possibility of T7 modified BMP delivery systems for targeted glioma therapy.97
The use of RGD (arginine-glycine-aspartic acid) peptides represents another promising approach, since RGD peptides are known to selectively bind the integrins overexpressed in glioma cells. Researchers have enhanced the specificity and efficiency of BMP delivery by conjugating BMPs to RGD peptides or RGD modified nanoparticles. Recent work has indicated that RGD targeted BMP formulations have shown highly enhanced internalization in glioma cells in comparison with non-targeted counterparts resulting in higher therapeutic effects.98
Peptide-based strategies hold exciting promise for BMP delivery, however, peptide-based strategies present challenges regarding peptide stability, specificity, and the possibility of immunogenicity. However, research is ongoing to develop peptide design and delivery systems that will safely deliver BMPs to gliomas without triggering harmful immune responses.99
Local Delivery Systems for BMPs in Glioma Treatment
BMPs delivery, either in local or systemic delivery systems, has emerged as an innovative and potentially more effective approach for their therapeutic use in glioma treatment.100 Sustained, localized release of these systems is possible with minimal systemic side effects and maintains the highest BMP concentrate in the tumor site.55 Local delivery strategies that are promising include injectable hydrogels and implantable scaffolds (Figure 4).
 |
Figure 4 Local Delivery Systems for Bone Morphogenetic Proteins in Glioma Treatment. |
Injectable Hydrogels for BMP Delivery
Injectable hydrogels constitute a versatile nanomedicinal platform for local delivery of BMPs owing to their inherent biocompatibility, tunable mechanical strength, and its capability for in situ formation. The system can encapsulate BMPs and release them in a sustained manner, delivering dose levels over time at the tumor site.101 The advantage of this approach is that it requires fewer repeated injections, as well as improving patient compliance.
Materials for hydrogels can be engineered from natural polymers (alginate, chitosan) and synthetic polymers (polyethylene glycol). Studies have also demonstrated that alginate-based hydrogels can be used to achieve sustained release over several weeks of encapsulated BMP-2. In addition, this sustained release helps prolong cell differentiation and improves the therapeutic effect on glioma cells.54 In addition to their ability to promote cell infiltration and integration within the surrounding tissue, injectable hydrogels also improve their efficacy. More recently, hydrogel formulations have included incorporation of bioactive molecules or growth factors with BMPs, that while synergistic for tissue regeneration, also inhibit glioma growth.102 Moreover, the employment of stimuli responsive hydrogels that liberate BMPs in response to environmental stimuli (pH, temperature) is suggested to provide BMP delivery on them, in an allegedly controlled fashion for the tumor microenvironment.103 However, challenges in optimizing hydrogel composition for BMP stability and activity despite their advantages remain. Development of hybrid hydrogels with the potential of combining the complementary properties of various polymer types as well as improving the retention and release profile of BMP is suggested as future research.
Implantable Scaffolds for Sustained Release
Another effective local delivery system of BMPs for glioma treatment is implantable scaffolds. Typically designed to deliver structural support while allowing for sustained BMPs release, these scaffolds are. In contrast to injectable systems, BMPs can be directly implanted into the tumor by surgical means rendering the supply of these factors local and continuous. Natural (collagen, gelatin) and synthetic (polylactic acid, polyglycolic acid) polymers are scaffold materials that can be grouped into. For example, collagen-based scaffolds have been promising to encourage cell adhesion and proliferation as well as suitable environment for BMP action.104 These unique features indicate that BMP-loaded scaffolds could be used to achieve combination therapy.105
In addition, the design of scaffolds can be modified to optimize controlled release kinetics, permitting the sustained delivery of BMPs over an extended period. It has been found that by embedding BMPs into a porous scaffold, local BMP concentrations can be gradually released towards tumor resection.106 Further, the inclusion of additional therapeutic agents between and within the scaffold matrix allows a multi-fold therapeutic approach encompassing both tumor growth and the surrounding microenvironment.107
However, the challenges around implantable scaffolds are foreign body reactions and the requirement for implantation. To account for these concerns, biocompatible and biodegradable materials are used, to prevent complications from occurring as the scaffolds degrade over time.108 Being a therapeutic application of Glioma, scaled investigations are being carried out on how to refine the scaffold design to optimize the delivery of BMP as a therapy to increase the outcomes of treatment.
Microspheres and Nanofibers for Localized BMP Delivery
BMPs in the treatment of glioma lend themselves to local delivery using microspheres and nanofibers. These systems deliver precise control over the release kinetics: sustained delivery with reduced risk of exposure to the systemic circulation. The microspheres are spherical particles composed of biodegradable polymers, for example poly (lactic-co-glycolic acid) (PLGA) that dissolve in time to release encapsulated BMPs.86,109 Unlike the polymer fibers, nanofibers are polymer fibers based with a high surface area for BMP adsorption and delivery for interaction in the tumor microenvironment. Particularly favorable are microspheres for having the capacity to enwrap BMPs without negatively affecting their bioactivity. The gradual and sustained BMP release from the polymer matrix facilitated a slow degradation of the polymer matrix that is the prerequisite for maintaining a gradual BMP release and promoting the differentiation of glioma cells and suppression of tumor growth.110
These systems can also be given locally, circumventing the BBB and lowering off target effects. In addition, some formulations contain dual-release systems in which BMPs are used in combination with chemotherapeutics to suppress tumors synergistically.111 An alternative platform based on nanofibers offers unique mechanical and biological properties. These materials can be functionalized with BMPs and other growth factors to electrospun nanofibers, which facilitate improved therapeutic results. BMP loaded nanofibers have been shown to differentiate glioma stem cells, while at the same time inhibiting proliferation.112 Nanofibers have tunable degradation rates and high porosity, making them good candidates for long-term implantation with subsequent continuous BMP release. However, microspheres and nanofibers have their challenges, including being susceptible to an immune reaction and not having a precise way to precisely control release. Biocompatibility of platinized nanoparticles and fine tuning the degradation rates to match the therapeutic requirements for glioma treatment aims at improving the effectiveness of therapy.113
Intratumoral Injection of BMPs: Limitations and Benefits
Direct method of BMPs delivery to glioma tissues is intratumoral injection, which delivers localized treatment, that avoids systemic circulation. This technique enables delivery of high concentrations of BMPs to benefit the tumor site. Gliomas resistant to conventional therapy can be particularly well treated with intratumoral injection for the direct modulation of tumor cell behavior through BMP-induced differentiation and apoptosis. The circumvention of the barrier posed by the BBB is one of the main advantages of intratumoral injection. This approach avoids the need for carriers or modifications permitting BBB penetration by delivering BMPs directly to the tumor. BMP-2 and BMP-4 have been shown to decrease glioma proliferation and induce differentiation of malignant to non-malignant cancerous phenotypes.37,114
In addition to reducing the systemic toxicity with high BMP doses, this localized delivery also reduces BMP dose to the patient. Nevertheless, there are some limitations regarding intratumoral injection. Short half lives coupled with rapid degradation of BMPs in the extra cellular environment require repeated injections to achieve and maintain desired levels of BMP. Furthermore, this invasive nature may be of patient safety concern since it may possibly lead to tumor dissemination during such a procedure.115 The stability and activity of BMPs in the tumor microenvironment is being improved using strategies including administering stabilizing agents or encapsulating the BMPs in protective matrices.
