")
Back to Journals » Advances in Medical Education and Practice » Volume 16
The Mediating Role of Self-Confidence in Medical Students’ Attitudes and Clinical Performance Toward People with Disability
Authors Yazbeck Karam VG, Bou Malhab S, Aoun Bahous S, Salameh P , El Khoury-Malhame M , Asmar N
Received 10 March 2025
Accepted for publication 29 June 2025
Published 4 July 2025 Volume 2025:16 Pages 1169—1179
DOI https://doi.org/10.2147/AMEP.S522243
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Vanda G Yazbeck Karam,1,2 Sandrella Bou Malhab,1,3 Sola Aoun Bahous,1 Pascale Salameh,1,3– 5 Myriam El Khoury-Malhame,6 Nadia Asmar1
1School of Medicine, Lebanese American University, Byblos, Lebanon; 2Department of Anesthesiology, Lebanese American University, Gilbert and Rose-Marie Chagoury School of Medicine, Byblos, Lebanon; 3Institut National de Santé Publique d’Épidémiologie Clinique et de Toxicologie-Liban (INSPECT-LB), Beirut, Lebanon; 4Faculty of Pharmacy, Lebanese University, Hadat, Lebanon; 5Department of Primary Care and Population Health, University of Nicosia Medical School, Nicosia, 2417, Cyprus; 6Department of Psychology and Education, School of Arts and Science, Lebanese American University, Byblos, Lebanon
Correspondence: Sandrella Bou Malhab, School of Medicine, Lebanese American University, Byblos, Lebanon, Email [email protected] Vanda G Yazbeck Karam, Department of Anesthesiology, Lebanese American University, Gilbert and Rose-Marie Chagoury School of Medicine, Byblos, Lebanon, Email [email protected]
Introduction: This study aimed to explore the mediating role of self-confidence in shaping the relationship between gender and year of enrollment, and medical students’ attitudes towards people with disability (PWD), and their clinical performance particularly in cultural contexts where stigma is prevalent.
Methods: A cross-sectional study was conducted as part of an internal assessment at a private medical school in Lebanon, involving 143 medical students from all four years of the program. Mediation analysis with PROCESS macro, was used to explore the impact of self-confidence on students’ attitudes and clinical performance with PWD.
Results: Students in higher years of medical training demonstrated more positive attitudes and better clinical performance with PWD, mediated by greater self-confidence. Conversely, female students reported lower self-confidence, negatively influencing their attitudes and clinical interactions with PWD.
Discussion: This research highlights the critical role of self-confidence in mediating medical students’ attitudes and performance with PWD. Findings suggest the need for curriculum reforms to incorporate disability-focused training and additionally address gender-specific barriers to confidence-building.
Keywords: medical student, self-confidence, mediation analysis, attitudes, patients with disability, medical education, clinical setting
Background
Medical school represents an intense learning environment where success is largely dependent on overcoming a range of doubt-inducing intellectual, social, and motivational challenges. In such environments, students often choose to engage in activities where success is assured, avoiding those perceived as riskier. This behavior aligns with the Self-Efficacy Theory (SET),1 a key component of Bandura’s social cognitive theory (SCT), which defines self-efficacy as the confidence to carry out the courses of action necessary to accomplish desired goals. Although skills and knowledge are crucial, beliefs about one’s capabilities to apply these resources effectively can mediate perceptions of success or failure.2
Within this framework, medical educators strive to understand the mechanisms underlying student learning, by considering various factors that mediate achievement during medical training and clinical practice, aiming to enhance curriculum design for trainees.3 It is hypothesized that self-efficacy plays a pivotal role in medical students’ learning, personal growth, and professional development.4
In the educational literature, “confidence” has often been used interchangeably with self-efficacy.5 In fact, the cumulative impact of positive or negative confidences shapes an individual’s overall sense of competence, influencing motivation, emotional responses, thoughts and behaviors.6
Furthermore, self-confidence is shaped by a one’s character, experiences, expectations, social and cultural conditioning. This is particularly relevant in contexts reinforcing social inequity such as gender race, disability and socio-economic status, even among individuals with initially equivalent abilities.7 In medical education, addressing these disparities through inclusive curricula and mentorship programs can bridge the gap in self-confidence between different groups of students, ensuring equitable professional development. Individuals who are encouraged to lead or believe in themselves tend to exhibit higher self-confidence compared to those who are not. In this context, biases, stereotypes, roles, division of labor and rewards system significantly influence the development of self-confidence, with more dominant groups generally demonstrating greater self-confidence than less dominant ones.8
In the context of dealing with people with disabilities (PWD), research on the preparedness and confidence of medical students using existing academic curricula is limited worldwide.9 This gap underscores the necessity for validated instruments to assess medical students’ attitudes toward PWD, as demonstrated by recent studies.10 This field is particularly understudied in Lebanon, a Levantine country where cultural and social stigmas around PWD might further complicate interactions. Lebanon’s unique socio-cultural landscape underscores the importance of localized research to inform tailored interventions for improving medical education on disability.
