")
Back to Journals » Advances in Medical Education and Practice » Volume 16
The Application of CT 3D Reconstruction and 3D Printing Technology Combined with CBL Teaching Mode in the Clinical Teaching of Joint Orthopedics
Authors Zhang W, Chen Y, Huang X
Received 12 December 2024
Accepted for publication 24 March 2025
Published 4 April 2025 Volume 2025:16 Pages 535—543
DOI https://doi.org/10.2147/AMEP.S509201
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Weiyue Zhang,1,* Yizhang Chen,2,* Xin Huang2
1Department of Endocrinology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, China; 2Department of Orthopaedics, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, China
*These authors contributed equally to this work
Correspondence: Xin Huang, Email [email protected]
Purpose: The traditional teaching mode Lecture Based Learning (LBL) often results in student’s poor initiative and independent thinking ability and low learning interest. This study aims to investigate the application of CT 3D reconstruction and 3D printing technology combined with CBL teaching mode in the clinical teaching of orthopedics and standardized training of residents.
Methods: Sixty residents of our hospital were randomly selected to conduct the teaching of joint orthopedic content in orthopedic surgery courses. They were randomly divided into three groups at the time of admission, which adopted LBL teaching mode, CBL teaching mode, CT 3D reconstruction and 3D printing technology combined with CBL teaching mode, respectively.
Results: The theoretical knowledge scores and clinical skills scores of the standardized training students in the CBL+3D printing group were significantly higher than those in the LBL or CBL group. Students in CBL+3D printing group had significantly higher recognition in self-ability evaluation. The overall teaching satisfaction of students in CBL+3D printing group was 85.00% (P < 0.05).
Conclusion: The combination of CT 3D reconstruction and 3D printing technology with CBL teaching mode can help the students to master the theoretical knowledge and practical skills in the standardized training of joint orthopedics residents, which can effectively improve the teaching quality.
Keywords: 3D printing, CBL teaching model, orthopedic joints, standardized training of residents
Introduction
The traditional teaching mode “Lecture Based Learning” (LBL) often results in student’s poor initiative, independent thinking ability and low learning interest. Additionally, LBL has a singular pattern which leads to limited chances in clinic experience and inadequate ability in operating practices. Especially in the clinical teaching of orthopedics such as hip or knee joints, using single LBL teaching mode might no longer meet the need of students’ understanding and mastery of diagnosis and treatment of joint orthopedic diseases. Accordingly, it is warranted to discover and innovate the clinical teaching mode of joint orthopedics. Case Based Learning (CBL) is a new learning strategy which could bridge the gap between traditional theoretical teaching and clinical experience.1,2 This teaching mode could better prepare students for clinical practice through the use of real or realistic clinical cases and has been used in many fields of medical education.3–6 By combining CT 3D reconstruction and 3D printing technology with CBL teaching mode, this study aims to investigate the teaching quality and effects of this novel teaching mode on clinical teaching of orthopedics and standardized training of residents.
Nowadays, the traditional teaching mode of standardized training of residents still highlights the importance of theoretical knowledge. This pattern weakens the cultivation of practice and leads to students’ poor studying autonomy. The core of CBL is aimed at case, based on problems, student-oriented, leading by teachers. The concrete processes of CBL are as follows. Teachers give a classic clinic case. After fully analyzing and discussing this case, students raise their questions and use their knowledge about the diagnosis and treatment of the disease to solve the problems.7 The advantage of CBL is that students participate in studying actively when introducing clinic cases, which can fully raise their interest and practice their ability of raising, analyzing, and solving problems.8 The CBL teaching mode can change the situation of poor practice of standardized training residents. However, orthopedic standardized training requires residents good command of topography anatomy knowledge. Simple CBL fails to satisfy the need of teaching, therefore the combination of CT 3D reconstruction and 3D printing technology with CBL is vital.9,10
CT 3D reconstruction and 3D printing technology has gradually become a hot topic in the field of orthopedic clinic teaching.11 Using CT 3D reconstruction, students get high-definition bone figures and use software tools for further analysis and presentation. 3D printing transfers the reconstructed figure into visual and three-dimensions solid models, thereby allowing students to touch and practice.12 The combination of CT 3D reconstruction and 3D printing technology can not only improve students’ comprehensive ability but also cultivate their practice ability, which improves the teaching quality and students’ participation.13 Additionally, using the printed model monitors orthopedic surgical procedure for students to practice, which ease the problems of bodies shortage.14,15 The integration of CT 3D reconstruction and 3D printing with CBL is grounded in constructivist learning theory, which emphasizes active knowledge construction through real-world cases and hands-on experiences. Additionally, cognitive load theory supports the use of 3D visualization to reduce extraneous cognitive load, enabling learners to focus on understanding and applying complex anatomical concepts. This combination aligns with the principles of technology-enhanced learning, which has been shown to improve engagement and outcomes in clinical education.