Emerging Advances in BMP Delivery Technologies
Smart Nanocarriers for Stimuli-Responsive Release
Delivery of BMPs has been revolutionized by smart nanocarriers with stimuli responsive, precise and controlled release. These systems are triggered by environmental stimulus, including pH, temperature, or oxidative stress, within the tumor microenvironment. To illustrate, gliomas develop an acidic microenvironment that may inadvertently facilitate the release of encapsulated BMPs from pH sensitive micelles or hydrogels, thereby minimizing premature release and enhancing targeting efficiency.99 In addition, it is possible to design thermosensitive lipid nanoparticles to disassemble at body temperature thereby increasing BMP release around the glioma site. This localized delivery is further ensured by the fact that enzyme-sensitive systems release their cargo when they interact with the specific proteases overexpressed in gliomas, including matrix metalloproteinases (MMPs).116 Synchronizing BMPs release with biological environment, these smart nanocarriers bolster the therapeutic potential and minimize off-target effects of BMPs. Nevertheless, there are still challenges in scaling up production and stability of these nanocarriers in blood circulation.60
Gene Therapy Approaches for BMP Expression in Glioma
Suppression of miR200 Fusion and direct delivery of BMP coding sequences into tumor cells represent promising gene therapy strategies for sustained BMP expression in glioma tissues.117 As an alternative to this approach, the short half life and rapid degradation of BMP proteins in circulation is bypassed. This purpose is usually conducted using viral vectors, such as adenoviruses or lentiviruses, which enable BMPs continuous production in glioma cells.118 There exists a great deal of difficulty in inducing immune responses by viral vectors, and research has focused on non-viral alternatives, namely lipid nanoparticles and polymeric carriers.
BMP-2 and BMP-7 gene delivery has recently been shown in glioma stem cells to cause differentiation, which decreases this tumorigenic potential.119 Furthermore, additional effects have been found using BMP gene therapy in conjunction with chemotherapeutic agents and together, they have synergistically inhibited tumor growth. Promising however, clinical translation of BMP gene therapy is hindered by the need for precise control of transgene expression and minimization of off target effects.120
Exosome-Mediated Delivery of BMPs to Glioma Cells
Naturally occurring extracellular vesicles, exosomes, have been shown to be effective delivery vehicles for BMPs due to their ability to cross the BBB and to deliver to glioma cells with minimal immunogenicity. To manifest specificity for glioma tissues, these vesicles can be loaded with BMP proteins or BMP-encoding RNA sequences and modified with targeting ligands. Exosome-based delivery systems have many advantages: low toxicity, ability to deliver to many different cell types, and ability to be repeatedly dosed without a strong immune response.121
Based on these preclinical models, exosome-mediated BMP delivery at therapeutic concentrations seems promising in promoting glioma cell differentiation, differentiation, reduction of stemness, and ensuing reduction in tumor growth.122 Despite these challenges, the yield of exosomes remains low and there is variability in targeting efficiency; this approach cannot be clinically adopted.
CRISPR/Cas-Based BMP Engineering for Enhanced Efficacy
CRISPR/Cas forms the genetic engineering hammer of precision, virtually rewiring gene expression. To control BMP expression at the genomic level within glioma therapy, researchers are looking into regulating BMP expression as a function of the CRISPR/Cas system either by inserting BMP coding sequences into tumor cells or upregulating BMP receptors. In combination, this strategy can increase glioma sensitivity to endogenous and exogenous BMPs, thus improving therapeutic outcome.123
Additionally, BMP signaling in glioma cells is being investigated via CRISPRa systems to activate the system and drive differentiation and apoptosis of the cells. However, due to the BBB, it is a great challenge to deliver CRISPR components across the BBB, and one would have to use advanced vehicles such as lipid nanoparticles or viral vectors. Furthermore, the risk of off target gene editing must be minimized to achieve the safety and efficacy of this.124
Preclinical and Clinical Studies on BMP Delivery in Glioma
Key Findings from Preclinical Studies
Innovative strategies for overcoming the delivery challenges in the brain microenvironment for BMP delivery in glioma have been investigated in preclinical studies. Insights into how BMPs can modulate tumor behavior, induce differentiation in cancer stem cells, limit tumor progression are derived from both in vivo animal models and in vitro glioma cell lines.19,22 These studies also point to the development of advanced delivery technology (nanoparticles or hydrogel) to maintain BMP stability, decrease degradation, and improve therapeutic outcome. Promising results in in vivo studies (rodent glioblastoma models, eg, murine orthotopic models) have been reported. When encapsulated in polymeric nanoparticles or delivered through hydrogel scaffolds, BMPs such as BMP-2, BMP-4 and BMP-7 both reduced tumor volume and improved survival outcomes.55,125 In a mouse model study using BMP-4 loaded chitosan nanoparticles, survival rates were greatly increased, and glioma cell differentiation was enhanced. In addition, researchers have investigated methods of local delivery (intracranial injections) that would bypass the BBB to maintain sufficiently high BMP concentrations at the tumor site.20,48
The advantage of the sustained-release formulations is the ability to have BMP bioactivity over sustained periods of time, which is important in glioma therapy reasoning the aggressive nature of the disease. Current challenges include immune reactions to exogenous BMPs, and variable tumor response. BMPs promote glioma stem cell differentiation in vitro to a nonproliferative state which degrades tumor aggressiveness in glioma cell lines (U87, U251).99,126 BMP2 and BMP7 studies show that these molecules inhibit glioma stem cell-like cell self renewal, which improves the chemotherapy and radiation treatment. BMPs have also been shown in combination with other therapeutic agents to work in synergy with effect on apoptosis and reduce the migratory potential of cancer cells.74 Also, crosstalk between BMP pathways and key oncogenic signaling cascades, such as PI3K/AKT and Wnt, was observed during the in vitro studies.19 These interactions also convey a glioma cell network that is intricately regulated and hints at the possibility of combination therapies targeting multiple pathways.
