")
Back to Journals » Advances in Medical Education and Practice » Volume 16
Teaching Neonatal Emergency Umbilical Venous Access to Untrained Medical Staff: A Pilot Study Using Video Instruction and Real Umbilical Cords
Authors Brickmann C , Zang FC, Klotz D, Kunze M, Hentschel R
Received 7 January 2025
Accepted for publication 29 March 2025
Published 17 May 2025 Volume 2025:16 Pages 801—809
DOI https://doi.org/10.2147/AMEP.S516071
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh B Arja
Newborn emergency umbilical venous access – Video abstract [516071]
Views: 80
Christian Brickmann,1,2 Fanny Carlotta Zang,3 Daniel Klotz,4 Mirjam Kunze,5 Roland Hentschel6
1Clinic for Neonatology, Muenchen Klinik, Munich, Germany; 2Department of Pediatrics, Kinderklinik München Schwabing, TUM University Hospital; Technical University of Munich, School of Medicine and Health, Munich, Germany; 3Department of Anesthesiology and Critical Care Medicine University of Freiburg, University Hospital Freiburg, University of Freiburg, Freiburg im Breisgau, Germany; 4Bethel Center for Pediatrics, Department of Neonatology and Pediatric Intensive Care Medicine, University Hospital OWL, University of Bielefeld, Bielefeld, Germany; 5Department of Obstetrics and Gynecology, Medical Center, University Hospital Freiburg, University of Freiburg, Freiburg im Breisgau, Germany; 6Division of Neonatology and Pediatric Intensive Care Medicine, Department of General Pediatrics, Medical Center, University Hospital Freiburg, University of Freiburg, Freiburg im Breisgau, Germany
Correspondence: Christian Brickmann, Clinic for Neonatology, Muenchen Klinik, Munich, Germany, Technical University of Munich, School of Medicine and Health, Department of Pediatrics, Kinderklinik München Schwabing, TUM University Hospital, Munich, Germany, Tel +49 89 6210 6318, Email [email protected]
Background: Establishing intravenous access in newborns in an emergency situation is a challenge even for well-trained neonatologists. As not all hospitals have a neonatology department, other specialists such as anaesthesiologists and obstetricians must also be able to quickly establishing venous access. Consequently, there is a need for teaching strategies that can be used for a large group of people.
Aim: To evaluate the applicability and the acceptance of a teaching method for umbilical venous access that can be implemented in hospitals with obstetric departments following the principles of simulation-based learning.
Methods: Single-center cross-over pilot-study with video-based teaching of medical students using a model with fresh umbilical cords. The volunteers performed three techniques: standard umbilical cord cut - umbilical button cannula (S-EUC), lateral incision - umbilical button cannula (L-EUC) and standard umbilical cord cut - umbilical catheter (S-UC). Participants’ acceptance of the teaching method was evaluated using Likert-scale.
Results: The video teaching was considered as easy to learn and understand for all three techniques. After practicing on the model, most participants believed that they could successfully apply at least one of the techniques if faced with a real emergency situation. Subjects were able to perform the techniques in similar timescales to those published in the literature for the standard technique (S-UC).
Conclusion: The teaching method combining video learning and practical training on real umbilical cords, is suitable for teaching venous access in newborns even for untrained personnel. The model can be replicated using materials every obstetrics department has at hand.
Plain Language Summary: This study was conducted to improve how medical staff learn to perform emergency procedures on newborns, specifically umbilical venous access. This procedure is crucial in emergencies but is rarely needed, making it hard to practice. The researchers wanted to create a teaching method that is easy to use and does not require a lot of resources. They used real umbilical cords to create a realistic training model and conducted explicit teaching videos for every technique. Medical students watched these instructional videos to learn the procedure. Students practiced the procedure using the model. The researchers found that the video teaching method was effective. Students felt prepared to handle real emergencies. One technique, called S-EUC, was the fastest and most successful. The teaching model and the video-based approach is cost-effective and can be used in hospitals with limited resources. These results mean that hospitals can adopt this teaching method to better prepare their staff for neonatal emergencies. The study suggests that using video instruction and real umbilical cords is a practical way to teach important medical skills. This approach could lead to faster and more successful emergency care for newborns.