Students’ attitudes and behavior to PWD are indeed influenced by the prevalent Lebanese local context and general attitude towards disability. Some of those stigmatizing attitudes might be worsened by the lack of governmental11 support, the lack of adequate infrastructures and facilities, the absence of awareness and conversations around disability. This might lead to interpersonal distance and hesitation to engage with PWD in the medical community.12 Negative social implicit attitudes additionally contribute to this discomfort. Medical students’ attitudes often reflect the attitudes of the broader society.13 On one hand, studies have shown that healthcare providers’ impressions and expectations of individuals seeking care are largely influenced by potential disability status, which could subsequently transform those attitudes into significant healthcare barriers.14 On the other hand, the absence of specialized services and facilities for disabled patients can be a direct critical challenge to medical and healthcare access in Lebanon.11 For instance, while hospitals are equipped for wheelchairs, they often lack accommodations for sensory impairment (vision, hearing) or intellectual disabilities.
Furthermore, medical education often provides students with limited formal training in working with PWD.15 With students reporting minimal exposure to such patients,16 and demonstrating better performance in scenarios involving patients without disabilities.17,18 There is also limited research on the place of PWD within the healthcare system in general, and more specifically in medical education. In fact, medical school curricula may reinforce implicit and explicit disability biases19 affecting medical students’ attitudes toward PWD.9 Addressing these challenges requires comprehensive training for healthcare professionals, as recommended by the WHO.20 Medical schools are urged to improve their curricula with equity, diversity, and embedding inclusivity towards PWD especially for female students since women and men do not differ in their clinical performance, but women in healthcare fields may perceive deficiencies in their abilities more often than their male counterparts.21 This may be achieved by challenging ableist messages effectively, and efforts to reform medical curricula anti sexist and anti-ableism language for PWD to be treated equitably.22,23
Along those lines, literature suggests that self-confidence is an important indicator of psychological adaptation,24 with individuals possessing higher self-confidence more likely to hold positive views about, and accept diverse populations such as PWD. Despite some reported feelings of fear and discomfort, healthcare students and professionals generally hold favorable attitudes toward PWD, although they often lack of knowledge and experience in providing care for PWD.25
The complexity of investigating the attitudes of healthcare professionals and students toward PWD in clinical settings also involves factors such as prior exposure and accumulated experiences. Research indicates that early and repeated interactions with PWD can foster empathy, improve attitudes, and strengthen clinical skills among medical students. Studies show that the association between previous experience with patients with physical disabilities and provider attitudes is causal, with greater experience correlating with more favorable attitudes.26
Given that students and learning environments are complex and multifaceted, it is crucial to consider a broad range of variables to develop a more comprehensive understanding of the learning process. While researchers in medical education have explored factors influencing clinical outcomes in PWD, the role of self-confidence in mediating these personal factors has been less addressed. To more accurately reflect real-life encounters, examining both the direct and indirect effects of personal self-confidence on medical students’ attitudes towards PWD and their clinical experiences with such patients is essential. By integrating these insights, educators can design interventions that build both competence and compassion in healthcare professionals. The objective of this study is thus to explore the mediating effect of medical student’s confidence in dealing with PWD on the relationship between gender and year of enrollment (as a proxy for experience), with their attitude towards PWD and performance in a clinical scenario involving PWD.
Methods
Study Design and Participants
This cross-sectional study was conducted at the Lebanese American University Gilbert & Rose-Marie Chagoury School of Medicine (LAUSOM) as part of a standard internal evaluation process. An online questionnaire, developed in English and administered via Google Forms, was distributed to students via Email from the Medical Education Department. The study sample was randomly drawn from a total population of medical students of 251 individuals, and 143 medical students from all four years of the medical program filled out the online survey. The study’s scope and purpose were clearly outlined at the beginning of the questionnaire. Participants were informed that their participation was voluntary and were assured that their responses would remain anonymous and confidential. After providing informed consent, participants completed the questionnaire. The study proposal received approval from the LAU Institutional Review Board (IRB00006954 LAUIRB#1).
LAUSOM’s curriculum integrates basic and clinical sciences with practical experience starting from the very first weeks. Disability is incorporated into the preclinical curriculum through Social Medicine and Ethics courses, featuring lectures, tutorials, and case-based discussions. The topic is explored in the pulmonary module in year 1 and in the Musculoskeletal and Neuropsychiatry modules in year 2. To enhance practical skills, an Objective Structured Clinical Examination (OSCE) station featuring a standardized patient with a disability was introduced for second-year medical students. This station assessed students’ abilities in patient-centered interviews, appropriate physical examinations, effective communication, and formulating tailored management plans. Scenarios included patients with mobility, speech, or visual impairments, providing practical experience in diverse clinical situations and enhancing clinical competence and confidence.