Clinical Trials and BMP-Based Glioma Therapies
Early phase clinical trials have been initiated to evaluate the safety, tolerability, and potential therapeutic application of BMPs in glioma patients with the clinical translation of BMP-based therapies still in its infancy. The aim of these trials is to determine optimal dosing strategy and safety profile as well as optimal delivery routes. BMPs have been first used to test their safety in glioma patients, and this has shown them to be feasible using localized delivery methods where systemic exposure is limited and off target effects are reduced. Immune responses to BMP-loaded nanoparticles and scaffolds used in these trials are minimal, with the only adverse effects slow resolution of inflammation around the injection site.127
Differentiated localized BMP delivery has been achieved via intracranial delivery using either catheters or injectable hydrogels to bypass BBB and reduce systemic toxicity.128 Additionally, these approaches greatly facilitate the precise dosing of BMPs directly at the tumor site minimizing potential off target effects. Preliminary trials show that BMP-based therapies can improve overall response and quality of life for patients with recurrent glioblastomas. BMP loaded nanoparticles have been shown in some, albeit limited, clinical studies to provide longer progression-free survival and reduced rates of tumor recurrence than standard therapies alone. Moreover, BMPs have been used in combination with conventional treatments, such as temozolomide chemotherapy and radiotherapy, to improve therapeutic outcomes, presumably through BMP consequent glioma stem cell differentiation.129
Nevertheless, these findings should be confirmed in larger, randomized clinical trials before these BMP-based therapies become routine clinical practice. Likewise, the variability in the individual responses to BMP treatment underscores the need for personalized treatment approaches that deliver BMP strategies that target these same tumor characteristics on a patient-specific basis. Table 1 shows the latest research about the BMPs Affecting Gliomas. It summarizes important empirical data, delivery strategies, potential direct therapeutic applications, and citations of studies reviewing the use of BMPs in glioma management.
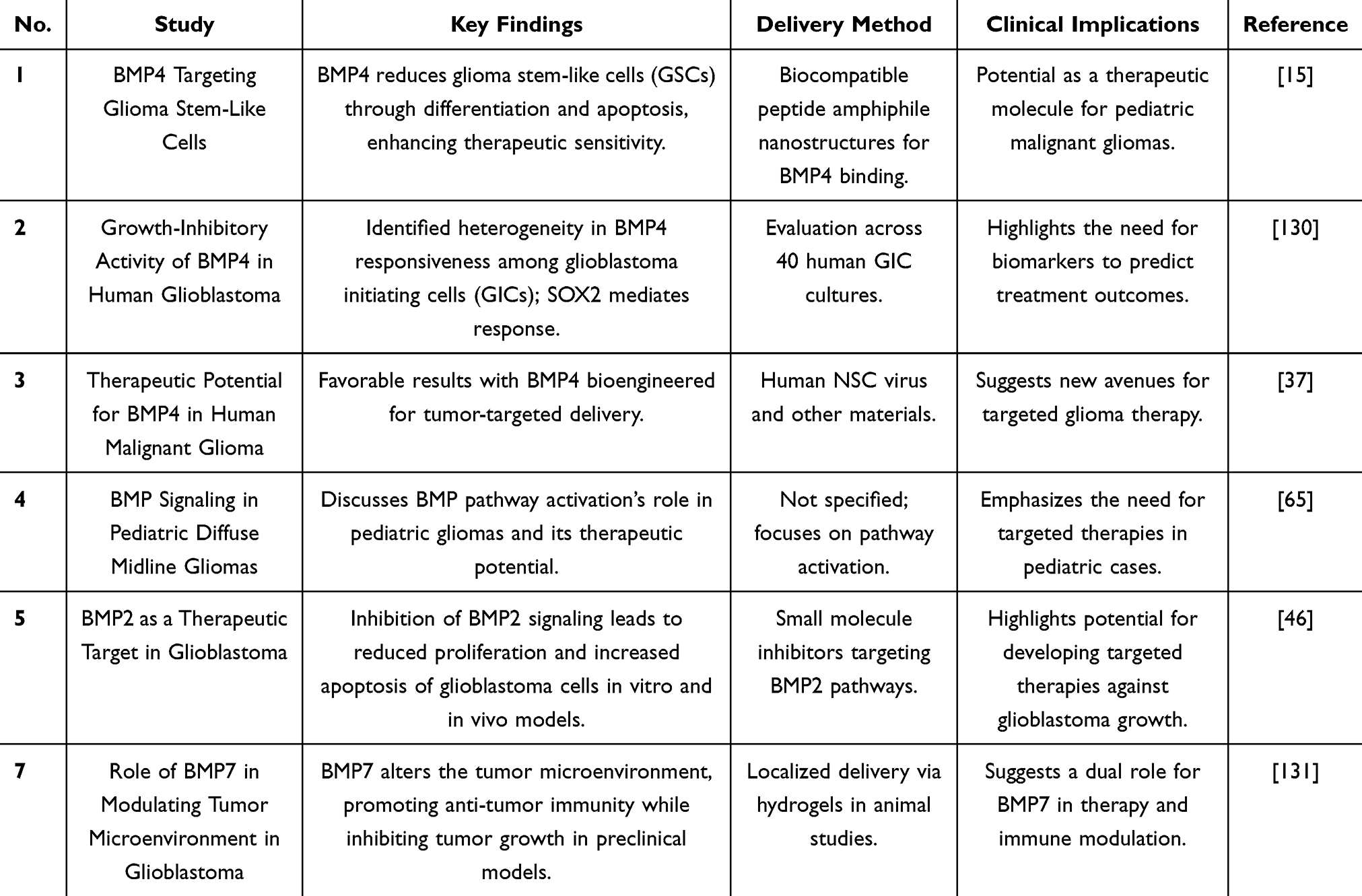 |
Table 1 Overview of the Latest Research About the BMPs Affecting Gliomas. It Summarizes Important Empirical Data, Delivery Strategies, Potential Direct Therapeutic Applications, and Citations of Studies Reviewing the Use of BMPs in Glioma Management |
Challenges and Future Prospects
BMPs delivery to glioma is an enormous challenge, which is due mainly to the BBB, that impedes the transportation of therapeutics into the brain. Nevertheless, nanotechnology driven solutions, such as lipid, polymeric and inorganic nanoparticles, that have demonstrated their ability to enhance BMP delivery by stabilizing the proteins, encapsulating proteins, and controlled delivery.132 Additional precision in delivery is provided by stimuli-responsive carriers which are activated upon exposure to environmental changes (pH, temperature). Hybrid platforms featuring nanoparticles with surface modifications (PEGylation) also enhance penetration of the BMP, while minimizing immune recognition.55
New synergies can be formed by combining BMPs with standard chemotherapeutic agents such as temozolomide (TMZ). BMPs direct glioma cells to differentiate, leading to a drop in the invincible cancer stem cell pool for recurrence and resistance.65 The combination of BMPs with these modalities improved survival and slowed tumor progression compared to any of the modalities alone in murine glioma models, according to preclinical data.133
Personalized medicine, with molecular profile tailored treatments, however, represents a major advantage given the heterogeneity of gliomas. RNA sequencing and tumor-specific biomarker identification can be used to choose the most efficient BMP-based treatment per patient. In addition, the CRISPR/Cas9-based engineering of BMPs provides enhanced selectivity in which BMP signaling pathways that are relevant to each tumor are precisely targeted.134 As this approach protects against off target effects and optimizes therapeutic outcome, it is preferred to earlier design approaches.