Despite its widespread use, traditional LBL has been criticized for its limited ability to foster student initiative, independent thinking, and clinical reasoning skills. While CBL and digital tools such as 3D printing have shown promise in addressing these limitations, their combined application in orthopedic resident training remains under-explored. This study seeks to bridge this gap by investigating the effectiveness of integrating CT 3D reconstruction and 3D printing with CBL in enhancing theoretical knowledge, practical skills, and learner satisfaction among orthopedic residents. This study combines CT 3D reconstruction and 3D printing technology with CBL teaching mode for joint orthopedic teaching at Wuhan Union Hospital. By using this teaching model in the clinical teaching of orthopedics and standardized training of residents, it is expected to harvest better education efficiency.
Methods
Design and Participants
We randomly selected 60 standardized training of residents in Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, to conduct the teaching of joint orthopedics. They were randomly divided into three groups at the time of admission, which adopted LBL teaching mode (LBL group), CBL teaching mode (CBL group), CT 3D reconstruction and 3D printing technology combined with CBL teaching mode (CBL+3D printing group), respectively. This was the first time for the three groups of participants to learn the joint orthopedics. There was no difference in the baseline data of gender and age among the three groups. Inclusion criteria: (1) Participants gave informed consent and participated voluntarily; (2) Participants completed the teaching tasks according to the plan; (3) Participants completed all exams and satisfaction surveys. Exclusion criteria: (1) Participants were absent from class; (2) Participants failed to cooperate with teaching tasks.
Randomization Procedure and Blinding
As for the randomization procedure, participants were randomly assigned by using a computer-generated random number sequence. This process was carried out by an independent researcher who was not involved in the recruitment or assessment of participants. The randomization sequence was concealed until the intervention was assigned. As for blinding, while the intervention made it challenging to blind participants and researchers to group allocation, we implemented blinding for outcome assessors and data analysts to minimize bias. Outcome assessors were unaware of the group assignments, and data were analyzed by a statistician who was blinded to the study conditions.
Ethics
This study was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology (2021-S258). Participation was voluntary in this study, and written informed consent was obtained prior to initiation of the study and data collection. Participants were informed about the purpose and benefits of this study and were also assured that the information collected during the study was anonymous and confidential.
LBL Group
Students in LBL group are taught in tradition LBL method. In teaching process, teachers follow syllabus to explain textbook, highlighting difficult and significant points. After that, students participate in clinical practice teaching in clinical department and teachers guide the students to complete the teaching tasks according to the established plan. Finally, student complete exams and questionnaire to evaluate learning outcome.
CBL Group
Students in CBL are taught in CBL teaching mode. Teachers give a classic clinical case in joint orthopedics and introduce relevant medical history and case information, according to the patient’s condition to raise the issues that need to be addressed. And instruct students to raise their questions and use their knowledge about the given case problems. Students are divided into four groups of five people each. Collect evidence-based medical evidence by group. Students discuss according to clinical manifestations of the disease and treatment options and present case report by PowerPoint. Finally, we conduct theoretical exams and questionnaire survey to evaluate learning outcome.
