")
Back to Journals » Clinical Ophthalmology » Volume 19
Retinopathy of Prematurity (ROP): An Overview of Biomarkers in Various Samples for Prediction, Diagnosis, and Prognosis
Authors Huang D, Liu Z, Deng Y
Received 24 January 2025
Accepted for publication 22 April 2025
Published 7 May 2025 Volume 2025:19 Pages 1515—1530
DOI https://doi.org/10.2147/OPTH.S519292
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dan Huang,1 ZhuoQi Liu,2 Yan Deng1,3
1Department of Ophthalmology Center, The Second Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang, People’s Republic of China; 2Department of Biochemistry and Molecular Biology, School of Basic Medical Sciences, Jiangxi Medical College, Nanchang University, Nanchang, People’s Republic of China; 3Jiangxi Key Laboratory of Molecular Medicine, The Second Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang, People’s Republic of China
Correspondence: ZhuoQi Liu, Department of Biochemistry and Molecular Biology, School of Basic Medical Sciences, Jiangxi Medical College, Nanchang University, Nanchang, People’s Republic of China, Tel +18970949577, Email [email protected] Yan Deng, Department of Ophthalmology Center, The Second Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang, People’s Republic of China, Tel +15970464160, Email [email protected]
Abstract: Retinopathy of Prematurity (ROP) is a proliferative retinal vascular disease marked by abnormal development of retinal vessels in low birth weight preterm infants. It is one of the leading causes of blindness in preterm infants. Current ROP screening methods impose high demands on both the equipment and the expertise of ophthalmologists, which limits their widespread application, particularly in secondary hospitals and remote areas. Thus, the identification of relevant biomarkers and the development of simpler detection methods are important and promising. Non-invasive or minimally invasive sampling methods, along with biomarkers possessing high sensitivity and specificity, could greatly enhance neonatal screening, facilitate early diagnosis, and improve prevention of blindness in preterm infants. This review provides relevant medical insights for clinical practice. This review explored, compares and analyzes various sampling sources. It compares and analyzes research on ROP-related biomarkers derived from these samples.
Plain Language Summary: This review compares different human fluid sampling sources for screening, predicting, diagnosing, and prognosticating ROP patients, and compares and analyzes the research on ROP-related biomarkers from different samples. Non-invasive or minimally invasive methods of obtaining samples and selecting biomarkers with high validity promise to be more beneficial for newborn, early diagnosis of ROP, and better prevention of blindness in preterm infants, providing relevant medical references for clinical practice.
Keywords: retinopathy of prematurity, biomarkers, neonatal screening, early diagnosis
Introduction
Retinopathy of Prematurity (ROP) is a proliferative retinal vascular disease that affects preterm infants.1,2 While ROP may regress spontaneously in some cases, it can progress from mild stages (ROP stages I and II) to more severe forms (ROP stages III, IV, and V) in others, potentially resulting in complete vision loss if not treated promptly.3 However, ROP is largely preventable, and reducing the incidence of blindness hinges on high-quality neonatal care, comprehensive ROP screening programs, and the expertise of skilled ophthalmologists.4 Although ROP is classified as a neovascular disease, the underlying molecular mechanisms remain unclear. It is hypothesized that multiple pathological risk factors, including low birth weight, gestational age, postnatal oxygen fluctuations, and inflammation, contribute to ROP progression by inducing retinal vascular occlusion and neovascularization.5 This, in turn, triggers oxidative stress and the release of pro-inflammatory and pro-angiogenic factors.6 These cytokines play a pivotal role in the onset and progression of ROP, prompting numerous studies to focus on detecting ROP-related factors for early prediction and intervention to mitigate the incidence and severity of ROP in preterm infants.
Currently, ROP screening by the neonatologist is based on birth weight and gestational age, with ROP staging based on binocular indirect ophthalmoscopy (BIO) and/or wide-field retinal imaging systems.7,8 However, both methods require pupil dilation, the use of an eyelid speculum, and may involve scleral indentation, potentially causing side effects such as physiological stress, apnea, and cardiovascular instability.9,10 Additionally, multiple examinations are often required to reach a clinical conclusion, with the decision to initiate treatment largely depending on the ophthalmologist’s clinical experience11–13 or AI.14 In light of research on the pathogenesis of ROP, various factors have been measured in different sample types, including peripheral blood, umbilical cord blood, amniotic fluid, placenta, vitreous fluid, aqueous humor, urine, and tears, to elucidate their correlation with ROP pathobiology15,16 (shown in Figure 1). This review aims to evaluate the existing ROP detection methods, with the goal of identifying more effective, safer, and simpler approaches that could reduce the frequency of ROP staging exams in preterm infants. Furthermore, it seeks to identify relevant biomarkers that could enable the development of more personalized ROP screening protocols, thereby improving the diagnosis and prognosis of ROP and alleviating the burden on patients, families, and healthcare providers.
 |
Figure 1 Different detection methods of ROP, including peripheral blood, umbilical cord blood, amniotic fluid, placenta, vitreous humor, aqueous humor, urine and tear fluid. |
Different Detection Methods
Peripheral Blood
Peripheral blood, composed of various cell types and compounds such as salts and proteins, has been extensively studied for its potential in screening, predicting, diagnosing, and prognosticating Retinopathy of Prematurity (ROP). Research by Villegas-Becerril et al has identified Vascular Endothelial Growth Factor (VEGF) and Insulin-like Growth Factor 1 (IGF-1) as important markers in predicting the risk of ROP.17 VEGF, a key molecule involved in pathological retinal vascular changes,18,19 is downregulated during stage I ROP and upregulated in the Müller glial cells of the peripheral avascular retina during stage II.20–22 Hellgren and Yenice discovered that preterm infants who later developed ROP had significantly lower circulating VEGF levels at birth.23,24 Additionally, studies by Pieh and Yalin demonstrated that VEGF levels significantly increased in the blood of patients with late-stage or treatment-requiring ROP.25,26 Thus, maintaining physiological levels of VEGF may prevent ROP progression, while reducing pathological VEGF levels in advanced ROP could help mitigate disease progression. These clinical findings are strongly supported by results from oxygen-induced retinopathy (OIR) animal models.27–29 IGF-1, essential for retinal vascular formation during normal eye development,30–32 stimulates VEGF synthesis.33 When IGF-1 levels are low, VEGF is unable to activate the Akt signaling pathway during the first stage of ROP, leading to endothelial cell apoptosis. Several studies have confirmed that low blood IGF-1 levels are associated with the development and increased severity of ROP,34–36 and early restoration of IGF-1 to normal levels can prevent the onset of ROP.37
A large body of research has also shown that various inflammatory factors in the blood, such as IL-6, IL-8, IL-18, and TNF-α, play significant roles in the occurrence and progression of ROP as regulators of angiogenesis. IL-6, which has both pro-inflammatory and anti-inflammatory effects,38 can promote VEGF expression.39 Multiple studies have reported elevated IL-6 levels in the plasma/serum of preterm infants before and after birth in those who eventually develop ROP, whether mild or severe.34,40–42 IL-8, the first chemokine studied, has notable angiogenic activity and induces ocular inflammation.43 Several studies have demonstrated a significant association between elevated IL-8 levels in the plasma/serum of preterm infants after birth and the development of severe ROP,42,44,45 findings that have been further validated in animal experiments.46 IL-18, a pro-inflammatory cytokine with immunomodulatory properties, exhibits both angiogenic and angiostatic effects.47 Sood et al observed lower serum IL-18 levels in preterm infants with ROP compared to those without the disease, although IL-18 levels increased within three weeks after birth.40 The biphasic pattern of IL-18 expression aligns with the two stages of ROP development,48 underscoring its role as a time-sensitive angiogenic regulator.40 TNF-α, primarily produced by monocytes or macrophages, is a major initiator of inflammation.49 It enhances the production of other cytokines, such as IL-8, basic Fibroblast Growth Factor (bFGF), and MCP-1,50 in perivascular retinal microglia through autocrine or paracrine mechanisms and plays a role in the formation of hypoxic retinal neovascularization.51,52 Clinical studies by Hellgren and Holm found that elevated TNF-α levels in the serum/plasma of preterm infants are associated with the development and severity of ROP.34,42,44 Moreover, animal studies have confirmed that inhibiting TNF-α significantly improves vascular restoration in the ischemic retina of the mouse OIR model and reduces pathological neovascularization.53,54
In addition to cytokine detection, immune cell infiltration in peripheral blood has also been linked to ROP. Peripheral Blood Mononuclear Cells (PBMCs), which include lymphocytes (T cells, B cells, and Natural Killer cells), monocytes, and dendritic cells, are central to the immune response.55 Kurtul and others demonstrated that lymphocyte count is negatively correlated with ROP, indicating its independent predictive value.56 Further studies by Zhou and Li on PBMCs in ROP patients requiring treatment revealed significant changes in non-coding RNAs (tsRNA, miRNA, circRNA), with hsa_circRNA_061346, hsa_circRNA_092369, and hsa_circRNA_103554 emerging as promising biomarkers and molecular targets for diagnosing treatment-required ROP.57,58
Moreover, research on the genetic polymorphisms of peripheral blood has identified numerous genes involved in pathways related to fetal retinal growth and development, angiogenesis, inflammation, neurodegeneration, and oxidative stress, which are associated with ROP.59 Rathi et al found that gene variants in the complement pathway (CFH, CFB, C3), ECM remodeling (FBLN5, MMP9), leukocyte transendothelial migration and activation (CXCR4), HIF1A signaling and angiogenesis (ANGPT2, H2AFX, and VEGF), and developmental processes (TGFb1, IHH) are closely linked to the pathogenesis of ROP.59 Fevereiro-Martins and others discovered that polymorphisms in genes involved in the WNT signaling pathway, VEGFA gene, eNOS gene, and Brain-Derived Neurotrophic Factor (BDNF) gene are also associated with ROP development.60 Xu et al highlighted the role of lactate metabolism in ROP development, finding that a large number of lactate metabolism-related genes (LMRGs) are significantly associated with ROP, confirming the involvement of these genes in the disease’s pathogenesis.61
Peripheral blood, typically collected from peripheral veins, is easily accessible and represents a minimally invasive and routine method for preterm infants, allowing for repeated analysis. Blood tests reflect cellular activity throughout the body and have been widely applied across various diseases.