However, during the clinical years, although students rotate through various hospitals and dispensaries, disability is not explicitly covered as a distinct topic, and none of the training sites are specifically focused on disability care.
Questionnaire and Variables
The study questionnaire covered the following sections (Supplementary Material Appendix 2):
- The sociodemographic information: This section covered data on age, gender, year of enrollment, and intended residency specialty.
- Clinical experience with PWD:10 This section presented two identical clinical scenarios. Scenario A involved a patient with no apparent disability, while in Scenario B (Cronbach alpha = 0.539), the patient was in a wheelchair and experienced spasticity and speech impairment. Each scenario was followed by the same four questions regarding the clinical situation and the student’s level of comfort, assessed using a four-point Likert scale.
- “Medical Students’ Attitudes Towards Patients with Disabilities” (MSA-PWD) scale:27 This tool was validated in this study population10 and measured the attitudes of medical students towards PWD using a four-point Likert scale (strongly disagree to strongly agree) and demonstrated good internal consistency (Cronbach alpha = 0.816).
- Confidence Dealing with PWD Index:10 This index (Supplementary Material Appendix 2) assessed the self-reported confidence of medical students in dealing with PWD, using a five-point Likert scale (strongly disagree to strongly agree). The total index score, ranging from 4 to 20, was calculated by summing all responses, with higher scores indicating a higher level of confidence (Cronbach alpha = 0.811).
Statistical Analysis
Data from completed forms was imported into a Microsoft Excel spreadsheet. Data analysis was then performed on SPSS software version 25 (Chicago, IL, USA). A descriptive analysis was performed using absolute frequencies and percentages for categorical variables and means and standard deviations (SD) for quantitative measures. Student’s t-test, ANOVA, and Pearson’s correlation were performed for the bivariate analysis. Assumptions of continuous variables’ normality and other conditions were checked via histogram and normal probability plot.
Construct validity of the used tools was assessed previously using the rotated component matrix technique. Moreover, the internal consistency of the scales was assessed using Cronbach’s alpha.
A mediation analysis using PROCESS Macro version 4.2 was used to calculate three pathways in the mediation analysis. While pathway A determined the regression coefficient for the effect of sociodemographic factors on the confidence dealing with PWD, pathway B examined the association between the confidence dealing with PWD on attitudes and clinical experience with disability, and pathway C estimated the total and direct effect of sociodemographic factors on attitudes and clinical experience with disability. The Macro generated bias-corrected bootstrapped 95% confidence intervals (CI) to test the significance of the indirect effect. Mediation was considered significant when the CI for the indirect effect did not include zero. A p-value less than 0.05 was considered statistically significant. (Figure 1) The covariates that were included in the mediation model were those that showed associations with p-value <0.2 in the bivariate analysis. A p-value less than 0.05 was considered significant.
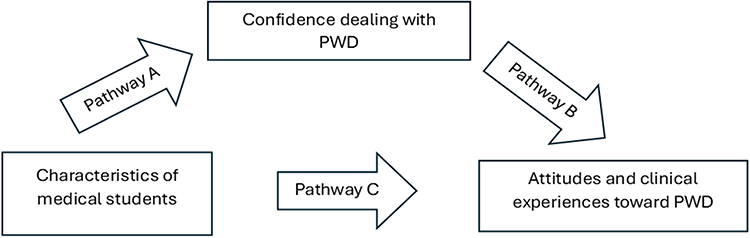 |
Figure 1 Mediation framework – assessment of the mediation of confidence in dealing with PWD on the association between medical students’ characteristics and attitudes toward PWD, and clinical experience with PWD. |
Results
Sample Description
The number of students was evenly distributed across enrollment years, in addition to an even gender distribution in each enrollment year. (Supplementary Table 1A) The study sample consisted of 143 medical students; the majority were of female gender. The mean age was 22.6 (1.42) years. They were distributed across enrollment years as follows: 33 (23.4%) students in med 1, 58 (41.1%) in med 2, 20 (14.2%) in med 3 and 30 (21.3%) in med 4. (Supplementary Table 1B) in addition the gender distribution across enrollment years showed no significant differences (Supplementary Table 1C).
Bivariate Analysis
Supplementary Table 2 showed that higher confidence in dealing with PWD was associated with a more positive attitude towards PWD and better performance in clinical settings involving PWD. Furthermore, female medical students scored significantly lower than their male counterparts in both confidence in dealing with PWD and clinical experience dealing with PWD. Moreover, Med 4 students scored higher in confidence and clinical experience with PWD compared to students in lower enrollment years.