Keywords: umbilical cord, medical teaching, video teaching, simulation-based teaching, umbilical vein, newborn resuscitation
Introduction
Teaching practical skills to medical staff is a challenge in today’s hospital environment due to staff shortages during ongoing hospital operations, high workloads and financial constraints. Emergency procedures, including advanced resuscitation, are infrequently required but rely heavily on the practitioner’s experience for success.1,2 This is especially true in neonatology, a field in which resuscitation is required in only 0.1 to 1% of births.3,4 Since not all hospitals have a specialized neonatology department, medical staff from the obstetric department and anaesthesiologists are more frequently affected by such situations than highly qualified neonatologists.5 Specific training can improve the quality of resuscitation in both high level (up to 30%) and low-level facilities (up to 20%).2 Therefore, the implementation of well-designed teaching and training models for neonatal emergencies is crucial.
One of the most challenging procedures in the delivery room is establishing access to the neonatal vascular system. Even well-trained neonatologists often face technical difficulties and require multiple attempts for this task.6 However, establishing venous access for the administration of drugs and fluids is a crucial step in neonatal emergencies. Current guidelines recommend umbilical venous catheterization (UVC) and intraosseous (IO) access, with UVC as the primary option and IO access as an alternative due to lack of data on the safety of IO access.7–9 However, simulation studies have implicated that the IO access can be placed faster than UVC access (52 sec (i.o) vs 134 sec (UVC), 45 vs 95 sec; 59 vs 105 sec; 86 vs 199 sec).10–12 In neonatal emergencies, physicians must choose the safest and quickest technique for venous access. It should also offer realistic training opportunities for ample preparedness.
Leaving the old mantra “see one, do one, teach one” behind, simulation-based learning has gained a prominent position in medical education over the last two decades.13,14 In its simplest form, it consists of a simulation in which participants perform a task on a model within a realistic, yet controlled environment. In this way, skills can be learned without jeopardizing patient safety.15–17 Simulation training can be integrated into an existing curriculum or delivered as a stand-alone unit with an associated theoretical unit. When teaching the positioning of UVCs, the theoretical knowledge can be taught through video sequences, which has proven to successfully enhance the skills of beginners and advanced practitioners in the past.18 Practical training can be carried out on commercially available plastic umbilical cords or on task trainers.19 However, the use of real umbilical cord specimens incorporated into models provides a more realistic training experience, as it is the actual organic material on which the emergency access techniques will later be applied.19
The aim of the study was to design a teaching and training model for umbilical venous access, based on the principles of simulation-based teaching. The field of neonatology is a perfect role model when considering the fact, that its contents are to be found in every part of the world, every kind of medical setting and accounts for a huge amount of possibly affected patients. It should be possible to implement it in almost any hospital using existing material with minimal personnel and financial effort. The main study hypothesis was that the training method would be evaluated positively by the participants, giving them the feeling of being well prepared for the task and the real emergency situation. We concluded that the training method and the video-based approach would adequately prepare unexperienced participants to apply a technique quickly, resulting in times to success comparable to those reported in existing literature for the standard procedure inserting the umbilical catheter through the standard umbilical cord cut (S-UC).10–12 Results concerning the time to successful cannulation have been published elsewhere.20 Mean time until successful vascular access was within the expected and hitherto known ranges for other kinds of emergency access in manikin studies. These results confirm that the video-teaching technique is able to match the standard teaching technique using a “bench-side” approach.
Materials and Methods
Setting and Subjects
A single-center, prospective, randomized, controlled study in a 3×3 cross-over design was conducted at the level III neonatal intensive care unit of the University Medical Center of Freiburg, Germany. 45 medical students from the third to tenth semester of the Medical Faculty of the University of Freiburg were enrolled between November 2019 and February 2020. None of the students had any previous practical experience in neonatology or obstetrics. Each participant had to agree to the potential biohazard of working with human tissue. Approval for the study was granted by the Ethics Committee of the University of Freiburg, Germany (No.10007/20). Registration was made with the German Clinical Trials Register, registration number DRKS00019197.