Umbilical Cord Blood
Umbilical cord blood, collected from the umbilical vein at the time of delivery, has been extensively studied for its relationship with ROP, particularly in the context of VEGF and IGF-1 levels. Research consistently shows that elevated VEGF levels in the cord blood of ROP patients and low serum VEGF content in umbilical cord blood are independent risk factors for the development of ROP in preterm newborns.15,24,35 IGF-1 levels are also decreased, with low levels of IGF-1 in the cord blood of very preterm infants negatively correlating with severe ROP,15,35,62,63 positioning cord blood IGF-1 as a biomarker for severe ROP risk. Cekmez et al found that levels of Apelin, a vascular endothelial growth factor necessary for normal vascular growth and endothelial cell proliferation,64,65 are lower in the umbilical cord blood of ROP patients at birth, with changes in Apelin levels positively correlating with changes in IGF-1 levels.62 Apelin is implicated in cell proliferation and angiogenesis.66
Furthermore, elevated expression of numerous inflammatory factors in umbilical cord blood has been linked to ROP development and severity, with the expression of inflammatory factors (MIP-1β, MCP-1) inversely correlated with gestational age (GA) and birth weight (BW).67 Yu et al reported that elevated levels of Monocyte Chemoattractant Protein-1 (MCP-1), Macrophage Inflammatory Proteins (MIP-1α, MIP-1β), and IL-7 in umbilical cord serum predict ROP risk, with MIP-1β associated with ROP severity.67 Park et al demonstrated that high concentrations of inflammatory mediators (IL-6 and C5a) in umbilical cord blood collected at birth are significantly associated with an increased risk of severe ROP and Type 1 ROP.68 Elevated IL-6 levels in umbilical cord plasma can predict ROP severity and serve as an independent marker for severe ROP, while increased C5a concentrations can assess ROP severity and the need for laser treatment.68 Thus, the combined analysis of various inflammatory factors offers a more accurate prediction of ROP development.
In addition to cytokines, protein level detection in umbilical cord blood has also been closely linked to ROP. TGFBI, an extracellular matrix protein associated with angiogenesis, inflammation, and embryonic development, plays a key role in regulating immune and inflammatory responses.69 Endoglin, critical in post-occlusive reperfusion and neovascular diseases, is involved in angiogenesis, neovascular formation, and vascular remodeling.70 Song et al found that reduced TGFBI levels in cord blood are significantly associated with severe ROP and Type 1 ROP, with low Endoglin levels serving as a predictor for Type 1 ROP.70 A combined predictive model based on TGFBI, Endoglin levels, and weight data can serve as a reliable birth indicator for neonatal ROP risk.70 Additionally, Madan et al found higher levels of deamidated globulin chains in the cord blood of preterm infants with severe ROP,71 where deamidation is a form of protein damage associated with various pathological conditions.72,73
Umbilical cord blood at birth directly reflects the intrauterine environment’s impact on the fetus, including hypoxia, stress, injury, and infection/inflammation.68 Compared to peripheral blood, it is collected at an earlier stage, allowing for a more timely reflection of the pathological processes involved in ROP.
Amniotic Fluid
Amniotic fluid, collected through direct puncture during delivery, has been examined in preterm infants to assess its relationship with Retinopathy of Prematurity (ROP). Studies, such as those by Woo et al, have identified significant correlations between elevated levels of inflammatory mediators (eg, IL-6 and IL-8) and angiogenic mediators (eg, Endoglin, Endostatin, and IGFBP-2) in the amniotic fluid and the severity of ROP.74 These biomarkers, combined with prenatal factors like gestational age and birth weight, can predict ROP’s occurrence and progression.74 Endostatin, known for inhibiting angiogenesis, may counteract the effects of VEGF and other growth factors.74 IGFBP-2, which plays a role in cell proliferation and angiogenesis, is also expressed in fetal and placental tissues.33,75 Additionally, Jang et al found that lower levels of IL-10 and TNF-α in amniotic fluid were significantly associated with ROP, and increased MMP-2 levels were identified as a risk factor for the disease.76 MMP-2, a protease involved in extracellular matrix degradation, is linked to pathological retinal neovascularization.77,78
Because amniotic fluid is collected early, it allows for the detection of factors that may reflect the initial stages of ROP, providing a timely insight into the disease’s development.
Placenta
The placenta serves as the critical interface between mother and fetus, facilitating the exchange of nutrients and oxygen. Research has shown that placental pathology significantly impacts postnatal conditions in preterm infants, such as bronchopulmonary dysplasia, necrotizing enterocolitis, and neurocognitive and neurovascular development.79–85 Histological examinations of the placenta can provide valuable insights into the risks of adverse neonatal outcomes, particularly in extremely preterm infants (EPT) born before 28 weeks of gestation.86
Placental function is directly linked to the underlying mechanisms of ROP. For instance, Leviton et al demonstrated that preterm infants with impaired placental implantation exhibited significantly lower IGF-1 levels in peripheral blood on the first day post-birth.87 However, the relationship between placental infection, inflammation, and ROP remains controversial. Some studies suggest a strong association between placental inflammation (eg, chorioamnionitis, funisitis) and an increased risk of ROP.88–92 Inflammatory conditions in the placenta may trigger cytokine release into the fetal circulation, contributing to ROP development. Chen et al, for example, found that co-existing placental bacterial infection and histological inflammation were linked to an increased risk of Zone I ROP but not severe ROP.88 Conversely, other studies have suggested no significant correlation and even a protective effect of placental inflammation against ROP.93–97 Owen et al posited a protective relationship between acute placental inflammation and ROP risk,16 a finding supported by Park et al, who observed a decreased ROP risk with the progression of acute histological chorioamnionitis (HCA).97 These contradictory findings indicate a complex relationship between placental function, inflammation, and ROP, warranting further investigation.
Moreover, epigenetic investigations by Bulka et al on placental tissue unveiled that placental DNA methylation at 16 CpG sites in 8 genes linked to mothers of extremely low gestational age newborns (ELGAN) is associated with early ROP onset risk.98 Methylation patterns in genes like Serum Amyloid A (SAA1 and SAA2), Myeloperoxidase (MPO), C-Reactive Protein (CRP), and Tumor Necrosis Factor Receptor Superfamily Member 1B (TNFRSF1B) exhibit a negative correlation with early ROP onset risk.98 Conversely, methylation at three sites in the Tumor Necrosis Factor Receptor Superfamily Member 1A (TNFRSF1A) gene is positively linked to early ROP risk. Furthermore, methylation at two sites in the Brain-Derived Neurotrophic Factor (BDNF) and Angiopoietin 1 (ANGPT1) genes respectively correlates positively/negatively with early ROP risk.98 Assessment of CpG methylation sites across multiple genes can serve as valuable predictive biomarkers for ROP, offering avenues for early intervention to mitigate disease severity.
Studies on other placental elements, such as chemical composition, have also been insightful. For example, Deev et al found altered levels of elements like nitrogen and potassium in the placentas of ROP patients, with nitrogen content potentially serving as a preclinical biomarker for the disease.99 Research into placental nutrients has similarly shown correlations between omega-3 receptor expression and ROP occurrence,100 emphasizing the role of omega-3 in retinal vascularization and reducing the severity of pathological neovascularization.54,101
Histological examination of placental tissue offers early insights into the pathological processes of ROP, enhancing our understanding of the disease’s pathogenesis and providing clinical insights for early prediction and prevention of ROP onset and progression.
Vitreous Fluid
The vitreous humor, which constitutes 80% of the eye’s volume, is predominantly composed of water (98–99.7%).102 It forms a transparent gel structure containing a myriad of diluted structural macromolecules (such as hyaluronic acid (HA), proteoglycans, collagen, and non-collagen proteins), non-structural proteins (serum), and a small population of cells (hyalocytes).103 Given its proximity to the retina, particularly when the blood-retinal barrier (BRB) is compromised, the vitreous can accumulate secretory products from the retina.104 Consequently, in vitreoretinal diseases, the composition of the vitreous undergoes alterations due to the varied expression of proteins under distinct pathological conditions.103
Studies have identified elevated levels of angiogenic factors like VEGF,59,105–107 erythropoietin,108 angiopoietin-1, and angiopoietin-2 in the vitreous of ROP patients,109 while anti-angiogenic factors such as pigment epithelium-derived factor and VEGF165b are decreased.106,110 Angiopoietins work in conjunction with VEGF, contributing to both physiological and pathological neovascularization.109 Higher levels of Ang-1 and Ang-2 have been observed in the vitreous of infants with moderate to late-stage ROP.111 Although intravitreal anti-VEGF injections are a common treatment for ROP, particularly aggressive posterior ROP.112,113 Nonetheless, some side effects have been observed in neonates treated with anti-VEGF for ROP, including neovascular recurrence,114 enduring impairments in photoreceptor integrity,115 and compromised eye and organ development.116–118 Studies also indicate resistance to anti-VEGF therapy in some patients,119 underscoring the necessity of identifying alternative angiogenic or anti-angiogenic cytokines implicated in ROP pathogenesis.
Beyond angiogenic factors, studies have documented escalated levels of numerous inflammatory factors, complement factors, and chemokines in the vitreous of ROP patients. Sato and Velez-Montoya, for example, found increased levels of erythropoietin, VEGF, IL-6, IL-7, IL-15, Eotaxin, G-CSF, IP-10, and RANTES in the vitreous.120 Complement factors like CFH, C3, and C4,59 typically downregulated in normal preterm infants due to immune immaturity,121,122 are upregulated in ROP patients, suggesting a significant role for the complement pathway in ROP development.59 The chemokine receptor CXCR4, which facilitates lymphocyte and monocyte migration,123 has been shown to influence retinal vascular sprouting,124 and RANTES, a chemokine critical for innate immunity in neonates, has demonstrated complex roles in ROP.125 Sato et al have found that RANTES exhibits significantly higher vitreous levels in both active and inactive ROP patients compared to non-ROP individuals.120 However, another study reported lower RANTES concentrations in the vitreous of preterm infants with severe ROP, with higher RANTES levels associated with reduced ROP risk,44 suggesting a protective role of RANTES.
Additionally, examinations of proteins in the vitreous of ROP patients, such as Opticin, a glycoprotein abundant in the human vitreous extracellular matrix (ECM) and an endogenous anti-angiogenic factor,126,127 have shown reduced expression of the anti-angiogenic protein Opticin in the vitreous of ROP patients.3 Intravitreal administration of Opticin has demonstrated efficacy in preventing retinal neovascularization development, with animal studies corroborating Opticin’s ability to promote regression of established retinal neovascularization in a mouse model of oxygen-induced retinopathy.3
However, due to the invasive nature of vitreous sampling, this method of “screening” or of prophylactic treatment, is not currently practical. Current knowledge primarily comes from animal studies, which provide valuable insights into retinal conditions and help guide clinical research on ROP’s pathogenesis.