To use exogenous proteins such as BMPs, and indeed to use gene-editing technologies, has regulatory and ethical challenges. Comprehensive safety assessments are a requirement of regulatory bodies such as the FDA of new delivery platforms and new therapeutic combinations. Gene-edited cells, genetically modified BMP constructs and their applications pose ethical issues too including transparency in protocols for patient consent and clinical trial design. In addition, GMP compliant scalable production processes will be necessary for the development and safety and availability of these therapies.135
BMPs have demonstrated efficacy in reducing revision surgery rates for pseudarthrosis in adult spinal deformity cases. However, their clinical application is limited by their high production costs. For instance, a study reported that the mean direct cost of BMP for index surgery was $14,000 ± $6400.136 Similarly, another analysis indicated that the mean direct cost of BMP per patient was $10,444 ± $4607.137 To reduce these costs, researchers are exploring alternative strategies, such as generating shorter peptides that mimic the therapeutic effects of full-length BMPs. These shorter peptides could potentially retain the biological activity of BMPs while being more cost-effective to produce. Additionally, advanced drug delivery systems like biodegradable hydrogels, polymeric microspheres, and nanoparticles are being developed to enhance BMP stability and targeted delivery, thereby reducing the required dosages and associated expenses. Pharmaceutical companies are working on advanced delivery platforms, implantable BMP-loaded scaffolds that can maintain protein release and long-term efficacy. Demonstrating cost-effectiveness, scalability and safety is going to be pivotal in enabling clinical adoption. Furthermore, the challenges to bringing these novel solutions into the mainstream of oncology care need to be addressed by healthcare providers and regulatory authorities.138 In addition, academic institutions collaborating with industry will be crucial to successful commercialization and patient access to treatments based on BMPs.
Methodology
A systematic literature review was conducted to assess recent advances in BMP delivery for glioma treatment. Key words “Bone Morphogenetic Proteins”, “Glioma treatment”, “Blood-Brain Barrier”, “Nanoparticle-based delivery”, and “Gene therapy strategies” were used to search PubMed, Scopus, and Google Scholar for published studies. Selected articles focused on BMP delivery methods, challenges, and preclinical/clinical outcomes. Data were extracted and synthesized to highlight emerging trends and therapeutic efficacy, ensuring the inclusion of high-quality, relevant studies.
Conclusion
This review examines the potential of BMPs in differentiating, inducing apoptosis, and modulating glioma stem cells, highlighting their therapeutic promise for glioma treatment. However, several challenges remain in the effective delivery of BMPs to gliomas, including issues related to degradation, limited penetration across the blood–brain barrier, and the risk of immune responses. Overcoming these obstacles relies on recent advancements in nanoparticle delivery systems, gene therapy, and CRISPR/Cas-based engineering. Additionally, exosome-mediated BMP delivery to differentiated cells has emerged as a novel approach for targeted therapy. Future research should focus on integrating these advanced delivery platforms with personalized medicine strategies to enhance therapeutic precision. BMPs hold significant potential for combinatorial treatments, synergistically working with chemotherapy, immunotherapy, and other targeted agents to reduce tumor recurrence and improve clinical outcomes. The development of new gene-editing technologies underscores the need to address ethical, regulatory, and safety challenges to enable clinical translation and commercialization. Ultimately, optimized BMP delivery systems may enhance glioma patient outcomes and serve as a foundation for the development of more effective therapies with broader clinical applications.
Data Sharing Statement
This is a review article and all relevant information is provided in the article.
Acknowledgments
The authors would like to thank the Medical and Health Science and Technology Project of Zhejiang Province (No. 2021KY064 to YHZ) for supporting this work.
Disclosure
The authors declare that they have no competing interests financial or non-financial or any other interests that might be perceived to influence the results and/or discussion reported in this paper.
References
1. Obrador E, Moreno-Murciano P, Oriol-Caballo M, et al. Glioblastoma therapy: past, present and future. Int J Mol Sci. 2024;25(5):2529. doi:10.3390/ijms25052529
2. Han PC, Baker TG. Glial and glioneuronal tumors: navigating the complexity of evolving concepts and new classification. J Neurol Sci. 2024;461:123058. doi:10.1016/j.jns.2024.123058
3. Jezierzański M, Nafalska N, Stopyra M, et al. Temozolomide (TMZ) in the treatment of glioblastoma multiforme—a literature review and clinical outcomes. Current Oncol. 2024;31(7):3994–4002. doi:10.3390/curroncol31070296
4. Fares J, Kanojia D, Cordero A, Ulasov I, Lesniak MS. Targeting the molecular mechanisms of glioma stem cell resistance to chemotherapy. In: Glioblastoma Resistance to Chemotherapy: Molecular Mechanisms and Innovative Reversal Strategies. Elsevier; 2021:587–634.
5. Wicher G, Holmqvist K, Forsberg-Nilsson K. Common denominators of self-renewal and malignancy in neural stem cells and glioma. Stem Cells Hum Dis. 2012;387–418.
6. Ferris SP, Hofmann JW, Solomon DA, Perry A. Characterization of gliomas: from morphology to molecules. Virchows Archiv. 2017;471(2):257–269. doi:10.1007/s00428-017-2181-4
7. Shaw R, Basu M, Karmakar S, Ghosh MK. MGMT in TMZ-based glioma therapy: multifaceted insights and clinical trial perspectives. Biochimica et Biophysica Acta (BBA)-Mol Cell Res. 2024;1871(3):119673. doi:10.1016/j.bbamcr.2024.119673
8. Verploegh IS, Conidi A, Brouwer RW, et al. Comparative single-cell RNA-sequencing profiling of BMP4-treated primary glioma cultures reveals therapeutic markers. Neuro-Oncology. 2022;24(12):2133–2145. doi:10.1093/neuonc/noac143
9. Bareke H, Ibáñez-Navarro A, Guerra-García P, et al. Prospects and advances in adoptive natural killer cell therapy for unmet therapeutic needs in pediatric bone sarcomas. Int J Mol Sci. 2023;24(9):8324. doi:10.3390/ijms24098324
10. Moysidou C-M, Barberio C, Owens RM. Advances in engineering human tissue models. Front Bioeng Biotechnol. 2021;8:620962.