Mediation Analysis Summary
Table 1 presents the correlation between students’ characteristics and attitudes toward PWD and clinical experience with PWD, with mediation analysis involving confidence in dealing with PWD.
 |
Table 1 Summary Mediation Results |
For the year of enrollment, while the indirect effect on the attitude toward PWD as well as the clinical experience with PWD was significant, the absence of a significant direct effect suggests full mediation.
Regarding the association of gender with the attitude toward PWD, the indirect effect was significant, with the absence of a significant direct effect suggesting full mediation.
Regarding the association of gender with clinical experience with PWD, the direct effect was significant, with a significant indirect effect, implying partial mediation (Supplementary Table 3).
Analysis Summary
Figure 2 illustrates the first Analysis: With year of enrollment as the independent variable and attitudes toward PWD as the dependent variable, the results indicated:
- Path A: Significant effect of enrollment year (Med 4 vs Med 1) on confidence in dealing with PWD (Beta = 1.764, p = 0.047).
- Path B: Significant effect of confidence on attitudes toward PWD (Beta = 0.767, p < 0.001).
- Path C (Total Effect): No significant effect of enrollment year on attitudes toward PWD. However, the indirect effect was significant (Beta = 1.353; 95% bootstrap CI = [0.375, 2.541]) (Figure 2).
 |
Figure 2 Mediating effect of self-confidence dealing with PWD on MSA-PWD in terms of year of enrollment (*Significant relationships). |
Figure 3 illustrates the second Analysis: With year of enrollment as the independent variable and clinical experience with PWD as the dependent variable, the findings were:
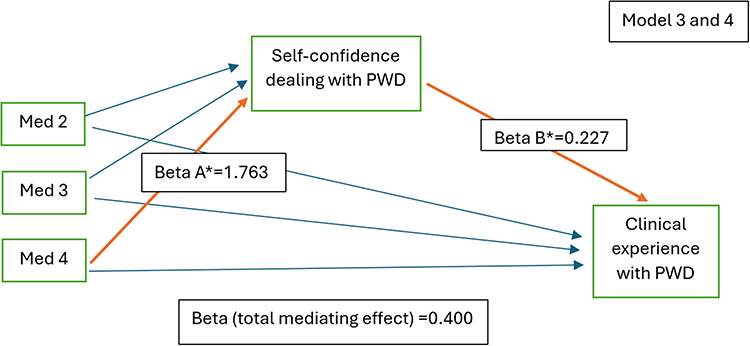 |
Figure 3 Mediating effect of self-confidence dealing with PWD on scenario B in terms of year of enrollment (*Significant relationships). |
- Path A: Significant effect of enrollment year on confidence in dealing with PWD (Beta = 1.764, p = 0.047).
- Path B: Significant effect of confidence on clinical experience with PWD (Beta = 0.227, p < 0.001).
- Path C (Total Effect): No significant direct effect of enrollment year on clinical experience with PWD, although the indirect effect was significant (Beta = 0.400; 95% bootstrap CI = [0.106, 0.740]) (Figure 3).
Figure 4 illustrates the third Analysis: Considering gender as the independent variable and attitudes toward PWD as the dependent variable:
- Path A: Significant effect of gender (Female vs Male) on confidence in dealing with PWD (Beta = −1.352, p = 0.023).
- Path B: Significant effect of confidence on attitudes toward PWD (Beta = 0.792, p < 0.001).
- Path C (Total Effect): No significant direct effect of gender on attitudes toward PWD, but the indirect effect was significant (Beta = −1.070; 95% bootstrap CI = [−2.065, −0.157]) (Figure 4).