Aqueous Humor
The aqueous humor is secreted by the ciliary epithelium, extending to the serrated margin and reaching the peripheral retina. Therefore, the cytokine levels in the aqueous humor of ROP patients are likely to reflect retinal-related cytokine levels, similar to those in the vitreous.107 Studies by Nonobe and Velez-Montoya have found elevated levels of VEGF in the aqueous humor of late-stage ROP patients, with a significant reduction in VEGF concentration after intravitreal injection of anti-VEGF (bevacizumab).107,128 Liang et al further observed that VEGF levels in the aqueous humor of preterm infants with severe ROP (aggressive retinopathy of prematurity, A-ROP) were higher than those with milder forms (threshold ROP and type 1 pre-threshold ROP).129 The VEGF levels were negatively correlated with the lesion area and stage of ROP but positively correlated with the degree of venous tortuosity, while unrelated to arterial tortuosity.129
Moreover, Lyu et al detected elevated levels of VEGF, interferon-γ (IFN-γ), IL-10, and IL-12 in the aqueous humor of ROP patients, correlating with the severity of ROP.130 Notably, higher levels of VEGF and MIP-1β were independently associated with the need for ROP retreatment.130
In addition to VEGF and cytokines, other anti-angiogenic factors such as Col1a1, tRF-1001, and 16K-PRL have been detected in the aqueous humor of ROP patients. Animal studies have shown that Col1a1 can reduce retinal neovascularization and ischemic areas, making it a promising therapeutic target.131 Clinical studies by Xia et al also observed upregulated expression of Col1a1 in the aqueous humor of ROP patients.131 tRF-1001, a novel class of non-coding RNA transcripts with anti-angiogenic properties, has shown downregulation in the retina of an oxygen-induced retinopathy (OIR) animal model and in the aqueous humor of patients with age-related macular degeneration (AMD).132 The upregulation of tRF-1001 could inhibit pathological angiogenesis, offering potential therapeutic avenues.132 16K-PRL, a potent angiogenesis inhibitor produced locally in the eyes of ROP patients, has been linked to the regression of intraocular vessels, with Dueñas et al reporting significantly elevated PRL levels in the aqueous humor of ROP patients.133
Aqueous humor is generally collected using a 30-gauge needle through a clear corneal puncture, obtaining 20–30 μL of undiluted aqueous humor from each eye, is somewhat invasive and may pose severe complications. Current research on aqueous humor predominantly focuses on glaucoma and certain fundus diseases post-intravitreal drug injection, collecting aqueous humor for relevant research to provide insights into ROP pathogenesis-related mechanisms.
Urine
Urinary VEGF levels are easily measurable and can be used for the early diagnosis of ROP. Studies by Levesque and others have found that low levels of VEGF in urine during the first month after birth are associated with the development of ROP.134 Early research by Kwinta and subsequent studies by Levesque and Yenice found that infants with ROP requiring active intervention exhibited decreased urinary VEGF levels.24,134,135
In addition to VEGF, other inflammatory markers such as IL-8 and IL-6 can also be detected in the urine of ROP patients. IL-8 plays a significant role in the recruitment of neutrophils in inflammation, cell adhesion, tumor growth, angiogenesis, neuronal protection, and brain development.43 Studies have shown similar levels of IL-6, IL-8, and VEGF in the urine of both ROP and non-ROP groups, but there is a positive correlation between the levels of IL-8, IL-6, and VEGF in urine, indicating that the level of IL-6 increases with the levels of IL-8 and VEGF in urine, and the level of VEGF also increases with the level of IL-8 in urine.45
Beyond VEGF and inflammatory markers, researchers have also explored the relationship between urine metabolites and ROP, including oxidative products like 8-hydroxy-2ʹ-deoxyguanosine (8-OHdG) and N-terminal pro B-type natriuretic peptide (NTproBNP). 8-OHdG, a sensitive biomarker of oxidative DNA damage,136 has been found at significantly higher levels in the urine of ROP patients, suggesting its potential as a screening indicator for ROP.137 NTproBNP, widely used to assess conditions such as heart failure and bronchopulmonary dysplasia,138,139 was also found to be elevated in the first month after birth in preterm infants under 30 weeks of gestation, correlating with a higher risk of severe ROP.140 Czernik et al identified a significant increase in the urine NTproBNP/creatinine ratio (UNBCR) in preterm infants with severe ROP, further underscoring its predictive value.141
However, urine collection in newborns presents challenges due to the difficulty in obtaining samples on demand. Typically, urine is collected using diapers or pads, which may lead to contamination and lower accuracy, limiting its utility as a diagnostic method.
Tears
Tears, a complex mixture of proteins, lipids, mucins, water, and salts, have recently been shown to contain 1526 proteins through proteomic analysis,142 making them less complex than serum or plasma. Tears are ideal for assessing biomarkers and molecular characteristics related to ocular vascular changes in both health and disease. Numerous studies have explored the relationship between ocular diseases and tear composition, including dry eye disease (DED), vernal conjunctivitis, diabetic retinopathy, Graves’ orbitopathy, ocular tumors, and glaucoma.142–147
Vinekar et al analyzed pro-angiogenic factors in the tears of preterm infants with ROP, finding lower VEGF levels in those with ROP, especially in progressing cases.148 Conversely, angiogenin levels were higher, and the ratio of angiogenin to birth weight, gestational age, and/or VEGF could serve as a potential non-invasive screening biomarker for ROP.148 Magnani and others further confirmed that tear VEGF levels negatively correlate with the severity of ROP, with significantly lower levels in late-stage (stage 3) ROP patients compared to those in earlier stages or those with regressed or resolving ROP.111 In contrast, Ang-1 and Ang-2 levels were positively correlated with ROP severity, with late-stage (stage 2) ROP patients showing significantly higher levels of these factors.111 However, VEGF, Ang-1, and Ang-2 levels in tears alone are not reliable biomarkers for assessing ROP severity or treatment needs.111
Additionally, studies have shown an upregulation of numerous inflammatory factors in tears, such as CCL2, RANTES-CCL5, and IL-8. Vinekar et al detected higher levels of RANTES-CCL5 and IL-8, along with lower levels of IL-6 and sL-selectin, in the tears of infants with ROP, though MCP1-CCL2 levels remained unchanged.149 Baba et al found significantly elevated CCL2 levels in the tears of severe ROP patients, suggesting that tear CCL2 could serve as a useful biomarker for assessing ROP severity.150 CCL2, a chemokine involved in monocyte and macrophage recruitment to inflammation sites, plays a role in the pathogenesis of various retinal vascular proliferative diseases.151
Tear protein concentrations are relatively high and can be easily obtained through minimally invasive methods.152 Tear proteomics has identified potential biomarkers for other ocular diseases, including growth factors and VEGF,153–155 with functions spanning angiogenesis, immune or inflammatory responses, visual perception, and metabolism.152 Shipton and others validated the feasibility of using tear proteins to assess ROP risk, finding an increase in LDH-B chains in infants at higher risk for ROP and a rise in immunoglobulin concentrations with postmenstrual and postnatal age.10 Rathi and Patnaik further found that MMP2 and MMP-9 expression was significantly higher in the tears of severe ROP patients compared to those with mild ROP or without the disease.3,59 These findings highlight the potential of tear MMPs as early predictive biomarkers for ROP, with MMP levels increasing with disease severity and showing no response to laser treatment, underscoring their diagnostic value.
Tear collection is relatively non-invasive and straightforward, most commonly done using sterile Schirmer strips (5 x 35 mm) to collect tears or conjunctival secretions. Other methods include glass capillaries, surgical sponges, glass rods and scrapers, and phenol red thread tear tests. Tears can be safely collected, reliably analyzed repeatedly, and associated with disease staging and progression, making them a valuable tool for predicting the onset and progression of ROP in preterm infants.
Comparison of Different Detection Methods and Factors
Comparison of Different Detection Methods
Research on ROP has revealed that various detection methods possess distinct advantages and disadvantages. The collection of vitreous and aqueous humor, while invasive and primarily used for laboratory research, offers a more direct insight into the retinal condition and aids in clarifying the pathogenesis of ROP. Sampling of amniotic fluid, umbilical cord blood, and placental tissue occurs relatively early, allowing for an assessment of the in utero environment, which can provide early predictions regarding the occurrence and progression of ROP. Peripheral blood and urine samples are easier to obtain; however, their collection typically occurs later and is susceptible to influence from a variety of systemic factors. Tears, on the other hand, can be collected safely at multiple time points, allowing for the dynamic monitoring of disease progression. This makes them an ideal source for identifying and validating molecular markers closely associated with ocular diseases, including ROP.156
Comparison of Different Detection Factors
VEGF has emerged as the most extensively studied and modifiable factor in ROP. The pathogenesis of ROP is divided into two phases: the first phase involves the downregulation of VEGF levels due to high environmental oxygen, which inhibits retinal vascular growth. The second phase is marked by accelerated retinal development and metabolism, leading to relative retinal hypoxia. This hypoxia stimulates increased VEGF production in the avascular retina, promoting extensive retinal neovascularization.20,157 Numerous studies have examined VEGF levels across various sample types in ROP patients, with most indicating elevated VEGF levels. Showing differences in severity in peripheral blood, ie, decreased VEGF in mild ROP patients and increased VEGF in severe ROP patients, consistent with the two development stages of ROP disease. Notably, VEGF levels in tears and urine are decreased in ROP patients. Lower tear VEGF levels may reflect systemic VEGF levels; Vinekar et al reported that infants with higher tear VEGF levels exhibited more systemic angiogenesis, likely as a response to prematurity-related inflammatory complications, independent of ROP status.148
Insulin-like growth factor-1 (IGF-1) is a critical peptide hormone with structural similarity to insulin, playing a fundamental role in fetal and neonatal growth and development.158 It promotes cell proliferation and differentiation, inhibits apoptosis, and has metabolic and immunomodulatory effects akin to insulin.159 IGF-1 is considered a positive regulator of VEGF, effectively facilitating retinal neovascularization.160 Recent studies have increasingly elucidated the relationship between IGF-1 and ROP, with multiple investigations into peripheral and umbilical cord blood suggesting that low IGF-1 levels are crucial in the onset and progression of ROP.