11. Janjua TI, Rewatkar P, Ahmed-Cox A, et al. Frontiers in the treatment of glioblastoma: past, present and emerging. Adv Drug Delivery Rev. 2021;171:108–138. doi:10.1016/j.addr.2021.01.012
12. Katagiri T, Watabe T. Bone morphogenetic proteins. Cold Spring Harbor Perspect Biol. 2016;8(6):a021899. doi:10.1101/cshperspect.a021899
13. Galluzzi L, Vitale I, Kroemer G. Past, present, and future of molecular and cellular oncology. Front Oncol. 2011;1:1. doi:10.3389/fonc.2011.00001
14. Bozzato E, Bastiancich C, Préat V. Nanomedicine: a useful tool against glioma stem cells. Cancers. 2020;13(1):9. doi:10.3390/cancers13010009
15. Nayak S, Mahenthiran A, Yang Y, et al. Bone morphogenetic protein 4 targeting glioma stem-like cells for malignant glioma treatment: latest advances and implications for clinical application. Cancers. 2020;12(2):516. doi:10.3390/cancers12020516
16. Jhanwar-Uniyal M, Labagnara M, Friedman M, Kwasnicki A, Murali R. Glioblastoma: molecular pathways, stem cells and therapeutic targets. Cancers. 2015;7(2):538–555. doi:10.3390/cancers7020538
17. Caja L, Bellomo C, Moustakas A. Transforming growth factor β and bone morphogenetic protein actions in brain tumors. FEBS Lett. 2015;589(14):1588–1597. doi:10.1016/j.febslet.2015.04.058
18. Kaminska B, Cyranowski S. Recent advances in understanding mechanisms of TGF beta signaling and its role in glioma pathogenesis. Glioma Signaling. 2020;179–201.
19. Sun Z, Cai S, Zabkiewicz C, Liu C, Ye L. Bone morphogenetic proteins mediate crosstalk between cancer cells and the tumour microenvironment at primary tumours and metastases. Int J Oncol. 2020;56(6):1335–1351. doi:10.3892/ijo.2020.5030
20. Cruz JVR, Batista C, Afonso B, et al. Obstacles to glioblastoma treatment two decades after temozolomide. Cancers. 2022;14(13):3203. doi:10.3390/cancers14133203
21. Sachdeva R, Wu M, Johnson K, et al. BMP signaling mediates glioma stem cell quiescence and confers treatment resistance in glioblastoma. Sci Rep. 2019;9(1):14569. doi:10.1038/s41598-019-51270-1
22. Zhou W, Yan K, Xi Q. BMP signaling in cancer stemness and differentiation. Cell Regener. 2023;12(1):37. doi:10.1186/s13619-023-00181-8
23. Danielpour D. Advances and challenges in targeting tgf-β isoforms for therapeutic intervention of cancer: a mechanism-based perspective. Pharmaceuticals. 2024;17(4):533. doi:10.3390/ph17040533
24. Ehata S, Miyazono K. Bone morphogenetic protein signaling in cancer; some topics in the recent 10 years. Front Cell Develop Biol. 2022;10:883523. doi:10.3389/fcell.2022.883523
25. Biserova K, Jakovlevs A, Uljanovs R, Strumfa I. Cancer stem cells: significance in origin, pathogenesis and treatment of glioblastoma. Cells. 2021;10(3):621. doi:10.3390/cells10030621
26. Loftus AE, Romano MS, Phuong AN, et al. An ILK/STAT3 pathway controls glioblastoma stem cell plasticity. Dev Cell. 2024;59(24):3197–212.e7. doi:10.1016/j.devcel.2024.09.003
27. Tamayo E, Alvarez P, Merino R. TGFβ superfamily members as regulators of B cell development and function—implications for autoimmunity. Int J Mol Sci. 2018;19(12):3928. doi:10.3390/ijms19123928
28. Morokoff A, Ng W, Gogos A, Kaye AH. Molecular subtypes, stem cells and heterogeneity: implications for personalised therapy in glioma. J Clin Neurosci. 2015;22(8):1219–1226. doi:10.1016/j.jocn.2015.02.008
29. Zhou Q, Heinke J, Vargas A, et al. ERK signaling is a central regulator for BMP-4 dependent capillary sprouting. Cardiovasc Res. 2007;76(3):390–399. doi:10.1016/j.cardiores.2007.08.003
30. Groblewska M, Mroczko B. Pro-and antiangiogenic factors in gliomas: implications for novel therapeutic possibilities. Int J Mol Sci. 2021;22(11):6126. doi:10.3390/ijms22116126
31. Wu M, Wu S, Chen W, Li Y-P. The roles and regulatory mechanisms of TGF-β and BMP signaling in bone and cartilage development, homeostasis and disease. Cell Res. 2024;34(2):101–123. doi:10.1038/s41422-023-00918-9
32. Gao H, Chen Z, Zhao L, Ji C, Xing F. Cellular functions, molecular signalings and therapeutic applications: translational potential of deubiquitylating enzyme USP9X as a drug target in cancer treatment. Biochimica Et Biophysica Acta (BBA)-Reviews on Cancer. 2024;1879(3):189099. doi:10.1016/j.bbcan.2024.189099
33. Carén H, Stricker SH, Bulstrode H, et al. Glioblastoma stem cells respond to differentiation cues but fail to undergo commitment and terminal cell-cycle arrest. Stem Cell Reports. 2015;5(5):829–842. doi:10.1016/j.stemcr.2015.09.014
34. Hover LD. BMP Signaling in High Grade Gliomas. Vanderbilt University; 2016.
35. Shetab Boushehri MA, Dietrich D, Lamprecht A. Nanotechnology as a platform for the development of injectable parenteral formulations: a comprehensive review of the know-hows and state of the art. Pharmaceutics. 2020;12(6):510.
36. Zhang J, Li L. BMP signaling and stem cell regulation. Dev Biol. 2005;284(1):1–11. doi:10.1016/j.ydbio.2005.05.009
37. Xi G, Best B, Mania-Farnell B, James CD, Tomita T. Therapeutic potential for bone morphogenetic protein 4 in human malignant glioma. Neoplasia. 2017;19(4):261–270. doi:10.1016/j.neo.2017.01.006
38. Dietrich J, Diamond EL, Kesari S. Glioma stem cell signaling: therapeutic opportunities and challenges. Expert Rev Anticancer Ther. 2010;10(5):709–722. doi:10.1586/era.09.190
39. Sabbadini F, Bertolini M, De Matteis S, et al. The multifaceted role of TGF-β in gastrointestinal tumors. Cancers. 2021;13(16):3960. doi:10.3390/cancers13163960
40. Carreira ACO, Zambuzzi WF, Rossi MC, Astorino Filho R, Sogayar MC, Granjeiro JM. Bone morphogenetic proteins: promising molecules for bone healing, bioengineering, and regenerative medicine. Vitamin Hormon. 2015;99:293–322.
41. Van Gulden S. Molecular diversity in human pluripotent stem cell derived astrocyte progenitors and their association with subtypes of glioblastoma: Northwestern University; 2021.
42. Stevanovic M, Kovacevic-Grujicic N, Mojsin M, Milivojevic M, Drakulic D. SOX transcription factors and glioma stem cells: choosing between stemness and differentiation. World J Stem Cells. 2021;13(10):1417. doi:10.4252/wjsc.v13.i10.1417
43. Qu C. Interaction of epigenetics and SMAD signaling in stem cells and diseases: University of Southern California; 2014.