Simulation Models
Fresh umbilical cord specimens were anonymously collected by midwives in the delivery room directly after birth with parental consent. The umbilical cords were cleaned externally from blood and the umbilical vein was rinsed with saline fluid. The cords were then stored in a refrigerator at 7°C for up to 120 hours or frozen for a maximum of two weeks. To simulate the situation in the delivery room the specimens were divided in three equal parts and then each part was integrated into a true-to-life model. The umbilical cord was drawn through the extended opening of a baby bottle suction teat (NUK, Zeven, Germany, size one) and clamped on the placenta-side part. In order to imitate a blood-filled umbilical vein, they were filled with coloured aqua ad iniectabilia (BRAUN, Melsungen; Colour solution: RAL Diff-Quik Solution II, RAL Diagnostics, Martillac) and the umbilical cord was clamped. To create a scenery comparable to the situation in the delivery room, the cord specimen model was covered with an incised sterile single-use drapes (Figure 1). Each test was continuously observed by the instructor who did not intervene but was allowed to hold and “milk” the umbilical cord to improve venous filling, which is comparable to real-life situation, where a 2nd person is also needed to assist.
 |
Figure 1 Experimental Setup. (A) Umbilical cord after retrograde filling of the umbilical vein with dye. (B) Study equipment used in each of the three parts of the experiment: umbilical cord string, forceps (2x), scalpel, emergency button cannula and umbilical catheter (from left to right). (C) Final umbilical cord set-up. |
Randomization
The statistic department of the University of Freiburg recommended testing the 3 different techniques in varying order. The participants were randomized electronically to one of three groups, with only the first technique being varied. The subsequent order was kept to avoid potential carry-over effects. Group 1 started with “lateral incision - emergency button cannula” (L-EUC), followed by “standard umbilical cord cut - umbilical catheter” (S-UC) and finally “standard umbilical cord cut - emergency button cannula” (S-EUC); Group 2: S-EUC/L-EUC/S-UC; Group 3: S-UC/S-EUC/L-EUC.
Teaching