A wide range of inflammatory factors, including TNF-α, IL-6, IL-8, IL-18, IL-10, MCP-1, MIP-1α/β, and CCL2, have been found to be elevated in various sample types from ROP patients and are believed to interact synergistically with VEGF. TNF-α, a key cytokine in inflammation with paradoxical anti-inflammatory properties, has been shown to influence retinal angiogenesis. Its expression is upregulated in animal models of retinal neovascularization and human proliferative eye diseases.161 Blocking TNF-α can enhance physiological angiogenesis while reducing pathological neovascularization in mouse models of oxygen-induced retinopathy.53,54 IL-6, known to promote pathological angiogenesis, including retinal angiogenesis, increases in diabetic retinopathy.162–164 IL-8, another inflammatory cytokine, plays a crucial role in promoting angiogenesis and is elevated under conditions of retinal neovascularization.162,163,165 However, some studies report conflicting results or no significant differences for these inflammatory markers. Additionally, certain studies have detected immune cells (PBMCs), complement factors (C3, C4), and angiopoietins (Ang-1 and Ang-2) as contributors to the development and progression of ROP.
Furthermore, specific factors demonstrate unique expression patterns in particular samples. For instance, reduced TGFBI levels in umbilical cord blood proteins are significantly associated with severe ROP. Increased MMP levels in amniotic fluid and tears are identified as risk factors for the onset and independent risk factors for the progression of ROP. Elevated opticin levels in the vitreous have been shown to prevent retinal neovascularization. Additionally, Col1a1 and 16K-PRL are significantly upregulated in the aqueous humor of ROP patients. Placental function and inflammation also exhibit a complex association with ROP, and significant elevations in 8-OHdG and NTproBNP have been observed in the urine of ROP patients.
Common influencing factors and their related mechanisms are shown in Table 1. The detection results of different factors across various, and even identical, sample types are largely consistent, though some contradictory findings may be attributed to differences in the stage of ROP at the time of sampling, variations in corrected gestational age, and the overall condition of the patients. Further research is needed to examine related factors in the same or different sample types at consistent stages to enhance our understanding of ROP pathogenesis and to provide more effective recommendations for early prevention and treatment in clinical practice.
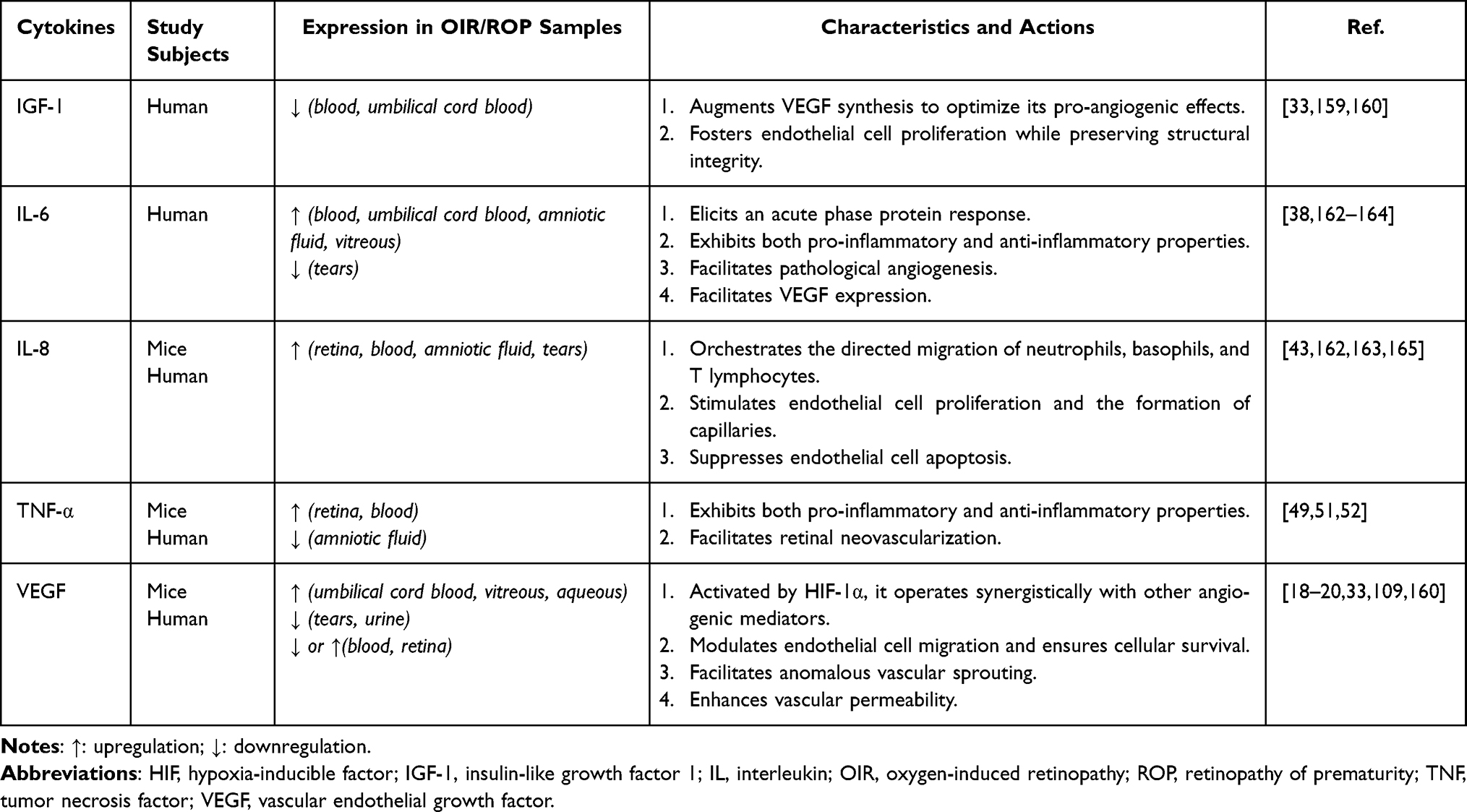 |
Table 1 Predominant Cytokines Implicated in Retinopathy of Prematurity and Their Mechanistic Roles |
Conclusion
Retinopathy of Prematurity (ROP), characterized by abnormal and uncontrolled vascular growth in the immature retina of preterm infants, remains a leading cause of potentially preventable blindness in children globally. Various detection methods for ROP, including peripheral blood, umbilical cord blood, amniotic fluid, placenta, vitreous humor, aqueous humor, urine, and tears, offer distinct advantages and limitations. Among these, the simplicity, safety, and speed of tear collection make it a particularly promising method for use in preterm infants. Tears can be safely and repeatedly collected, and they are associated with disease staging and progression. Previous studies have investigated relevant cytokines in the tears of premature infants with retinopathy, such as angiogenic factors (VEGF, Ang-1, and Ang-2), inflammatory factors (CCL2, RANTES-CCL5, IL-8), and MMPs (MMP-2 and MMP-9). It was found that the levels of MMPs (MMP-2 and MMP-9) increased with the severity of the disease. The establishment of tear protein expression profiles has also played a significant role in the study of ocular diseases, facilitating patient compliance and longitudinal monitoring. Identifying biomarkers that accurately predict the risk and severity of ROP is critical for many infants, their families, and the healthcare system. As neonatal medicine continues to evolve, the clinical and practical challenges associated with ROP are likely to grow, underscoring the need for further investigation into potential tear biomarkers for ROP. Such research could lead to more effective early detection and intervention strategies, ultimately reducing the incidence of ROP-related blindness.
Retinal vascular disorders such as Familial Exudative Vitreoretinopathy (FEVR), Incontinentia Pigmenti (IP), and Coats Disease severely impair infant vision by damaging retinal vasculature. Previous studies have identified disease-specific biomarkers, such as Okamoto et al166 reported that the combination of V-shaped vascular notch, brushy vascular ends, and csAR serves as a biomarker for autosomal dominant FEVR (AD-FEVR) patients with pathogenic variants in the Norrin/β-catenin genes. Woffendin et al167 demonstrated that marked skewing of X–inactivation patterns is a hallmark of IP. Zhang et al168 proposed angiogenin as a potential biomarker for retinal vascular abnormalities, with VEGF and MCP-1 concentrations positively correlating with the severity of retinal exudation. These disorders, along with Retinopathy of Prematurity (ROP), share common features of retinal vascular dysfunction. The biomarkers discussed in this study may provide a cross-disease reference framework for early prediction and severity assessment of such retinal vascular abnormalities.
Abbreviations
AMD, age-related macular degeneration; ANG, Angiopoietin; bFGF, basic fibroblast growth factor; BDNF, brain-derived neurotrophic factor; BIO, binocular indirect ophthalmoscopy; BRB, blood-retinal barrier; BW, birth weight; C5a, complement Component 5a; Col1a1, Collagen Type I Alpha 1 Chain; CRP, C-Reactive Protein; CXCR4, C-X-C Motif Chemokine Receptor 4; DED, dry eye disease; ECM, extracellular matrices; ELGAN, extremely low gestational age newborns; HA, hyaluronic acid; HCA, acute histological chorioamnionitis; IGF-1, insulin-like growth factor 1; IFN-γ, interferon-γ; IL, interleukin; IP, interferon-inducible protein; GA, gestational age; G-CSF, Granulocyte colony-stimulating factor; LMRGs, lactate metabolism-related genes; MCP, monocyte chemotactic protein; MIP, macrophage inflammatory protein; MMPs, matrix metalloproteinases; MPO, Myeloperoxidase; NTproBNP, N-terminal pro B-type natriuretic peptide; 8-OHdG, 8-hydroxy-2ʹ-deoxyguanosine; OIR, oxygen-induced retinopathy; PBMCs, peripheral blood mononuclear cells; PRL, prolactin; RANTES (CCL5), C-C Motif Chemokine Ligand 5; ROP, retinopathy of prematurity; SAA, Serum Amyloid A; TGF, transforming growth factor; TNF, tumor necrosis factor; tRFs, transfer RNA-derived fragments; UNBCR, creatinine ratio; VEGF, vascular endothelial growth factor.
Acknowledgment
We sincerely appreciated the guidance from our tutors and every member in our team.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was supported by grants from the National Natural Science Foundation of China (82160203).