44. Jin J, Grigore F, Chen CC, Li M. Self-renewal signaling pathways and differentiation therapies of glioblastoma stem cells. Int J Oncol. 2021;59(1):1–11. doi:10.3892/ijo.2021.5225
45. Zhao Z, Bo Z, Gong W, Guo Y. Inhibitor of differentiation 1 (Id1) in cancer and cancer therapy. Int J Med Sci. 2020;17(8):995. doi:10.7150/ijms.42805
46. Kaye J, Mondal A, Foty R, Jia D, Langenfeld J. Bone morphogenetic protein receptor inhibitors suppress the growth of glioblastoma cells. Mol Cell Biochem. 2022;477(5):1583–1595. doi:10.1007/s11010-022-04383-7
47. Jiapaer S, Furuta T, Tanaka S, Kitabayashi T, Nakada M. Potential strategies overcoming the temozolomide resistance for glioblastoma. Neurologia medico-chirurgica. 2018;58(10):405–421. doi:10.2176/nmc.ra.2018-0141
48. Miranda A, Blanco-Prieto M, Sousa J, Pais A, Vitorino C. Breaching barriers in glioblastoma. Part I: molecular pathways and novel treatment approaches. Int J Pharm. 2017;531(1):372–388. doi:10.1016/j.ijpharm.2017.07.056
49. Gallo GO. Characterization of cellular and molecular responses of human glioblastoma to transforming growth factor-β signalling pathway inhibition. 2016.
50. Curry RN, Glasgow SM. The role of neurodevelopmental pathways in brain tumors. Front Cell Develop Biol. 2021;9:659055. doi:10.3389/fcell.2021.659055
51. Nieto-Sampedro M, Valle-Argos B, Gómez-Nicola D, Fernández-Mayoralas A, Nieto-Díaz M. Inhibitors of glioma growth that reveal the tumour to the immune system. Clin Med Insights. 2011;5:CMO–S7685.
52. Alfranca A, Martinez-Cruzado L, Tornin J, et al. Bone microenvironment signals in osteosarcoma development. Cell Mol Life Sci. 2015;72(16):3097–3113. doi:10.1007/s00018-015-1918-y
53. Shao R, Wang Y, Li L, Dong Y, Zhao J, Liang W. Bone tumors effective therapy through functionalized hydrogels: current developments and future expectations. Drug Delivery. 2022;29(1):1631–1647. doi:10.1080/10717544.2022.2075983
54. Carrêlo H, Soares PI, Borges JP, Cidade MT. Injectable composite systems based on microparticles in hydrogels for bioactive cargo controlled delivery. Gels. 2021;7(3):147. doi:10.3390/gels7030147
55. Djoudi A. Development of innovative nanocomposite hydrogels for locoregional treatment of glioblastoma: Université d’Angers. 2022.
56. Bin Haji Mansor MS. Functionalized polymer implants for the trapping of glioblastoma cells: Universite de Liege (Belgium); 2019.
57. Mansor MSBH. Functionalized polymer implants for the trapping of glioblastoma cells. 2019.
58. Hogan KJ. Development of extracellular matrix-based biomaterials for musculoskeletal tissue engineering: Rice University; 2023.
59. Kaur M, Sodhi RK, Jyothi VGS, et al. Brain targeting drug delivery systems for the management of brain disorders: molecular targets and nanotechnological strategies. In: Multifunctional Nanocarriers. Elsevier; 2022:289–345.
60. Karlsson J, Luly KM, Tzeng SY, Green JJ. Nanoparticle designs for delivery of nucleic acid therapeutics as brain cancer therapies. Adv Drug Delivery Rev. 2021;179:113999. doi:10.1016/j.addr.2021.113999
61. Duan M, Cao R, Yang Y, et al. Blood–brain barrier conquest in glioblastoma nanomedicine: strategies, clinical advances, and emerging challenges. Cancers. 2024;16(19):3300. doi:10.3390/cancers16193300
62. Deng CX. Targeted drug delivery across the blood–brain barrier using ultrasound technique. Therapeutic Delivery. 2010;1(6):819–848. doi:10.4155/tde.10.66
63. Martinez PJ, Green AL, Borden MA. Targeting diffuse midline gliomas: the promise of focused ultrasound-mediated blood-brain barrier opening. J Control Release. 2024;365:412–421. doi:10.1016/j.jconrel.2023.11.037
64. Bell M, Rooks CP, Agrahari V. Drug delivery approaches and imaging techniques for brain tumor. Nanother Brain Tumor Drug Delivery. 2021;109–126.
65. González-Gómez P, Anselmo NP, Mira H. BMPs as therapeutic targets and biomarkers in astrocytic glioma. Biomed Res Int. 2014;2014(1):549742. doi:10.1155/2014/549742
66. Zhang S, Uludağ H. Nanoparticulate systems for growth factor delivery. Pharm Res. 2009;26(7):1561–1580. doi:10.1007/s11095-009-9897-z
67. Zheng Q, Liu H, Yu W, et al. Mechanical properties of the brain: focus on the essential role of Piezo1‐mediated mechanotransduction in the CNS. Brain Behav. 2023;13(9):e3136. doi:10.1002/brb3.3136
68. Xu -Y-Y, Gao P, Sun Y, Duan Y-R. Development of targeted therapies in treatment of glioblastoma. Cancer Biol Med. 2015;12(3):223.
69. Cruz Da Silva E, Mercier M-C, Etienne-Selloum N, Dontenwill M, Choulier L. A systematic review of glioblastoma-targeted therapies in phases II, III, IV clinical trials. Cancers. 2021;13(8):1795. doi:10.3390/cancers13081795
70. Anjum T, Hussain N, Iqbal HM, Jedrzak A, Jesionowski T, Bilal M. Magnetic nanomaterials as drug delivery vehicles and therapeutic constructs to treat cancer. J Drug Delivery Sci Technol. 2023;80:104103. doi:10.1016/j.jddst.2022.104103
71. Sanchez-Duffhues G, Williams E, Goumans M-J, Heldin C-H, Ten Dijke P. Bone morphogenetic protein receptors: structure, function and targeting by selective small molecule kinase inhibitors. Bone. 2020;138:115472. doi:10.1016/j.bone.2020.115472
72. Ganjoo S, Puebla-Osorio N, Nanez S, et al. Bone morphogenetic proteins, activins, and growth and differentiation factors in tumor immunology and immunotherapy resistance. Front Immunol. 2022;13:1033642. doi:10.3389/fimmu.2022.1033642
73. Tang X, Zuo C, Fang P, et al. Targeting glioblastoma stem cells: a review on biomarkers, signal pathways and targeted therapy. Front Oncol. 2021;11:701291. doi:10.3389/fonc.2021.701291
74. Davis H, Raja E, Miyazono K, Tsubakihara Y, Moustakas A. Mechanisms of action of bone morphogenetic proteins in cancer. Cytokine Growth Factor Rev. 2016;27:81–92. doi:10.1016/j.cytogfr.2015.11.009
75. Patil A, Shaikh I, Kadam V, Jadhav K. Nanotechnology in therapeutics-current technologies and applications. Curr Nanosci. 2009;5(2):141–153. doi:10.2174/157341309788185532
76. King JL. Harnessing a platform hydrogel technology and stem cell therapies for cancer treatment and regenerative medicine: The University of North Carolina at Chapel Hill; 2023.