For each technique, a two-minute instructional video was created to explain the upcoming procedure and the equipment to be used. The equipment included: 1 surgical forceps, 1 anatomical forceps, 1 umbilical cord string, 1 scalpel size 11, 1 umbilical emergency button cannula (Meiser Medical GmbH, Neuenstein, Germany, Size 70 mm), 1 umbilical catheter (Vygon, Ecouen, France, Size 4 Fr; 20 cm), a 2-mL saline filled syringe (BRAUN, Melsungen, Germany). The videos show the execution of the respective technique from start to finish with additional explanations and instructions. The participants were consecutively tested in all 3 techniques. Directly before the respective technique to be tested the corresponding video was available for 10 minutes and could be watched on demand by the subjects.
Assessment of Satisfaction
A standardized questionnaire with 21 items, rated on a 1-5-point or a 1-4-point Likert-scale, was used to evaluate the subjects’ satisfaction with each of the three techniques as well as the with teaching method. A further question asked the participants about their pre-existing experience with the application of central and peripheral lines. The questions and the participants’ answers are shown in Table 1 and Table 2.
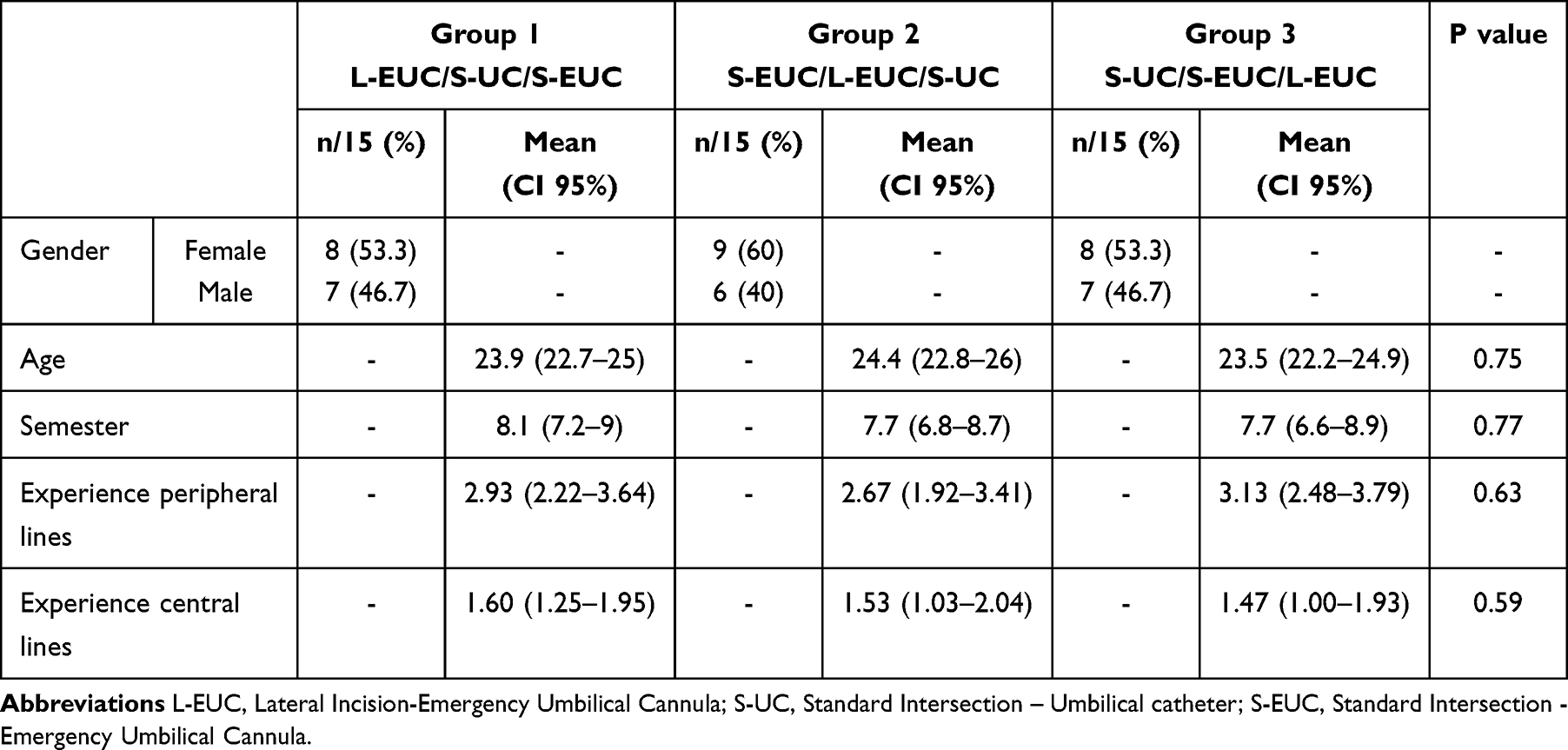 |
Table 1 Demographic data and already existing experience with handling of peripheral and central lines |
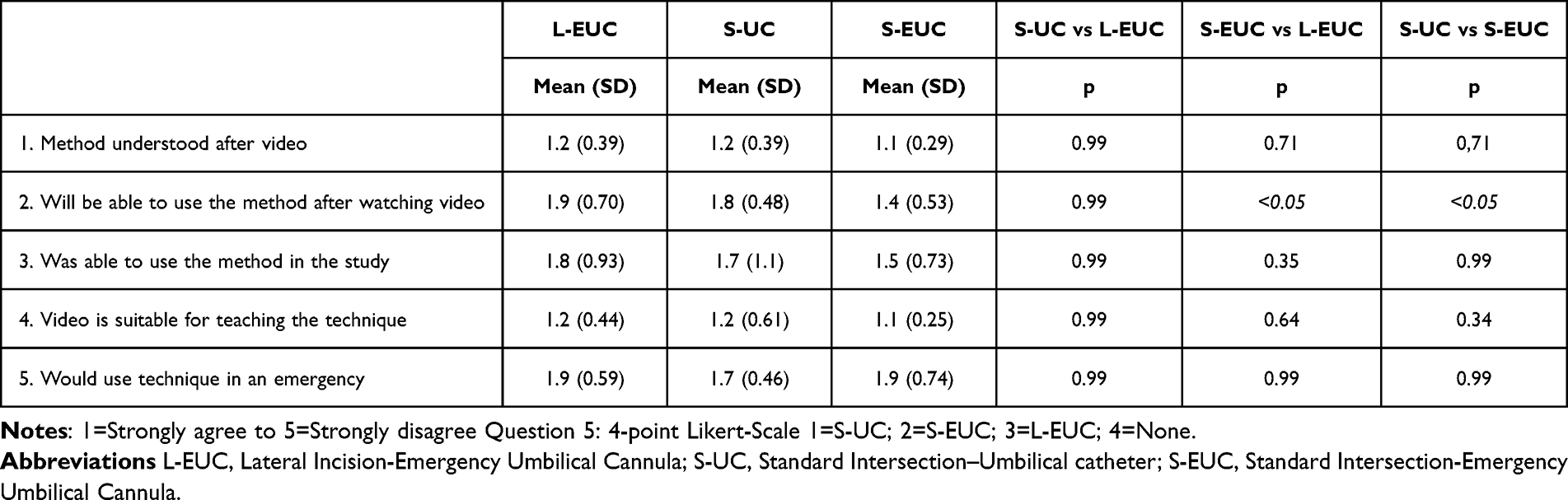 |
Table 2 Questions 1-4: Evaluation of teaching technique before (questions 1 and 2) and after (questions 3 and 4) the practical exercises with standardized questionnaire rated on a 5-point Likert-Scale |
Outcomes
The primary outcome was the effectiveness of the video teaching technique by measuring the duration in seconds to establish access to the umbilical vein, defined as the time from the first touching of the materials to aspiration of the coloured solution after successful insertion of the device to an insertion depth of 5 cm. Inability to gain intravenous access or a catheter misplacement in Wharton’s jelly outside the umbilical vein that could not be corrected were both rated as failures and recorded as a time duration of 300 seconds. Participants’ evaluation of the video-based teaching method was a secondary outcome.