Disclosure
The authors declare that they have no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Kim SJ, Port AD, Swan R, et al. Retinopathy of prematurity: a review of risk factors and their clinical significance. Surv Ophthalmol. 2018;63(5):618–637. doi:10.1016/j.survophthal.2018.04.002
2. Giusti B, Vestrini A, Poggi C, et al. Genetic polymorphisms of antioxidant enzymes as risk factors for oxidative stress-associated complications in preterm infants. Free Radic Res. 2012;46(9):1130–1139. doi:10.3109/10715762.2012.692787
3. Patnaik S, Rai M, Jalali S, et al. An interplay of microglia and matrix metalloproteinase MMP9 under hypoxic stress regulates the opticin expression in retina. Sci Rep. 2021;11(1):7444. doi:10.1038/s41598-021-86302-2
4. Sen P, Wu WC, Chandra P, et al. Retinopathy of prematurity treatment: Asian perspectives. Eye. 2020;34(4):632–642. doi:10.1038/s41433-019-0643-4
5. Dammann O, Hartnett ME, Stahl A. Retinopathy of prematurity. Dev Med Child Neurol. 2023;65(5):625–631. doi:10.1111/dmcn.15468
6. Hartnett ME, Penn JS. Mechanisms and management of retinopathy of prematurity. N Engl J Med. 2012;367(26):2515–2526. doi:10.1056/NEJMra1208129
7. Wu C, Petersen RA, VanderVeen DK. RetCam imaging for retinopathy of prematurity screening. J Aapos. 2006;10(2):107–111. doi:10.1016/j.jaapos.2005.11.019
8. Yonekawa Y, Thomas BJ, Thanos A, et al. The cutting edge of retinopathy of prematurity care: expanding the boundaries of diagnosis and treatment. Retina. 2017;37(12):2208–2225. doi:10.1097/iae.0000000000001719
9. Mitchell AJ, Green A, Jeffs DA, Roberson PK. Physiologic effects of retinopathy of prematurity screening examinations. Adv Neonatal Care. 2011;11(4):291–297. doi:10.1097/ANC.0b013e318225a332
10. Shipton C, Aitken J, Atkinson S, et al. Tear proteomics in infants at risk of retinopathy of prematurity: a feasibility study. Transl Vis Sci Technol. 2024;13(5):1. doi:10.1167/tvst.13.5.1
11. Chawla D, Deorari A. Retinopathy of prematurity prevention, screening and treatment programmes: progress in India. Semin Perinatol. 2019;43(6):344–347. doi:10.1053/j.semperi.2019.05.006
12. Yu TY, Donovan T, Armfield N, Gole GA. Retinopathy of prematurity: the high cost of screening regional and remote infants. Clin Exp Ophthalmol. 2018;46(6):645–651. doi:10.1111/ceo.13160
13. Quinn GE, Vinekar A. The role of retinal photography and telemedicine in ROP screening. Semin Perinatol. 2019;43(6):367–374. doi:10.1053/j.semperi.2019.05.010
14. Bai A, Dai S, Hung J, et al. Multicenter validation of deep learning algorithm ROP.AI for the automated diagnosis of plus disease in ROP. Transl Vis Sci Technol. 2023;12(8):13. doi:10.1167/tvst.12.8.13
15. Tan W, Li B, Wang Z, et al. Novel potential biomarkers for retinopathy of prematurity. Front Med. 2022;9:840030. doi:10.3389/fmed.2022.840030
16. Owen LA, Zhang C, Shirer K, et al. Placental inflammation significantly correlates with reduced risk for retinopathy of prematurity. Am J Pathol. 2023;193(11):1776–1788. doi:10.1016/j.ajpath.2023.02.003
17. Villegas-Becerril E, González-Fernández R, Perula-Torres L, Gallardo-Galera JM. [IGF-I, VEGF and bFGF as predictive factors for the onset of retinopathy of prematurity (ROP)]. Arch Soc Esp Oftalmol. 2006;81(11):641–646. Interlingue. doi:10.4321/s0365-66912006001100005
18. Hartnett ME. Pathophysiology and mechanisms of severe retinopathy of prematurity. Ophthalmology. 2015;122(1):200–210. doi:10.1016/j.ophtha.2014.07.050
19. Wu WC, Lien R, Liao PJ, et al. Serum levels of vascular endothelial growth factor and related factors after intravitreous bevacizumab injection for retinopathy of prematurity. JAMA Ophthalmol. 2015;133(4):391–397. doi:10.1001/jamaophthalmol.2014.5373
20. Enríquez AB, Avery RL, Baumal CR. Update on anti-vascular endothelial growth factor safety for retinopathy of prematurity. Asia Pac J Ophthalmol. 2020;9(4):358–368. doi:10.1097/apo.0000000000000302
21. Le YZ. VEGF production and signaling in Müller glia are critical to modulating vascular function and neuronal integrity in diabetic retinopathy and hypoxic retinal vascular diseases. Vision Res. 2017;139:108–114. doi:10.1016/j.visres.2017.05.005
22. Young TL, Anthony DC, Pierce E, Foley E, Smith LE. Histopathology and vascular endothelial growth factor in untreated and diode laser-treated retinopathy of prematurity. J Aapos. 1997;1(2):105–110. doi:10.1016/s1091-8531(97)90008-2
23. Hellgren G, Lundgren P, Pivodic A, et al. Decreased platelet counts and serum levels of VEGF-A, PDGF-BB, and BDNF in extremely preterm infants developing severe ROP. Neonatology. 2021;118(1):18–27. doi:10.1159/000512282
24. Yenice O, Cerman E, Ashour A, et al. Serum erythropoietin, insulin-like growth factor 1, and vascular endothelial growth factor in etiopathogenesis of retinopathy of prematurity. Ophthalmic Surg Lasers Imaging Retina. 2013;44(6):549–554. doi:10.3928/23258160-20131105-05
25. Pieh C, Agostini H, Buschbeck C, et al. VEGF-A, VEGFR-1, VEGFR-2 and Tie2 levels in plasma of premature infants: relationship to retinopathy of prematurity. Br J Ophthalmol. 2008;92(5):689–693. doi:10.1136/bjo.2007.128371
26. Yalin Imamoglu E, Gunay M, Gursoy T, et al. Effect of laser photocoagulation on plasma levels of VEGF-A, VEGFR-2, and Tie2 in infants with retinopathy of prematurity. J Aapos. 2014;18(5):466–470. doi:10.1016/j.jaapos.2014.07.159
27. Alon T, Hemo I, Itin A, et al. Vascular endothelial growth factor acts as a survival factor for newly formed retinal vessels and has implications for retinopathy of prematurity. Nat Med. 1995;1(10):1024–1028. doi:10.1038/nm1095-1024
28. Pierce EA, Foley ED, Smith LE. Regulation of vascular endothelial growth factor by oxygen in a model of retinopathy of prematurity. Arch Ophthalmol. 1996;114(10):1219–1228. doi:10.1001/archopht.1996.01100140419009
29. Zhao M, Shi X, Liang J, et al. Expression of pro- and anti-angiogenic isoforms of VEGF in the mouse model of oxygen-induced retinopathy. Exp Eye Res. 2011;93(6):921–926. doi:10.1016/j.exer.2011.10.013
30. Hellström A, Carlsson B, Niklasson A, et al. IGF-I is critical for normal vascularization of the human retina. J Clin Endocrinol Metab. 2002;87(7):3413–3416. doi:10.1210/jcem.87.7.8629
31. Hellström A, Ley D, Hansen-Pupp I, et al. Insulin-like growth factor 1 has multisystem effects on foetal and preterm infant development. Acta Paediatr. 2016;105(6):576–586. doi:10.1111/apa.13350
32. Liegl R, Löfqvist C, Hellström A, Smith LE. IGF-1 in retinopathy of prematurity, a CNS neurovascular disease. Early Hum Dev. 2016;102:13–19. doi:10.1016/j.earlhumdev.2016.09.008
33. Bach LA. Endothelial cells and the IGF system. J Mol Endocrinol. 2015;54(1):R1–13. doi:10.1530/jme-14-0215
34. Hellgren G, Löfqvist C, Hansen-Pupp I, et al. Increased postnatal concentrations of pro-inflammatory cytokines are associated with reduced IGF-I levels and retinopathy of prematurity. Growth Horm IGF Res. 2018;39:19–24. doi:10.1016/j.ghir.2017.11.006
35. Cakir U, Tayman C, Yucel C, Ozdemir O. Can IL-33 and endocan be new markers for retinopathy of prematurity? Comb Chem High Throughput Screen. 2019;22(1):41–48. doi:10.2174/1386207322666190325120244
36. Jensen AK, Ying GS, Huang J, Quinn GE, Binenbaum G. Postnatal serum insulin-like growth factor I and retinopathy of prematurity. Retina. 2017;37(5):867–872. doi:10.1097/iae.0000000000001247
37. Hellstrom A, Perruzzi C, Ju M, et al. Low IGF-I suppresses VEGF-survival signaling in retinal endothelial cells: direct correlation with clinical retinopathy of prematurity. Proc Natl Acad Sci U S A. 2001;98(10):5804–5808. doi:10.1073/pnas.101113998
38. Opal SM, DePalo VA. Anti-inflammatory cytokines. Chest. 2000;117(4):1162–1172. doi:10.1378/chest.117.4.1162
39. Cohen T, Nahari D, Cerem LW, Neufeld G, Levi BZ. Interleukin 6 induces the expression of vascular endothelial growth factor. J Biol Chem. 1996;271(2):736–741. doi:10.1074/jbc.271.2.736
40. Sood BG, Madan A, Saha S, et al. Perinatal systemic inflammatory response syndrome and retinopathy of prematurity. Pediatr Res. 2010;67(4):394–400. doi:10.1203/PDR.0b013e3181d01a36
41. Song JS, Woo SJ, Park KH, et al. Association of inflammatory and angiogenic biomarkers in maternal plasma with retinopathy of prematurity in preterm infants. Eye. 2023;37(9):1802–1809. doi:10.1038/s41433-022-02234-9
42. Silveira RC, Fortes Filho JB, Procianoy RS. Assessment of the contribution of cytokine plasma levels to detect retinopathy of prematurity in very low birth weight infants. Invest Ophthalmol Vis Sci. 2011;52(3):1297–1301. doi:10.1167/iovs.10-6279
43. Ghasemi H, Ghazanfari T, Yaraee R, Faghihzadeh S, Hassan ZM. Roles of IL-8 in ocular inflammations: a review. Ocul Immunol Inflamm. 2011;19(6):401–412. doi:10.3109/09273948.2011.618902
44. Holm M, Morken TS, Fichorova RN, et al. Systemic inflammation-associated proteins and retinopathy of prematurity in infants born before the 28th week of gestation. Invest Ophthalmol Vis Sci. 2017;58(14):6419–6428. doi:10.1167/iovs.17-21931