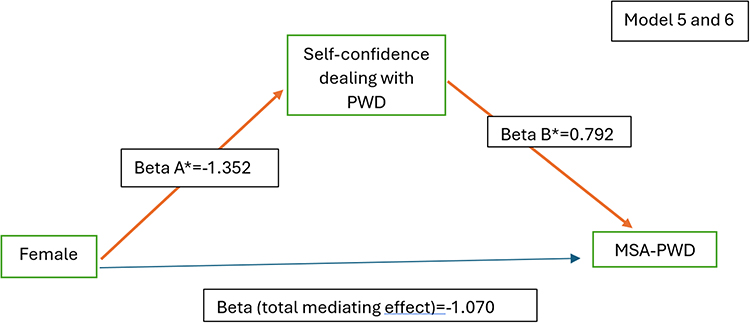 |
Figure 4 Mediating effect of self-confidence dealing with PWD on MSA-PWD in terms of gender (*Significant relationships). |
Figure 5 illustrates the fourth Analysis: With gender as the independent variable and clinical experience with PWD as the dependent variable:
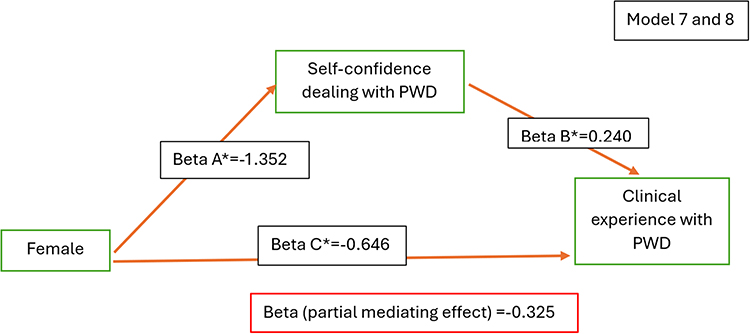 |
Figure 5 Mediating effect of self-confidence dealing with PWD on Scenario B in terms of gender (*Significant relationships). |
- Path A: Significant effect of gender on confidence in dealing with PWD (Beta = −1.352, p = 0.023).
- Path B: Significant effect of confidence on clinical experience with PWD (Beta = 0.240, p < 0.001).
- Path C (Total Effect): Significant direct effect of gender on clinical experience with PWD (Beta = −0.646, p = 0.019), with a significant indirect effect (Beta = −0.325; 95% bootstrap CI = [−0.650, −0.046]) (Figure 5).
Discussion
This study explored the relationship between medical students’ demographic factors, such as gender and class year, and their attitudes and clinical experiences with PWD. It highlights gaps in medical education regarding disability inclusion, a critical component of holistic patient care. To the best of our knowledge, this is the first study to examine the mediating role of students’ self-confidence in dealing with PWD, providing valuable insights into healthcare professionals’ competencies in disability care.
Our findings reveal a significant statistical association between higher enrollment class (Med 4) and both more positive attitudes toward PWD and better clinical experiences with PWD. Self-confidence emerged as a key factor, mediating the relationship between female gender and clinical performance, as well as the indirect positive effects of advanced enrollment years on attitudes and experiences. This suggests that self-confidence is not just a personal trait but a skill that can be nurtured through structured educational strategies. These results emphasize the need for gender-sensitive approaches and structured early interventions in medical education to address disparities and improve confidence.
While we hypothesized that students in their fourth year, with greater knowledge and clinical exposure, would demonstrate more positive attitudes, our findings align with prior studies indicating that the impact of training on attitudes toward PWD may be limited due to methodological challenges.28,29 However, self-confidence appears to play a pivotal role in bridging this gap. Structured early interventions, such as disability-focused training and repeated clinical exposures, could support the development of positive attitudes and clinical skills.30–32 Research consistently supports the link between increased familiarity with PWD and more positive attitudes and clinical outcomes.33–35 To address these issues, medical curricula should integrate simulations, patient interactions, and reflective exercises aimed at building empathy and addressing biases. Empowering medical students to confidently interact with PWD is crucial for their professional development and fostering inclusive healthcare systems that prioritize equitable access and high-quality care for all patients.
Contrary to some studies suggesting that female medical students generally have more positive attitudes toward PWD,36,37 our findings did not support a direct positive effect of gender on these attitudes. Instead, female students reported lower self-confidence in dealing with PWD, which negatively influenced both their attitudes and clinical experiences. This finding underscores the need for gender-sensitive interventions to address confidence gaps through targeted strategies, such as mentorship programs, skill-building workshops, and supportive feedback mechanisms. These approaches should empower female students to overcome cultural and systemic barriers, fostering equity in clinical preparedness.
This mediation model highlights the complex relationship between gender, self-confidence, and attitudes toward PWD, emphasizing the pivotal role of self-confidence as a mediator. While academic and clinical performances often show no consistent gender differences,38,39 our findings revealed that female students reported significantly more negative self-perceptions in clinical settings involving PWD, largely mediated by lower self-confidence. Additionally, societal and cultural factors contributing to gender disparities in confidence must be acknowledged. Efforts to promote gender equity within the learning environment such as implementing inclusive policies, fostering leadership opportunities for female students, and addressing implicit biases could help mitigate these disparities and improve both attitudes and clinical performance.
Several culturally relevant factors may contribute to the observed gender differences. In Levantine societies, cultural norms and social conditioning often emphasize traditional gender roles, which can influence women’s self-perception and professional interactions. Women are often conditioned to express emotions more openly and may underestimate their competencies compared to men, resulting in lower self-reported confidence and heightened anxiety. Additionally, gender bias and subtle forms of discrimination can exacerbate this anxiety, diminishing self-efficacy and confidence particularly in challenging clinical scenarios. Moreover, women in the Middle East may face discrimination influenced by legal, socio-cultural, and religious factors, as well as decision-making structures, public policies, and security issues.40,41 The patriarchal norms prevalent in many Middle Eastern societies can further undermine women’s confidence, adversely affecting their clinical performance and attitudes towards PWD.42 Addressing these systemic issues within medical education through policies promoting gender equity and inclusion is critical to mitigating such disparities.