77. Attia N, Mashal M, Pemminati S, et al. Cell-based therapy for the treatment of glioblastoma: an update from preclinical to clinical studies. Cells. 2021;11(1):116. doi:10.3390/cells11010116
78. Yi Y, Hsieh I-Y, Huang X, Li J, Zhao W. Glioblastoma stem-like cells: characteristics, microenvironment, and therapy. Front Pharmacol. 2016;7:477. doi:10.3389/fphar.2016.00477
79. S Hersh D, S Wadajkar A, B Roberts N, et al. Evolving drug delivery strategies to overcome the blood brain barrier. Curr Pharm Des. 2016;22(9):1177–1193. doi:10.2174/1381612822666151221150733
80. Pandit A, Begum Y, Saha P, Swarnakar S. Nanotechnology based gene delivery strategies towards disease therapy; advances and applications. Adv Nanotechnol-Based Drug Delivery Systems. 2022;197–226.
81. Miranda A, Blanco-Prieto MJ, Sousa J, Pais A, Vitorino C. Breaching barriers in glioblastoma. Part II: targeted drug delivery and lipid nanoparticles. Int J Pharm. 2017;531(1):389–410. doi:10.1016/j.ijpharm.2017.07.049
82. Yuan M, Han Z, Liang Y, et al. mRNA nanodelivery systems: targeting strategies and administration routes. Biomater Res. 2023;27(1):90. doi:10.1186/s40824-023-00425-3
83. da Costa PMC. MicroRnas as molecular targets for non-viral gene therapy of glioblastoma: development of a lipid-based nanosystem for nucleic acid delivery to brain tumor cells: Universidade de Coimbra (Portugal); 2013.
84. Gu Z. Bioinspired and Biomimetic Polymer Systems for Drug and Gene Delivery. John Wiley & Sons; 2015.
85. Maso K, Grigoletto A, Vicent MJ, Pasut G. Molecular platforms for targeted drug delivery. Int Rev Cell Mol Biol. 2019;346:1–50.
86. Reguera-Nuñez E, Roca C, Hardy E, de la Fuente M, Csaba N, Garcia-Fuentes M. Implantable controlled release devices for BMP-7 delivery and suppression of glioblastoma initiating cells. Biomaterials. 2014;35(9):2859–2867. doi:10.1016/j.biomaterials.2013.12.001
87. Belkhodja F. Targeted therapy to overcome the blood-brain barrier in treating Glioblastoma: Hochschule Rhein-Waal; 2023.
88. Fateh ST, Moradi L, Kohan E, Hamblin MR, Dezfuli AS. Comprehensive review on ultrasound-responsive theranostic nanomaterials: mechanisms, structures and medical applications. Beilstein J Nanotechnol. 2021;12(1):808–862. doi:10.3762/bjnano.12.64
89. Ghorai SM, Deep A, Magoo D, Gupta C, Gupta N. Cell-penetrating and targeted peptides delivery systems as potential pharmaceutical carriers for enhanced delivery across the blood–brain barrier (BBB). Pharmaceutics. 2023;15(7):1999. doi:10.3390/pharmaceutics15071999
90. Chirasani SR. Cellular and molecular mechanisms of glioma growth control. 2009.
91. Rui Y, Green JJ. Overcoming delivery barriers in immunotherapy for glioblastoma. Drug Delivery Transl Res. 2021;11(6):2302–2316. doi:10.1007/s13346-021-01008-2
92. Sun M, Lee J, Chen Y, Hoshino K. Studies of nanoparticle delivery with in vitro bio-engineered microtissues. Bioact Mater. 2020;5(4):924–937. doi:10.1016/j.bioactmat.2020.06.016
93. Jiramongkolchai P, Owens P, Hong CC. Emerging roles of the bone morphogenetic protein pathway in cancer: potential therapeutic target for kinase inhibition. Biochem Soc Trans. 2016;44(4):1117–1134. doi:10.1042/BST20160069
94. Miao T, Wang J, Zeng Y, Liu G, Chen X. Polysaccharide‐based controlled release systems for therapeutics delivery and tissue engineering: from bench to bedside. Adv Sci. 2018;5(4):1700513. doi:10.1002/advs.201700513
95. Antoniac I. Bioceramics and Biocomposites: From Research to Clinical Practice. John Wiley & Sons; 2019.
96. Toome K. Homing peptides for targeting of brain diseases. Tartu; 2020.
97. Jeyapalan Z. Development of an inducible expression system for bone morphogenetic proteins (BMPs) in mammalian cells. 2008.
98. Agrawal AK, Urimi D, Jain S. Multifunctional polymeric nano-carriers in targeted drug delivery. In: Targeted Drug Delivery: Concepts and Design. 2015:461–500.
99. Ribeiro MLRC. Local treatment of glioblastoma with a hydrogel designed to recruit and efficiently damage cancer cells: Universidade do Minho (Portugal); 2021.
100. Bos EM, Binda E, Verploegh IS, et al. Local delivery of hrBMP4 as an anticancer therapy in patients with recurrent glioblastoma: a first-in-human Phase 1 dose escalation trial. Mol Cancer. 2023;22(1):129. doi:10.1186/s12943-023-01835-6
101. Sun Y, Chen L-G, Fan X-M, Pang J-L. Ultrasound responsive smart implantable hydrogels for targeted delivery of drugs: reviewing current practices. Int J Nanomed. 2022;17:5001. doi:10.2147/IJN.S374247
102. Aguilar LMC, Silva SM, Moulton SE. Growth factor delivery: defining the next generation platforms for tissue engineering. J Control Release. 2019;306:40–58. doi:10.1016/j.jconrel.2019.05.028
103. Hallbergson A. Recruitment of endogenous cortical progenitor cells by trophic factor gene delivery: Rosalind Franklin University of Medicine and Science; 2005.
104. Muzzio N, Moya S, Romero G. Multifunctional scaffolds and synergistic strategies in tissue engineering and regenerative medicine. Pharmaceutics. 2021;13(6):792. doi:10.3390/pharmaceutics13060792
105. Bordbar-Khiabani A, Gasik M. Smart hydrogels for advanced drug delivery systems. Int J Mol Sci. 2022;23(7):3665. doi:10.3390/ijms23073665
106. Ribeiro J, Astudillo-Ortiz EA, Babo PS, Gomes ME. Tissue engineering strategies for the treatment of skeletal maxillofacial defects resulting from neoplasms resections. In: Biomaterials for 3D Tumor Modeling. Elsevier; 2020:697–730.