45. Sehgal P, Narang S, Chawla D, et al. Systemic biomarkers of retinopathy of prematurity in preterm babies. Int Ophthalmol. 2023;43(5):1751–1759. doi:10.1007/s10792-022-02576-z
46. Powers MR, Davies MH, Eubanks JP. Increased expression of chemokine KC, an interleukin-8 homologue, in a model of oxygen-induced retinopathy. Curr Eye Res. 2005;30(4):299–307. doi:10.1080/02713680590923276
47. Qiao H, Sonoda KH, Ikeda Y, et al. Interleukin-18 regulates pathological intraocular neovascularization. J Leukoc Biol. 2007;81(4):1012–1021. doi:10.1189/jlb.0506342
48. Daruich A, Bremond-Gignac D, Behar-Cohen F, Kermorvant E. Retinopathy of prematurity: from prevention to treatment. Med Sci. 2020;36(10):900–907. doi:10.1051/medsci/2020163
49. Pfeffer K. Biological functions of tumor necrosis factor cytokines and their receptors. Cytokine Growth Factor Rev. 2003;14(3–4):185–191. doi:10.1016/s1359-6101(03)00022-4
50. Yoshida S, Yoshida A, Ishibashi T. Induction of IL-8, MCP-1, and bFGF by TNF-alpha in retinal glial cells: implications for retinal neovascularization during post-ischemic inflammation. Graefes Arch Clin Exp Ophthalmol. 2004;242(5):409–413. doi:10.1007/s00417-004-0874-2
51. Sivakumar V, Foulds WS, Luu CD, Ling EA, Kaur C. Retinal ganglion cell death is induced by microglia derived pro-inflammatory cytokines in the hypoxic neonatal retina. J Pathol. 2011;224(2):245–260. doi:10.1002/path.2858
52. Luna JD, Chan CC, Derevjanik NL, et al. Blood-retinal barrier (BRB) breakdown in experimental autoimmune uveoretinitis: comparison with vascular endothelial growth factor, tumor necrosis factor alpha, and interleukin-1beta-mediated breakdown. J Neurosci Res. 1997;49(3):268–280. doi:10.1002/(sici)1097-4547(19970801)49:3<268::aid-jnr2>3.0.co;2-a
53. Gardiner TA, Gibson DS, de Gooyer TE, et al. Inhibition of tumor necrosis factor-alpha improves physiological angiogenesis and reduces pathological neovascularization in ischemic retinopathy. Am J Pathol. 2005;166(2):637–644. doi:10.1016/s0002-9440(10)62284-5
54. Connor KM, SanGiovanni JP, Lofqvist C, et al. Increased dietary intake of omega-3-polyunsaturated fatty acids reduces pathological retinal angiogenesis. Nat Med. 2007;13(7):868–873. doi:10.1038/nm1591
55. Sen P, Kemppainen E, Orešič M. Perspectives on systems modeling of human peripheral blood mononuclear cells. Front Mol Biosci. 2017;4:96. doi:10.3389/fmolb.2017.00096
56. Kurtul BE, Kabatas EU, Zenciroglu A, et al. Serum neutrophil-to-lymphocyte ratio in retinopathy of prematurity. J Aapos. 2015;19(4):327–331. doi:10.1016/j.jaapos.2015.04.008
57. Zhou Y, Wang Z, Zhou H, et al. Identification and clinical significance of tsRNAs and miRNAs in PBMCs of treatment-requiring retinopathy of prematurity. Exp Eye Res. 2023;232:109518. doi:10.1016/j.exer.2023.109518
58. Li Y, Zhou H, Huang Q, et al. Potential biomarkers for retinopathy of prematurity identified by circular RNA profiling in peripheral blood mononuclear cells. Front Immunol. 2022;13:953812. doi:10.3389/fimmu.2022.953812
59. Rathi S, Jalali S, Patnaik S, et al. Abnormal complement activation and inflammation in the pathogenesis of retinopathy of prematurity. Front Immunol. 2017;8:1868. doi:10.3389/fimmu.2017.01868
60. Fevereiro-Martins M, Guimarães H, Marques-Neves C, Bicho M. Retinopathy of prematurity: contribution of inflammatory and genetic factors. Mol Cell Biochem. 2022;477(6):1739–1763. doi:10.1007/s11010-022-04394-4
61. Xu J, Zhang Y, Gan R, Liu Z, Deng Y. Identification and validation of lactate metabolism-related genes in oxygen-induced retinopathy. Sci Rep. 2023;13(1):13319. doi:10.1038/s41598-023-40492-z
62. Cekmez F, Pirgon O, Aydemir G, et al. Correlation between cord blood apelin and IGF-1 levels in retinopathy of prematurity. Biomarker Med. 2012;6(6):821–825. doi:10.2217/bmm.12.82
63. Nagano N, Katayama D, Hara K, et al. Association of umbilical cord insulin-like growth factor 1 levels with severe retinopathy in extremely preterm infants. Pediatr Neonatol. 2023;64(2):126–132. doi:10.1016/j.pedneo.2022.05.015
64. Cox CM, D’Agostino SL, Miller MK, Heimark RL, Krieg PA. Apelin, the ligand for the endothelial G-protein-coupled receptor, APJ, is a potent angiogenic factor required for normal vascular development of the frog embryo. Dev Biol. 2006;296(1):177–189. doi:10.1016/j.ydbio.2006.04.452
65. Cleaver O, Tonissen KF, Saha MS, Krieg PA. Neovascularization of the Xenopus embryo. Dev Dyn. 1997;210(1):66–77. doi:10.1002/(sici)1097-0177(199709)210:1<66::Aid-aja7>3.0.Co;2-#
66. Kasai A, Shintani N, Oda M, et al. Apelin is a novel angiogenic factor in retinal endothelial cells. Biochem Biophys Res Commun. 2004;325(2):395–400. doi:10.1016/j.bbrc.2004.10.042
67. Yu H, Yuan L, Zou Y, et al. Serum concentrations of cytokines in infants with retinopathy of prematurity. Apmis. 2014;122(9):818–823. doi:10.1111/apm.12223
68. Park YJ, Woo SJ, Kim YM, et al. Immune and inflammatory proteins in cord blood as predictive biomarkers of retinopathy of prematurity in preterm infants. Invest Ophthalmol Vis Sci. 2019;60(12):3813–3820. doi:10.1167/iovs.19-27258
69. Thapa N, Lee BH, Kim IS. TGFBIp/betaig-h3 protein: a versatile matrix molecule induced by TGF-beta. Int J Biochem Cell Biol. 2007;39(12):2183–2194. doi:10.1016/j.biocel.2007.06.004
70. Song JS, Woo SJ, Park KH, et al. Cord blood transforming growth factor-β-induced as predictive biomarker of retinopathy of prematurity in preterm infants. Graefes Arch Clin Exp Ophthalmol. 2023;261(9):2477–2488. doi:10.1007/s00417-023-06056-7
71. Madan A, El-Ferzli G, Carlson SM, et al. A potential biomarker in the cord blood of preterm infants who develop retinopathy of prematurity. Pediatr Res. 2007;61(2):215–221. doi:10.1203/pdr.0b013e31802d776d
72. Hoenders HJ, Bloemendal H. Lens proteins and aging. J Gerontol. 1983;38(3):278–286. doi:10.1093/geronj/38.3.278
73. Takemoto L, Emmons T, Granstrom D. The sequences of two peptides from cataract lenses suggest they arise by deamidation. Curr Eye Res. 1990;9(8):793–797. doi:10.3109/02713689008999575
74. Woo SJ, Park JY, Hong S, et al. Inflammatory and angiogenic mediators in amniotic fluid are associated with the development of retinopathy of prematurity in preterm infants. Invest Ophthalmol Vis Sci. 2020;61(5):42. doi:10.1167/iovs.61.5.42
75. Bach LA. IGF-binding proteins. J Mol Endocrinol. 2018;61(1):T11–t28. doi:10.1530/jme-17-0254
76. Jang JH, Kim JG, Lee YH, Bae JG, Park JH. The association between amniotic fluid-derived inflammatory mediators and the risk of retinopathy of prematurity. Medicine. 2022;101(27):e29368. doi:10.1097/md.0000000000029368
77. Lorenc VE, Subirada Caldarone PV, Paz MC, et al. IGF-1R regulates the extracellular level of active MMP-2, pathological neovascularization, and functionality in retinas of OIR mouse model. Mol Neurobiol. 2018;55(2):1123–1135. doi:10.1007/s12035-017-0386-9
78. Kowluru RA, Mishra M. Regulation of matrix metalloproteinase in the pathogenesis of diabetic retinopathy. Prog Mol Biol Transl Sci. 2017;148:67–85. doi:10.1016/bs.pmbts.2017.02.004
79. Brett KE, Ferraro ZM, Yockell-Lelievre J, Gruslin A, Adamo KB. Maternal-fetal nutrient transport in pregnancy pathologies: the role of the placenta. Int J Mol Sci. 2014;15(9):16153–16185. doi:10.3390/ijms150916153
80. Çakir U, Yildiz D, Kahvecioğlu D, et al. Placenta, secret witness of infant morbidities: the relationship between placental histology and outcome of the premature infant. Turk Patoloji Derg. 2019;35(1):28–35. doi:10.5146/tjpath.2018.01443
81. Mehta R, Nanjundaswamy S, Shen-Schwarz S, Petrova A. Neonatal morbidity and placental pathology. Indian J Pediatr. 2006;73(1):25–28. doi:10.1007/bf02758255
82. Mestan KK, Check J, Minturn L, et al. Placental pathologic changes of maternal vascular underperfusion in bronchopulmonary dysplasia and pulmonary hypertension. Placenta. 2014;35(8):570–574. doi:10.1016/j.placenta.2014.05.003
83. Redline RW. Severe fetal placental vascular lesions in term infants with neurologic impairment. Am J Obstet Gynecol. 2005;192(2):452–457. doi:10.1016/j.ajog.2004.07.030
84. Nosarti C, Reichenberg A, Murray RM, et al. Preterm birth and psychiatric disorders in young adult life. Arch Gen Psychiatry. 2012;69(6):E1–8. doi:10.1001/archgenpsychiatry.2011.1374
85. Tomlinson MS, Santos HP, Stewart JR, et al. Neurocognitive and social-communicative function of children born very preterm at 10 years of age: associations with microorganisms recovered from the placenta parenchyma. J Perinatol. 2020;40(2):306–315. doi:10.1038/s41372-019-0505-8
86. Budal EB, Ebbing C, Kessler J, et al. Placental histology predicted adverse outcomes in extremely premature neonates in Norway-population-based study. Acta Paediatr. 2022;111(3):546–553. doi:10.1111/apa.16198
87. Leviton A, Allred EN, Fichorova RN, et al. Early postnatal IGF-1 and IGFBP-1 blood levels in extremely preterm infants: relationships with indicators of placental insufficiency and with systemic inflammation. Am J Perinatol. 2019;36(14):1442–1452. doi:10.1055/s-0038-1677472