CBL+3D Printed Group
Students in CBL+3D printed group are taught in CT 3D reconstruction and 3D printing technology combined with CBL teaching mode. Teachers give a classic clinical case in joint orthopedics and introduce relevant medical history and case information, according to the patient’s condition to raise the issues that need to be addressed. And instruct students to raise their questions and use their knowledge about the given case problems. Students are divided into four groups (n = 5). Collect evidence-based medical evidence by group. Teachers provided prepared CT 3D reconstruction images of pelvis anteroposterior projection (Figure 1A), pelvis lateral projection (Figure 1B), knee joint anteroposterior projection (Figure 1C), and knee joint lateral projection (Figure 1D), and 3D printed models of hip joint (Figure 2A), proximal femur (Figure 2B), and knee joint (Figure 2C) to guide students to operate on 3D printed models. Students discuss according to clinical manifestations of the disease and treatment options and present case report by PowerPoint.
 |
Figure 1 CT 3D reconstruction images of (A) pelvis anteroposterior projection, (B) pelvis lateral projection, (C) knee joint anteroposterior projection, and (D) knee joint lateral projection. |
 |
Figure 2 3D printed models of (A) Hip joint, (B) proximal femur, and (C) knee joint. |
Training Procedures and Data Collection
Theoretical Knowledge Achievements
At the end of teaching, a teacher will arrange a joint orthopedic theory knowledge test for three groups of students (total score of 100 points), involving the common diseases of joint orthopedic such as hip fracture, necrosis of the femoral head, osteoarthritis etc. According to the evaluation criteria, test scores will be divided according to the following grades: less than 60 points for poor, 60–80 points for average, and above 80 points for excellent.
Clinical Skill Achievements
Clinic skills tests are divided into two parts (100 points). The first part is the demonstration of orthopedic related skills (50 points). And the second part is the analysis and writing of joint orthopedic cases (50 points) According to the evaluation criteria, test scores will be divided according to the following grades: less than 60 points for poor, 60–80 points for average, and above 80 points for excellent.
Self-Evaluation
After learning in three different methods, students evaluate their ability from theoretical knowledge, image interpretation, communication to clinical thinking. According to the evaluation criteria, test scores could be divided according to the following grades: less than 60 points for poor, 60–80 points for average, and above 80 points for excellent.
Teaching Satisfaction Evaluation
After the assessment, each student will be given an anonymous teaching effect questionnaire. Satisfaction will be evaluated according to five aspects: teachers’ performance, teaching content, teaching difficulty, students’ learning interest and practice (10 points). According to the evaluation criteria, test scores will be divided according to the following grades: less than 2 points for dissatisfied, 4–6 points for general, and above 8 points for satisfaction. Every student rates according to their studying situation.
Statistical Analysis
GraphPad Prism 6.0 and SPSS were used to conduct the data analysis. Continuous variables, such as theoretical knowledge scores and clinical skills scores, were compared among the three groups using one-way ANOVA, followed by post-hoc Tukey’s tests for pairwise comparisons. Categorical variables, such as teaching satisfaction levels (eg, satisfied, neutral, dissatisfied), were analyzed using the chi-square test. P < 0.05 was statistically significant.
Results
Theoretical Knowledge Achievements
The theoretical knowledge achievements of students in CBL groups were higher than that of LBL group (χ2= 6.53, P = 0.04, Table 1). Students in CBL+3D printing group were higher than students in CBL group (χ2= 7.46, P = 0.02, Table 1). The participants of the lecture are the standardized training of residents in our hospital, who study the orthopedic for the first time and knowledge base are relatively weak. However, to fully command common disease in joint orthopedic such as hip fracture, necrosis of the femoral head, osteoarthritis needs a stable knowledge of anatomy.
 |
Table 1 Comparison of Theoretical Knowledge Achievements of Joint Orthopedics Residents |
Clinical Skill Achievements
As for clinical skill achievements, the score of students in CBL group has no significant difference with that of students in LBL group (χ2= 0.42, P = 0.81, Table 2). The clinical skill achievements in CBL+3D printing group were significantly higher than that in CBL group (χ2= 8.88, P = 0.01, Table 2). Compared with LBL teaching mode, CBL teaching mode has no significant improvement in students’ clinical skills. However, the combination of CT 3D reconstruction and 3D printing technology with CBL teaching mode could improve students’ clinical skills significantly.
 |
Table 2 Comparison of Clinical Skill Achievements of Joint Orthopedics Residents |
Self-Evaluation
As for self-evaluation, students in CBL+3D printing group generally felt that their grades were good and had a positive assessment of their abilities. The result shows this new teaching mode has significant advantages (χ2= 6.47, P = 0.04, Table 3). However, the self-evaluation of students in CBL group has no significant difference with that of students in LBL group (χ2= 1.92, P = 0.38, Table 3).