Implications for Medical Education
The findings of this study underscore the importance of integrating targeted interventions within medical curricula to enhance self-confidence among students, particularly in interactions with PWD. Implementing structured clinical exposures, such as OSCEs featuring standardized patients with disabilities, can provide practical experience and improve comfort levels in managing diverse patient populations. Additionally, incorporating reflective practices and mentorship programs may help address self-confidence disparities, especially among female students, fostering a more inclusive and supportive learning environment.
Limitations
While this study makes important strides by examining the mediation effect of self-confidence on medical students’ attitudes and clinical performance dealing with PWD, it is not without limitations. The cross-sectional design precludes the ability to establish causality, and our methodology does not fully eliminate the potential for selection or information bias, which could lead to an underestimation of the findings. Additionally, the reliance on self-reported measures may have introduced social desirability bias, as students might overstate their confidence or positive attitudes toward PWD. There is also, some concerns about the low internal consistency for the Scenario B clinical tool, despite being common in practical assessments.
A notable limitation is the lack of qualitative data, which could provide richer insights into the personal experiences and challenges faced by students when interacting with PWD. Future studies could incorporate mixed methods to combine the strengths of qualitative and quantitative approaches. Another limitation lies in the generalizability of the findings, as the study was conducted in a single institution with a specific cultural context. Expanding this research to include multiple institutions across diverse socio-cultural settings could provide a more comprehensive understanding of the issues at hand. Despite these challenges, the study holds strengths such as a robust sample size, rigorous standardized analysis, and a theoretical framework grounded in “self-efficacy theory” applied within complex models. These strengths ensure that the findings provide valuable insights for improving medical education.
Conclusion
This research highlights the role of self-confidence in mediating medical students’ attitudes and performance with PWD. Students in higher years showed more positive attitudes and better performance, while female students exhibited lower confidence and less positive attitudes. These findings suggest the need for curriculum reforms that not only incorporate disability-focused training but also address gender-specific barriers to confidence-building. Enhancing curriculum design to include simulation-based learning, structured clinical exposures (OSCEs), and mentorship programs can foster greater competence and self-efficacy, ensuring all students are equipped to provide compassionate and effective care to PWD. This will help inform on policy and accreditation implications for medical schools striving to meet inclusive education standards.
Future research should prioritize longitudinal studies to evaluate the impact of repeated clinical exposures to PWD on self-confidence, attitudes, and clinical performance. Additionally, interventions designed to enhance self-efficacy in dealing with PWD, along with qualitative studies exploring students’ personal experiences, could provide deeper insights for curriculum development. Such efforts would contribute to building healthcare systems that prioritize equity and inclusion, ensuring high-quality care for PWD and other marginalized populations.
Abbreviations
PWD, persons with disabilities; MSA-PWD, Medical Students’ Attitudes Towards Patients with Disabilities; LAUSOM, Lebanese American University Gilbert & Rose-Marie Chagoury School of Medicine; OSCE, Observed Structured Clinical Examination.
Ethical Considerations
The revised manuscript complies with the Declaration of Helsinki.
Acknowledgments
This study has been supported by the Lebanese American University President Intramural Research Fund, project number 10069.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors reported that there is no funding associated with the work featured in this article.