88. Chen ML, Allred EN, Hecht JL, et al. Placenta microbiology and histology and the risk for severe retinopathy of prematurity. Invest Ophthalmol Vis Sci. 2011;52(10):7052–7058. doi:10.1167/iovs.11-7380
89. Sato M, Nishimaki S, Yokota S, et al. Severity of chorioamnionitis and neonatal outcome. J Obstet Gynaecol Res. 2011;37(10):1313–1319. doi:10.1111/j.1447-0756.2010.01519.x
90. Ogunyemi D, Murillo M, Jackson U, Hunter N, Alperson B. The relationship between placental histopathology findings and perinatal outcome in preterm infants. J Matern Fetal Neonatal Med. 2003;13(2):102–109. doi:10.1080/jmf.13.2.102.109
91. Moscuzza F, Belcari F, Nardini V, et al. Correlation between placental histopathology and fetal/neonatal outcome: chorioamnionitis and funisitis are associated to intraventricular haemorrage and retinopathy of prematurity in preterm newborns. Gynecol Endocrinol. 2011;27(5):319–323. doi:10.3109/09513590.2010.487619
92. Polam S, Koons A, Anwar M, Shen-Schwarz S, Hegyi T. Effect of chorioamnionitis on neurodevelopmental outcome in preterm infants. Arch Pediatr Adolesc Med. 2005;159(11):1032–1035. doi:10.1001/archpedi.159.11.1032
93. Lau J, Magee F, Qiu Z, et al. Chorioamnionitis with a fetal inflammatory response is associated with higher neonatal mortality, morbidity, and resource use than chorioamnionitis displaying a maternal inflammatory response only. Am J Obstet Gynecol. 2005;193(3 Pt 1):708–713. doi:10.1016/j.ajog.2005.01.017
94. Woo SJ, Park KH, Jung HJ, et al. Effects of maternal and placental inflammation on retinopathy of prematurity. Graefes Arch Clin Exp Ophthalmol. 2012;250(6):915–923. doi:10.1007/s00417-011-1648-2
95. Mitra S, Aune D, Speer CP, Saugstad OD. Chorioamnionitis as a risk factor for retinopathy of prematurity: a systematic review and meta-analysis. Neonatology. 2014;105(3):189–199. doi:10.1159/000357556
96. Owen LA, Morrison MA, Hoffman RO, Yoder BA, DeAngelis MM. Retinopathy of prematurity: a comprehensive risk analysis for prevention and prediction of disease. PLoS One. 2017;12(2):e0171467. doi:10.1371/journal.pone.0171467
97. Park JY, Park CW, Moon KC, et al. Retinopathy of prematurity in infants without fetal growth restriction is decreased with the progression of acute histologic chorioamnionitis: new observation as a protective factor against retinopathy of prematurity. Placenta. 2021;104:161–167. doi:10.1016/j.placenta.2020.12.007
98. Bulka CM, Dammann O, Santos HP, et al. Placental CpG methylation of inflammation, angiogenic, and neurotrophic genes and retinopathy of prematurity. Invest Ophthalmol Vis Sci. 2019;60(8):2888–2894. doi:10.1167/iovs.18-26466
99. Deev LA, Nivenitsyn EL, Novikov IA, et al. Nitrogen and oxygen levels in placenta - a predictor for retinopathy of prematurity. Vestn Oftalmol. 2019;135(6):33–41. doi:10.17116/oftalma201913506133
100. Carré C, Acar N, Daruich A, et al. Study protocol of OmegaROP-2 prospective study: expression of placental fatty acid receptors in preterm newborns with retinopathy of prematurity. BMC Ophthalmol. 2023;23(1):404. doi:10.1186/s12886-023-03156-0
101. SanGiovanni JP, Chew EY, Agrón E, et al. The relationship of dietary omega-3 long-chain polyunsaturated fatty acid intake with incident age-related macular degeneration: AREDS report no. 23. Arch Ophthalmol. 2008;126(9):1274–1279. doi:10.1001/archopht.126.9.1274
102. Phillips JD, Hwang ES, Morgan DJ, Creveling CJ, Coats B. Structure and mechanics of the vitreoretinal interface. J Mech Behav Biomed Mater. 2022;134:105399. doi:10.1016/j.jmbbm.2022.105399
103. Bishop P. The biochemical structure of mammalian vitreous. Eye. 1996;10(Pt 6):664–670. doi:10.1038/eye.1996.159
104. Crane IJ, Liversidge J. Mechanisms of leukocyte migration across the blood-retina barrier. Semin Immunopathol. 2008;30(2):165–177. doi:10.1007/s00281-008-0106-7
105. Nath M, Chandra P, Halder N, et al. Involvement of renin-angiotensin system in retinopathy of prematurity - a possible target for therapeutic intervention. PLoS One. 2016;11(12):e0168809. doi:10.1371/journal.pone.0168809
106. Zhao M, Xie WK, Bai YJ, et al. Expression of total vascular endothelial growth factor and the anti-angiogenic VEGF 165 b isoform in the vitreous of patients with retinopathy of prematurity. Chin Med J. 2015;128(18):2505–2509. doi:10.4103/0366-6999.164937
107. Velez-Montoya R, Clapp C, Rivera JC, et al. Intraocular and systemic levels of vascular endothelial growth factor in advanced cases of retinopathy of prematurity. Clin Ophthalmol. 2010;4:947–953. doi:10.2147/opth.s11650
108. Sato T, Kusaka S, Shimojo H, Fujikado T. Vitreous levels of erythropoietin and vascular endothelial growth factor in eyes with retinopathy of prematurity. Ophthalmology. 2009;116(9):1599–1603. doi:10.1016/j.ophtha.2008.12.023
109. Sato T, Shima C, Kusaka S. Vitreous levels of angiopoietin-1 and angiopoietin-2 in eyes with retinopathy of prematurity. Am J Ophthalmol. 2011;151(2):353–357.e351. doi:10.1016/j.ajo.2010.08.037
110. Sugioka K, Saito A, Kusaka S, Kuniyoshi K, Shimomura Y. Identification of vitreous proteins in retinopathy of prematurity. Biochem Biophys Res Commun. 2017;488(3):483–488. doi:10.1016/j.bbrc.2017.05.067
111. Magnani JE, Omar M, Mercy P, et al. Quantitative analysis of tear angiogenic factors in retinopathy of prematurity: a pilot biomarker study. J Aapos. 2023;27(1):14.e11–14.e16. doi:10.1016/j.jaapos.2022.10.007
112. Mintz-Hittner HA, Kennedy KA, Chuang AZ. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. 2011;364(7):603–615. doi:10.1056/NEJMoa1007374
113. Stahl A, Lepore D, Fielder A, et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): an open-label randomised controlled trial. Lancet. 2019;394(10208):1551–1559. doi:10.1016/s0140-6736(19)31344-3
114. Wong RK, Hubschman S, Tsui I. Reactivation of retinopathy of prematurity after ranibizumab treatment. Retina. 2015;35(4):675–680. doi:10.1097/iae.0000000000000578
115. Araújo RS, Santos DF, Silva GA. The role of the retinal pigment epithelium and Müller cells secretome in neovascular retinal pathologies. Biochimie. 2018;155:104–108. doi:10.1016/j.biochi.2018.06.019
116. Arima M, Akiyama M, Fujiwara K, et al. Neurodevelopmental outcomes following intravitreal bevacizumab injection in Japanese preterm infants with type 1 retinopathy of prematurity. PLoS One. 2020;15(3):e0230678. doi:10.1371/journal.pone.0230678
117. Natarajan G, Shankaran S, Nolen TL, et al. Neurodevelopmental outcomes of preterm infants with retinopathy of prematurity by treatment. Pediatrics. 2019;144(2). doi:10.1542/peds.2018-3537
118. Morin J, Luu TM, Superstein R, et al. Neurodevelopmental Outcomes Following Bevacizumab Injections for Retinopathy of Prematurity. Pediatrics. 2016;137(4). doi:10.1542/peds.2015-3218
119. Toy BC, Schachar IH, Tan GS, Moshfeghi DM. Chronic vascular arrest as a predictor of bevacizumab treatment failure in retinopathy of prematurity. Ophthalmology. 2016;123(10):2166–2175. doi:10.1016/j.ophtha.2016.06.055
120. Sato T, Kusaka S, Shimojo H, Fujikado T. Simultaneous analyses of vitreous levels of 27 cytokines in eyes with retinopathy of prematurity. Ophthalmology. 2009;116(11):2165–2169. doi:10.1016/j.ophtha.2009.04.026
121. Wolach B, Dolfin T, Regev R, Gilboa S, Schlesinger M. The development of the complement system after 28 weeks’ gestation. Acta Paediatr. 1997;86(5):523–527. doi:10.1111/j.1651-2227.1997.tb08924.x
122. Grumach AS, Ceccon ME, Rutz R, Fertig A, Kirschfink M. Complement profile in neonates of different gestational ages. Scand J Immunol. 2014;79(4):276–281. doi:10.1111/sji.12154
123. Bleul CC, Farzan M, Choe H, et al. The lymphocyte chemoattractant SDF-1 is a ligand for LESTR/fusin and blocks HIV-1 entry. Nature. 1996;382(6594):829–833. doi:10.1038/382829a0
124. Unoki N, Murakami T, Nishijima K, et al. SDF-1/CXCR4 contributes to the activation of tip cells and microglia in retinal angiogenesis. Invest Ophthalmol Vis Sci. 2010;51(7):3362–3371. doi:10.1167/iovs.09-4978
125. Sarafidis K, Diamanti E, Taparkou A, et al. Plasma RANTES increase during the first month of life independently of the feeding mode. Eur J Pediatr. 2007;166(8):819–823. doi:10.1007/s00431-006-0329-3
126. Klaska IP, White A, Villacampa P, et al. Intravitreal administration of recombinant human opticin protects against hyperoxia-induced pre-retinal neovascularization. Exp Eye Res. 2022;215:108908. doi:10.1016/j.exer.2021.108908
127. Le Goff MM, Sutton MJ, Slevin M, et al. Opticin exerts its anti-angiogenic activity by regulating extracellular matrix adhesiveness. J Biol Chem. 2012;287(33):28027–28036. doi:10.1074/jbc.M111.331157
128. Nonobe NI, Kachi S, Kondo M, et al. Concentration of vascular endothelial growth factor in aqueous humor of eyes with advanced retinopathy of prematurity before and after intravitreal injection of bevacizumab. Retina. 2009;29(5):579–585. doi:10.1097/IAE.0b013e3181a3b848