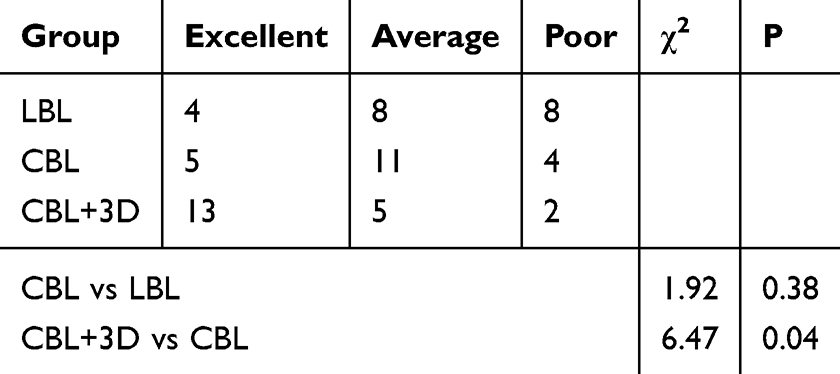 |
Table 3 Comparison of Self-Evaluation of Joint Orthopedics Residents |
Teaching Satisfaction Evaluation
Total satisfaction ratings in CBL+3D printing were significantly higher than CBL group (85.00% vs 45.00%, χ2= 7.46, P = 0.02, Table 4). However, satisfaction ratings in CBL group have no significant difference with that in LBL group (45.00% vs 30.00%, χ2= 1.89, P = 0.34, Table 4).
 |
Table 4 Comparison of Teaching Satisfaction Evaluation of Joint Orthopedics Residents |
Discussion
The diagnosis and treatment of joint orthopedic diseases is highly associated with anatomical structures, which require spatial imagination ability among students. However, traditional teaching mode relies on anatomy and iconography, which often lack the necessary visualization and practical applicability. Consequently, students may not engage fully in clinical practice. Thus, there is a pressing need to improve joint orthopedic clinic teaching. CBL teaching mode presents certain limitations. Primarily, CBL highly depends on the selection of cases, which directly impacts the quality of instruction. Additionally, teaching quality also influenced by the content, instructional methods, teaching methods and the interaction among students. One study learned from CBL in surgery noted that alignment with clinical placements is equally significant with weakness above, which could help students see relevance and applicability in a clinic case.1 In recent years, digital technology has been widely used in many aspects of clinical teaching as a new teaching pattern due to its simple and effective operation and visual structure. Another study applied in tetralogy of Fallot teaching shows the combination of CBL with 3D printing models is feasible and effective, which better improves performance, promotes diagnostic skills, bolsters self-assurance in managing cases, enhanced satisfaction, cultivate critical thinking and clinical reasoning abilities.16 Given the specific of orthopedic diseases, there are abundant figures and models suitable for CBL. Thus, digital technology has natural advantages on the spread in orthopedic clinic teaching and improves teaching quality remarkably.
This study suggests that students in the CBL+3D printing group significantly outperformed those in the LBL group or the CBL group in both theoretical knowledge and clinical skills achievement. This indicates that digital technology-assisted CBL teaching has advantages in imparting knowledge during the standardized training of joint orthopedics residents. Through animated scene simulations, students could intuitively observe the movement, morphology, and stability of the hip and knee joints, thereby deepening their understanding of abstract theoretical knowledge such as CT 3D reconstruction images of femoral neck fracture (Figure 3A), intertrochanteric fracture (Figure 3B), osteonecrosis of the femoral head (ONFH, Figure 3C), and knee osteoarthritis (OA, Figure 3D).17 Additionally, by collecting imaging data from clinical cases to create models of different types of orthopedic diseases through 3D printing technology, teaching and operational demonstrations can be conducted to explain the key surgical points for various diseases.18 It is well known that 3D printing model could also have better insight into specific anatomy, better pre-operative planning, simulation-based training and education.19 By practicing on the models, students can improve their clinical practice skills. Compared to traditional teaching methods, this approach effectively addresses the issue of insufficient clinical practice participation among standardized training of joint orthopedics residents.