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. Artino AR. Academic self-efficacy: from educational theory to instructional practice. Perspect Med Educ. 2012;1(2):76–85. doi:10.1007/s40037-012-0012-5
2. Bandura A. On the functional properties of perceived self-efficacy revisited. J Manage. 2012;38(1):9–44. doi:10.1177/0149206311410606
3. Stegers-Jager KM, Cohen-Schotanus J, Themmen APN. Motivation, learning strategies, participation and medical school performance. Med Educ. 2012;46(7):678–688. doi:10.1111/j.1365-2923.2012.04284.x
4. RM K, JRL K. Self-efficacy beliefs of medical students: a critical review. Perspect Med Educ. 2018;7(2):76–82. doi:10.1007/s40037-018-0411-3
5. Mowlaie M, Besharat MA, Pourbohlool S, Azizi L. The mediation effects of self-confidence and sport self-efficacy on the relationship between dimensions of anger and anger control with sport performance. Procedia Soc Behav Sci. 2011;30:138–142. doi:10.1016/j.sbspro.2011.10.027
6. Heffernan CJ. Social foundations of thought and action: a social cognitive theory, Albert Bandura Englewood Cliffs, New Jersey: prentice Hall, 1986, xiii + 617 pp. Hardback. US$39.50. Behav Change. 1988;5(1):37–38. doi:10.1017/S0813483900008238
7. Blanch DC, Hall JA, Roter DL, Frankel RM. Medical student gender and issues of confidence. Patient Educ Couns. 2008;72(3):374–381. doi:10.1016/j.pec.2008.05.021
8. Gottlieb M, Chan TM, Zaver F, Ellaway R. Confidence-competence alignment and the role of self-confidence in medical education: a conceptual review. Med Educ. 2022;56(1):37–47. doi:10.1111/medu.14592
9. Santoro JD, Yedla M, Lazzareschi DV, Whitgob EE. Disability in US medical education: disparities, programmes and future directions. Health Educ J. 2017;76(6):753–759. doi:10.1177/0017896917712299
10. Karam VGY, Malhab SB, Bahous S, Salameh P, Khoury-Malhame ME, Asmar N. Medical students attitudes towards patients with disability: a scale validation study. BMC Med Educ. 2024;24(1):1226. doi:10.1186/s12909-024-06238-9
11. Baroud M, Ola M. Healthcare needs and barriers of persons with disabilities: an exploratory study among Syrian refugees, Palestine refugees from Syria and Lebanon. 2018. Available from: https://www.aub.edu.lb/ifi/Documents/publications/research_reports/2018-2019/20181004_healthcare_needs_persons_with_disabilities.pdf.
12. Wilson MC, Scior K. Attitudes towards individuals with disabilities as measured by the implicit association test: a literature review. Res Develop Disab. 2014;35(2):294–321. doi:10.1016/j.ridd.2013.11.003
13. Guzowski A, Kulak-Bejda A, Stelcer B, et al. Medical students’ perceptions of people with disabilities. Progress Health Sci. 2016;6(2):125. doi:10.5604/01.3001.0009.5159
14. Smith DL. Erratum to disparities in patient-physician communication for persons with a disability from the 2006 medical expenditure panel survey (MEPS). Disability Health J. 2010;3(2):130. doi:10.1016/j.dhjo.2009.11.005
15. Meeks LM, Poullos P, Swenor BK, DeIorio NM. Creative approaches to the inclusion of medical students with disabilities. AEM Educ Train. 2020;4(3):292–297. doi:10.1002/aet2.10425
16. Marzolf B, Harper D, Plegue M, Okanlami O. Are medical students adequately trained to care for persons with disabilities? Ann Family Med. 2022;20(Suppl 1). doi:10.1370/afm.20.s1.2620
17. Brown RS, Graham CL, Richeson N, Wu J, McDermott S. Evaluation of medical student performance on objective structured clinical exams with standardized patients with and without disabilities. Acad Med. 2010;85(11):1766–1771. doi:10.1097/ACM.0b013e3181f849dc
18. Sneed RC, May WL, Stencel CS. Training of pediatricians in care of physical disabilities in children with special health needs: results of a two-state survey of practicing pediatricians and national resident training programs. Pediatrics. 2000;105(3):554–561. doi:10.1542/peds.105.3.554
19. VanPuymbrouck L, Friedman C, Feldner H. Explicit and implicit disability attitudes of healthcare providers. Rehab Psychol. 2020;65(2):101–112. doi:10.1037/rep0000317
20. Long-Bellil LM, Robey KL, Graham CL, Minihan PM, Smeltzer SC, Kahn P. Teaching medical students about disability: the use of standardized patients. Acad Med. 2011;86(9):1163–1170. doi:10.1097/ACM.0b013e318226b5dc
21. Vajapey SP, Weber KL, Samora JB. Confidence gap between men and women in medicine: a systematic review. Current Orthopaedic Prac. 2020;31(5):494–502. doi:10.1097/BCO.0000000000000906
22. Shakespeare T, Iezzoni L, Groce N. The art of medicine: disability and the training of health professionals. Lancet. 2009;374(9704):1815. doi:10.1016/S0140-6736(09)62050-X
23. Faught E, Morgan TL, Tomasone JR. Five ways to counter ableist messaging in medical education in the context of promoting healthy movement behaviours. Can Med Ed J. 2022. doi:10.36834/cmej.74119