Sample Size
The mean time to venous access was assumed to be 117 seconds,8 according to published data, giving a total sample size of 45 participants at a significance level of p<0.05 with a power of 80%.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism 10.02 and SPSS (V.24.0; IBM). A non-parametric Wilcoxon rank-sum test was used to analyse non-parametric data, the chi-squared test for contingency data and the Kruskal–Wallis test for comparison tests. A linear mixed-effects model as described by Senn was used to analyse positioning times in this three-group cross-over design, which can separate the (a) effect of time period (ie, whether the participant performs his or her first, second, or third technique) from (b) the effect of the group to which the participant belongs and from (c) the effect of the technique used.21 The results of this contrast analysis represent the number of seconds a participant needs to perform a specific technique within a certain period while belonging to a particular group. Subsequently, the effect of the different techniques on the expected outcome can be calculated allowing a statistically reliable conclusion to be made as to whether one technique is significantly superior to the others in terms of time. To compare the positioning times from this study with the times reported in the literature, the average time for each access method was also calculated. To analyse the influence of prior experience and education level in connection to performance, a linear regression analysis was performed, using the mean positioning times of the probands as the dependent variable. A two-tailed p-value of <0.05 was considered significant. Data are described using means and 95% confidence intervals.
Results
Randomized into 3 groups of 15 participants each, all 45 students completed the study. There were no significant statistical differences between the three groups in terms of education level, previous experience with peripheral and central line placement and gender distribution. The demographic data of the subjects are listed in Table 1.
Overall mean duration for the L-EUC technique until intravascular access was 89.3 sec (95% CI: 72.3–106.5 sec) while the failure rate was 4.4% (n=2). S-EUC was the fastest technique with an overall mean duration of 89.2 sec (95% CI: 66.9–97.6 sec), also showing the lowest failure rate: 2.2% (n=1). The S-UC technique showed the longest overall mean duration until placement with 115.1 sec (95% CI: 94.7–135.5 sec), also having the overall highest failure rate of 8.9% (n=4) (see Figure 2).
 |
Figure 2 Time to success to implement the cannula correctly and comparison of mean CI values between the different techniques. Abbreviations: L-EUC, Lateral Incision-Emergency Umbilical Cannula; S-UC, Standard Intersection-Umbilical Catheter; S-EUC, Standard Intersection-Emergency Umbilical Cannula. |
We also assessed whether the time to successful cannulation was influenced by the students’ level of training. Using the linear regression model, neither previous experience with central venous access (p=0.49; R² =0.011; rc =−5.02) nor with peripheral venipuncture (p=0.095; R² =0.064; rc=−7.53) had a significant impact, but the regression indices indicated slightly shorter times with increasing training level and pre-existing knowledge (p=0.15; R² =0.048; rc=−0.22).