 |
Figure 3 CT 3D reconstruction images of (A) femoral neck fracture, (B) intertrochanteric fracture, (C) osteonecrosis of the femoral head (ONFH), and (D) knee osteoarthritis (OA). |
The combination of CBL with CT 3D reconstruction and 3D printing significantly enhances students’ clinical knowledge and their ability to analyze visual data. This pattern not only increases student satisfaction with the educational experience but also strengthens their foundational clinical theories and skills. Another study applied in clinical teaching of cerebrovascular disease suggested that this combination showed higher satisfaction, learning interest, and improvement in the spatial thinking ability of resident. Furthermore, it could also strengthen their problem-analysis and solving skills.10,20 The outcomes of this teaching mode show notably positive, demonstrating originality and representativeness. To further advance the CBL teaching model supported by digital technologies, it is essential for educators and academic institutions to invest more to ensure enough scientific and technological personnel and to allocate sufficient funding and provide appropriate instructional environments. Implementing these measures can lead to improved educational outcomes and facilitate the broader adoption of this innovative teaching approach. The cost, time, and feasibility of 3D printed models need consideration. For example, in our study, all 3D models are derived from clinical materials at no additional cost. If it is a clinically unavailable model, we have provided a timeline for the creation of 3D printed models, from data acquisition and model design to printing and post-processing (about 1–2 days). Accordingly, the implementation of 3D printed models in educational or clinical settings is highly feasible. As for the lack of long-term follow-up data in the present study, we have proposed a future research direction to address this gap. Specifically, we plan to conduct a longitudinal study to evaluate the retention of knowledge and skills acquired through 3D printed models over a period of 3 years. Additionally, we aim to assess the impact of these models on clinical outcomes, such as diagnostic accuracy or surgical performance.
The limitations of this study are concluded as follows. The sample size of 60 residents, though adequate for preliminary analysis, may restrict the statistical power and broader applicability of the findings. Conducted in a single institution, the study may suffer from institutional bias and limited generalizability to other settings with different resources or resident demographics. The short follow-up period focused solely on immediate learning outcomes, neglecting long-term knowledge and skill retention, which is crucial for assessing the sustained impact of the CBL+3D printing teaching model. Additionally, potential confounding factors, such as residents’ prior experience with 3D technology or individual learning preferences, were not accounted for, possibly influencing the results. The generalizability of the study is constrained by its single-institution setting and specific teaching resources. The effectiveness of the CBL+3D printing approach depends on access to 3D reconstruction software, printers, and trained personnel, which may not be available in resource-limited settings. Adaptations may be necessary to fit different cultural or educational contexts. To enhance generalizability, future studies should replicate this approach in diverse settings, including multiple institutions and regions, and evaluate long-term knowledge retention and clinical performance impact. Larger, multi-center trials are needed to validate the model’s effectiveness across varied populations. Comparative studies with other innovative methods like VR or AR, as well as cost-effectiveness analyses, would provide further insights. For clinical application, the CBL+3D printing model should be integrated into orthopedic residency curricula as a supplementary tool for teaching complex anatomy and surgical planning. Institutions should train educators in using 3D technology and consider investing in the necessary equipment to support this innovative teaching method.
Conclusions
In conclusion, the teaching mode offers the benefit of facilitating the rapid application of knowledge by students, thereby enhancing the effectiveness of their learning through visual presentations. The combination of digital technology with CBL in standardized training for joint orthopedics might meet the needs of residents more effectively. And it could improve their clinical skills and competencies, thus fulfilling the requirements of standardized training.
Data Sharing Statement
All data are available in the main text.
Ethics
This study was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology. Participation was voluntary in this study, and written informed consent was obtained prior to initiation of the study and data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study is supported by the National Natural Science Foundation of China (82203059, 82300932) and the Post-graduation Education and Teaching Research Project of the First Clinical College of Tongji Medical College, Huazhong University of Science and Technology (Owned by Xin Huang).
Disclosure
The authors declare that they have no competing interests.
References
1. Nordquist J, Sundberg K, Johansson L, Sandelin K, Nordenström J. Case-based learning in surgery: lessons learned. World J Surg. 2012;36:945–955. doi:10.1007/s00268-011-1396-9
2. Kelly M, Feeley I, Boland F, O’Byrne JM. Undergraduate clinical teaching in orthopedic surgery: a randomized control trial comparing the effect of case-based teaching and bedside teaching on musculoskeletal OSCE performance. J Surg Educ. 2018;75:132–139. doi:10.1016/j.jsurg.2017.06.024
3. Ricci FL, Consorti F, Gentile M, et al. Case-based learning: a formal approach to generate health case studies from electronic healthcare records. Stud Health Technol Inform. 2016;221:107–111.