24. Findler L, Vilchinsky N, Werner S. The multidimensional attitudes scale toward persons with disabilities (MAS): construction and validation. Rehab Counsel Bulletin. 2007;50(3):166–176. doi:10.1177/00343552070500030401
25. Tervo RC, Palmer G. Health professional student attitudes towards people with disability. Clin Rehabilitat. 2004;18(8):908–915. doi:10.1191/0269215504cr820oa
26. Satchidanand N, Gunukula SK, Lam WY, et al. Attitudes of healthcare students and professionals toward patients with physical disability: a systematic review. Am J Phys Med Rehabil. 2012;91(6):533–545. doi:10.1097/PHM.0b013e3182555ea4
27. Symons AB, Fish R, Mcguigan D, Fox J, Akl EA. Development of an instrument to measure medical students’ attitudes toward people with disabilities. Intell Develop Disab. 2017;50(3):251. doi:10.1352/1934-9556-50.3.251
28. Cocksedge S, Ahmed A, Barr N, Hart J, Sanders T. Maintenance of learning following teaching communication, disability and diversity to medical students. EIMJ. 2014;6(1). doi:10.5959/eimj.v6i1.196
29. Ioerger M, Flanders RM, French-Lawyer JR, Turk MA. Interventions to teach medical students about disability: a systematic search and review. Am J Phys Med Rehabil. 2019;98(7):577–599. doi:10.1097/PHM.0000000000001154
30. Almohayya BM, Alotaibi AA. Disability attitudes in healthcare scale: translation and cross-cultural validation into Arabic using various medical samples. Disabil Rehabil. 2024;1–10. doi:10.1080/09638288.2024.2385735
31. Robey KL, Gwiazda J, Morse J. Nursing students’ self-attributions of skill, comfort, and approach when imagining themselves caring for persons with physical impairments due to developmental disability. J Dev Phys Disabil. 2001;13(4):361–371. doi:10.1023/A:1012233428850
32. Wilkinson J, Dreyfus D, Cerreto M, Bokhour B. “Sometimes I feel overwhelmed”: educational needs of family physicians caring for people with intellectual disability. Intellect Dev Disabil. 2012;50(3):243–250. doi:10.1352/1934-9556-50.3.243
33. Shakespeare T, Kleine I. Educating health professionals about disability: a review of interventions. Health Soc Care Educ. 2023;2(2):20–37. Available from: https://www.tandfonline.com/doi/abs/10.11120/hsce.2013.00026.
34. Clarke L, Tabor HK, Gisondi MA. How are students learning to care for people with disabilities?: exploring the curriculum design of a sample of disability electives offered by US health professions schools. Disabil Rehabil. 2024;46(16):3749–3759. doi:10.1080/09638288.2023.2254694
35. Lynch J, Last J, Dodd P, Stancila D, Linehan C. “Understanding disability”: evaluating a contact-based approach to enhancing attitudes and disability literacy of medical students. Disabil Health J. 2019;12(1):65–71. doi:10.1016/j.dhjo.2018.07.007
36. Paris MJ. Attitudes of medical students and health-care professionals toward people with disabilities. Arch Phys Med Rehabil. 1993;74(8):818–825. doi:10.1016/0003-9993(93)90007-w
37. Tervo RC, Azuma S, Palmer G, Redinius P. Medical students’ attitudes toward persons with disability: a comparative study. Arch Phys Med Rehabil. 2002;83(11):1537–1542. doi:10.1053/apmr.2002.34620
38. Robinson KA, Perez T, White-Levatich A, Linnenbrink-Garcia L. Gender differences and roles of two science self-efficacy beliefs in predicting post-college outcomes. J Exp Educ. 2022;90(2):344–363. doi:10.1080/00220973.2020.1808944
39. Hartman RL, Barber EG. Women in the workforce. Gender Manage. 2020;35(1):92–118. doi:10.1108/GM-04-2019-0062
40. Nora LM, McLaughlin MA, Fosson SE, et al. Gender discrimination and sexual harassment in medical education: perspectives gained by a 14-school study. Acad Med. 2002;77(12):1226–1234. doi:10.1097/00001888-200212000-00018
41. Babaria P, Abedin S, Berg D, Nunez-Smith M. “I’m too used to it”: a longitudinal qualitative study of third year female medical students’ experiences of gendered encounters in medical education. Soc Sci Med. 2012;74(7):1013–1020. doi:10.1016/j.socscimed.2011.11.043
42. Moghadam VM. Patriarchy in transition: women and the changing family in the middle east. J Comp Family Stud. 2019. doi:10.3138/jcfs.35.2.137
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
How Do Medical Students Perceive Their Research Experiences and Associated Challenges?
Alyousefi N, Alnojaidi J, Almohsen A, Alghanoum S, Alassiry G, Alsanad L, Alzeer S
Advances in Medical Education and Practice 2023, 14:9-20
Published Date: 6 January 2023
Knowledge, Attitudes, and Educational Gaps About Vaccination in Chinese Medical Students and Residents: A Pilot Study from a Single Tertiary Referral Center
Liu X, Chen Y, Dai H, Li R, Ding Y, Wu J, Shi X
Infection and Drug Resistance 2024, 17:5315-5323
Published Date: 29 November 2024