The results of the questionnaire regarding the preference for a specific technique as well as on the video-based teaching approach are shown in Figure 3 and Table 2. In terms of the used device, the emergency button cannula was preferred to the standard umbilical catheter by 68.9% of the students and 80% rated the standard umbilical cord cut access more promising than the lateral incision. 62.2% would use the S-EUC technique if confronted with a delivery room emergency (S-UC: 26.7%; L-EUC: 11.1%).
 |
Figure 3 Preferred technique as stated by the participants in the questionnaire. Pie charts for the whole group (n=45) (top) and for the 3 different rotation groups (n=15 each) in columns (bottom). (A) Preferred technique if emergency access required in the event of an emergency (B) Favoured device after testing all three techniques. (C) Favoured intersection technique after testing all three techniques. Abbreviations: L-EUC, Lateral Incision - Emergency Umbilical Cannula; S-UC, Standard Intersection - Umbilical Catheter; S-EUC, Standard Intersection - Emergency Umbilical Cannula. |
Prior to the practical exercises and after watching the explanatory videos of each of the three vascular access techniques, participants rated the video-based teaching method as easy to understand (S-EUC 91.1/8,9%; L-EUC 82.2/17,8%; S-UC 82.2/17.8% strongly agree/agree). They also rated their chances of successfully applying the respective technique in the following scenario as positive (S-EUC 64.4%/33.3%; L-EUC 28.9%/51.1%; S-UC 26.7%/71.1% strongly agree/agree). After completing the practical exercises, participants assessment of their ability to perform the respective techniques remained positive (S-EUC 64.4/22.2%; L-EUC 46.7/35.6%; S-UC 60.0/17.8% strongly agree/agree). Overall, the videos were rated as suitable for teaching the different techniques (S-EUC 93.3/6.7%; L-EUC 84.4/13.3% S-UC 82.2/13.3% strongly agree/agree). Only one question showed a statistical difference for the three techniques: Prior to and after the practical exercises, the participants rated the probability of successful use of the S-EUC technique better than for the L-EUC and S-UC techniques (see Table 2). After the video teaching and practical exercises, most participants thought that they could successfully apply at least one of the techniques if faced with a real emergency situation (37.8/48.9 strongly agree/agree).
Discussion
The aim of this study was to develop a useful teaching strategy for neonatal emergency vascular access techniques using the umbilical cord. Because not all hospitals have a specialized neonatology department, different medical specialties and therefore many individuals within a hospital need to be capable of establishing venous access in neonatal emergencies.5 Consequently, the teaching strategy should be temporally flexible, easy to replicate, should require minimal human resources and be cost efficient.
Theoretical knowledge was taught through video training in this study. This form of visual instruction is well-suited for imparting practical skills and has been successfully utilized in the surgical field.22,23 The advantage of video-based teaching is the standardized form, the continuous and unlimited availability and reduced necessity of teachers. When uploaded to an online platform, students can watch the videos at home and on demand, giving them the opportunity to customize the sequence and pace according to their needs.24 In this way, the learning process can take place independently of the hospital’s practical working hours and implements the possibility for long lasting retention of knowledge by using the video and model over and over again. The video teaching was well perceived by the study participants. When asked if they had understood the video, all of them answered positively. The majority also thought that they could perform the technique well after watching the video. As expected, the more applicable techniques in clinical use were found to be the most popular (S-UC and S-EUC). Eleven participants opted to answer neutrally, with most students giving this answer regarding the L-EUC technique, which might suggest that the technique itself was perceived as difficult to perform. Virtual reality simulation was thought to enhance the quality of simulation models and transfer of knowledge. Unfortunately, even recent research could not present suitable evidence for the teaching of technical skills.25,26
Models within simulation-based training can take various forms, such as virtual reality simulators, simulation mannequins or task trainer.27 When selecting the model, the objective should be kept in mind. In the case of this study, the aim was to design a teaching method for a specific technique that should be imparted on many people, putting the focus on low cost, easy reproduction and almost unlimited availability of materials while also entailing the highest fidelity possible. Task trainers offer a useful option for this type of teaching. They are partial body simulators that are used for teaching specific techniques or tasks.27 The fidelity of these models can vary. In the case of umbilical venous access, the actual material on which the emergency access will be placed on later can be used, giving it the highest degree of realism in contrast to commercially available task trainers for different emergency access techniques.
The mean time until successful vascular access in our model was within the previously reported ranges for other kinds of emergency access in other manikin studies.10–12 The participants also answered the question of whether they could imagine using one of the techniques in a real emergency largely positively, apparently thinking that the haptics and technique would not differ greatly from our model. These two findings give us reason to believe that the model has sufficient accuracy for comprehensive teaching. It is also cost-effective and has an almost unlimited availability, since umbilical cords can be easily collected in hospitals with obstetrics departments. They can be frozen for several weeks before further processing. Consequently, umbilical cords can be collected over an extended period and preserved for extensive training sessions. All other material used in this study should also be easily available in every low-level hospital.