107. Chang C-W, Holter JC, Song JW. Microfluidic Models of the Tumor Microenvironment. 2022.
108. Echeverria Molina MI, Malollari KG, Komvopoulos K. Design challenges in polymeric scaffolds for tissue engineering. Front Bioeng Biotechnol. 2021;9:617141.
109. Floyd JA, Galperin A, Ratner BD. Drug encapsulated polymeric microspheres for intracranial tumor therapy: a review of the literature. Adv Drug Delivery Rev. 2015;91:23–37. doi:10.1016/j.addr.2015.04.008
110. Zhang S, Fang H, Tian H. Recent advances in degradable biomedical polymers for prevention, diagnosis and treatment of diseases. Biomacromolecules. 2024.
111. Garcia-Mazas C, Csaba N, Garcia-Fuentes M. Biomaterials to suppress cancer stem cells and disrupt their tumoral niche. Int J Pharm. 2017;523(2):490–505. doi:10.1016/j.ijpharm.2016.12.013
112. Hosseini FS, Laurencin CT. Advanced electrospun nanofibrous stem cell niche for bone regenerative engineering. Regenerative Engineering Transl Med. 2023;9(2):165–180. doi:10.1007/s40883-022-00274-x
113. Fornaguera Puigvert C. Development of multifunctional polymeric nanoparticles by nano-emulsion templating as advanced nanocarriers targeting the blood-brain barrier. 2015.
114. Raja E, Komuro A, Tanabe R, et al. Bone morphogenetic protein signaling mediated by ALK-2 and DLX2 regulates apoptosis in glioma-initiating cells. Oncogene. 2017;36(35):4963–4974. doi:10.1038/onc.2017.112
115. Aguilera-Márquez J, de Dios-Figueroa G, Reza-Saldivar E, Camacho-Villegas T, Canales-Aguirre A, Lugo-Fabres P. Biomaterials: emerging systems for study and treatment of glioblastoma. Neurol Perspectives. 2022; 2:S31–S42.
116. Crivii C-B, Boșca AB, Melincovici CS, et al. Glioblastoma microenvironment and cellular interactions. Cancers. 2022;14(4):1092. doi:10.3390/cancers14041092
117. La Rosa L. A novel immune-competent murine model to evaluate the efficacy of a microRNA-based therapy for the pediatric brain tumor Medulloblastoma. 2024.
118. Abadi B, Ahmadi-Zeidabadi M, Dini L, Vergallo C. Current status and challenges of stem cell-based therapy for the treating of glioblastoma multiforme. Hematol/Oncol Stem Cell Ther. 2021;14(1):1–15. doi:10.1016/j.hemonc.2020.08.001
119. Bach D-H, Park HJ, Lee SK. The dual role of bone morphogenetic proteins in cancer. Mol Therapy-Oncolytics. 2018;8:1–13. doi:10.1016/j.omto.2017.10.002
120. Banerjee K, Núñez FJ, Haase S, et al. Current approaches for glioma gene therapy and virotherapy. Front Mol Neurosci. 2021;14:621831. doi:10.3389/fnmol.2021.621831
121. Zhang M, Hu S, Liu L, et al. Engineered exosomes from different sources for cancer-targeted therapy. Signal Transduction Targeted Ther. 2023;8(1):124. doi:10.1038/s41392-023-01382-y
122. Jin X, Zhang J, Zhang Y, et al. Different origin-derived exosomes and their clinical advantages in cancer therapy. Front Immunol. 2024;15:1401852. doi:10.3389/fimmu.2024.1401852
123. Capoferri D, Filiberti S, Faletti J, Tavani C, Ronca R. Ten years of CRISPRing cancers in vitro. Cancers. 2022;14(23):5746. doi:10.3390/cancers14235746
124. Zeng J, Zeng XX. Systems medicine for precise targeting of glioblastoma. Mol Biotechnol. 2023;65(10):1565–1584. doi:10.1007/s12033-023-00699-x
125. Brown CFC. Characterization of Bioactive Components in Decellularized Adipose Tissue Scaffolds for Tissue Engineering. Queen’s University (Canada); 2014.
126. Wang X. Neuronal conversion of human glioblastoma cells by single neuronal transcription factor: The Pennsylvania State University; 2020.
127. Calori IR, Braga G, de Jesus P, Bi H, Tedesco AC. Polymer scaffolds as drug delivery systems. Eur Polym J. 2020;129:109621.
128. Chen A. Development and delivery of genome-editing therapies for improved glioblastoma treatment: Yale University; 2022.
129. Liebelt BD, Shingu T, Zhou X, Ren J, Shin SA, Hu J. Glioma stem cells: signaling, microenvironment, and therapy. Stem Cells Int. 2016;2016(1):7849890. doi:10.1155/2016/7849890
130. Dalmo E, Johansson P, Niklasson M, Gustavsson I, Nelander S, Westermark B. Growth-inhibitory activity of bone morphogenetic protein 4 in human glioblastoma cell lines is heterogeneous and dependent on reduced Sox2 expression. Mol Cancer Res. 2020;18(7):981–991. doi:10.1158/1541-7786.MCR-19-0638
131. Golán-Cancela I, Caja L. The TGF-β family in glioblastoma. Int J Mol Sci. 2024;25(2):1067. doi:10.3390/ijms25021067
132. Mansor MH, Garcion E, Ramalapa B, et al. Polymer-based protein delivery systems for loco-regional administration. In: Green Synthesis in Nanomedicine and Human Health. CRC Press; 2021:249–270.
133. Chen Y-HM. Pre-Clinical Assessment and Optimization of the IGF-Trap for the Treatment of High-Grade Gliomas. McGill University (Canada); 2021.
134. Humphreys PA, Woods S, Smith CA, et al. Optogenetic control of the BMP signaling pathway. ACS Synth Biol. 2020;9(11):3067–3078. doi:10.1021/acssynbio.0c00315
135. Stawarska A, Bamburowicz-Klimkowska M, Runden-Pran E, et al. Extracellular vesicles as next-generation diagnostics and advanced therapy medicinal products. Int J Mol Sci. 2024;25(12):6533. doi:10.3390/ijms25126533
136. Malham GM, Louie PK, Brazenor GA, Mobbs RJ, Walsh WR, Sethi RK. Recombinant human bone morphogenetic protein-2 in spine surgery: recommendations for use and alternative bone substitutes—a narrative review. J Spine Surg. 2022;8(4):477. doi:10.21037/jss-22-23
137. Onafowokan OO, Uzosike AC, Sharma A, et al. Treatment of adult spine deformity: a retrospective comparison of bone morphogenic protein and bone marrow aspirate with bone allograft. Acta Neurochirurgica. 2024;166(1):448. doi:10.1007/s00701-024-06346-x
138. Martinez PJ. Enhancing drug delivery in diffuse midline gliomas using focused ultrasound mediated bbb opening: optimization of acoustic and microbubble parameters: University of Colorado at Boulder; 2024.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.