129. Liang T, Qian Z, Tao Y, et al. The relationship between the aqueous VEGF level and the severity of type 1 retinopathy of prematurity. J Clin Med. 2022;11(18). doi:10.3390/jcm11185361
130. Lyu J, Zhang Q, Jin H, et al. Aqueous cytokine levels associated with severity of type 1 retinopathy of prematurity and treatment response to ranibizumab. Graefes Arch Clin Exp Ophthalmol. 2018;256(8):1469–1477. doi:10.1007/s00417-018-4034-5
131. Xia M, Jiao L, Wang XH, et al. Single-cell RNA sequencing reveals a unique pericyte type associated with capillary dysfunction. Theranostics. 2023;13(8):2515–2530. doi:10.7150/thno.83532
132. Jiang Q, Ma Y, Zhao Y, et al. tRNA-derived fragment tRF-1001: a novel anti-angiogenic factor in pathological ocular angiogenesis. Mol Ther Nucleic Acids. 2022;30:407–420. doi:10.1016/j.omtn.2022.10.016
133. Dueñas Z, Rivera JC, Quiróz-Mercado H, et al. Prolactin in eyes of patients with retinopathy of prematurity: implications for vascular regression. Invest Ophthalmol Vis Sci. 2004;45(7):2049–2055. doi:10.1167/iovs.03-1346
134. Levesque BM, Kalish LA, Winston AB, et al. Low urine vascular endothelial growth factor levels are associated with mechanical ventilation, bronchopulmonary dysplasia and retinopathy of prematurity. Neonatology. 2013;104(1):56–64. doi:10.1159/000351040
135. Kwinta P, Bik-Multanowski M, Mitkowska Z, Tomasik T, Pietrzyk JJ. The clinical role of vascular endothelial growth factor (VEGF) system in the pathogenesis of retinopathy of prematurity. Graefes Arch Clin Exp Ophthalmol. 2008;246(10):1467–1475. doi:10.1007/s00417-008-0865-9
136. Loft S, Fischer-Nielsen A, Jeding IB, Vistisen K, Poulsen HE. 8-Hydroxydeoxyguanosine as a urinary biomarker of oxidative DNA damage. J Toxicol Environ Health. 1993;40(2–3):391–404. doi:10.1080/15287399309531806
137. Ates O, Alp HH, Caner I, et al. Oxidative DNA damage in retinopathy of prematurity. Eur J Ophthalmol. 2009;19(1):80–85. doi:10.1177/112067210901900112
138. Sugimoto M, Manabe H, Nakau K, et al. The role of N-terminal pro-B-type natriuretic peptide in the diagnosis of congestive heart failure in children–correlation with the heart failure score and comparison with B-type natriuretic peptide. Circ J. 2010;74(5):998–1005. doi:10.1253/circj.cj-09-0535
139. Kulkarni M, Gokulakrishnan G, Price J, et al. Diagnosing significant PDA using natriuretic peptides in preterm neonates: a systematic review. Pediatrics. 2015;135(2):e510–525. doi:10.1542/peds.2014-1995
140. Bührer C, Erdeve Ö, van Kaam A, et al. N-terminal B-type natriuretic peptide urinary concentrations and retinopathy of prematurity. Pediatr Res. 2017;82(6):958–963. doi:10.1038/pr.2017.179
141. Czernik C, Metze B, Müller C, Müller B, Bührer C. Urinary N-terminal B-type natriuretic peptide predicts severe retinopathy of prematurity. Pediatrics. 2011;128(3):e545–549. doi:10.1542/peds.2011-0603
142. Aass C, Norheim I, Eriksen EF, Thorsby PM, Pepaj M. Single unit filter-aided method for fast proteomic analysis of tear fluid. Anal Biochem. 2015;480:1–5. doi:10.1016/j.ab.2015.04.002
143. Aluru SV, Agarwal S, Srinivasan B, et al. Lacrimal proline rich 4 (LPRR4) protein in the tear fluid is a potential biomarker of dry eye syndrome. PLoS One. 2012;7(12):e51979. doi:10.1371/journal.pone.0051979
144. Matheis N, Grus FH, Breitenfeld M, et al. Proteomics differentiate between thyroid-associated orbitopathy and dry eye syndrome. Invest Ophthalmol Vis Sci. 2015;56(4):2649–2656. doi:10.1167/iovs.15-16699
145. Torok Z, Peto T, Csosz E, et al. Tear fluid proteomics multimarkers for diabetic retinopathy screening. BMC Ophthalmol. 2013;13(1):40. doi:10.1186/1471-2415-13-40
146. Patnaik K, Pradeep AR, Nagpal K, et al. Human chemerin correlation in gingival crevicular fluid and tear fluid as markers of inflammation in chronic periodontitis and type-2 diabetes mellitus. J Investig Clin Dent. 2017;8(1). doi:10.1111/jicd.12181
147. Leonardi A, Palmigiano A, Mazzola EA, et al. Identification of human tear fluid biomarkers in vernal keratoconjunctivitis using iTRAQ quantitative proteomics. Allergy. 2014;69(2):254–260. doi:10.1111/all.12331
148. Vinekar A, Nair AP, Sinha S, et al. Tear fluid angiogenic factors: potential noninvasive biomarkers for retinopathy of prematurity screening in preterm infants. Invest Ophthalmol Vis Sci. 2021;62(3):2. doi:10.1167/iovs.62.3.2
149. Vinekar A, Nair AP, Sinha S, et al. Early detection and correlation of tear fluid inflammatory factors that influence angiogenesis in premature infants with and without retinopathy of prematurity. Indian J Ophthalmol. 2023;71(11):3465–3472. doi:10.4103/ijo.Ijo_3407_22
150. Baba T, Uotani R, Inata K, et al. Tear fluid cytokine analysis: a non-invasive approach for assessing retinopathy of prematurity severity. Jpn J Ophthalmol. 2024. doi:10.1007/s10384-024-01084-0
151. Baba T, Miyazaki D, Inata K, et al. Role of IL-4 in bone marrow driven dysregulated angiogenesis and age-related macular degeneration. Elife. 2020;9:e54257. doi:10.7554/eLife.54257
152. de Souza GA, Godoy LM, Mann M. Identification of 491 proteins in the tear fluid proteome reveals a large number of proteases and protease inhibitors. Genome Biol. 2006;7(8):R72. doi:10.1186/gb-2006-7-8-R72
153. Ihnatko R, Edén U, Lagali N, Dellby A, Fagerholm P. Analysis of protein composition and protein expression in the tear fluid of patients with congenital aniridia. J Proteomics. 2013;94:78–88. doi:10.1016/j.jprot.2013.09.003
154. Ang WJ, Zunaina E, Norfadzillah AJ, et al. Evaluation of vascular endothelial growth factor levels in tears and serum among diabetic patients. PLoS One. 2019;14(8):e0221481. doi:10.1371/journal.pone.0221481
155. Zhou L, Beuerman RW. The power of tears: how tear proteomics research could revolutionize the clinic. Expert Rev Proteomics. 2017;14(3):189–191. doi:10.1080/14789450.2017.1285703
156. Hagan S, Martin E, Enríquez-de-salamanca A. Tear fluid biomarkers in ocular and systemic disease: potential use for predictive, preventive and personalised medicine. EPMA J. 2016;7(1):15. doi:10.1186/s13167-016-0065-3
157. Dogra MR, Katoch D, Dogra M. An update on retinopathy of prematurity (ROP). Indian J Pediatr. 2017;84(12):930–936. doi:10.1007/s12098-017-2404-3
158. Takahashi Y. The role of growth hormone and insulin-like growth factor-I in the liver. Int J Mol Sci. 2017;18(7). doi:10.3390/ijms18071447
159. Nicholls AR, Holt RI. Growth hormone and insulin-like growth factor-1. Front Horm Res. 2016;47:101–114. doi:10.1159/000445173
160. Reddy MA, Patel HI, Karim SM, et al. Reduced utility of serum IGF-1 levels in predicting retinopathy of prematurity reflects maternal ethnicity. Br J Ophthalmol. 2016;100(4):501–504. doi:10.1136/bjophthalmol-2015-307234
161. Capitão M, Soares R. Angiogenesis and inflammation crosstalk in diabetic retinopathy. J Cell Biochem. 2016;117(11):2443–2453. doi:10.1002/jcb.25575
162. Minaker SA, Mason RH, Lahaie Luna G, et al. Changes in aqueous and vitreous inflammatory cytokine levels in diabetic macular oedema: a systematic review and meta-analysis. Acta Ophthalmol. 2022;100(1):e53–e70. doi:10.1111/aos.14891
163. Mason RH, Minaker SA, Lahaie Luna G, et al. Changes in aqueous and vitreous inflammatory cytokine levels in proliferative diabetic retinopathy: a systematic review and meta-analysis. Eye. 2022. doi:10.1038/s41433-022-02127-x
164. Rojas M, Zhang W, Lee DL, et al. Role of IL-6 in angiotensin II-induced retinal vascular inflammation. Invest Ophthalmol Vis Sci. 2010;51(3):1709–1718. doi:10.1167/iovs.09-3375
165. Heidemann J, Ogawa H, Dwinell MB, et al. Angiogenic effects of interleukin 8 (CXCL8) in human intestinal microvascular endothelial cells are mediated by CXCR2. J Biol Chem. 2003;278(10):8508–8515. doi:10.1074/jbc.M208231200
166. Okamoto M, Matsushita I, Nagata T, Fujino Y, Kondo H. Angiographic characteristics in mild familial exudative vitreoretinopathy with genetically confirmed autosomal dominant inheritance. Ophthalmol Retina. 2025;9(2):187–193. doi:10.1016/j.oret.2024.08.013
167. Woffendin H, Jakins T, Jouet M, et al. X-inactivation and marker studies in three families with incontinentia pigmenti: implications for counselling and gene localisation. Clin Genet. 1999;55(1):55–60. doi:10.1034/j.1399-0004.1999.550110.x
168. Zhang J, Jiang C, Ruan L, Huang X. Associations of cytokine concentrations in aqueous humour with retinal vascular abnormalities and exudation in Coats’ disease. Acta Ophthalmol. 2019;97(3):319–324. doi:10.1111/aos.13971
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
From COPD to Lung Cancer: Mechanisms Linking, Diagnosis, Treatment, and Prognosis

Qi C, Sun SW, Xiong XZ
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2603-2621
Published Date: 17 October 2022
CXCL12 and CXCR4 as Potential Early Biomarkers for Luminal A and Luminal B Subtypes of Breast Cancer
Motyka J, Gacuta E, Kicman A, Kulesza M, Malinowski P, Ławicki S
Cancer Management and Research 2023, 15:573-589
Published Date: 4 July 2023