Regarding the secondary study objective, it was found that the techniques using the button cannula allowed faster placement than the one using an umbilical catheter. Therefore, these techniques were more comparable to the placement times of the IO method. As there is still uncertainty about the safety of IO access and since the time advantage of IO access over UVC placement seems to decrease when using the button cannula this new method with its two different access routes could strengthen the position of umbilical venous over the IO access in national and international guidelines with further research.
However, there are different limitations of our model. For example, since the dye filled into the umbilical vein stained the vessel more than blood in the umbilical vein, the probands had an advantage compared to the real situation. Since no model study depicts the real-life situation perfectly, it cannot be ruled out that in a real emergency the success rate and time to success may vary from our study.
Conclusion
According to our results, the teaching method of this study seems to be well suited to teach umbilical venous access to a large group of non-pre-trained medical staff in a hospital. The method of imparting theoretical knowledge and training venous access is easy to replicate, cost-effective, and requires minimal financial and human resources while ensuring rapid skill acquisition. We are aware that a combination of video instruction followed by individual training cannot cover the subtleties of neonatal emergency care, we believe our model serves as an effective alternative to hands-on instruction by an experienced neonatologist. Furthermore, the new technique using the button cannula instead of the standard umbilical catheter displayed shorter duration until correct placement of the device as well as a low failure rate, making it a promising alternative that should be investigated further.
Our model is a practical and cost-effective method for teaching neonatal emergency venous access, with implications for medical education theory as well as real-world hospital training protocols. Video-assisted learning combined with real umbilical cords is an effective training approach that could be widely adopted in hospitals with limited neonatal expertise. Future research could focus on validating this method in additional clinical settings and the approach to optimize training for neonatal emergency protocols.
Data Sharing Statement
The dataset supporting the findings of this study, including questionnaire results and time measurements, is available upon reasonable request. Researchers interested in accessing the data may contact the corresponding author.
Ethics Approval and Informed Consent
Approval for the study was granted by the Ethics Committee of the University of Freiburg, Germany (No.10007/20). Informed consent about the use of the human tissue has been obtained before use. Our study is in accordance with the Declaration of Helsinki.
Consent for Publication
All authors gave consent for publication.
Acknowledgments
The authors would like to thank all midwives and the whole staff of the Department of Obstetrics and Gynecology, University Hospital Freiburg for contributing to this study.
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or non-profit sectors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Lamperti M, Bodenham AR, Pittiruti M, et al. International evidence-based recommendations on ultrasound-guided vascular access. Intensive Care Med. 2012;38(7):1105–1117. doi:10.1007/s00134-012-2597-x
2. Lee AC, Cousens S, Wall SN, et al. Neonatal resuscitation and immediate newborn assessment and stimulation for the prevention of neonatal deaths: a systematic review, meta-analysis and Delphi estimation of mortality effect. BMC Public Health. 2011;11(Suppl 3):S12. doi:10.1186/1471-2458-11-S3-S12
3. Association AH, Pediatrics AAo. 2005 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) of pediatric and neonatal patients: neonatal resuscitation guidelines. Pediatrics. 2006;117(5):e1029–38. doi:10.1542/peds.2006-0349
4. Perlman JM, Risser R. Cardiopulmonary resuscitation in the delivery room. Associated clinical events. Arch Pediatr Adolesc Med. 1995;149(1):20–25. doi:10.1001/archpedi.1995.02170130022005
5. Halamek LP, Weiner GM. State-of-the art training in neonatal resuscitation. Semin Perinatol. 2022;46(6):151628. doi:10.1016/j.semperi.2022.151628
6. Monasor-Ortolá D, Cortés-Castell E, Martínez-Pascual C, Esteve-Ríos A, Rizo-Baeza MM. Factors influencing the success of peripheral venous access in neonates. J Pediatr Nurs. 2019;47:e30–e35. doi:10.1016/j.pedn.2019.04.017
7. Madar J, Roehr CC, Ainsworth S, et al. European resuscitation council guidelines 2021: newborn resuscitation and support of transition of infants at birth. Resuscitation. 2021;161:291–326. doi:10.1016/j.resuscitation.2021.02.014
8. Aziz K, Lee HC, Escobedo MB, et al. Part 5: neonatal resuscitation: 2020 American heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142(16_suppl_2):S524–S550. doi:10.1161/CIR.0000000000000902
9. Nolan JP, Maconochie I, Soar J, et al. Executive summary: 2020 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2020;142(16_suppl_1):S2–S27. doi:10.1161/CIR.0000000000000890
10. Abe KK, Blum GT, Yamamoto LG. Intraosseous is faster and easier than umbilical venous catheterization in newborn emergency vascular access models. Am J Emerg Med. 2000;18(2):126–129. doi:10.1016/s0735-6757(00)90001-9
11. Rajani AK, Chitkara R, Oehlert J, Halamek LP. Comparison of umbilical venous and intraosseous access during simulated neonatal resuscitation. Pediatrics. 2011;128(4):e954–8. doi:10.1542/peds.2011-0657
12. Schwindt EM, Hoffmann F, Deindl P, Waldhoer TJ, Schwindt JC. Duration to establish an emergency vascular access and how to accelerate it: a simulation-based study performed in real-life neonatal resuscitation rooms. Pediatr Crit Care Med. 2018;19(5):468–476. doi:10.1097/PCC.0000000000001508
13. Guze PA. Using technology to meet the challenges of medical education. Trans Am Clin Climatol Assoc. 2015;126:260–270.