4. Ma W, Gao H, Liu X, et al. An exploration into the application of specialty-orientated CBL pedagogy in undergraduate teaching in pediatric surgery. Front Pediatr. 2022;10:948853. doi:10.3389/fped.2022.948853
5. Li H, Qi X, Nie T. PBL and CBL integrated picture example in the teaching of gastrointestinal tumor. Asian J Surg. 2022;45:3042–3043. doi:10.1016/j.asjsur.2022.09.051
6. Zhang M, Hu W. Application of PBL combined with CBL teaching method in clinical teaching of vascular surgery. PLoS One. 2024;19:e0306653. doi:10.1371/journal.pone.0306653
7. McLean SF. Case-based learning and its application in medical and health-care fields: a review of worldwide literature. J Med Educ Curric Dev. 2016;3. doi:10.4137/jmecd.S20377
8. Cen XY, Hua Y, Niu S, Yu T. Application of case-based learning in medical student education: a meta-analysis. Eur Rev Med Pharmacol Sci. 2021;25:3173–3181. doi:10.26355/eurrev_202104_25726
9. Brumpt E, Bertin E, Tatu L, Louvrier A. 3D printing as a pedagogical tool for teaching normal human anatomy: a systematic review. BMC Med Educ. 2023;23:783. doi:10.1186/s12909-023-04744-w
10. Jiang W, Jiang W, Jin P, et al. Application of 3D printing technology combined with PBL teaching method in clinical teaching of cerebrovascular disease: an observational study. Medicine. 2022;101:e31970. doi:10.1097/md.0000000000031970
11. Maglara E, Angelis S, Solia E, et al. Three-Dimensional (3D) printing in orthopedics education. J Long Term Eff Med Implants. 2020;30:255–258. doi:10.1615/JLongTermEffMedImplants.2020036911
12. Squelch A. 3D printing and medical imaging. J Med Radiat Sci. 2018;65:171–172. doi:10.1002/jmrs.300
13. Feng S, Sun Y-J, Zhu Q-R, et al. Integration of 3D printing and case-based learning in clinical practice for the treatment of developmental dysplasia of the Hip. BMC Med Educ. 2024;24:986. doi:10.1186/s12909-024-05934-w
14. Weidert S, Andress S, Suero E, et al. [3D printing in orthopedic and trauma surgery education and training: possibilities and fields of application]. Unfallchirurg. 2019;122:444–451. German. doi:10.1007/s00113-019-0650-8
15. Girotto MC, Lucena RD, Schwartsmann CR, et al. Use of 3D printing in planning the reconstruction of total hip arthroplasty: a teaching tool. Rev Bras Ortop. 2021;56:809–812. doi:10.1055/s-0041-1726064
16. Zhao J, Gong X, Ding J, et al. Integration of case-based learning and three-dimensional printing for tetralogy of Fallot instruction in clinical medical undergraduates: a randomized controlled trial. BMC Med Educ. 2024;24:571. doi:10.1186/s12909-024-05583-z
17. Keating TC, Jacobs JJ. Augmented reality in orthopedic practice and education. Orthop Clin North Am. 2021;52:15–26. doi:10.1016/j.ocl.2020.08.002
18. De Backer P, Allaeys C, Debbaut C, Beelen R. Point-of-care 3D printing: a low-cost approach to teaching carotid artery stenting. 3D Print Med. 2021;7:27. doi:10.1186/s41205-021-00119-3
19. Meyer-Szary J, Luis MS, Mikulski S, et al. The role of 3D printing in planning complex medical procedures and training of medical professionals-cross-sectional multispecialty review. Int J Environ Res Public Health. 2022;19. doi:10.3390/ijerph19063331
20. Michel MC, Bischoff A, Jakobs KH. Comparison of problem-and lecture-based pharmacology teaching. Trends Pharmacol Sci. 2002;23:168–170. doi:10.1016/s0165-6147(00)01940-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.