14. Motola I, Devine LA, Chung HS, Sullivan JE, Issenberg SB. Simulation in healthcare education: a best evidence practical guide. AMEE Guide No. 82. Med Teach. 2013;35(10):e1511–30. doi:10.3109/0142159X.2013.818632
15. Kovacs G, Levitan R, Sandeski R. Clinical cadavers as a simulation resource for procedural learning. AEM Educ Train. 2018;2(3):239–247. doi:10.1002/aet2.10103
16. Rippey JC, Blanco P, Carr PJ. An affordable and easily constructed model for training in ultrasound-guided vascular access. J Vasc Access. 2015;16(5):422–427. doi:10.5301/jva.5000384
17. Troianos CA, Hartman GS, Glas KE, et al. Special articles: guidelines for performing ultrasound guided vascular cannulation: recommendations of the American society of echocardiography and the society of cardiovascular anesthesiologists. Anesth Analg. 2012;114(1):46–72. doi:10.1213/ANE.0b013e3182407cd8
18. Tolerton SK, Hugh TJ, Cosman PH. The production of audiovisual teaching tools in minimally invasive surgery. J Surg Educ. 2012;69(3):404–406. doi:10.1016/j.jsurg.2011.10.017
19. Sawyer T, Starr M, Jones M, et al. Real vs simulated umbilical cords for emergency umbilical catheterization training: a randomized crossover study. J Perinatol. 2017;37(2):177–181. doi:10.1038/jp.2016.194
20. Brickmann C, Zang FC, Klotz D, Kunze M, Lenz S, Hentschel R. Emergency button cannula vs. umbilical catheter as neonatal emergency umbilical vein access - a randomized cross-over pilot study. J Perinat Med. 2023;51(1):27–33. doi:10.1515/jpm-2022-0071
21. Senn S. Cross-Over Trials in Clinical Research.
22. Mota P, Carvalho N, Carvalho-Dias E, João Costa M, Correia-Pinto J, Lima E. Video-based surgical learning: improving trainee education and preparation for surgery. J Surg Educ. 2018;75(3):828–835. doi:10.1016/j.jsurg.2017.09.027
23. Rapp AK, Healy MG, Charlton ME, Keith JN, Rosenbaum ME, Kapadia MR. YouTube is the most frequently used educational video source for surgical preparation. J Surg Educ. 2016;73(6):1072–1076. doi:10.1016/j.jsurg.2016.04.024
24. Bridge PD, Jackson M, Robinson L. The effectiveness of streaming video on medical student learning: a case study. Med Educ Online. 2009;14:11. doi:10.3885/meo.2009.Res00311
25. Putnam EM, Rochlen LR, Alderink E, et al. Virtual reality simulation for critical pediatric airway management training. J Clin Trans Res. 2021;7(1):93–99.
26. Abulfaraj MM, Jeffers JM, Tackett S, Chang T. Virtual reality vs. high-fidelity mannequin-based simulation: a pilot randomized trial evaluating learner performance. Cureus. 2021;13(8):e17091. doi:10.7759/cureus.17091
27. Lopreiato JO, Sawyer T. Simulation-based medical education in pediatrics. Acad Pediatr. 2015;15(2):134–142. doi:10.1016/j.acap.2014.10.010
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.